
Abstract
Background
Traumatic attacks from large feline predators cause a small yet significant burden of disease in rural populations, are increasing in frequency, cause complex injuries and worsen human–wildlife conflicts. Data on the traumatic injury pattern found in victims of these animals is sparse, and this study aimed to collate and synthesise patterns of injury to inform the care and management of these patients.
Methods
A multi-ethnographic literature search (PubMed, Embase, Web of Science, Google Scholar, and other sources) was performed on 12/1/21 to capture all available data describing anatomical injury and the mechanism of injury sustained by humans from attacks by lions, leopards and tigers. Quality and bias assessment was performed using the Joanna Briggs Critical Evaluation tools.
Results
Of 5110 studies identified, 42 were included in this review totalling 84 individual patient cases. A total of 85% of fatal injuries were due to exsanguination combined with neuroaxis injury of the neck. All wounds were susceptible to tissue loss, infection and long-term neuro-vascular complications. Leopards injured anterior-midline structures of the neck more often than did lions and tigers, while the latter caused high-energy fractures. Time lag to treatment for survivors of wild attacks extended to multiple days, and occult injury was common.
Conclusion
In addition to the primary finding of complex neck injury, this study generated specific patterns of injury seen from the included species and highlighted occult injury and healthcare disparity as challenges in providing patient care.
Introduction
Injury patterns from apex predators such as felid carnivores are poorly described and understood. 1 While infrequent, attacks by Panthera species (lions, leopards and tigers) generate a significant burden of traumatic injury in communities that reside near these species. Many hundreds of attacks occur each decade in the habitat countries of lions, 2 leopards 3 and tigers. 4 Outside of habitat regions, large volume captivity in the global northwest, 5 and encroaching suburbia into the wilderness of developing countries 6 means the global number of attacks is rising.
This produces morbidity and mortality in communities that depend on agrarian occupations for subsistence, 7 undermines conservation efforts and has become an important concern for those managing human–wildlife conflict. 8
Available injury data from big cats is sparse and is largely confined to case reports, 1 with current management based on expert opinion and scoping trauma algorithms. Clinically the wounds inflicted are high energy, complex and require pre-hospital input and multi-disciplinary secondary care. Sequalae include polymicrobial infection, 9 enduring neurology 10 and complex bony and soft tissue neck wounds. 5 Generating knowledge of common injuries or complications from the specific mode of injury of a big cat attack, may lead to earlier identification of occult and treatable injury at the scene, and within a hospital. Identifying these patients as victims of complex trauma may lead to earlier multi-specialty treatment. Overall, improved patient care may improve human–wildlife conflict relations, especially in the context of reduced human tolerance to living near conservation species. 11 This study, therefore, aims to generate both a general and species-specific injury pattern resulting from attacks by lions, leopards and tigers, so that future healthcare providers can plan for these unique types of injuries.
Methods
Registration and protocol
A structured pre-registered search protocol was registered with PROSPERO 12 (ID-CRD42020223448) and conducted according to PRISMA guidelines. 13
The search protocol was completed with no deviation. After expert opinion suggested captive animals would attack similarly to wild animals, as they are non-domesticated, this study also included events from captive settings.
Endpoints were altered to focus on injury patterns alone due to the severe methodological heterogeneity found in studies quoting only mortality figures.
PEO and inclusion criteria
The
Only English language studies were included. There was no timeframe limitation, and all study types were eligible. Patients could only be included if the species of attacking animal was clearly stated as one of interest.
Search strategy and data collection
A multi-ethnographic search protocol was created including electronic databases PubMed, Embase, Web of Science (WoS) and Google Scholar, in addition to backwards and forwards searching of the included studies. A total of 60 organisations, field experts and government departments were contacted to supply new or supplementary data of which 11 responded (Supplementary Material: Appendix 1). The search terms for PubMed, Embase and Web of Science are found in Figure 1 and Supplementary Material: Appendix 2, while for Google Scholar, the search strategy included ‘Attack (species of big cat)’ for three searches, and ‘Bite (species of big cat)’ for three searches. The final study was included on 20/5/21 and all searches were conducted by the author JK.
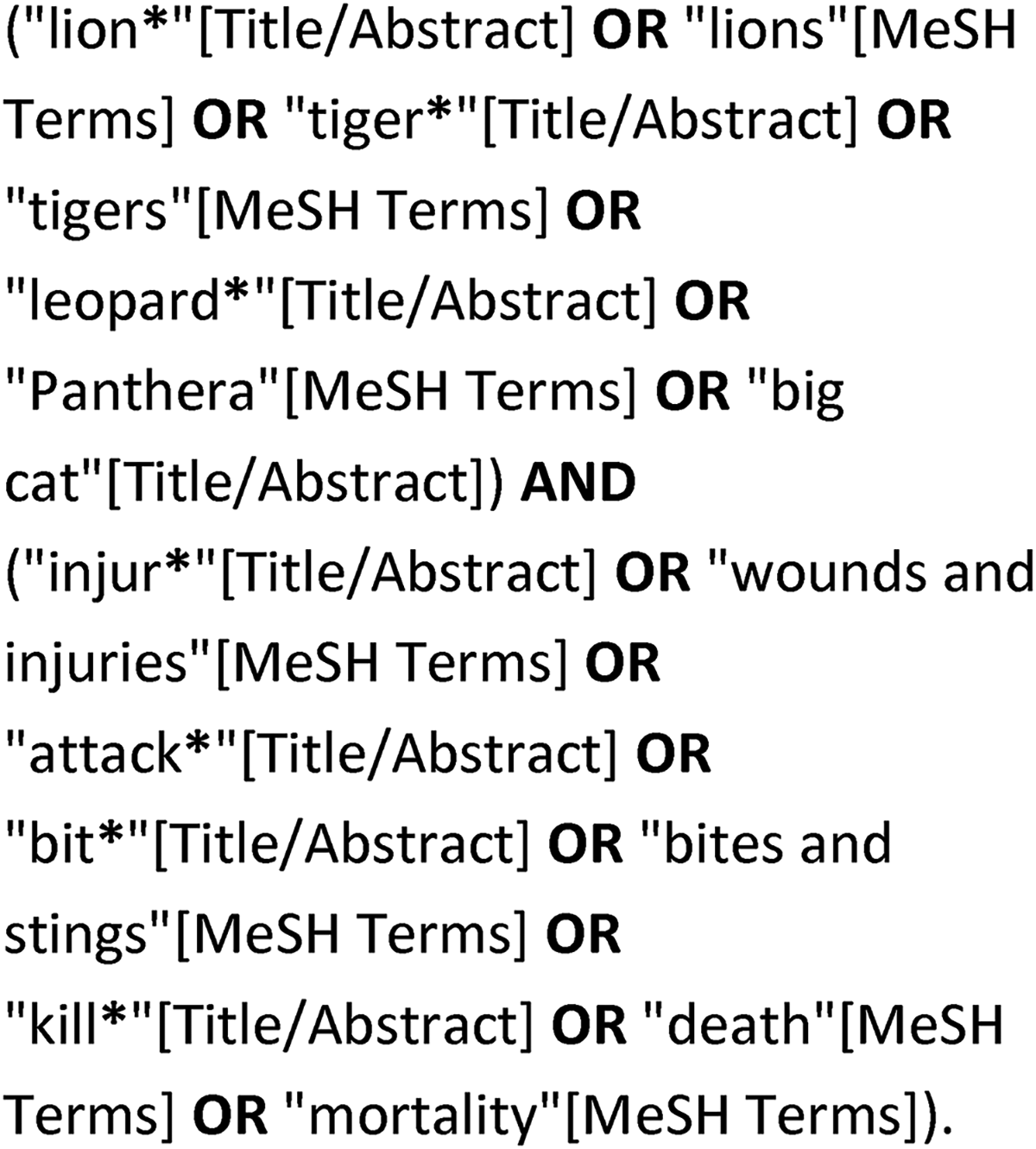
Pubmed search strategy.
