
Abstract
Introduction
There has been little systematic study of the epidemiology of traumatic spinal cord injury (TSCI) in Nepal, South-East Asia, and low- and middle-income countries (LMICs) in general. One third of the global morbidity and mortality due to injuries is concentrated in South-East Asia. We need to better understand the circumstances leading to TSCI if we are to make progress with prevention.
Method
The Spinal Injury Rehabilitation Centre (SIRC) in Nepal systemically collected prospective data describing people with TSCI admitted between September 2015 and August 2016. Descriptive analyses of variables yielded demographic, aetiological and clinical descriptors of this cohort. Cross-tabulations were used to explore the associations between variables.
Results
Of 184 admissions over one year, males were admitted to SIRC almost 2.3 times more often than females. Young adults (21–30 years) were the largest age group (34%). The majority of TSCI resulted in paraplegia (67%) and was complete in nearly half (49%). Falls caused the majority of TSCI (69%), and falls from trees were the most common. Road traffic injuries (RTIs) were the second leading cause (29%); the majority involved two- or three-wheeled motorised vehicles and patients were most commonly driving.
Conclusion
Falls were the leading cause of TSCI across both genders and all age groups, followed by RTIs, which occurred most often in young adults and men. Injury surveillance and further research would provide a greater understanding of the pattern of TSCI and enable progress in TSCI prevention and rehabilitation.
Introduction
One third of the global morbidity and mortality due to injuries is concentrated in the South-East Asia Region (SEAR). 1 Meanwhile, research into traumatic spinal cord injury (TSCI) focuses on high-income countries (HICs), with limited applicability to low- and middle-income countries (LMICs). TSCI represents one of the most extreme forms of survivable injuries, 2 and one of the largest contributors to disability-adjusted life years, 3 with substantial functional impact on an individual’s life. The overall incidence of TSCI is increasing, 4 and this increase is concentrated in LMICs. 5
Understanding the epidemiology of TSCI is essential to identify vulnerable groups and inform interventions to reduce its incidence. Worldwide, significantly more men suffer from TSCI than women, with the largest group being men aged 30–40 years. 4 The causes of TSCI vary in different regions of the world. Road traffic injuries (RTIs) are the main cause of TSCI in HICs, particularly from crashes involving four-wheeled vehicles. In contrast, injuries sustained while driving two-wheeled vehicles predominate in LMICs, including those across South-East Asia. Falls are the leading cause of TSCI in LMICs, 6 with falls from rooftops and trees the most common aetiology in Southern Asia, 7 and falls from trees reported as the largest cause of TSCI in Nepal.8–10 Nepal also experiences earthquakes leading to TSCI. 11 In Nepal, TSCI has a significant impact on an individual’s quality of life, with over half of people living with TSCI having below average quality of life scores. 12 Considering the economic and social burdens arising from TSCI, such as healthcare expenses, loss of income and disability, there is a distinct lack of attention and resources allocated to it. 13
The Spinal Injury Rehabilitation Centre (SIRC) is a national referral centre of excellence committed to improving outcomes and raising awareness of TSCI. SIRC commenced systematic prospective TSCI data collection in 2015. Our objectives were to describe the demographics, antecedent causes, and associations between these factors, using observational data from a representative patient cohort presenting to SIRC.
Methods
Setting
SIRC is a non-profit organisation providing specialized, multidisciplinary rehabilitation to individuals with TSCI. It is the largest centre of its kind in Nepal and is the primary site of TSCI rehabilitation referral from tertiary care centres throughout the country. It receives patients from every district of Nepal; the majority of patients come from the densely populated central region in which the centre is located. Links with a government-funded hospital, coupled with the centre’s provision of financial assistance for patients with limited resources, result in a high proportion of patients from very poor socioeconomic backgrounds.
Design
A descriptive epidemiological study was conducted on a one-year cohort of patients admitted to SIRC. The minimum dataset was collected by SIRC, using fields described in the International SCI Core Dataset and Minimal Injury/Safety Dataset. The data elements were developed by the International Spinal Cord Society (ISCoS). 14 Data were recorded using a collection form provided by ISCoS as part of their pilot study within the Asian Spinal Cord Network (ASCoN) known as ISCoS Database ASCON Pilot Project (IDAPP). 15 The form was read out to patients and filled out by a healthcare professional using information provided by the patient and information from the patient’s clinical records. This study analysed a one-year cohort (September 2015–August 2016) extracted from the dataset. Data collection forms and patient’s clinical records were securely stored on site and were accessible for reference. Inclusion criteria for enrolment in the study were that the SCI must be traumatic and initially classified with the American Spinal Injury Association (ASIA)’s impairment scale of A–D, 16 and informed consent from the patient must have been obtained for their data to be included in the dataset. Patients were only eligible for enrolment once; readmissions during the study period were not enrolled a second time.
