
Abstract
Introduction
Major trauma centres are increasingly managing a significant injury burden in older patients, with falling downstairs being a prevalent mechanism of injury. Literature evaluating the impact of falls on stairs upon UK trauma networks is limited. Gaining a greater understanding of this may allow for more effective planning of services and improvements in training and education. This study evaluates the impact of falls downstairs on a UK major trauma centre.
Methods
A single centre retrospective service evaluation of local major trauma data over a 3-year period from 01/01/2017 to 31/12/2019. Included were patients who activated a trauma call whose mechanism of injury recorded at the time of admission was a fall downstairs. We excluded patients less than 16 years of age.
Results
There were 4480 major trauma patients who presented in the study period and of these, 860 (19.2%) sustained injuries following a fall downstairs. The most common age group presenting was 70–79 years; younger patients (<60 years) made up 43.3% with the majority (56.7%) being older. All but one patient were managed by a consultant-led trauma team, 6.4% of patients were admitted to critical care and 1% received an urgent operation. The overall mortality rate was 8.5%. Older patients made up 85% of those who died and had nearly four times longer average length of stay than younger patients (9.69 v 2.49 days).
Conclusion
Falls downstairs place a significant burden on the major trauma centre. There is a stark contrast in the use of hospital resources and outcomes between older and younger patients.
Introduction
Preconceptions of major trauma in England from the main stream media suggest the workload consists of severe penetrating trauma within a young, healthy population. Increasingly, however, major trauma networks are managing a significant injury burden in older patients, with falls being the most common causative mechanism and falling downstairs in itself being a prevalent and significant mechanism of injury.1–3 A study from the Netherlands of 5880 patients who presented to hospital following a fall found that over half of those diagnosed with a traumatic brain injury had fallen up or down a flight of stairs. 3 Friedland et al. in the UK confirmed this finding, with stairway falls being a leading cause of fall-related traumatic brain injury 4 and Chatha et al. concluded that older patients are more likely to incur serious injury and younger patients are more likely to be intoxicated. 2
Despite the clear burden, literature evaluating the impact of falls on stairs upon UK trauma networks is limited when compared to that of other higher-velocity mechanisms such as gunshot wounds, stabbings and road traffic collisions. Gaining a greater understanding of this may allow for more effective planning of major trauma services, improvements in training and education and identification of gaps that exist in current practices. This study evaluates the impact of falls downstairs on a UK major trauma centre.
Methods
Aintree University Hospital is part of the Liverpool University Hospitals NHS Foundation Trust and has been the single receiving site for major trauma for Cheshire and Merseyside since 2016. Specialist neurosurgical services are provided by the Walton Centre NHS Foundation Trust which sits adjacent to the Aintree site and connected by a link bridge. In 2019, 1397 major trauma patients presented to the trust and activated a trauma call (Table 1). Patients are triaged as ‘major trauma’ based on the assessment of either the local ambulance service in the pre-hospital setting or the trust upon their arrival to hospital. Patients are initially assessed in the emergency department by an assembled trauma team. Typically, this is consultant-led and made up of clinicians from the emergency department, orthopaedics, general surgeons and anaesthetics with other specialities involved as clinical need dictates. Patients are managed based on the assessment and this varies according to their condition. If patients are admitted, this is typically to the hospitals dedicated major trauma ward, though some patients require an urgent operation (<4h), critical care admission or transfer to the specialist neurological centre at the Walton Centre. Some patients will be admitted for medical need rather than as a result of their injuries. Such patients may be admitted under the hospital medical team. All patients who activate a major trauma call have their details entered onto a local database.