Data screening and extraction
Reference titles and abstracts from all sources were screened manually for relevancy and reduced to a list for full-text retrieval by JK. Full texts were assessed for quality and content by two reviewers (JK and JLT) and reduced to the final list. The included studies data were extracted into Microsoft ExcelTM to comprise event demographics, wild/captive event, species of cat, injury description, complications and mortality.
Quality assessment
Risk of Bias combined with methodological quality was assessed with the Joanna Briggs Tools for Case Reports 14 and Case Series 15 by JK. Publication bias and selective reporting were addressed by contacting authors, governmental departments and non-governmental organisations, and the inclusion of grey literature from non-medical databases. Missing data were addressed by contacting the authors. Studies of poor descriptive quality were excluded and agreement on the final included studies was achieved by two reviewers (JK and JLT).
Meta-analysis
The descriptive nature of the endpoints and the apparent population, clinical and methodological heterogeneity prohibited a statistical meta-analysis. A narrative analysis was conducted, and key data synthesised included mechanism of injury, anatomical site most affected, wound characteristics and long-term complications. To account for the heterogeneity in the event demographics, subgroup analyses were conducted on captive versus wild exposures, adult versus paediatric injury patterns and the injury pattern inflicted by each species of big cat.
Results
Search results
A total of 5110 items from all sources were returned, of which 211 full texts were assessed for eligibility, yielding 42 included studies (Figure 2 and Table 1). Of those excluded; 103 lacked sufficient detail relating to injuries (including all author and organisational responses), five had inseparable data collated with other animals, 53 had no relevant data, six contained duplicated data and two were non-English language.
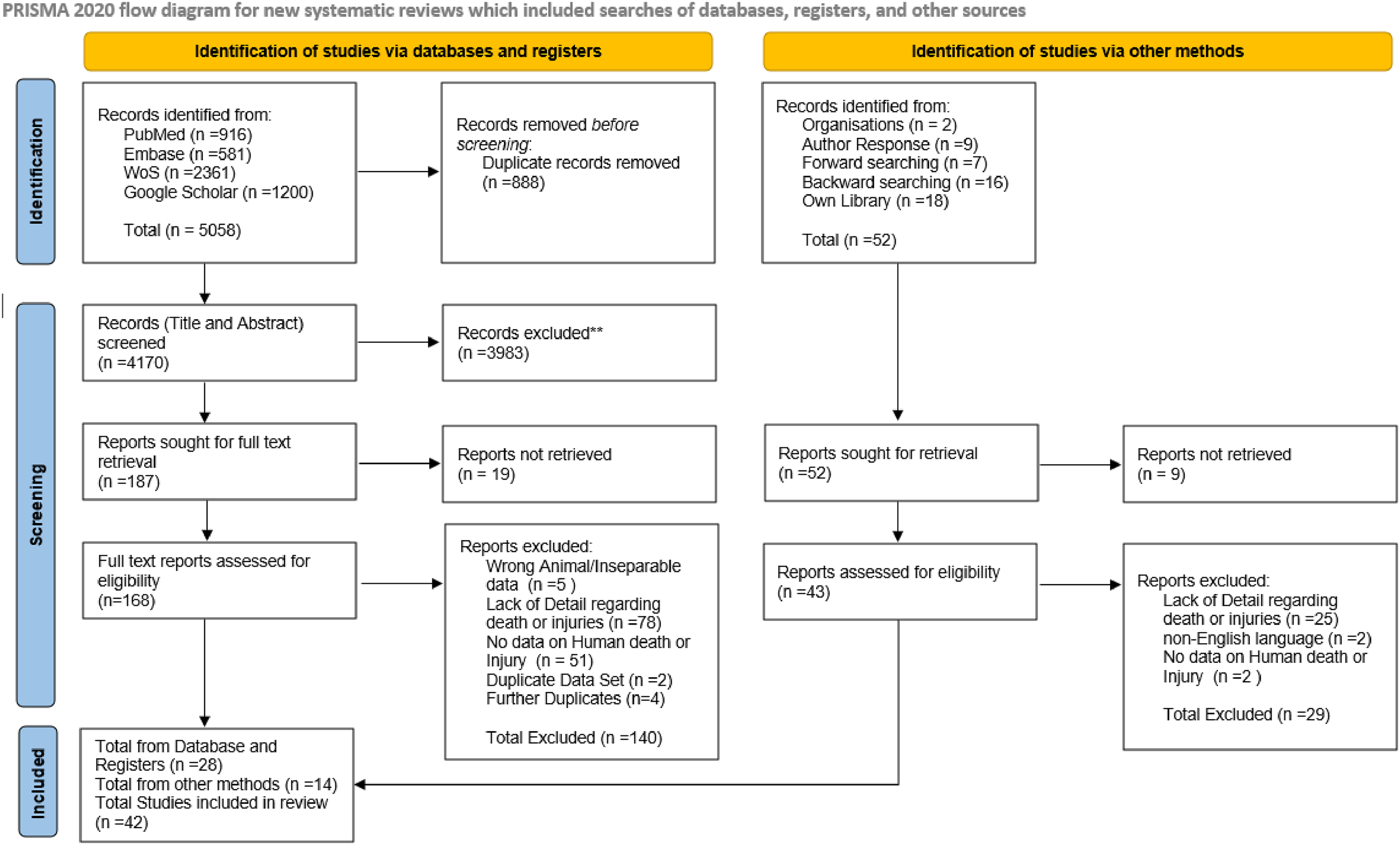
PRISMA flowchart of search and study selection.