Ethical approval and oversight was provided by the Nepal Health Research Council for the analysis of data collected during the study period.
Selected variables and assessment tools
Collected data included patient demographics, type of vertebral injury, and International Standards for Neurological Classification of Spinal Cord injury (ISNCSCI) examination, as well as associated injuries according to the ISCoS definitions. 14 Both injury aetiology (such as sports, assault, transport, and falls, and treatment details (time from injury to hospital admission, spinal surgery (presence/absence), and length of stay at SIRC) were collected.
ISNCSCI is the internationally accepted gold standard to determine the neurological level of injury and completeness of TSCI
16
(see supplementary material online for example form). It is made up of two components: Neurological level of injury: most caudal segment of the spinal cord that is intact. ASIA impairment scale (AIS): completeness of injury, scored from A-E (A = complete, B = sensory incomplete, C/D = motor incomplete, E = normal).
Analysis
Statistical analyses of the cases were conducted using SPSS (version 25). 17 Descriptive analyses were carried out for each of the selected variables, with the proportion of missing data enumerated. Tables state the total number of cases with data included in the analysis for each variable. Graphical representations were produced and the results interpreted. Associations between variables were explored using cross-tabulations.
Results
Demographics
Between September 2015 and August 2016, 236 patients were admitted to SIRC. Of these, 52 patients did not meet the inclusion criteria and were excluded, most commonly for having a non-traumatic SCI (e.g. due to tuberculosis, tumour, transverse myelitis, etc.), a repeat admission, or a non-SCI admission (stroke, traumatic brain injury, orthopaedic). The remaining 184 patients formed the cohort studied. Participants ranged from 8 to 78 years old, with an average age of 36 (SD: 14.366) and a median age of 33.5 (IQR: 23). The largest age group of patients was 21–30 years (33.7%) (Figure 1); most cases were male (128, 69.6%) producing a male to female ratio of 2.29:1. Age distribution.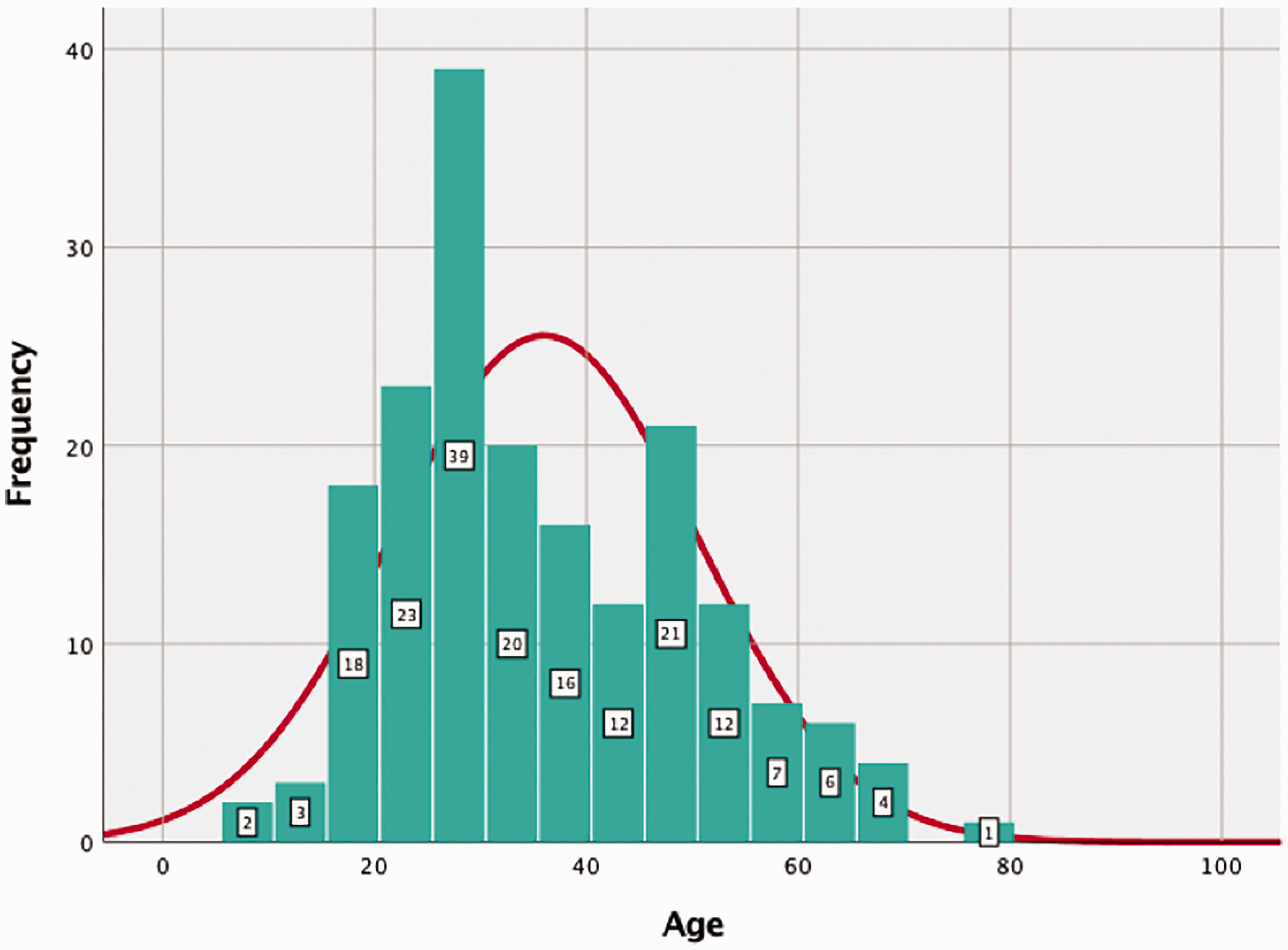
The majority of patients had a vertebral injury alongside their TSCI (160/178; 89.9%), and few (24/165; 14.5%) had an additional associated injury; most patients (144/182; 79.1%) were managed surgically. According to the INSCSI exam,
16
nearly half (48.9%) of the patients had complete (AIS A) injuries on admission, with 13.6% having AIS B, 19.9% AIS C, and 17.6% had AIS D. The majority of cases (123/184; 66.8%) sustained paraplegia (level of injury below T1). Most injuries were lower thoracic, most