
Abstract
Background:
Postoperative urinary retention (POUR) is a frequent complication after total knee arthroplasty (TKA), contributing to prolonged hospital stays, higher healthcare costs, and an increased risk of urinary tract infections (UTIs) and other postoperative complications. Despite the widespread use of bladder ultrasound to guide catheterization decisions, evidence supporting its superiority over symptom-based monitoring is limited. The UREA trial evaluates whether patients undergoing TKA can be safely monitored for POUR based solely on urinary symptoms, potentially reducing unnecessary catheterizations and resource use.
Methods:
The UREA study is a randomized clinical open-label single-center trial including 170 patients undergoing elective TKA. Participants are randomized in a 1:1 ratio through a sex-stratified sealed-envelope method into either (1) an ultrasound monitoring group or (2) a symptoms monitoring group. In the ultrasound group, bladder volume is assessed repeatedly with a portable scanner, with catheterization performed at a threshold of 800 mL or upon symptoms. In the symptoms monitoring group, follow-up relies exclusively on patient-reported urinary symptoms, with catheterization performed only if symptoms occur or if no spontaneous urination has occurred by 10 h postoperatively. The primary outcome is the difference in International Prostate Symptom Score (IPSS) between groups at 3 months. Secondary outcomes include IPSS at 12 months, urinary complications, and health-related quality of life assessed with the 15D instrument at 3 and 12 months. Statistical analyses will be performed on an intention-to-treat basis, with adjustments for relevant baseline variables.
Discussion:
This trial is the first randomized study to compare symptom-based with ultrasound-based monitoring of postoperative urinary retention after TKA. If symptom-based monitoring is found to be safe, it may allow for substantial reductions in unnecessary catheterization, procedural discomfort, infection risk, and resource burden. The findings have the potential to inform future clinical guidelines and promote more efficient, patient-centered postoperative care.
Keywords
Summary
A study protocol of an open-label, single-center, randomized clinical trial comparing symptoms monitoring with ultrasound-based monitoring of postoperative urinary retention after total knee arthroplasty—can patients be safely monitored without routine bladder volume measurements and a predefined catheterization threshold?
Context and relevance
Routine ultrasound-based bladder scanning with predefined catheterization thresholds is widely used to guide postoperative monitoring for urinary retention after total knee arthroplasty (TKA), despite limited evidence supporting a specific threshold or the necessity of routine scanning for all patients. There is a major knowledge gap regarding whether symptom-based monitoring can serve as the primary postoperative strategy without compromising patient safety. This Urinary REtention after Arthroplasty (UREA) study protocol, to our knowledge, is the first randomized clinical trial designed to compare symptom-based and ultrasound-based monitoring of urinary retention after TKA. The study aims to determine whether routine ultrasound-based bladder scanning can be safely omitted in postoperative monitoring of urinary retention.
Background
Postoperative urinary retention (POUR) refers to the situation where a patient is unable to urinate normally after surgery. However, there is no universally accepted definition of clinically relevant urinary retention. 1 POUR is a common complication after lower joint arthroplasty with the incidence ranging between 0% and 75%. 2 Varying definitions of POUR can explain the large range, the lack of consensus on bladder volume management, and catheterization thresholds. 3 POUR results in prolonged hospital stays and higher total hospital costs.4,5
Catheterization increases the risk of urinary tract infection (UTI), which can cause sepsis and hematogenous infection of the prosthesis6–8 also consuming nursing staff’s resources and is unpleasant for the patients. Although generally safe when performed by trained professionals, catheterization may cause complications such as urinary tract infections, urethral trauma, blood in the urine (hematuria), or bladder spasms underlining the importance of minimizing unnecessary catheterizations whenever possible. Nowadays the need for catheterization is determined with an ultrasound scanner. A catheterization threshold of 800 mL is shown to be safe among patients undergoing total hip and knee arthroplasty. 9 Nevertheless, there are no evidence-based recommendations on the optimal catheterization threshold for treating POUR.