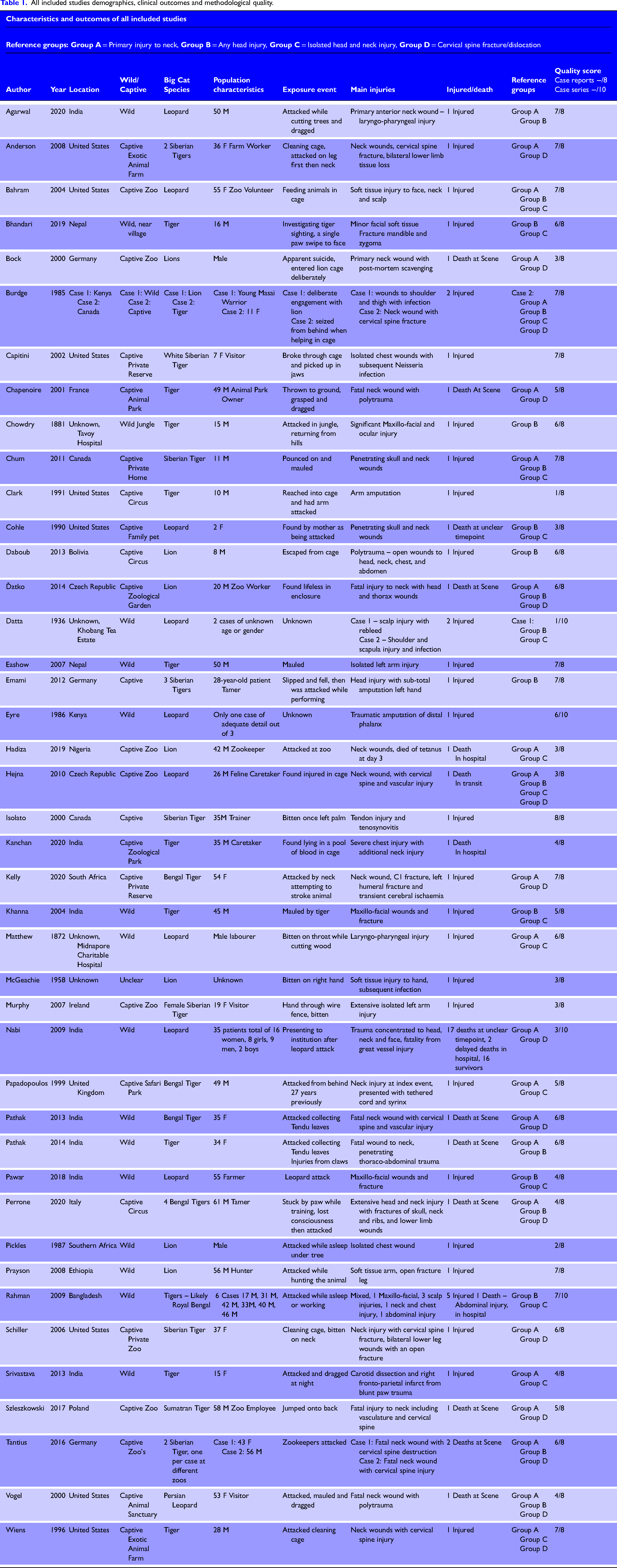
All included studies demographics, clinical outcomes and methodological quality.
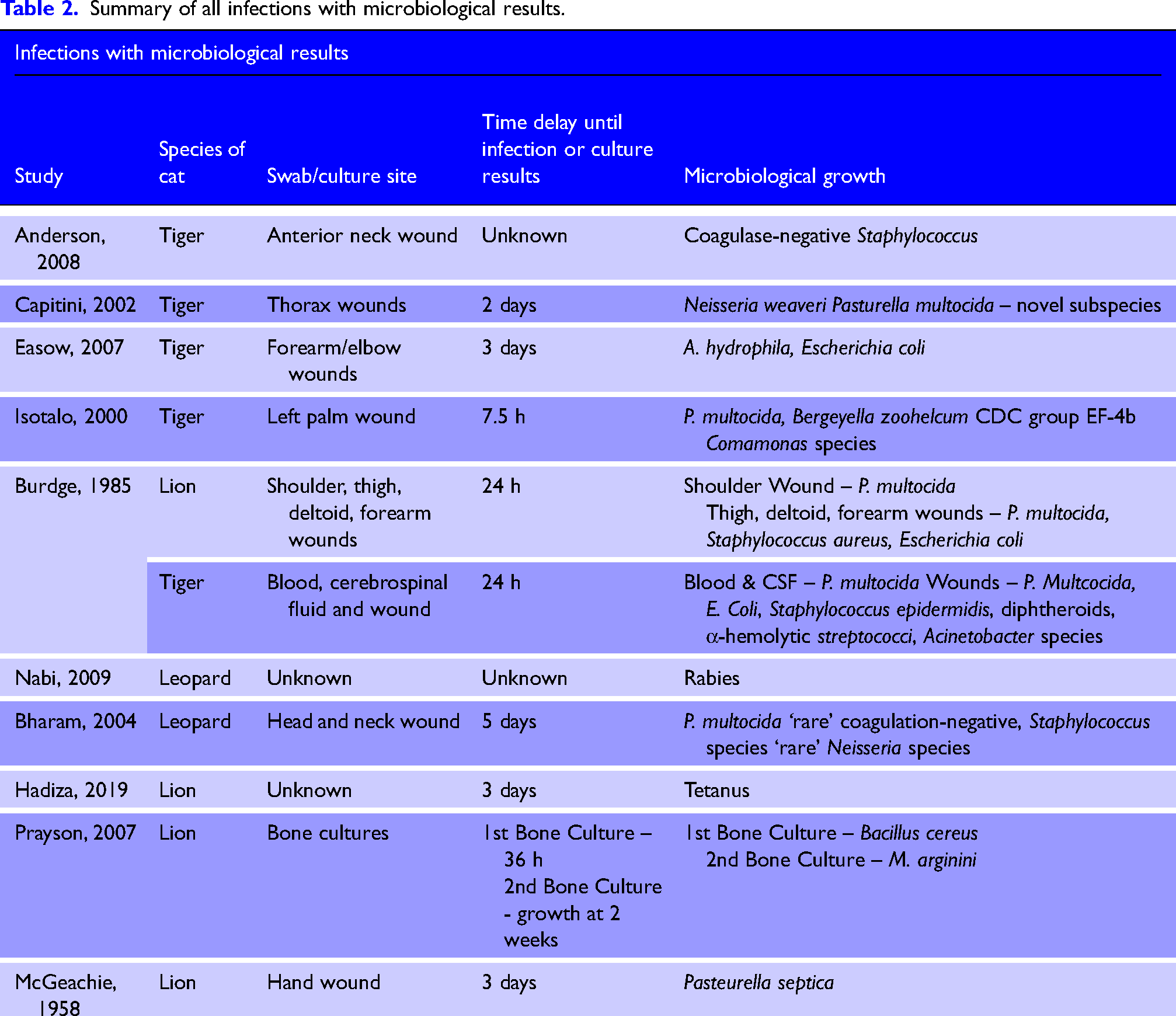
Summary of all infections with microbiological results.
Quality of included research
A total of 84 total patients’ cases were of a sufficient descriptive quality to facilitate data extraction; 38 studies were case reports and four were case series. Case reports described injuries in detail and were generally high quality with 21 studies scoring ≥ 6/8. Only five studies reported patient demographics adequately,16–20 and detail of the clinical timeline and status on arrival to the hospital varied, including the recording of subjective observations such as ‘pale’ 21 and ‘toxic’ 22 rather than numerical clinical parameters. Only one case series scored highly in the domains 9 for consecutive and complete inclusion. The largest study, numbering 35 cases, did not report consecutive or complete inclusion and pooled injury data from deceased patients and survivors. 23 A full quality assessment is found in Supplementary Material: Appendix 3.
Key characteristics of study population and exposures