commonly T10-T11 (30% of all TSCI), and of the cases of tetraplegia (61/184; 33.2%), C3 was the most common level of injury (Figure 2). Level of TSCI identified by neurological examination on admission.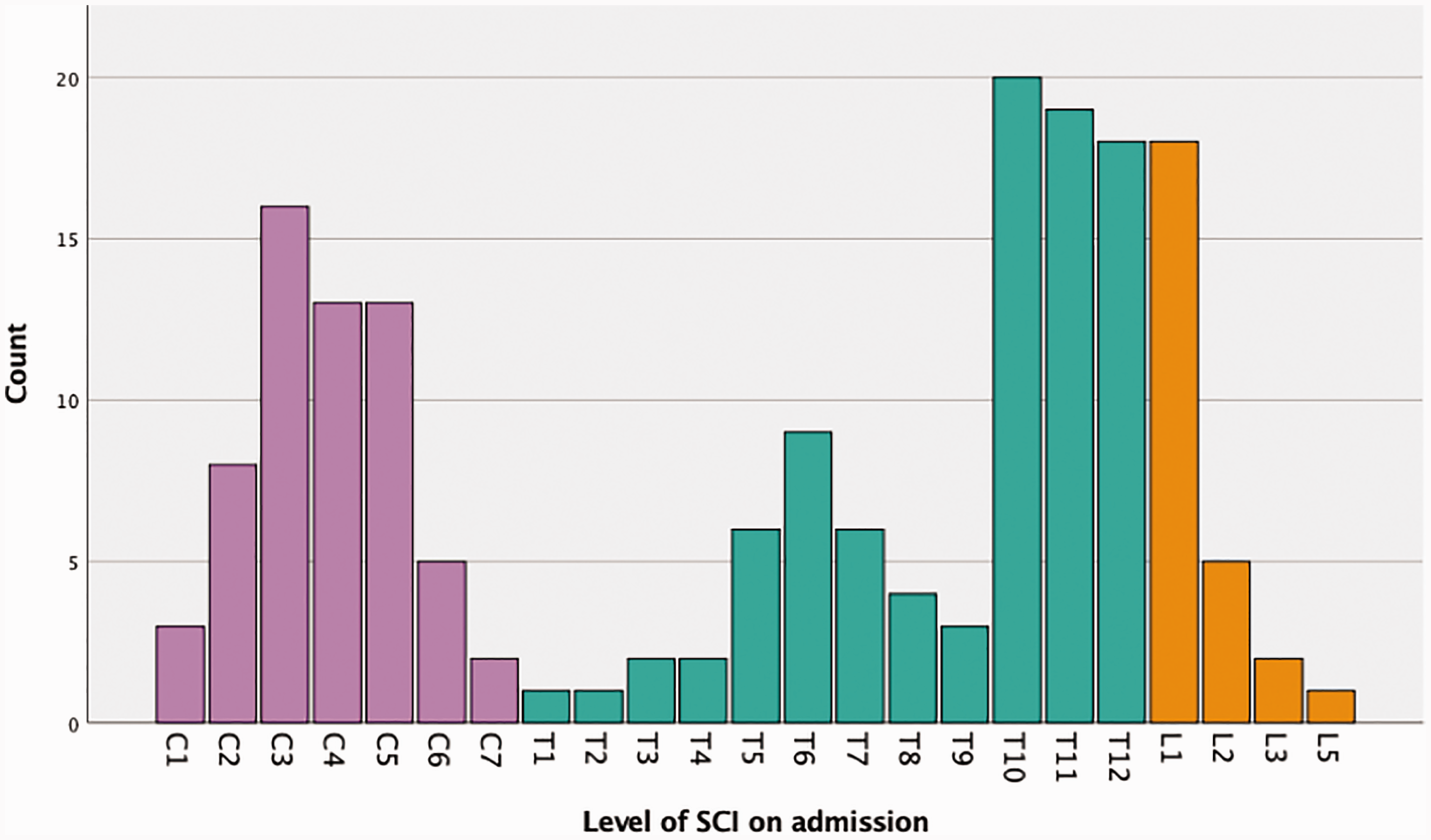
Almost two thirds of patients (128/184; 69.6%) were admitted to a hospital within 24 h of injury, 12.5% (23/184) in less than a week (1–6 days), 2.7% (5/184) in under a month (7–28 days), 4.9% (9/184) in under a year (29 days–a year), and 9.2% (19/184) in a year or more. Patients’ duration of stay at SIRC ranged from 1 to 200 days, with an average stay of 73 days; most patients (N = 158, 85.9%) spent less than 120 days in hospital (Figure 3). Length of stay at SIRC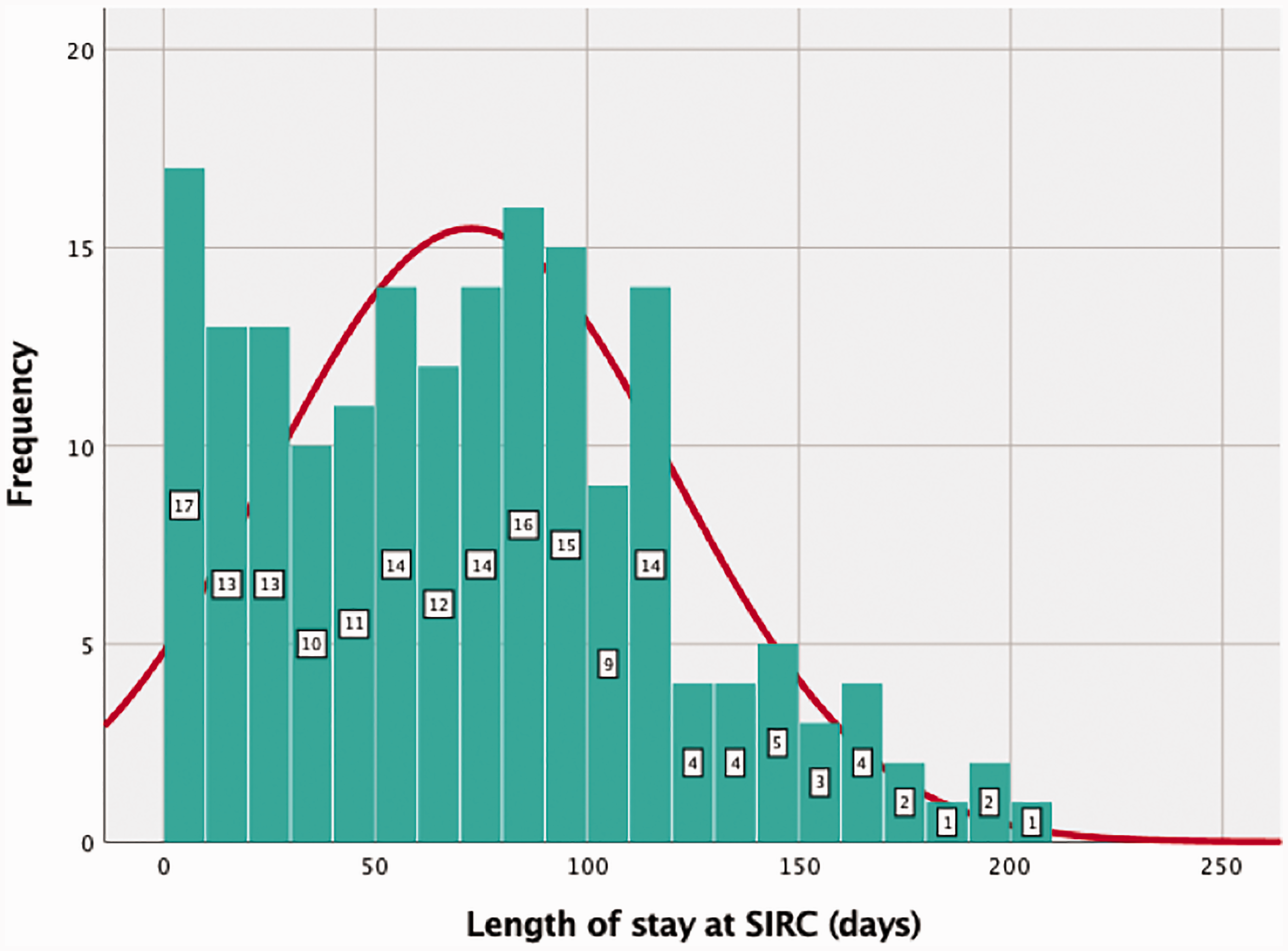
Aetiology of injury
The commonest cause of TSCI was falls (69.6% of cases), followed by RTIs (Figure 4); nearly half of the falls (47.1%) were from a tree, one third (33.6%) from a building or structure, and 10.1% fell from a cliff or mountainside. Out of the RTIs, 40.7% involved motorised two- or three-wheeled vehicles, 29.6% transport vehicles with four or more wheels, 14.8% a bicycle, and 3.7% an animal-drawn vehicle – nearly half of patients (48.1%) were driving during the RTI, were passengers in the vehicle in 25.9%, and pedestrians in 11.1%. Aetiology of injury.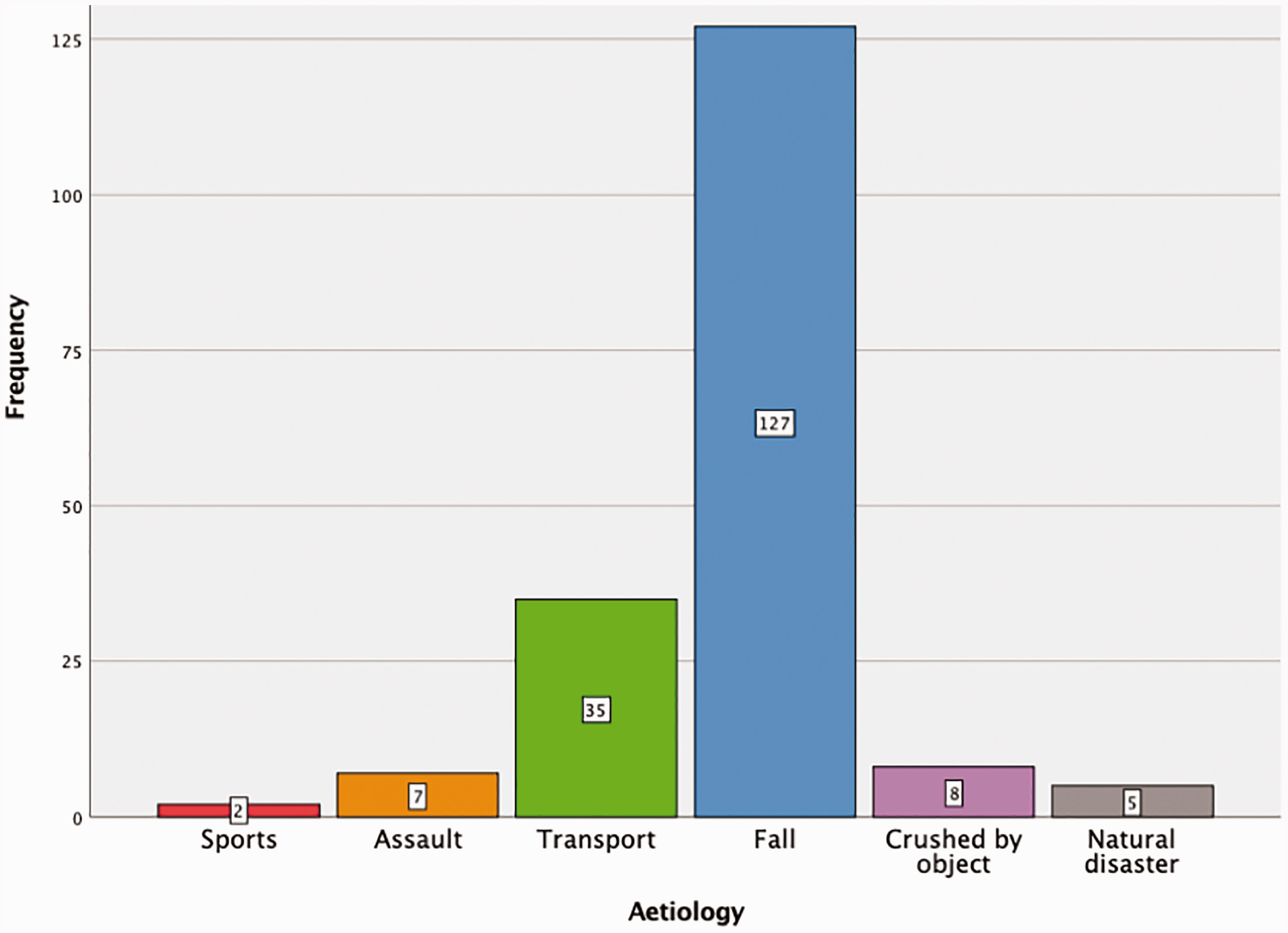
Identification of vulnerable groups
Fall-related TSCI was fairly evenly distributed across the age groups, whereas RTIs appear to be a more common cause of TSCI amongst the younger adults, with more than half occurring in the 21–30 year age group (20/35, 57.1%) and a further 25.7% in the 31–40 year age group (9/35) (Figure 5). Cause of TSCI, by age.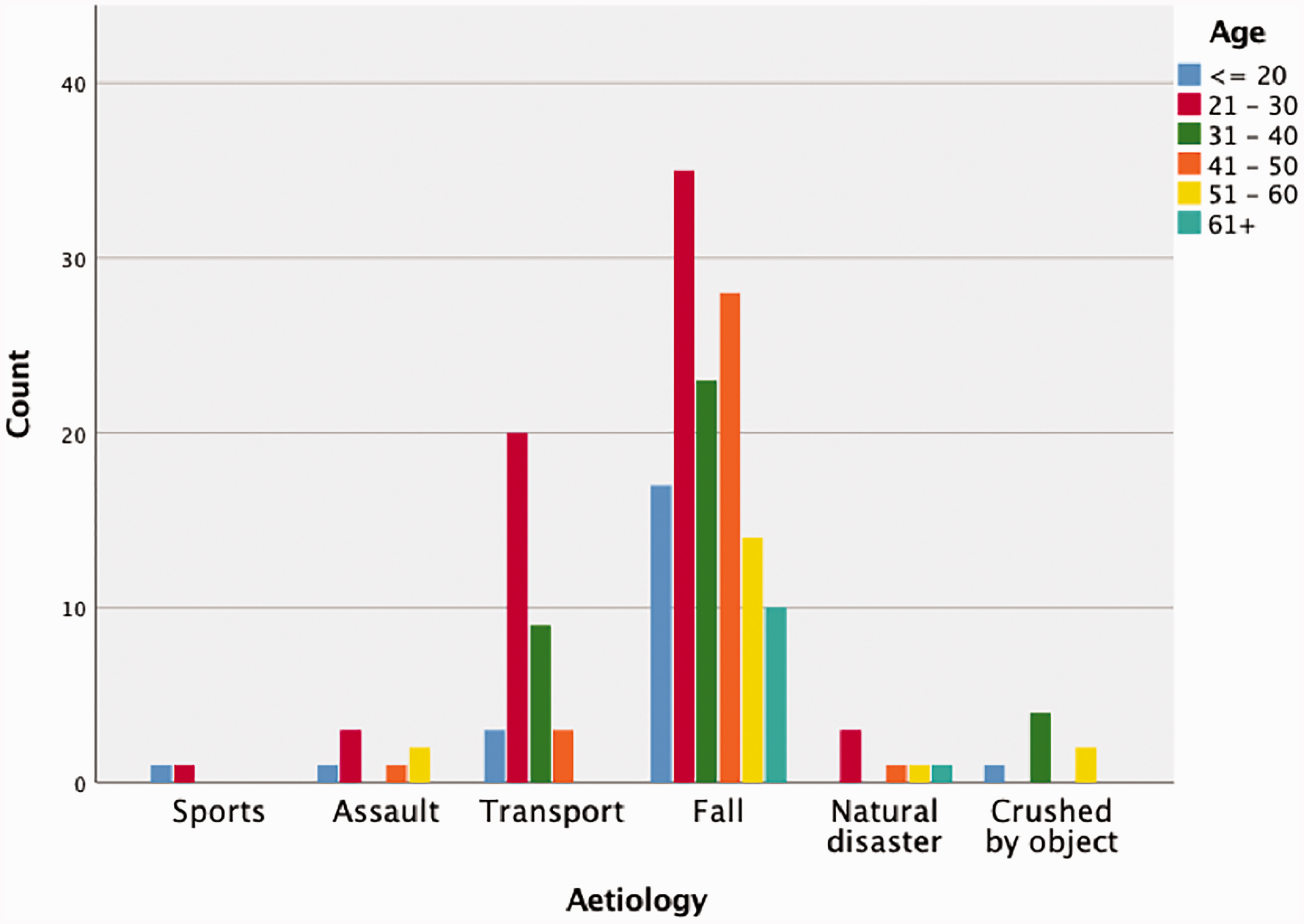
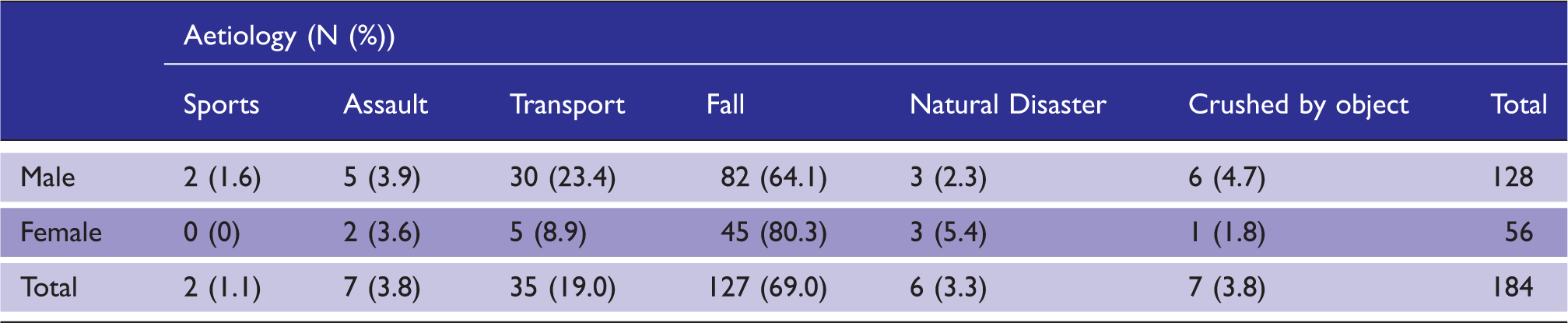
Gender and aetiology cross-tabulation. N = 184.