The International Prostate Symptom Score (IPSS) is based on the symptom index for benign prostate hyperplasia developed by the American Urological Association. 10 IPSS can be used to predict POUR after lower limb arthroplasty.11,12 The safety of different POUR catheterization thresholds can be assessed pre- and postoperatively by IPSS to detect possible differences between the measurements. 9 IPSS can also be used to evaluate lower urinary tract symptoms in women. 13 Men are known to have a substantially higher risk of postoperative urinary retention than women, largely due to anatomical and functional differences such as prostatic enlargement and bladder outlet obstruction. 14
The aim of this randomized clinical trial (RCT) is to assess the potential difference in symptoms measured by IPSS at 3 months after TKA between patients who have ultrasound monitoring for urinary retention compared with patients monitored only based on symptoms.
In addition, this study also aims to assess whether there is a difference in symptoms 12 months after surgery and the occurrence of urinary complications, such as the need for catheterization, hematuria, urinary tract infections (UTIs), and urinary incontinence, at both 3 and 12 months after surgery. Finally, the study will evaluate the differences in quality of life (QOL) between the two groups at 3 and 12 months, using a validated Finnish general health-related QOL questionnaire (15D score). 15
Methods
Hypothesis
The study hypothesis is that there will be no clinically relevant and statistically significant differences between the two groups in symptoms at 3 and 12 months after surgery.
Study design