Of the 84 cases from the included 42 studies, there were 31 tiger cases, 45 leopard cases and eight cases of a lion attack; 24 studies took place in captive settings and 16 in wild settings – one study included patients from both settings, 22 and one study was unclear on the setting. 24
The captive-setting injuries mainly took place in the global northwest while attacks in the wild took place in habitat countries of continental Africa and Asia. Population demographics, activities and time of death in relation to the attack are recorded in Table 1, with a total of 50 survivors and 34 deaths, of which 10 were confirmed at the scene. There were nine10,21,22,25–30 paediatric cases of sufficient detail and only one paediatric fatality. 29
Pooled data from all cats: Anatomical injuries
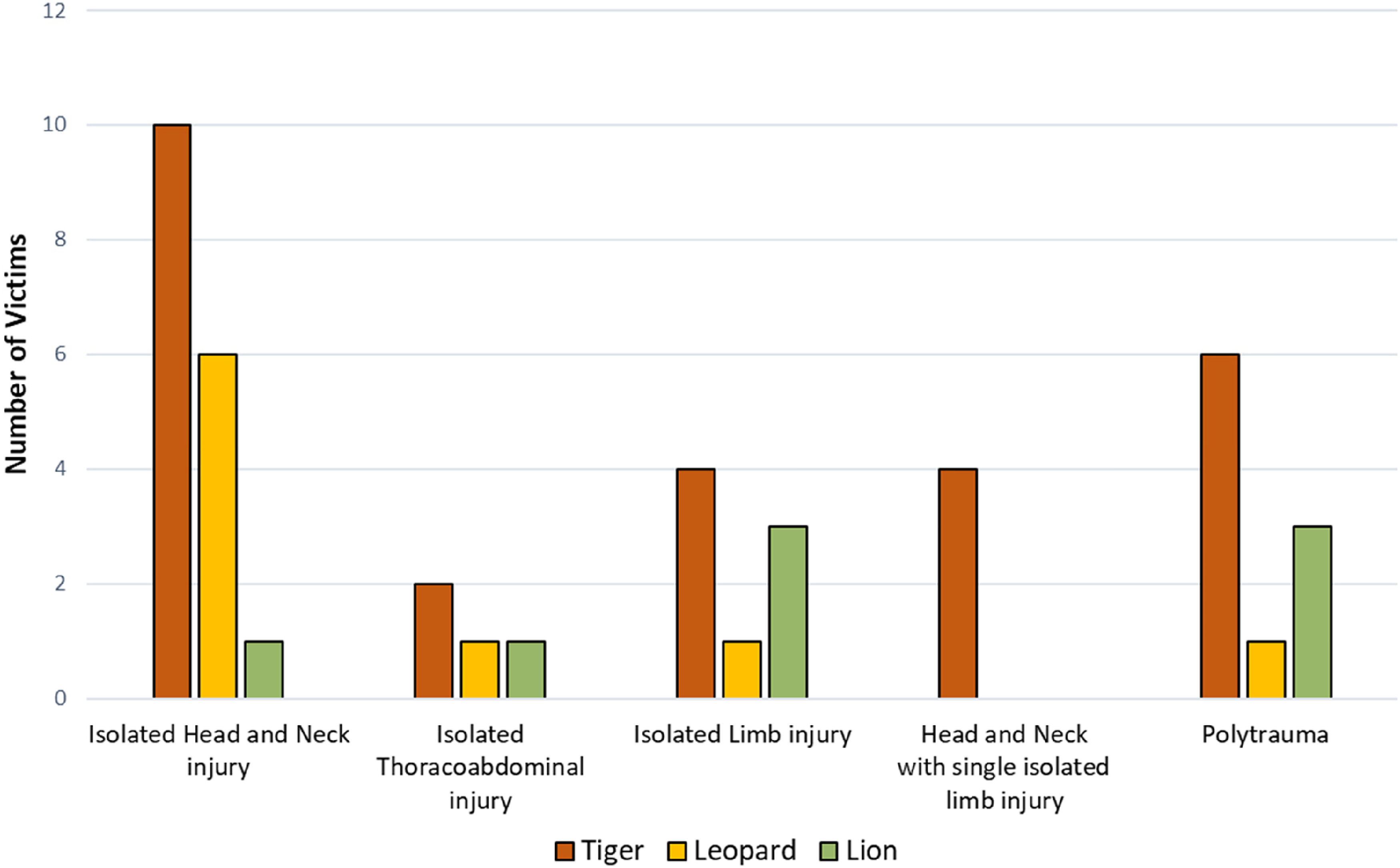
Of 84 included cases, 40 sustained their primary injury to the neck (Table 1, Group A), of which 29 were fatal. The anterior and posterior triangles were equally affected, and wounds were spaced at the extremes of the neck by paired infra-auricular and supraclavicular wounds. The second most wounded was the head, including face and calvarium, with one fatal injury 29 and 109,25,27,31–34 primary injuries in survivors. Additionally, a large proportion of all cases, no matter their primary injury, sustained at least one head wound (Table 1, Group B).
