
Abstract
Introduction
Frailty is a known risk factor for falls and subsequent fractures and is linked to greater hospitalisation, morbidity, and mortality in various areas of medicine. A 2017 Trauma Audit and Research Network (TARN) report identified that further research was needed to determine the effect of frailty on outcomes in trauma patients. The UK Best Practice Tariff currently awards a financial incentive for frailty scoring for all patients sustaining major trauma who are managed at Major Trauma Centres (MTCs). However, this currently does not extend to Trauma Units (TUs) or to patients without major trauma. This retrospective cohort study sought to investigate whether frailty also has a significant effect on outcomes in patients presenting with fragility fractures presenting to trauma units without major trauma.
Methods
Notes from all patients aged ≥65 admitted to Gloucestershire Royal Hospital in 2019 with any fragility fracture were reviewed retrospectively. Age, injury, length of stay, and mortality were recorded. A Clinical Frailty Score (CFS) was assigned retrospectively using the Rockwood Clinical Frailty Scale.
Results
Eight hundred sixty patients were reviewed (male:female 258:602, mean age 83 ± 8.2). Each consecutive stepwise increase in CFS was independently associated with an average cumulative increase in mortality rate at 30-day and 1 year (OR 1.55 and 1.58 respectively, p < 0.001), as well as average cumulative percentage increase in length of stay (OR 1.094, p < 0.001).
Conclusion
Clinical frailty score independently predicts adverse outcome in patients with fragility fractures managed at trauma units. Clinical frailty score could be used to easily identify patients at risk of poorer outcomes and may assist in allocation of limited orthogeriatric resources and future BPT guidelines. Further work should promote recognition of frailty within trauma settings, investigate how additional resources affect outcomes for patients of varying degrees of frailty, and consider multicentre studies relating to frailty-associated outcomes in trauma.
Keywords
Introduction
The British Geriatric Society describes frailty as “a distinctive health state related to the ageing process in which multiple body systems gradually lose their in-built reserves.” 1 Frailty is repeatedly linked to greater hospitalisation, morbidity, and mortality. 1 It is predicted that approximately 10% of people aged over 65 have frailty, a number that is predicted to continue to rise. 2 Frailty is well-recognised as a major risk factor for falls, 3 and indeed, in 2017 the Trauma Audit and Research Network (TARN) reported that falls from a standing height are now the most common cause of major trauma. 4 Fractures sustained from these low energy falls are defined by the World Health Organisation as “fragility fractures”. 5
Frailty has been shown to predict outcomes such as increased mortality, length of hospital stay, and postoperative complications.
2
Furthermore, proactive identification of frailty has been predicted to increase patient-centred care by identifying the most vulnerable patients and implementing preventative strategies accordingly.
6
Several models have been developed to measure frailty.
1