This is a randomized clinical open-label single-center trial comparing ultrasound urinary retention monitoring and symptoms monitoring in patients undergoing TKA. The trial has been registered at ClinicalTrials.gov (NCT04707001). All patients participating in the study will give written consent. Potential participants are identified from the patient pool at the Wellbeing Services County of Central Finland. The protocol adheres to the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) statement. 16 A flowchart of the trial is shown in Fig. 1.
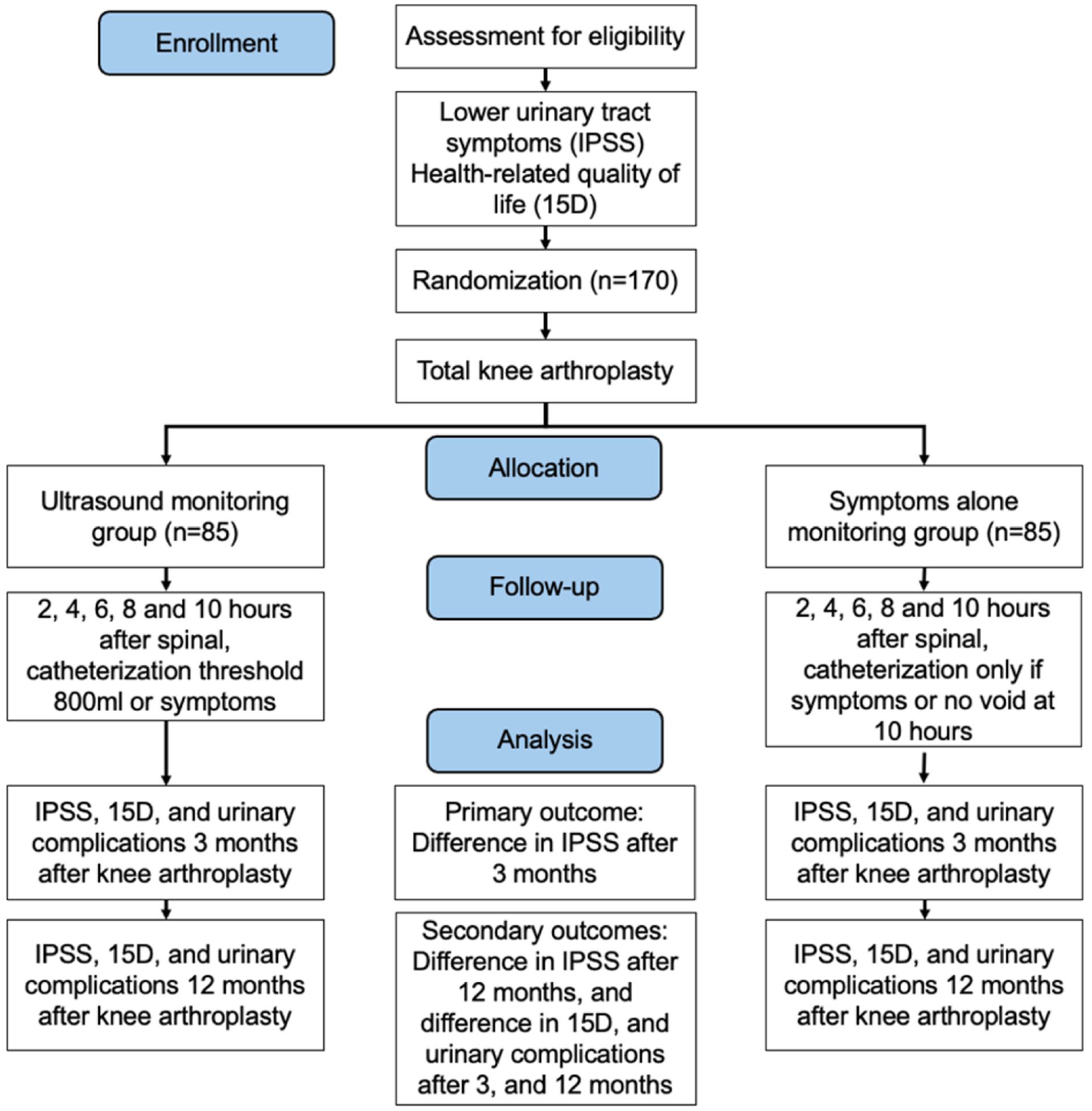
UREA trial flow diagram.
Patient selection
All adult patients (18 years and above) undergoing elective TKA in the Wellbeing Services County of Central Finland will be evaluated for enrollment. Patients referred to an orthopedic surgeon for TKA evaluation will receive general information about the study, and those scheduled for TKA will be pre-screened for eligibility (Table 1).
Participant timeline of the study: Content for the schedule of enrollment, interventions, and assessments.
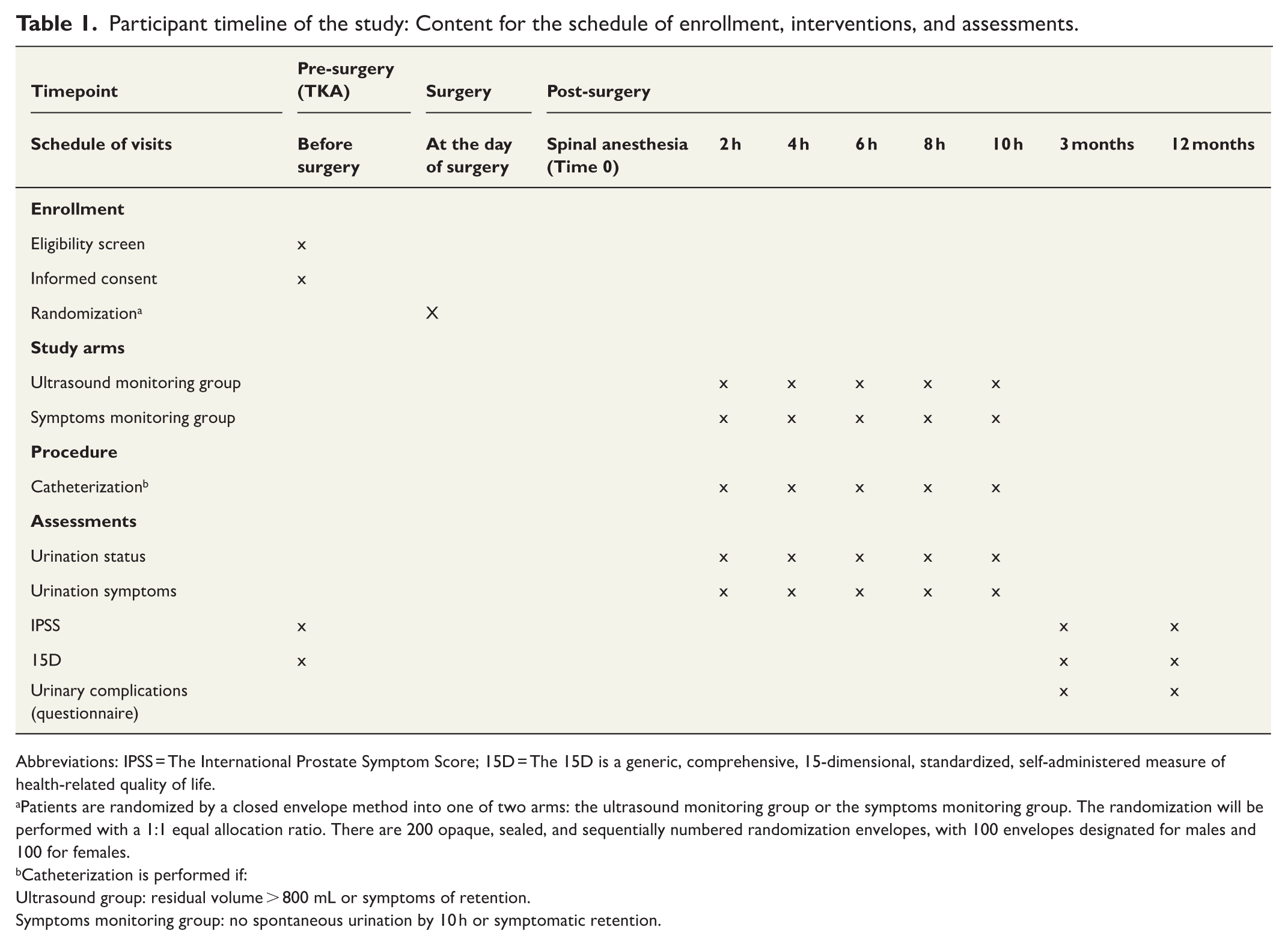
Abbreviations: IPSS = The International Prostate Symptom Score; 15D = The 15D is a generic, comprehensive, 15-dimensional, standardized, self-administered measure of health-related quality of life.
Patients are randomized by a closed envelope method into one of two arms: the ultrasound monitoring group or the symptoms monitoring group. The randomization will be performed with a 1:1 equal allocation ratio. There are 200 opaque, sealed, and sequentially numbered randomization envelopes, with 100 envelopes designated for males and 100 for females.
Catheterization is performed if:
Ultrasound group: residual volume > 800 mL or symptoms of retention.
Symptoms monitoring group: no spontaneous urination by 10 h or symptomatic retention.