There were six9,18,26,35–37 primary injuries to the thorax with two fatalities,18,35 the only case of isolated abdominal injury proved fatal, 9 and all cases involving only limb injuries survived.20,22,24,28,38–41
Pooled data from all cats: Pattern of injury themes
An attack confined solely above the clavicles was the most common injury pattern (Table 1, Group C) (Figure 3). Of the eight patients who sustained only limb injuries, four were results of captive events28,38 or attempts to engage the animal.22,40 Polytrauma with multi-organ involvement was frequent (n = 10)5,16,18,21,35,36,42–45 and lethal with only three survivors.5,21,42 Deaths at the scene or in transit were due to combined exsanguination from carotid sheath contents and lethal neuroaxis injury. The five deaths in those surviving to hospital arose from infection in four cases – rabies 23 from a leopard, tetanus 46 from a lion and two cases of sepsis.9,23 Only one patient died in hospital from bleeding, 35 while all other exsanguination deaths occurred prehospital. All species dragged their victims once clasped in their jaws with distances reaching 60 m 44 and associated wound contamination was recorded in 38 patients.5,6,23,32 Transfixion of the neck by canines was identified in six cases,5,19,42,43,47,48 and was a causal agent of spinal injury5,19,43,47,48 and vascular injury42,48 due to ligamentous rupture and vessel shearing.
Common patterns of injury.
Pooled injury pattern of all cats: Wound morphology and fracture pattern
Wounds from bites and claws were deep, involved neurovascular structures and tracked to the cervical spine 48 and base of the skull. 17 Except for six cases where paws or claws were the main inflictor,9,10,18,22,25,31 bites were the primary vehicle of injury. Bite wounds were paired17,36,43,44,48 consisting of two to four wounds separated in space generating large oval injuries at the skin with diameters of 2–3 cm,17,35,48 and depths up to 7 cm, 44 with a surrounding soft tissue crush injury. 49