Among the best known is the Rockwood Clinical Frailty Scale (CFS) (Figure 1), a global frailty score ranging from 1 (very fit) to 9 (terminally ill). Praised for its useability and independence,
7
CFS is widely used to predict prognosis and allocate appropriate resources in various fields of medicine, most recently during the COVID-19 outbreak.8,9 Rockwood Clinical Frailty Scale. Clinical frailty scale provides a global frailty score ranging from 1 (very fit) to 9 (terminally ill).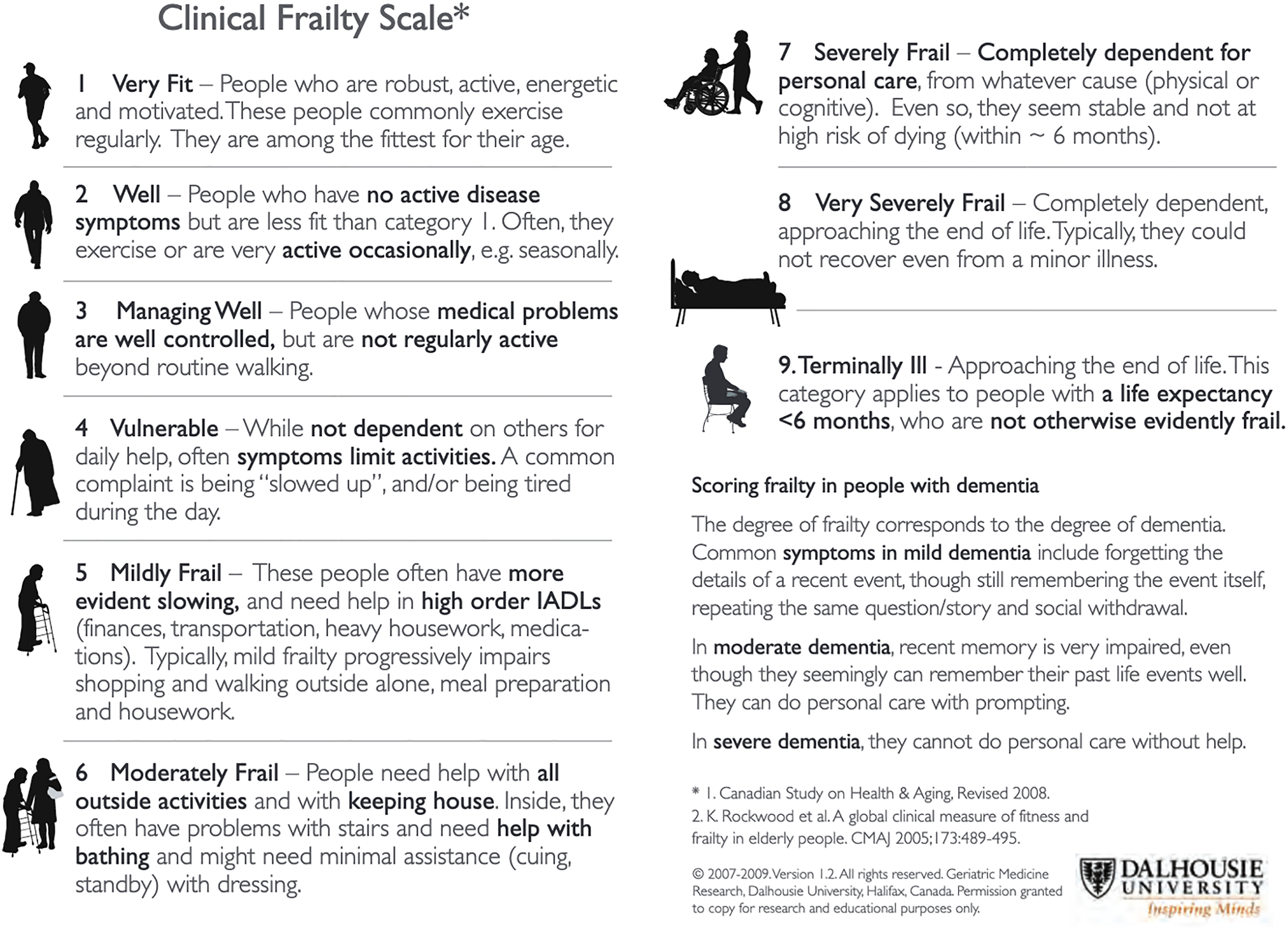
The 2017 TARN report highlighted the risk of under-triage, delayed diagnosis and sub-optimal care in frail patients and recommended that the relationship between age, comorbidity and frailty needed further exploration. 4 Evidence that patients with higher levels of pre-existing frailty sustain typically less severe injuries, but worse outcomes 10 increases the potential that frail patients may be under-recognised on admission.
As a result of this increased recognition, CFS is progressively being recognised in national trauma guidelines as an inclusion criteria indicative of complex medical need, regardless of age. The British Orthopaedic Association Standards for Trauma (BOAST) guidelines for care of the older or frail orthopaedic trauma patient make specific care recommendations for patients with any fragility fracture and CFS 5+, regardless of age. 11 The NHS Improvement Best Practice Tariff (BPT) for major trauma delivers a financial incentive for all patients ≥65 with “Major Trauma” (i.e. an Injury Severity Score (ISS) of >15) who have a CFS recorded on admission. 12
However, there remain outstanding issues and questions. The Major Trauma BPT for recording CFS currently only applies to patients treated at major trauma centres (MTCs) who qualify as “Major Trauma” and existing UK data regarding outcomes in frail trauma patients is derived mainly from MTCs only.10,13 This is despite older people with trauma being more likely treated at trauma units (TUs), 4 and frailer patients more likely to sustain injuries with an ISS of <15. 10 Furthermore, the hip fracture BPT currently remains purely based on age (65+) with no consideration of CFS.
With current BPT guidelines remaining focussed on either injury severity and major trauma centres only or age only, rather than degree of frailty, it is possible that frail trauma patients treated at TUs are not only at risk of under-triage and delayed care, but also losing out on valuable input that may potentially reduce morbidity and improve outcome from their injuries, whilst older but less frail patients could be utilising resources unnecessarily. 14
This retrospective cohort study sought to investigate whether the degree of frailty in patients is a predictor to outcome in patients sustaining fragility fractures managed at a TU, and thus whether frailty deserves greater consideration in future provision of resources and management of these cohort of patients.
Methods
Study design
This was a single-centre, retrospective observational cohort study assessing the impact of pre-existing frailty on patient outcomes in those admitted with trauma to a TU. Ethics approval was not required as all data was routinely collected and held as part of routine care. The project was locally registered (20/103/GHT).