The inclusion criteria include: (1) age 18 years and above, (2) elective TKA, (3) preoperative plan to use spinal anesthesia, and (4) patients must be able to provide a written signed informed consent.
Exclusion criteria include: (1) pre-planned general anesthesia, (2) previous surgery for urologic cancer, (3) fracture as an indication for surgery, (4) unwillingness to volunteer, (5) untreated urinary retention, (6) nephrostomy, (7) indwelling catheter, (8) intermittent catheterization, and (9) existing suprapubic catheter.
At the Wellbeing Services County of Central Finland, almost all primary TKA procedures are performed under spinal anesthesia. Because the risk of POUR differs between general and spinal anesthesia, 3 patients with pre-planned general anesthesia are excluded to avoid confounding.
After providing informed consent, participants complete the baseline questionnaires (IPSS and 15D).
Randomization
Patients are randomized by a closed envelope method into one of two arms: the ultrasound monitoring group or the symptoms monitoring group. The randomization will be performed with a 1:1 equal allocation ratio. To account for the known sex-related differences in the risk of postoperative urinary retention, randomization is stratified by sex. The primary investigator prepares 200 opaque, sealed envelopes, with 100 designated for male patients and 100 for female patients. The envelopes are then shuffled and sequentially numbered by the primary investigator before being distributed to the preoperative outpatient clinic. Randomization will be performed before surgery on the morning of operation. To randomize a patient, the nurse on duty in the preoperative clinic opens a consecutively numbered sex-specific envelope containing information regarding the randomization group assignment. None of the nurses are part of the core study group.