Teeth caused direct fracture to the skull 29 and cervical spine, 48 and deep longitudinal scalp wounds were a common source of bleeding in 16 cases.6,9,16,17,21,22,27,29–31,33,44,50,51
Penetrating thoracoabdominal trauma was principally perpetrated by claws (n = 8).18,19,31,35,36,43,45,48 Claw wounds were lesser in diameter, 18 linear rather than oval and typified by superficial grazes leading to the puncture site.16,48 Blunt injuries such as facial fractures, 25 vascular shearing 10 and unconsciousness 36 were results of single paw swipes or holds.
Ongoing bleeding was recorded in 11 cases at prolonged intervals post-trauma,6,9,21,27,31,34,49 ranging from 5 h 6 to more than 2 days (n = 2).31,34 Infection and inoculation were noted in 16 cases9,20,22,23,26,31,39,40,42,44,46,50 and was often polymicrobial with unusual organisms (Table 2). Long-term complications manifested in enduring hemiplegia,10,22 single limb weakness,5,49 pseudomeningocele, 42 syrinx 52 and pharyngeal and swallowing problems.30,53 Compound cervical spine fracture or dislocation was common (Table 1, Group D) and included multilevel injury in seven patients16,19,36,42,43,45,48 (Figure 4). Mandibular fracture6,9,17,25,29,34,36 accounted for 70% of maxillofacial fractures, and the temporal and occipital bones were the most fractured of the calvarium.21,22,29,30,36
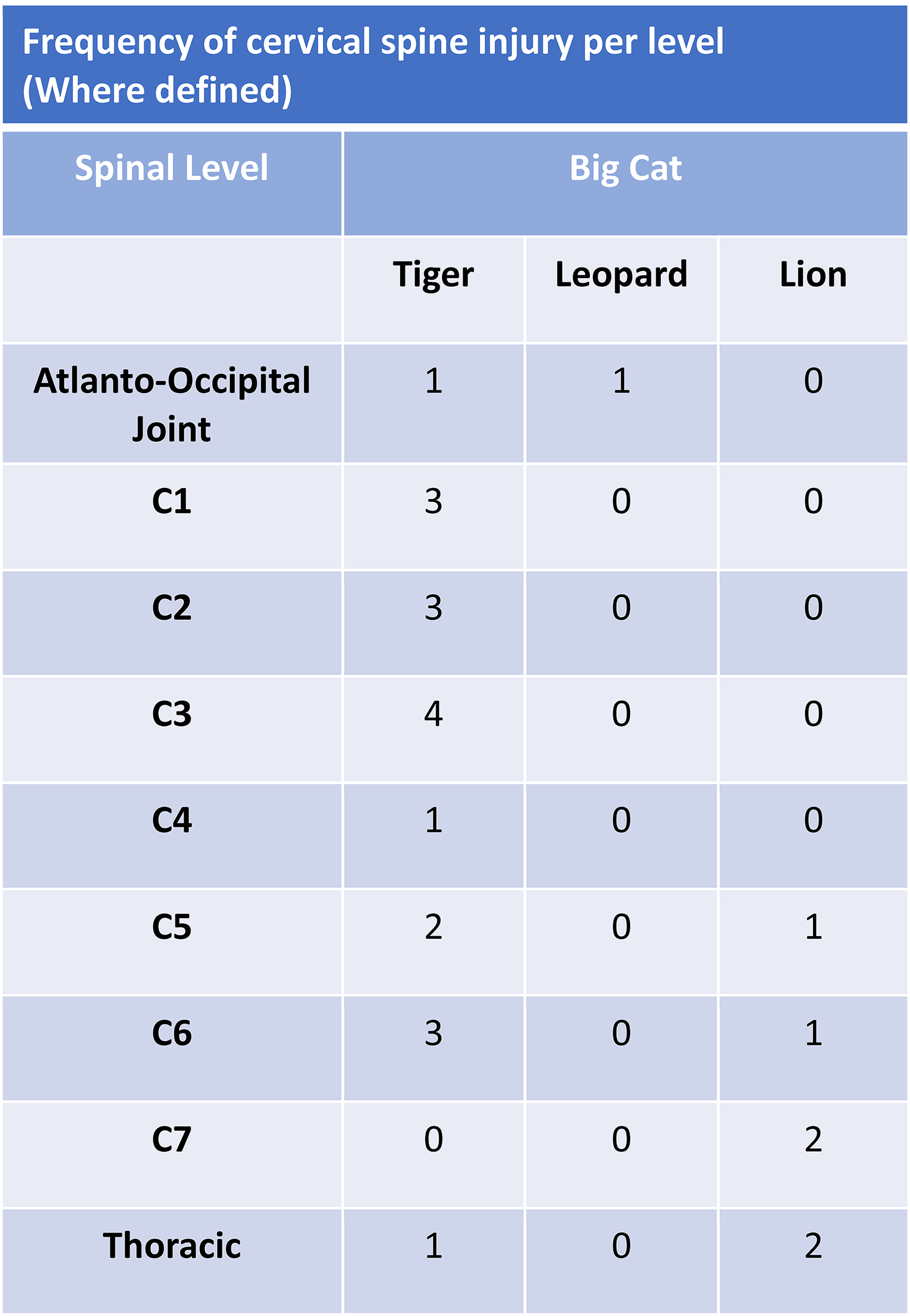
Frequency of cervical spine injury per level.
Unique injury patterns per species
Differences between species were found in the global fracture pattern, and bite locations of the neck. Fractures below the clavicles were more common in lions and tigers (Figure 5), the latter causing bilateral rib fractures,35,36 a scapula fracture 35 and the only sternal fracture-dislocations in this review.19,36 Cervical spine injury pattern in tigers involved the higher and lower spinal levels with only one recorded C4 fracture, 36 while lions fractured lower spinal levels (Figure 4).
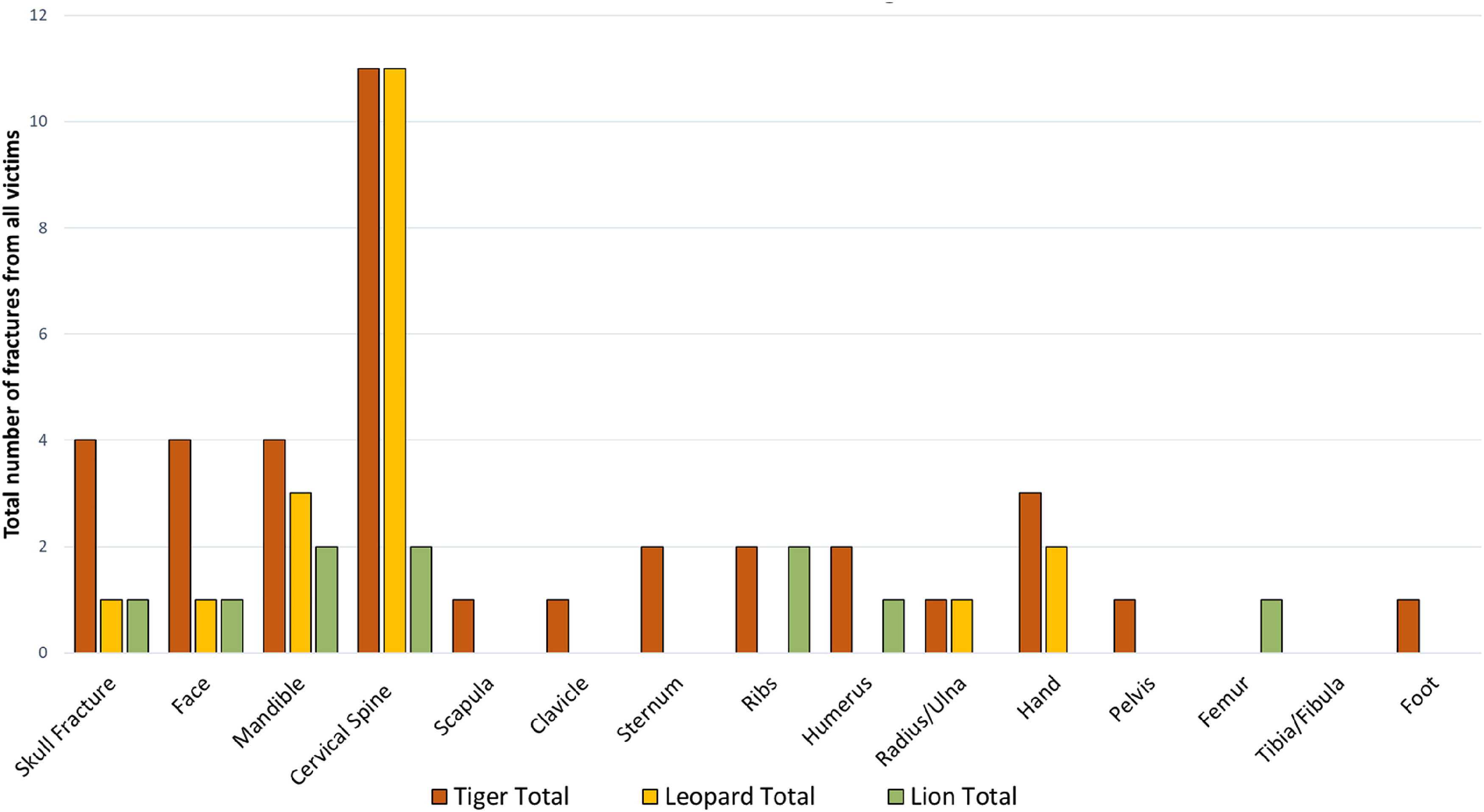
Numbers of pooled fractures from all big cats.