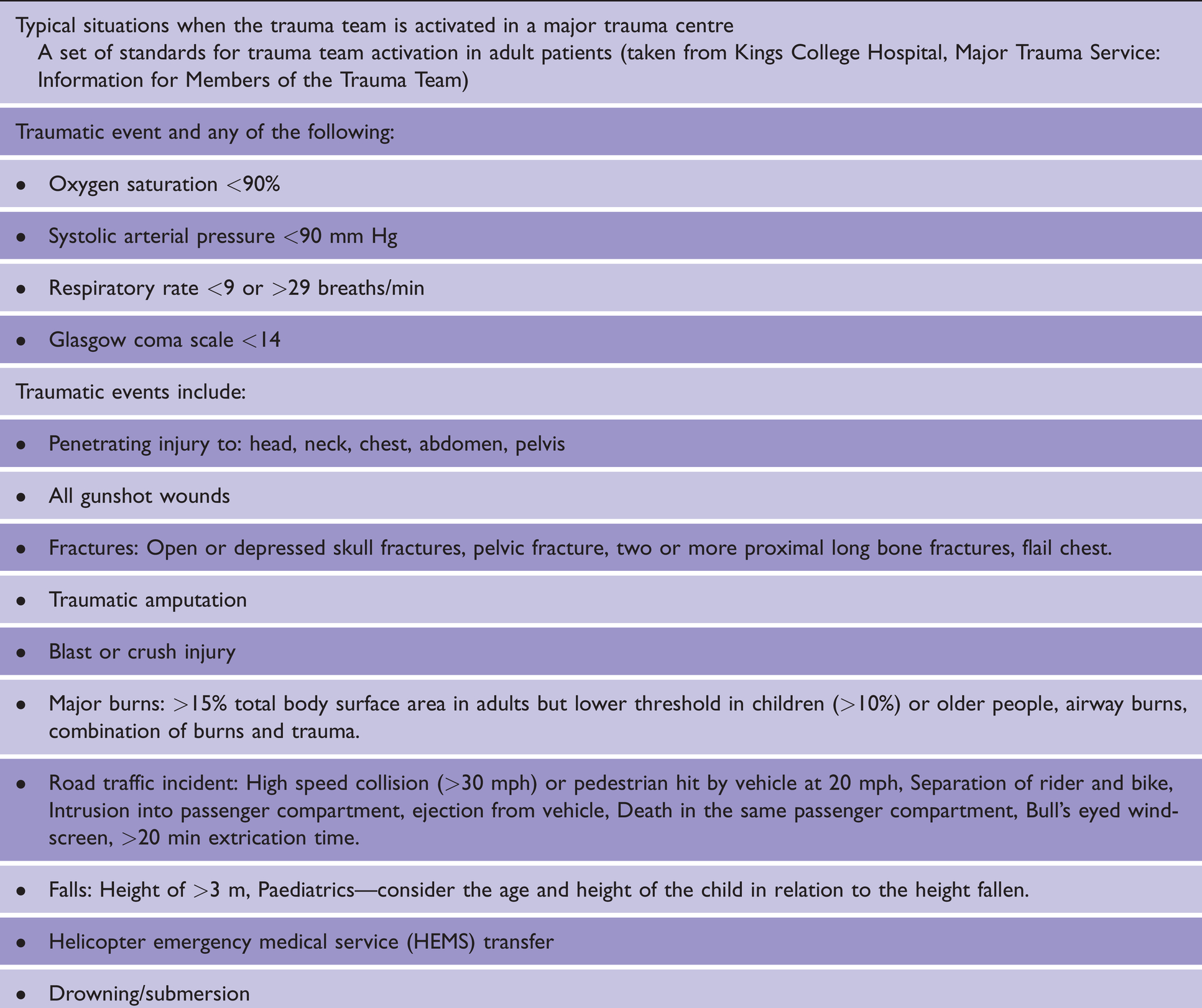
Typical situations where the trauma team is activated in a major trauma centre. 5
Following approval from the Clinical Audit Department a single centre retrospective service evaluation of local major trauma data over a 3-year period from 1 January 2017 to 31 December 2019 was undertaken. The inclusion criterion was that the mechanism of injury recorded at the time of admission was a fall downstairs and patients less than 16 years of age were excluded. Patients were included based on their activation of a trauma call, regardless of whether they met the Trauma Audit and Research Network (TARN) definition of a major trauma patient. Details included were selected from our local database including demographics and information relating to patients’ presentation, investigation, management, discharge and length of stay.
Results
In the three-year study period (2017–2019), 4480 major trauma patients presented to Aintree University Hospital Emergency Department, 860 (19.2%) of which sustained injuries following a fall downstairs; 387 (45%) were male and 473 (55%) were female. There was a wide age distribution with the most common age group presenting being 70–79 years (19.3%) with mean and median ages being 62.2 and 64 years respectively (range 16–101yrs). TARN define older trauma patients as being aged 60 years or older and we adopted this figure when analysing our results. 6 Younger patients (<60 years) made up 43.3% of those presenting, with the majority (56.7%) being older; patients presented to hospital at all times of the day, with the most common time of presentation being between 1800–2359 (30.4%) and the least common 0600–1159 (18.7%).
All patients bar one were cared for by a consultant-led trauma team in the emergency department; 93.3% of patients had a CT scan on presentation to Aintree and 3.5% had had one at a local hospital prior to transfer. Overall, 2.1% patients warranted a Code Red Protocol’ for patients where it is deemed they may require immediate blood products on arrival 5 and a further 3.1% required activation of the hospital’s major haemorrhage protocol. There were 13.8% of patients who were discharged directly from the emergency department, with the majority (86.2%) requiring hospital admission.
Mortality
Only 1.1% of patients required an urgent operation (<4h from admission), over half of which (55.6%) were orthopaedic with neurosurgical, general surgical and interventional radiological procedures accounting for the rest. A third of patients undergoing surgery within 4 hours of admission died within 30 days of their operation. Critical care admission accounted for 6.4% of patients and those aged 70–79 made up both the most common age group and the highest proportion of patients per age group admitted to critical care. A third of patients admitted to critical care died in hospital with these patients making up 26.0% of all patients who died on admission. Of all 860 patients who presented, 73 died, demonstrating an overall mortality in this patient group of 8.5%. One patient under the age of 50 died, whilst the highest mortality was seen in those aged between 90–99 years, with over a quarter of patients in this age group dying (25.8%). The most common age group to die in hospital (41.1%) were aged between 80–89. The mean length of stay of those who died was 6 days though nearly a third of patients died within 1 day and 74.0% of all deaths happened within a week of admission.