Sample size calculation
We aim to recruit 170 patients equally in the two arms. The study is designed as a superiority randomized clinical trial, with the primary endpoint being the between-group difference in IPSS at 3 months after TKA. The lowest pre-defined minimally clinically important difference in IPSS (primary outcome) is 3 points. 17 In the general population, the standard deviation is 6.5 points. Calculating with 150 patients, 75 in each group, this study has 80% power with a two-sided 5% type I error to detect a between-group difference of 3 IPSS points. Factoring in a 10% dropout rate, the total estimated sample size of 170 subjects is deemed more than adequate to detect statistically significant differences between groups in the primary outcome.
Interventions
Ultrasound monitoring group (control arm)
In the ultrasound group, urinary retention is monitored with an ultrasound scanner (CUBEscan™ BioCon-700, South Gloucestershire, UK) 2, 4, 6, 8, and 10 h after the onset of spinal anesthesia. The patient is catheterized if residual urine exceeds 800 mL or if the patient is symptomatic. The control arm adheres to the current clinical practice in the Wellbeing Services County of Central Finland, where bladder volume is routinely monitored post-surgery.
The recovery room nurse performs bladder ultrasound monitoring. The CUBEscan™ BioCon-700 is a portable ultrasound device used to measure bladder volume non-invasively. It operates by emitting ultrasound waves that reflect from the bladder wall, allowing calculation of bladder volume. Studies have shown that such devices provide reasonably accurate and reproducible readings of bladder capacity, particularly in detecting urinary retention.18,19 However, the accuracy can be influenced by factors such as the operator’s skill, the patient’s body habitus (e.g. obesity), and the position of the bladder during scanning. While highly useful, it is important to note that, like all ultrasound devices, CUBEscan measurements may have limitations in very small or very large bladder volumes.
In comparison with invasive methods like catheterization, CUBEscan offers a safer, less discomforting alternative with a reasonable degree of precision. For routine monitoring, its reliability is sufficient for clinical decision-making, but repeated measurements may sometimes be necessary for borderline cases.
Symptoms monitoring group (intervention arm)
In the symptoms monitoring group, urination is monitored by asking at regular intervals (2, 4, 6, 8, and 10 h after the onset of spinal anesthesia) about the onset of spontaneous urination, and the patient is catheterized only on a symptomatic basis or if spontaneous urination has not started 10 h after the onset of spinal anesthesia. Symptoms that indicate catheterization are lower abdominal pain or an urge to but inability to urinate voluntarily.
Bladder catheterization
Bladder catheterization is generally a safe and routine procedure in the recovery room after surgery for relieving urinary retention. It is a common intervention that helps to prevent bladder overdistension, which can lead to more serious complications if untreated.
Bladder catheterization is performed routinely by trained nurses. If the indication is unclear or there are technical difficulties, the nurses consult the surgeon on call. Careful preparation is performed by cleaning the urethral meatus, followed by instillation of lidocaine gel into the urethra. Using sterile technique and without excessive force, the catheter is inserted into the bladder. Intermittent catheterization is used, that is, the catheter is removed immediately after bladder emptying. Thin catheters (Ch 10–14) are typically used; in males with prostate enlargement, a Tiemann tip catheter can be used. When performed by trained healthcare professionals, catheterization is considered a low-risk procedure with a high benefit for managing postoperative urinary retention. Proper aseptic techniques and monitoring minimize the likelihood of complications.
Follow-up
The study was initiated in May 2021. All the patients have been randomized with complete follow-up finalized in 2025.
In both groups, patients are monitored 10 h after the initiation of spinal anesthesia (hyperbaric bupivacaine) (Fig. 1). The typical dose of hyperbaric bupivacaine is 2–2.5 mL (5 mg/mL), with the exact amount determined by the attending anesthesiologist according to clinical judgment. There is no standardized protocol for perioperative use of other drugs that may affect urinary retention (e.g. opioids, gabapentinoids), and their use is not systematically recorded. Patients receiving medication for benign prostatic hyperplasia continue their regular treatment according to clinical practice, but this is not specifically documented for study purposes.
At 3 months after surgery, participants receive the IPSS, 15D, and urinary complications questionnaires by mail and are asked to return the completed forms to the study hospital. The same questionnaires are administered at 12 months postoperatively.
Outcome measures and statistical analysis
Primary and secondary outcomes
The primary outcome of this study is the difference in IPSS scores at 3 months after TKA in patients undergoing ultrasound urinary retention monitoring compared to patients undergoing symptoms monitoring.