Neck injuries from leopards were distinct in anterior midline-structure involvement and had a higher association with pharyngeal, laryngeal and oesophageal injury (n = 12),6,23,44,53 rarely seen in the other cats (Figure 6).
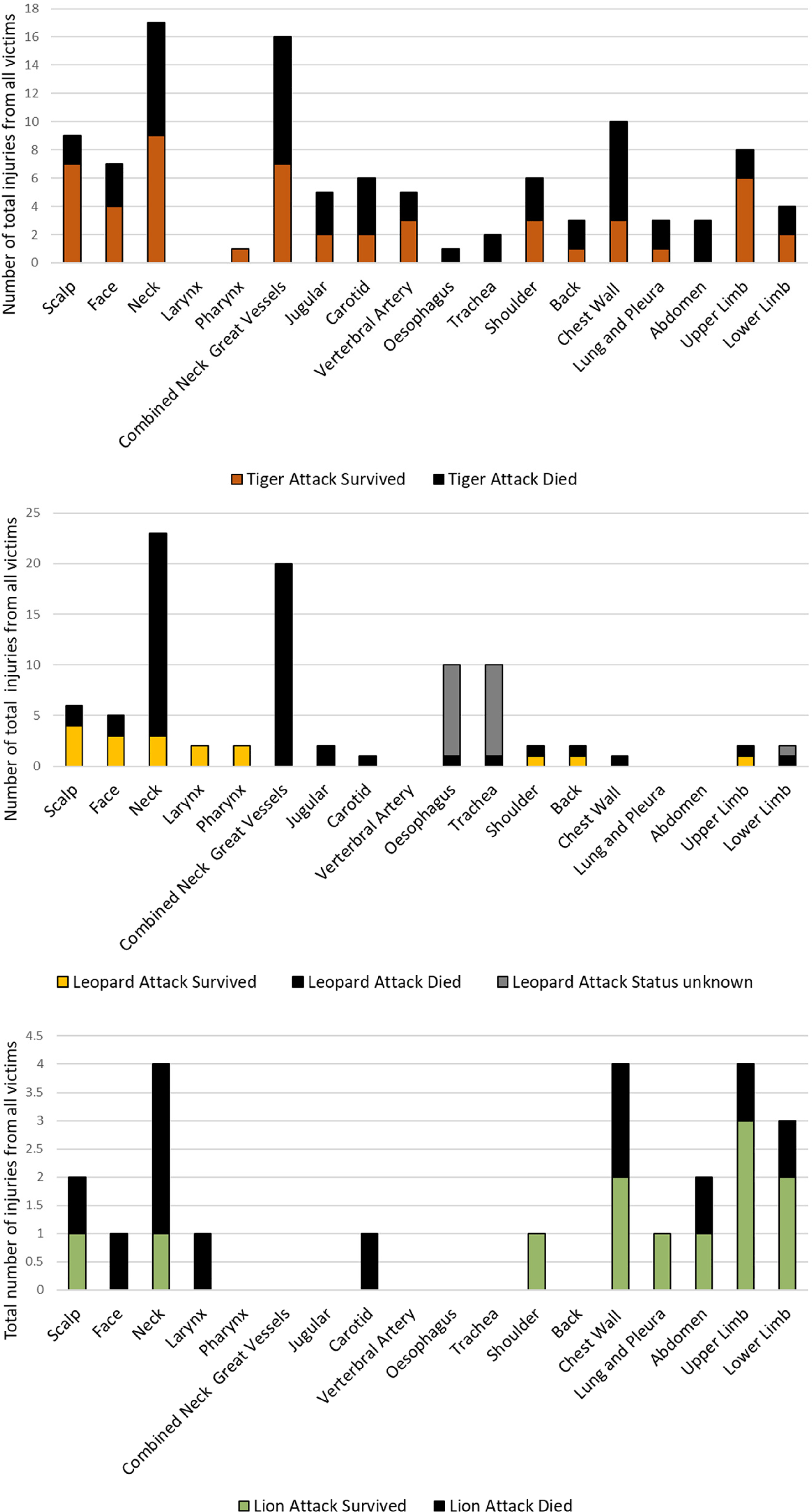
Summary of wounds sustained by victims of each big cat, including survivorship.
Lion injuries included both pride-based and solitary attacks in a wide range of captive and wild settings, including three cases of deliberate engagement with the animal (one person hunting, 40 one ritual fight 22 and one suicide 45 ). Lions engaged in two episodes of post-mortem scavenging including the bowel and genitals16,45 which was not seen in the other cats where limbs were predominantly attacked post-mortem.44,48
Paediatric and captivity analysis
Paediatric injury patterns did not differ from adults, with primary head or neck injury remaining the dominant injury form in 78% of victims.10,21,22,25,27,29,30 The sole paediatric fatality was due to polytrauma from a leopard in a 2-year-old female with major skull and neck wounds. 29
Head and neck also remained the most injured region irrespective of location or captivity (wild 56%, captive 73%). Captive settings introduced unusual injury patterns in the form of the isolated mauling of limbs placed through cage bars28,38 and the participation of multiple tigers, who typically hunt alone, in an attack (n = 3).33,36,42
Of the 83 cases where the setting was clear, deaths in the wild group (n = 22, 53%) were slightly commoner than in the captive group (n = 11, 46%); however, 17 of the wild deaths were from a low detail case series and further commentary was unfeasible. 23
Of the recorded times to the hospital, the median time in the wild group was long at 18 h (range 2–96 h) versus a median time of 5.5 h (range 0.16–7.5 h) in the captive group.