Discussion
This study identified the demographics of patients who sustained TSCI and were admitted to SIRC, as well as the aetiology of their TSCI. Male admissions to SIRC were almost 2.3 times higher than female admissions. Young adults were more frequently admitted, with a third of patients coming from the 21–30 year age group. Falls caused the majority of TSCI for both genders, and across all age groups, with over two thirds of the cases classified as fall-related; falls from trees accounted for nearly half of fall-related injuries. RTIs were the second most frequent cause, mainly involving two- or three-wheeled motorised vehicles and mostly involving the driver; they were commonest amongst young adults and men.
Consistent with other national 8 and international 4 studies, significantly more men were admitted than women; various explanations have been proposed for this difference, including a higher tendency amongst men to engage in high-risk behaviour 18 and being more likely to work in a hazardous occupation.19,20 TSCI was highest amongst people aged 21–30 years old, which is compatible with existing global data, 21 especially for LMICs. 4 Young adults are thought to be more susceptible to TSCI due to a higher exposure to injury risk. 22
Falls caused nearly 70% of TSCI, in common with other studies from Nepal.8–10 Whilst falls have become increasingly recognised as contributors to TSCI, 23 the magnitude of its contribution has not been fully appreciated. The presentation of TSCI in Nepal is different to that of developed countries, and most other developing countries, because RTIs are not the leading cause. 24 It appears likely that falls continue to predominate as a cause of TSCI because this primarily agricultural society still remains at a comparatively early stage of mass motorised transportation. This is changing rapidly with an expanding road network and a huge growth in two-wheeled motorised transportation.
A typical description of a fall resulting in injury, abbreviated from responses in the patient reported data, ‘I was in the tree, cutting the leaves. I slipped and fell, hitting the ground’. Falls predominantly affect farmers and members of rural communities who climb trees in order to collect fruits and leaves 25 to provide fodder for their animals. Agriculture contributes heavily to Nepal’s economy, which would explain why TSCI from falls are so common. Falls from buildings may be due to unsafe buildings and a lack of safety precautions.
Falls were a commoner cause of TSCI in female than male patients (80% and 64%, respectively), and it has been reported that women in rural areas of Nepal are the primary collectors of fodder and fuel wood 26 ; however, practices are likely to vary by district and partly depend on whether the male members of the household are working away from home or abroad. Even so, there were still nearly twice as many men admitted with fall-related TSCI than women, which suggest that the epidemiology of fall injuries is complex and the data in this sample may be affected by factors such as differential exposure to fall risks by gender and lower frequency of admission from rural districts further away from the SIRC.
Motorised two- or three-wheeled vehicles are the most commonly involved vehicle in RTIs leading to TSCI, being reported in 40% of cases, similar to other studies in the South-East Asia region. 7 Motorised two or three-wheeled vehicles are more prevalent in Nepal than in HICs, with motorbikes making up 79% of all registered vehicles in Nepal. 27 There are also fewer safety restrictions for these vehicles than larger vehicles, and enforcement is relatively limited, 28 which could explain why two- or three-wheeled motorised vehicles were more commonly involved. RTIs rarely occurred in women: the odds of an RTI being the cause of TSCI were 2.7 times higher in men than women, which is again consistent with other international studies suggesting a higher susceptibility in men, 29 and is likely explained by a lower usage of motorcycles amongst women, a higher risk of driver faults amongst men, and a greater risk of serious injury during RTIs in men. 30 The majority of RTIs resulting in TSCI involved drivers rather than passengers or pedestrians. The reasons for this are likely to be complex and may include factors such as the proportion of motorcycle journeys travelled solo or with passengers and whether driver behaviour is more dangerous (e.g. speeding, overtaking) when travelling solo rather than with passengers.