Discussion
It is clear that injuries sustained following falls downstairs place a significant burden on the major trauma centre, with nearly 1 in 5 of all major trauma patients presenting with this mechanism. All age groups are affected, and as expected in a major trauma patient cohort, the majority required hospital admission. There is, however, a stark difference in outcomes seen between older and younger patients. Of younger patients (<60 years) who presented following a fall downstairs, 3% died on admission, making up 15% of all those who died, conversely 85% of those who died from a fall downstairs were over 60 years of age with a mortality rate of over 12%. Furthermore, older patients aged 60 years or over had nearly a four times longer average length of stay than younger patients (9.69 v 2.49 days). One explanation for these worse outcomes could be inferred from the results of Chatha et al who identified that older patients were more likely to suffer serious injury from falling downstairs. 2 Equally, it has previously been shown that older age is itself an independent predictor of mortality in elderly trauma. 7 Regardless of the reasoning, what can be deduced from the results found here is that as a cohort, older patients have a greater impact on hospital resources.
Less than 7% of patients required a critical care admission. No patients over the age of 90 years and less than 5% of those aged 80–89 years were admitted to critical care compared to nearly 10% of those aged 60–79 years. This is perhaps to be expected, despite the higher morbidity and mortality caused by their injuries, a proportion of these older patients may have been frail and co-morbid and as such critical care admission could have been deemed unsuitable or futile.
It has been suggested previously that ‘older patients with less reserve are more likely to suffer harm from delays in accessing evidence-based treatment on specialist units’. 5 The lower proportion of elderly patients admitted to critical care could explain why the mortality in all patients was higher than the rate of critical care admission. A more likely reason for this is that nearly a third of those who died did so within one day and thus may have died before critical care admission was possible. Less than one in ten patients were transferred for specialist neurosurgical, neurological or neuro-rehabilitation care. The majority were transferred within 24 hours of admission, though less than 4% of these patients had an urgent neurosurgical operation (in both cases a decompressive craniotomy). Patients aged 80 years or older made up less than 6% of those transferred to the tertiary neurosciences centre. It is not clear from the data whether or not this is due to a higher incidence of head injuries, though it has previously been identified that younger patients are more likely to suffer a traumatic brain injury following a fall downstairs. 2 On the other hand, this could represent a further example of the systemic ageism discussed in the TARN report on Major Trauma in Elderly People. 5
Studies have shown that elderly patients are at risk of being undertriaged, with Amoako and colleagues identifying advanced aged as being an independent factor associated with failure to appropriately transport injured patients to a trauma centre. 8 If this were to be true in our regional network population, the number of older patients requiring major trauma care following a fall downstairs could be understated in the data presented here. Consequently, as triage systems are refined, the proportion of elderly patients, and by association the burden of their increased morbidity and mortality, may rise.
Limitations
As a single centre study, the patients included here are from a particular geographical area, assessed and managed in one NHS major trauma centre. Collectively, these results could represent this patient group more widely though the possibility of regional discrepancies should be accounted for. Equally, demographic data beyond sex and age have not been included in the data set, meaning comment cannot be passed based on differences in race and socioeconomic status amongst other parameters. Injury pattern and severity has not been identified here. While this is purposeful given the aim being to evaluate the impact of these patients as a group on major trauma services, caution should be used if assuming severity or difference of injury based on resource use.
The influence of age on outcomes identified here has been discussed at length. Increasingly though, clinical frailty scores (CFS) are being utilised to determine an individuals’ vulnerability to adverse outcomes independent of age. 9 Unfortunately, CFS’s were not documented in the primary data collection sources used here. Linking them to the outcomes identified here could help to determine the effect of frailty on the impact that these patients have on the major trauma centre.
Conclusions
Patients who present having sustained injuries following a fall downstairs place a significant burden on the major trauma centre, making up nearly a fifth of all major trauma patients presenting to the Emergency Department. There is a stark contrast in the use of hospital resources and outcomes between older and younger patients. On average, older patients had nearly four times longer lengths of stay than younger patients and despite making up less than 60% of those who presented, equated to 85% of patients who died on admission. Notwithstanding this, patients in extreme older age groups were admitted to critical care and transferred for specialist neurosurgical management in lower proportions than younger patients.
It is clear that certain resources provided as a regional major trauma centre are being delivered to a significant proportion of patients. Almost all patients had a CT scan as part of their injury assessment and indeed every patient bar one received consultant-led care in the Emergency Department. Further studies are warranted to further investigate individual factors and how they impact on hospital services. This may allow for more efficient delivery of resources and perhaps greater equity in care for all patient groups.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Following guidance from the Medical Research Council and the NHS Health Research Authority, this study was not considered research by the NHS and therefore ethical approval was not required.
Informed consent
Informed consent was not required as this study was a retrospective service review that did not require ethical approval.
Guarantor
SM.
Contributorship
JC and SM conceived and designed the study. JC and SM analysed the data. JC wrote the first draft of the manuscript. All authors reviewed and approved the final version of the manuscript. SM provided senior supervision to the project.
Acknowledgements
None.
Provenance and peer review
Not commissioned, externally peer reviewed.