Setting
Gloucestershire Royal Hospital is a district general hospital trauma unit (TU) within the Severn Major Trauma Network. Regionally agreed trauma triage tools identify patients who are appropriate for assessment and admission to the TU, 15 with those requiring specialist intervention (including unstable pelvic fractures) being transferred to the local major trauma centre (MTC). At this TU, adults 65 years of age and older admitted with a hip fracture are seen by an orthogeriatrician within 24 h of admission for a comprehensive geriatric assessment. Other adult trauma patients, regardless of any degree of frailty, routinely receive solely trauma and orthopaedic team input.
Participants
Study participants were enrolled retrospectively. Eligibility included all patients ≥65 years old admitted under the trauma and orthopaedic department between 1 January 2019, and 31 December 2019 with a fragility fracture as defined as per the World Health Organisation (WHO) definition (forces equivalent to a fall from a standing height or less). 5 Both native and periprosthetic fractures, and operatively and non-operatively managed patients were included. Exclusion criteria included open fractures, transfer to or from another TU or MTC, patients discharged from the emergency department, and mechanism of injury other than a fall from standing height or less.
Data collection
All data were collected on the study protocol guidelines by one of three designated study personnel (RB, SG, and MR). A standardised spreadsheet was used for data input.
Eligible patients were identified from the local electronic inpatient trauma database with participant characteristics extracted from existing database input. Participant characteristics recorded included; age, gender, and type of fracture (hip, femur, periprosthetic femoral, vertebral, pelvic, ankle, knee, tibial shaft, upper limb [humerus, forearm, wrist]).