Strengths and limitations
SIRC receives patients from all over Nepal, providing a sample that originates in many different areas. This is particularly relevant in Nepal, as there is considerable variation between the mountainous, hill, and plain regions, as well as between the central Kathmandu valley and surrounding rural areas; however, there is a geographical bias in the presenting population towards Province number 3, in which SIRC is located, as it is more accessible and better known amongst patients and doctors. Other biases may exist in the cohort, but it is difficult to ascertain without data from another TSCI centre to compare. Data were collected systematically using a standardised data collection form from all admitted patients, ensuring reliability and comparability to other standardised studies and were restricted to one TSCI centre, excluding TSCI patients that may have been admitted elsewhere. Wealthier patients are more likely to be admitted to private facilities for rehabilitation, which results in the SIRC population having a socioeconomic background that is shifted towards the lower end of the spectrum, meaning that the results may not be representative of the more affluent populations. Measures of socieconomic status were not routinely collected in this dataset limiting the ability to explore this hypothesis further. The dataset analysed was established to describe the injuries and healthcare needs of the patients at this specialist centre and was not designed to explore the details of the event leading to the injury. Therefore, data on variables useful to identify vulnerable groups suitable for targeted prevention activity variables were not necessarily collected. Due to insufficient outcome data, it was not possible to make associations between the selected variables and patient outcomes.
Implications
Policy
TSCI is often the result of a preventable sequence of events. The results of this study suggest that a public health focus to identify the risk factors for TSCI and how to manage them is warranted. The growing concerns about RTIs could usefully be channelled into public health messages on the risk of life changing TSCI for young men on two-wheeled vehicles. This study provides useful information to SIRC about the demographics of their patients and can help inform future policy development within their centre.
Future research
The results of this study highlight the utility of standardised tools, such as the ISNSCI tool, across clinical settings to help place these findings in the context of TSCI across Nepal. In addition, the routine collection of factors such as ethnicity, caste, and socioeconomic status would be helpful to explore inequality in TSCI in addition to that by age and sex. The collection of routine outcome data would enable regression analyses to explore the predictors of good and poor outcomes. The limited comparative literature for this study highlights the need for wider and increased research into TSCI in Nepal and other LMICs in South-East Asia. Qualitative methods including interviews and observation could inform better understanding of the details of the event leading to TSCI, particularly with regard to falls and RTI and to better understand variability in injury risk between rural and urban areas. Specifically, qualitative research with rural communities could help understand their perspectives of risk whilst climbing trees for animal fodder and whether there are actions that could be taken to reduce the risk of injury. Furthermore, health economic research to estimate the economic impact of TSCI could be beneficial in producing a powerful argument for an increased focus on prevention.
Conclusion
This paper highlights the demographics and causes of TSCI at the main SCI rehabilitation centre in Nepal and places these findings in the context of TSCI across Nepal and internationally. Most importantly, it identifies falls as the leading cause of TSCI across both genders and all age groups. In addition, it shows RTIs to be an increasingly important cause of TSCI amongst young adult males. It reinforces findings from the limited number of existing studies and adds detail on associations between factors. This study demonstrates a need for injury surveillance and further research, as a better understanding of the pattern of TSCI in Nepal, and other similar LMICs in South-East Asia, is essential in order to enable much needed progress in SCI prevention and rehabilitation within these contexts.
Supplemental Material
sj-pdf-1-tra-10.1177_1460408620941342 - Supplemental material for The demographics and traumatic causes of spinal cord injury in Nepal: An observational study
Supplemental material, sj-pdf-1-tra-10.1177_1460408620941342 for The demographics and traumatic causes of spinal cord injury in Nepal: An observational study by Arran Willott, Raju Dhakal, Christine Groves, Julie Mytton and Matthew Ellis in Trauma
Footnotes
Declaration of conflicting interests
The author(s) declared no conflict of interest with regards to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Nepal Health Research Council provided ethical approval and oversight. The University of Bristol ethics council approved the descriptive analysis.
Informed consent
Informed consent was obtained from patients by SIRC and a signed record is retained within patient records. Data for this descriptive analysis has been anonymised.
Guarantor
AW.
Contributorship
RD and CG were involved with data collection and conceived the idea of the study. AW was involved with data analysis and wrote the first draft of the article. All authors reviewed and edited the article and approved the final version of the article.
Acknowledgements
We would like to thank the International Spinal Cord Society (ISCoS) and the Asian Spinal Cord Network (ASCoN) for all their help and for the data collected through the IDAPP pilot study.
Provenance and peer review
Not commissioned, externally peer reviewed.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.