Discussion
This study demonstrated attacks by big cats are typified by open cervical spine fractures, exsanguinating jugular-carotid injury and complex soft tissue neck wounds caused by bites; in survivors, this produced infection, cerebrovascular pathology and occult injury. The soft tissue and bony injury patterns seen in this study correlate well with known large felid anatomy and physiology surrounding their canines, claws and hunting techniques.
The teeth of big cats can apply high bite forces to bone (up to 2152 N 54 ) causing compound fractures. 48 Additionally, tiger canines can reach 7 cm in diameter and 9 cm in length 19 with inter-canine distances of 4–6.8 cm17,29 recorded in this study for leopards, and 7–9 cm for tigers.19,48 This explains the location of the large, paired bite wounds at the inferior and superior extremes of the neck seen in this review. These anatomical features combined with canine proprioception, a physiological trait allowing them to target intervertebral spaces with their teeth,17,43 accounts for the bony, ligamentous and spinal cord injuries seen.
The claws of big cats, reaching lengths of 10 cm, 18 are less rounded and more blade-shaped than the canines and inflict deeply penetrating yet appearing superficial incisional wounds. 18 Carrying these claws are the muscular paws and forelimbs, and combined, can inflict serious visceral and orthopaedic injury with little outward sign.18,35,36 Therefore, all wounds, whether from claws or canines should be evaluated individually to avoid missing serious and treatable pathology.
The high survivorship despite extensive neck wounds in 11 cases5,6,9,10,21,22,30,42,47,49,53 may be due to the sparing of the great neck vessels, of which no surviving patients had penetrating injuries. Cervical spine fracture was still common in these surviving patients (n = 5)5,22,42,47,49 and so even superficial neck wounds should raise suspicion of occult spinal injury.5,54
The greater number of fractures outside of the neck and head region seen in lions and tigers is likely due to their preferred hunting method of knocking large prey to the floor with their body weight,16,18,34 which is > 200 kg for adult male Siberian (Amur) tigers, 26 a pattern not seen in leopards who weighed substantially less in this review (maximally 72 kg 17 ). Leopard attacks however displayed a preponderance of anterior midline structures injury of the neck, which may be due to their natural targeting of anterior structures such as the carotid sheath. 17
Notable was the lack of haemostasis in 11 cases, where bleeding persisted for up to 2 days, mostly from capillary ooze, which may be explained by the degree of associated crush injury. 49 This is an important haemodynamic consideration for those delayed in seeking healthcare, which is likely in the rural locations these attacks occur. 55 The reasons for these time delays to attend a treatment facility in wild cases were not well documented, although the event was often remote from definitive facilities6,21 (up to 30 miles 9 ) and in areas with poor access to transport.9,22 Delays to definitive care also existed in high-income countries with transfers from local hospitals to specialist centres,20,22 highlighting the need to recognise the complexity of these injuries at the scene.
Infection was responsible for 80% of in-patient deaths and addressing infection should form part of the holistic treatment for those surviving to hospital. The polymicrobial nature of these infections fit recorded examples from big cat bites, 39 who are prone to impart tetanus, rabies 23 and species-specific pathogens such as P. multocida. 26 The high survivorship seen in paediatrics may be due to the child either being rescued10,27,30 or the attack itself is short,22,28 preventing further injury. In paediatric cases, the animal frequently had to be moved, killed, or distracted before victims could be attended too.10,18,19,27,43,47,51,52
Thus, these injuries occur in remote locations with on-scene threats from the animal, and appropriate trauma services are usually located an average of 126 min 56 by road from wildlife reserve entrances. Given the primary mode of death is exsanguination, this introduces time and hazard barriers to key medical interventions. These attacks, therefore, generate public-health needs surrounding trauma care infrastructure, which has not followed the human population into these remote regions. 6
There was little difference in the resulting anatomical injury pattern regardless of captivity status or population characteristics. These are non-domesticated animals, and despite being held in captivity they appeared to instinctually attack as though in the wild,17,35 aiming for the neck.
An apparent gap existed between the high number of recorded attacks globally, and the documented attacks available for review, of which only 42 studies were found. This bias is likely multi-factorial due to the rurality of the exposure, reporting to local authorities, 7 lack of reporting by local authorities3,7 and the availability 57 and affordability58–60 of health services in habitat countries. Collectively the challenge to human–wildlife conflict within the scope of human injury not only lies in the medical complexity of these injuries but the health-inequity relating to trauma care in those areas most affected by animal-related incidents.
Limitations
Habitat countries are non-English primary language regions highlighting the language restriction as an inherent flaw in researching regional topics without local stakeholders, which other researchers have attempted to address. 61
Publication bias from a selection of high-interest cases was identified in high-income countries; only nine cases were included from the United States when it is recorded that up to nine attacks per year from captive tigers may occur. 62
The quality varied in all included papers with a heterogeneous final data set in methodology, population and exposure. The inclusion of the large case series by Nabi et al. 23 describing leopard attacks as a group rather than individual cases may have introduced reporting bias, especially surrounding the finding of oesophageal and pharyngeal injury where the survivorship was not known.
Conclusion
This review demonstrates a clear pattern of injury inflicted by big cats, involving complex bony, neurovascular and soft tissue wounds to the neck. These were survivable if patients made it to the hospital. If occurring, fatality did so at the scene and was due to exsanguination and central nervous system injury, highlighting a public health and pre-hospital care opportunity for improved outcomes.
Further research should be founded in the form of a dedicated, species-specific, big cat study including government and community stakeholders to facilitate complete and consecutive inclusion, and precise case details.
Footnotes
Acknowledgements
We would like to thank Jacqueline Rappoport for their kind guidance on the initial formatting of this project. I would like to thank all those organisations and experts around the world who replied to the authors request for information without whom this review would not have been possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Provenance and peer review - Not commissioned, externally peer reviewed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for this article because it is a systematic review of previously published material.
Informed consent
Informed consent was not sought for this article because it is a systematic review of previously published material.
Trial registration
Not applicable - this article is not a trial.
Contributorship
JK was the primary author and reviewer. JLT was the secondary reviewer, provided veterinarian expertise and contributed significantly to the authorship. CT assisted significantly in the authorship and provided extensive expert guidance on the topics of this review.
Supplemental material
Supplemental material for this article is available online.
Correction (February 2024):
This article has been updated to move the Appendices to Supplemental Material since its original publication