Degree of frailty was measured using the Rockwood CFS and assigned to subjects by manual review of documented social history from admission medical records. All reviewers were familiarised in the use of CFS and reviewed each record alongside this scale. Those with insufficient documentation to undertake a CFS were excluded. Group consensus was gained in cases of uncertainty. Those with CFS 9 were excluded due to the definition of CFS 9 being of terminal illness with a life expectancy of <6 months regardless of degree of frailty, therefore potentially skewing data.
Data regarding period of admission and discharge from inpatient care, as well as time of death (where applicable) were extracted from electronic patient records.
Outcome measures
The primary outcome measure was 30-day mortality (defined as days from injury to date of death of any cause). Secondary outcome measures were 1-year mortality and length of stay (with length of stay defined as date of admission to date of discharge from the acute hospital). Those who did not survive to discharge were excluded from length of stay calculations.
Statistical analysis
Analyses were performed using IBM SPSS Statistics for Windows, version 27 (IBM Corp, Armonk, N.Y., USA). Normality testing was undertaken to determine continuous data distribution. Multivariable logistic regression was used to identify which baseline variables were independently associated with mortality and multivariate linear regression was used to identify whether input factors were independently associated with length of stay. Age was included in the regression model as a known association with adverse outcomes in the study population. Statistical significance was defined at p < 0.05. Those who died prior to discharge were excluded from length-of-stay analysis.
Results
Participants
Of 1051 patients identified from the database, 860 patients over the one-year study period were deemed eligible for mortality analyses and 799 for length of stay analysis (Figure 2). Identification process for eligible patients.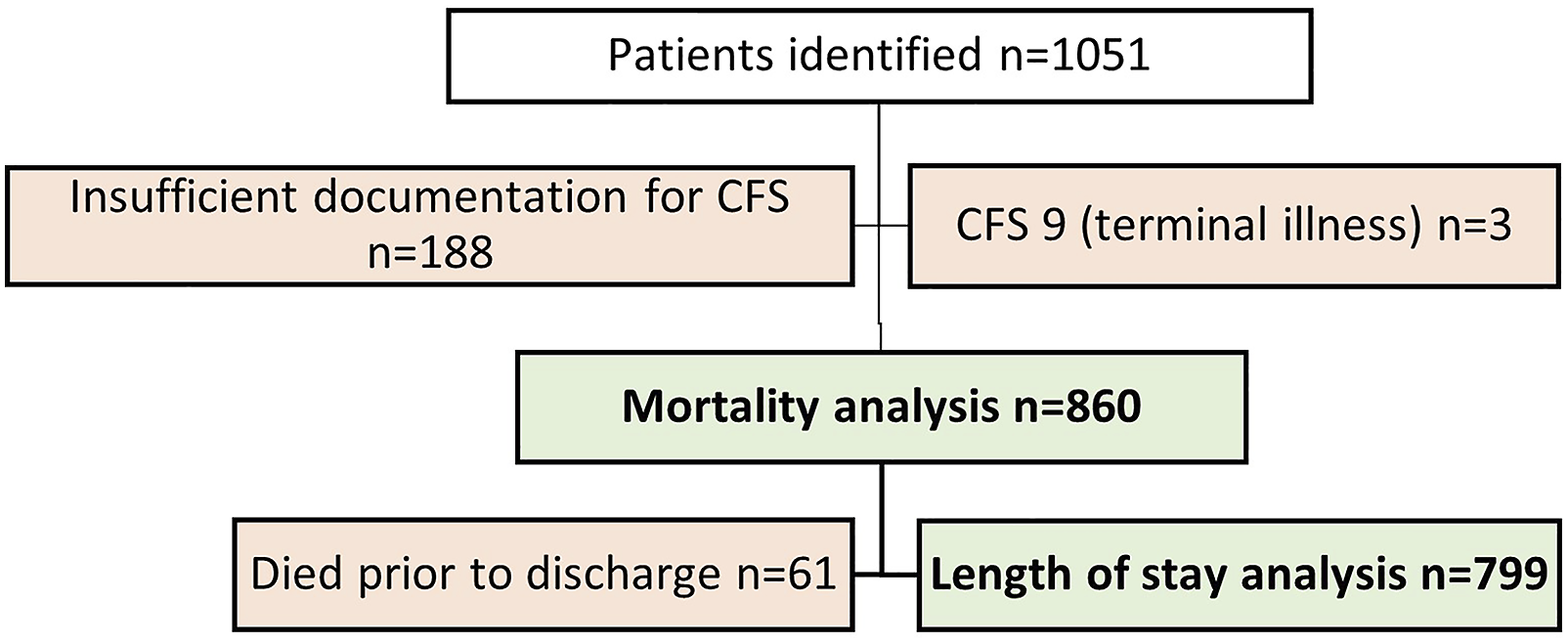
Description of trauma admissions stratified by Clinical Frailty Scale (CFS).

Distribution of clinical frailty score by fracture type.
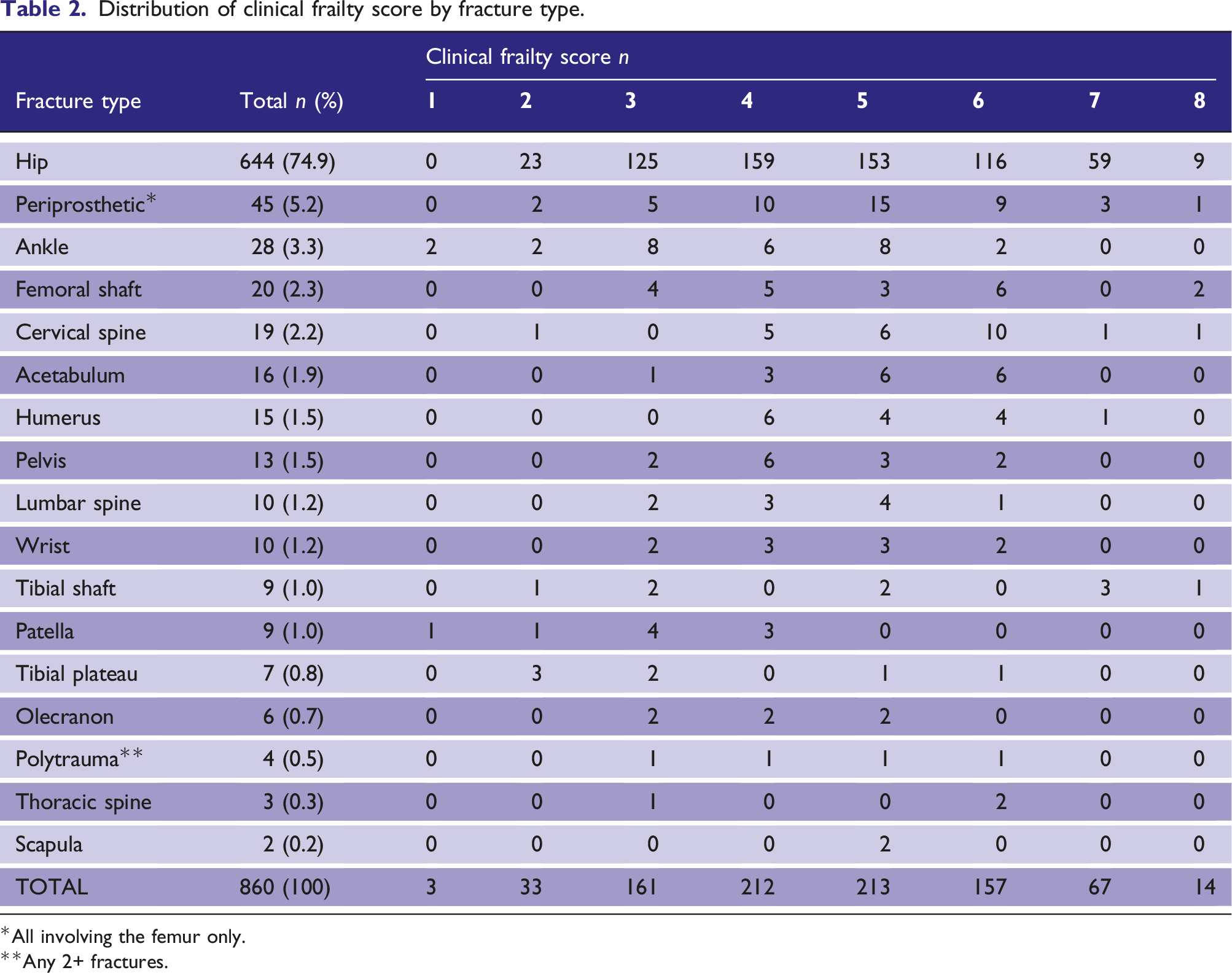
*All involving the femur only.
**Any 2+ fractures.
Outcome data
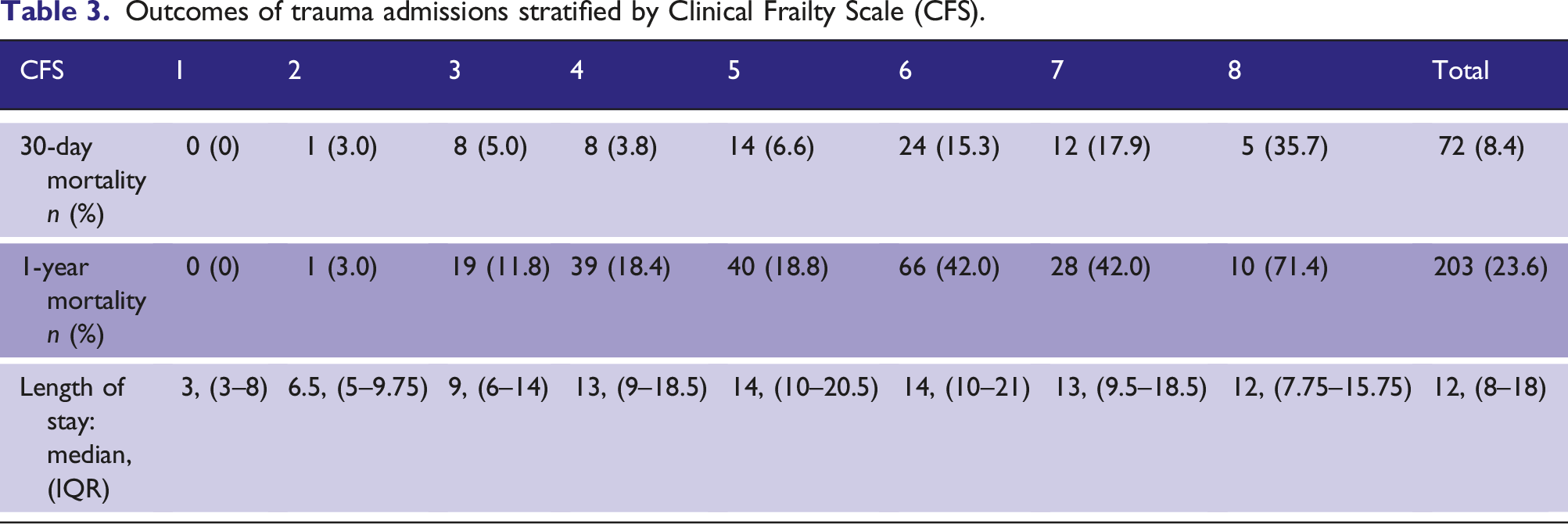
Outcomes of trauma admissions stratified by Clinical Frailty Scale (CFS).
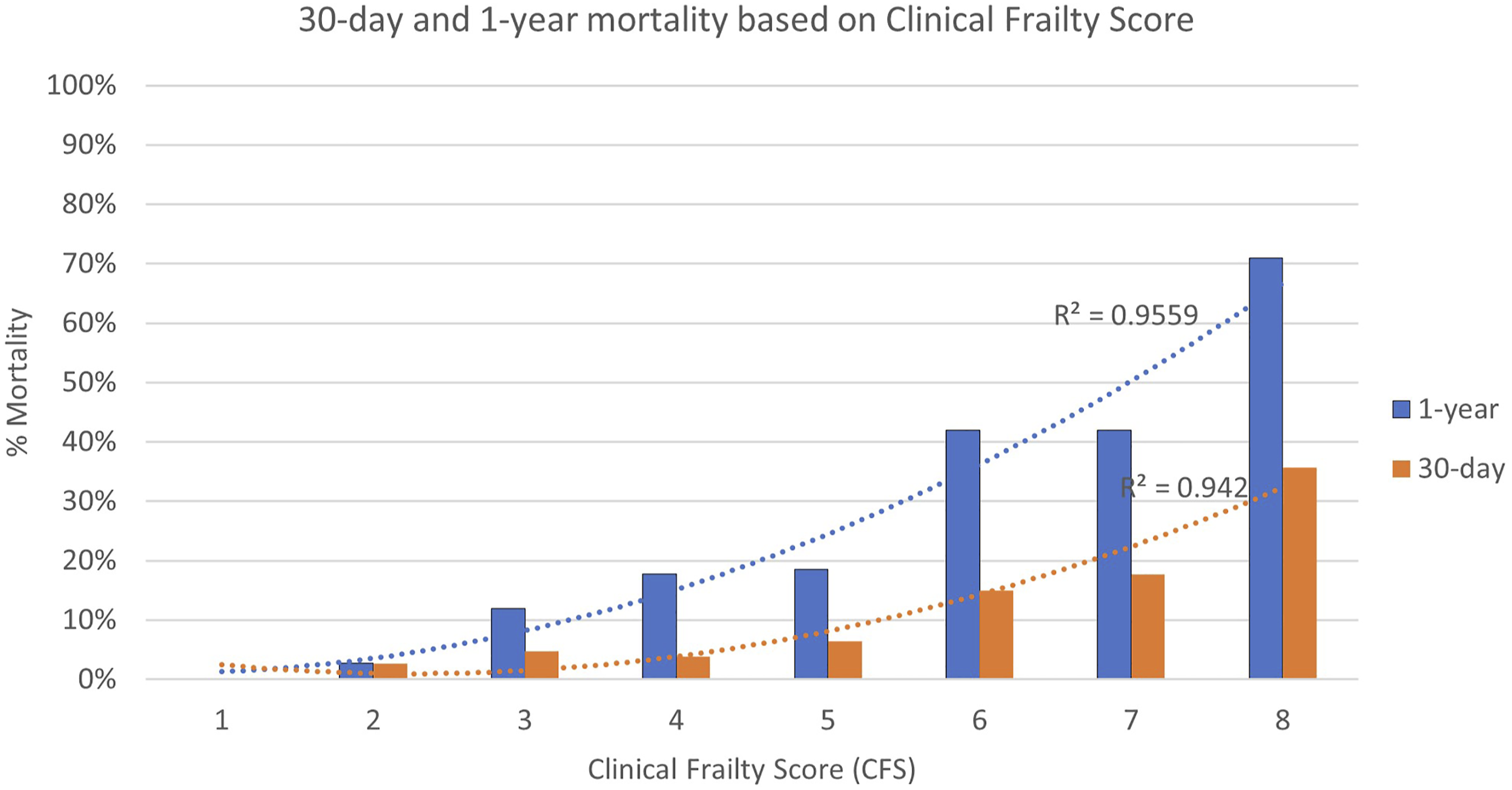
Comparison of 30-day (orange) and one-year (blue) mortality within each Clinical Frailty Score.
Factors associated with 30-day mortality, 1-year mortality, and length of stay
Multivariate analyses for association with 30-day mortality, 1-year mortality, and length of stay.
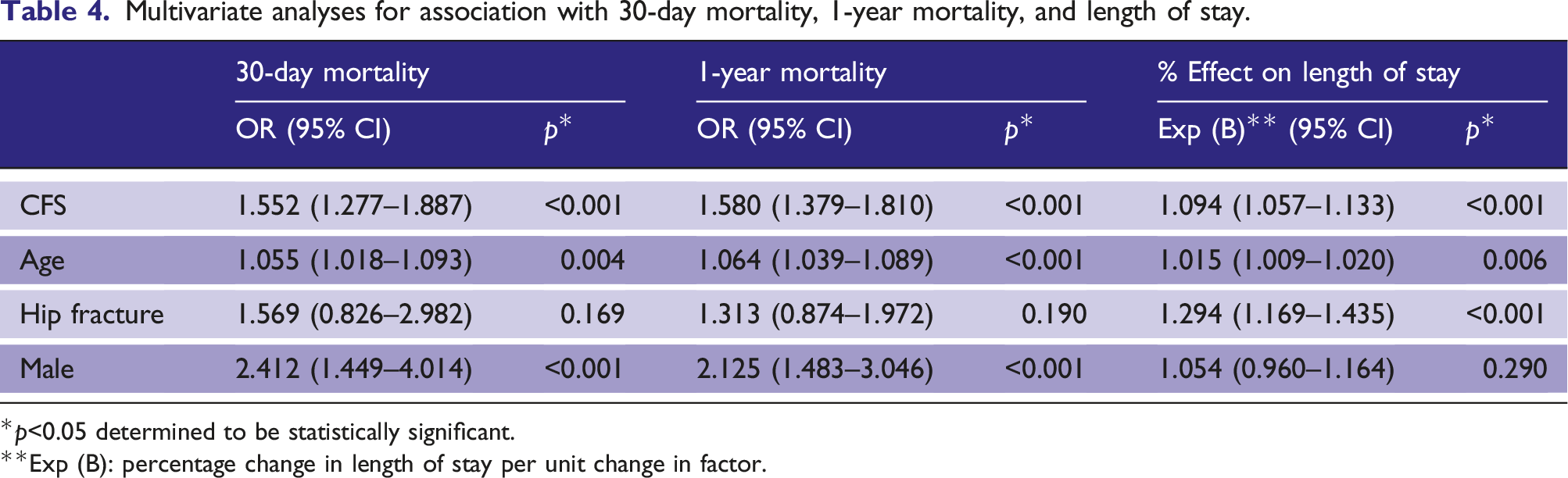
*p<0.05 determined to be statistically significant.
**Exp (B): percentage change in length of stay per unit change in factor.
Increasing age also showed a significant independent association with increased mortality. For every year of life, there was on average a stepwise increase in odds of 30-day and 1-year mortality of 5.5% and 6.4% respectively (OR 1.055, p = 0.004 and OR 1.064, p < 0.001 respectively).
Compared with non-hip fracture injuries, sustaining a hip fracture did not have a significant effect on odds of 30-day mortality (p = 0.169) or 1-year mortality (p = 0.190). However, hip fracture did significantly increase length of stay by 29% compared to non-hip fractures (OR = 1.294, p < 0.001). There were insufficient data to analyse whether sustaining other specific fracture types resulted in higher risk of mortality.
Male gender more than doubled the odds of 30-day and 1-year mortality (OR 2.41 and 2.125, p < 0.001) but had no significant effect on length of stay (p = 0.290).
Discussion
Although the relationship between CFS and outcomes treated at Major Trauma Centres (MTCs) has been previously investigated,10,13 to our knowledge, this is the first study to show the impact of frailty on outcomes within a trauma unit (TU) setting in patients with fragility fractures. Typically, TUs receive high volumes of frail patients with typically less severe injuries (as defined by Injury Severity Score) than those seen at MTCs, with a common mechanism of injury being a “fall from standing height”. Therefore, TUs are in an optimal position to assess the significance of frailty on outcomes in what is now the most common trauma presentation.
Frailty burden
Our data demonstrates wide ranging degrees of frailty with a significant burden of higher frailty scores (CFS 5+) in older patients presenting to TUs. In fact, based on previously described classifications, the burden of moderate and severe frailty (CFS 5–6 and CFS 7–8 respectively) in our study was 43.1% and 9.4% respectively. This significantly exceeds the incidence described in previous medical studies,16,17 but is similar to that seen in other recent UK trauma studies.10,13 This demonstrates both the rapidly increasing burden of frailty as predicted by Wittenberg et al. 18 and the significance of fracture as a marker of frailty.
Mortality
Our data shows that in a TU setting, each stepwise increase in CFS independently increases risk of death at both 30 days and 1 year. Previous studies in MTC settings have also shown this relationship,10,13 although little focus was placed on non-major trauma: Pecheva et al. excluded those with ISS <15, and although Rickard et al.‘s data suggested that greater frailty was seen amongst those with less severe injuries (ISS <15), the data was not further sub-analysed based upon those in this group. Our TU-based study identifies patients within the ISS <15 group and shows that the impact of frailty on mortality extends to patients with injuries not severe enough to require MTC transfer. This is a particularly significant finding, given that current best practice tariffs (BPTs) recognise and reward the documentation of CFS as part of their financial incentive, but currently exclude patients with either ISS <15 or any patient treated in a TU. Our work demonstrates that calculating CFS in patients within these two excluded categories should be valued with equal importance to those treated in MTCs and with ISS >15, given its impact on resources and clinical outcomes.
Although not the focus of our study, the reduced incidence but significantly increased risk of mortality seen in males with fragility fractures reflects results seen in several other studies.13,19 These studies have postulated that fragility fractures and osteoporosis appear to be secondary to other comorbidities in males, whereas they are related to the normal ageing process in females, thus these comorbidities predispose men to both fragility fractures and poorer outcomes.
CFS frailty threshold
In contrast to previous studies who grouped CFS, this study also assessed stepwise changes in outcomes. This revealed that outcomes worsen at every step up in CFS, reaching >10% 30-day mortality and >30% 1-year mortality at CFS 6. Despite this, the current BOAST and TARN inclusion criteria begin at CFS 5. 11 Further research is required to investigate and discuss the most appropriate threshold at which additional medical resources would have the greatest impact and cost-effectiveness when using CFS. However, in agreement with previous studies, 8 this work highlights the value of a comprehensive geriatric assessment (CGA) in targeted patient cohorts, and that CFS could provide a straightforward, user-friendly scoring system to stratify that need based on available resources.
Length of stay
Our TU results showed an average cumulative increase in median length of stay for each stepwise increase in CFS, although the steepest increase was from CFS 1 to 4 with CFS scores above demonstrating wider ranges and median lengths consistently between 12-14 days. Interestingly, an average increase in length of stay with increasing frailty is in agreement with work based at a US-based MTC, 20 but contrasts to results from Rickard et al.‘s MTC, who were conducting a service development delivering CGA-based medical optimisation to older patients sustaining any trauma and reported no significant increase in length of stay based on CFS. 10 These contrasting results support their suggestion that increased medical input may reduce length of stay as indicated by a recent Cochrane review. 21 Further work implementing and assessing the impact of CGA-optimisation in different settings across different CFS grades will demonstrate whether this association is causal. Notably, there was a vast range of lengths of stays across CFS scores. This may suggest that length of stay could be influenced by other factors such as variations in patients’ pre-existing community support. Further research into reasons for delayed discharges amongst this cohort would be of use.
Limitations
Despite its significant findings, the authors appreciate that there are several limitations to this study.
This is a single-centre study and therefore results cannot necessarily be generalised to all other trusts and geographical regions. However, this method of data collection would be easily repeatable in additional centres to demonstrate generalisability. To negate the retrospective nature of data collection, records were carefully excluded if insufficient information was provided to assign a CFS. Regarding inter-observer reliability, although the records were not all reviewed in duplicate, the Rockwood CFS contains clear descriptions of frailty scores, making it highly repeatable, and is widely praised for its ease of use amongst healthcare professionals. 7 Furthermore, group consensus was gained in cases of uncertainty.
This study did not capture all demographic and physiological variables at interplay which may also influence outcomes e.g. ISS, American Society of Anaesthesiologists Physical Status Classification (ASA), comorbidities, and Nottingham Hip Fracture Score (NHFS). However, the authors question the practical use of these variables, regardless of their possible influence. ASA and ISS require specialists to calculate them and have shown significant inter-observer variability even amongst experts.22,23 Therefore, although potentially being influencers of outcome, they are impractical scoring systems in triaging patients upon presentation and so of little use in stratifying pre-operative resource allocation. Comorbidity data, although routinely collected at presentation and easily scored using systems such as Charlson Comorbidity Index (CCI), are limited by failing to consider disease severity. Indeed, the advent of modern-day drugs have revolutionised the management of those living with comorbidities and questions the use of comorbidity alone in stratifying patients. In fact, a recent paper failed to demonstrate independent association with mortality in elderly trauma patients, whilst use of medications was independently associated with reduced mortality. 24 In contrast to this, CFS elegantly captures the functional variability which exists within comorbidities, and is a simple, user-friendly scoring system which can be used at presentation to stratify risk of poor outcome. The NHFS is currently used to stratify those with hip fractures and incorporates functional and demographic measurements. It has shown correlation with CFS in predicting outcomes within the hip fracture population 25 and value in predicting outcome in distal femoral fractures. 26 However, as this score is not routinely collected in those without hip fractures, it has not been included in our analysis. Given our results have demonstrated similar outcomes between those with and without hip fractures, further work should be undertaken to compare CFS and NHFS as predictors of outcomes in fragility fractures outside of the hip fracture population.
Finally, length of stay could be questioned as a useful marker of overall outcome given that it can be mitigated by the availability of community-based resources e.g. community hospital or reablement bed. Nevertheless, awareness of specific groups with typically longer hospital stays aids financial buy-in when discussing allocation of hospital and community resources.
Conclusion
Our study highlights that the importance of CFS in correlation with elderly trauma mortality prediction extends outside of those with major trauma to those with fragility fractures treated at TUs. It adds to evidence that this simple, user-friendly scoring system could help stratify need based on limited geriatric resources, and that BPTs and guidelines should also consider non-major trauma (ISS <15) and TUs.
Future research should investigate how resources affect outcomes for patients of varying severities of frailty. Robust systems should be implemented to record CFS routinely and prospectively for all trauma patients at both MTCs and TUs, and multicentre studies investigating frailty-related outcomes in trauma should be sought.
Footnotes
Acknowledgements
The authors would like to thank Chris Foy, statistician, for assistance in the statistical analysis of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report these cases was obtained from Gloucestershire Research and Development Department (20/103/GHT).
Informed consent
Written informed consent was obtained from a legally authorized representative for anonymised patient information to be published in this article.
Guarantor
RB.
Contributorship
MR, SG, and RB contributed to data collection. RB undertook statistical analysis and wrote the first draft of the manuscript. RB, NP, and AT undertook review and edit of the manuscript. All authors approved the final version of the manuscript.