The secondary outcomes include IPSS at 12 months, the incidence of urinary complications (need for catheterization, hematuria, UTIs, and urinary incontinence) at 3 and 12 months, and health-related quality of life (QOL) using the validated 15D questionnaire at 3 and 12 months after surgery.
Patient reported outcomes
The study utilizes the IPSS, 15D, and self-made urinary complication questionnaires. IPSS can be utilized to measure the severity of lower urinary tract symptoms. 10 It is a validated, reproducible scoring system to assess disease severity. The questionnaire includes seven questions related to urination symptoms. A score of 0–7 indicates mild symptoms, 8–19 indicates moderate symptoms, and 20–35 indicates severe symptoms.
The 15D is a generic, comprehensive (15-dimensional), self-administered instrument for measuring HRQoL among adults (age 16+ years). 15 It combines the advantages of a profile and a preference-based, single index measure. A set of utility or preference weights is used to generate the 15D score (single index number) on a 0–1 scale. In most of the important properties, the 15D compares favorably with other preference-based generic instruments.
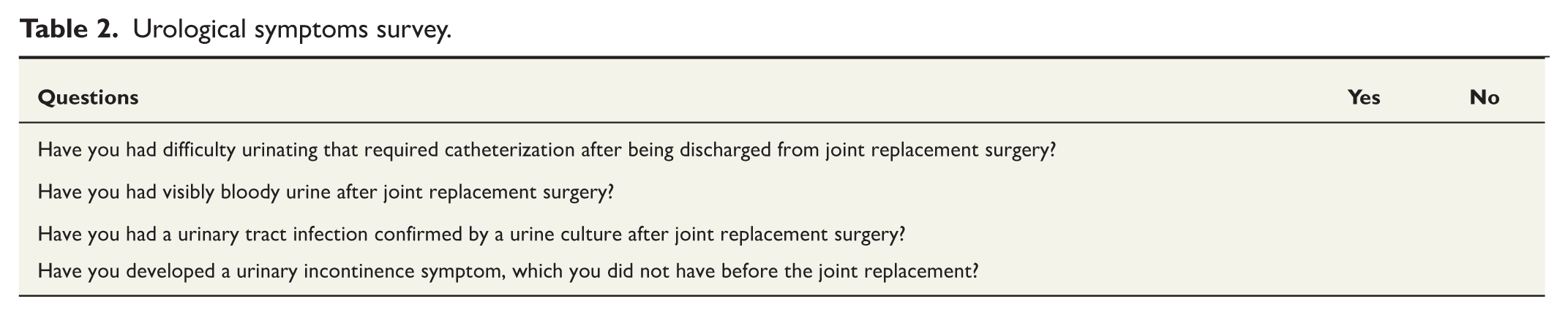
A self-made urinary complication questionnaire (Table 2), which is based on the typical complications observed in our normal clinical practice, includes the following themes: (1) difficulty in urinating, requiring catheterization; (2) visible blood during urinating; (3) urinary tract infections, which have been confirmed by urine culture; and (4) development of urinary incontinence symptoms.
Urological symptoms survey.
Patient-reported (PRO) questionnaires provide insights into the patient’s perspective on their health status, symptoms, and quality of life, which may not be fully captured through clinical measures alone. PROs can help identify issues such as symptoms or side effects early, allowing for timely interventions and adjustments in treatment.
Data collection
Study data will initially be collected on paper forms and then recorded in the online database. All data are handled confidentially and the information in the datasets in the analyses is non-identifiable. Data is gathered during the orthopedic referral, hospitalization for the surgery, follow-up questionnaires, and phone calls if needed. The primary investigator will be in charge of the common database with full access to the data, while access for others will be restricted. The researchers need full access to the data in order to be able to correct possible false data entries, enter missing data, and to track the number of enrolled patients. The online database will not be used for other purposes during the trial.
Statistical hypothesis
The study is designed as a superiority randomized clinical trial. The primary outcome is IPSS at 3 months after surgery. The primary objective is to evaluate whether there is a between-group difference in mean IPSS at 3 months between patients undergoing ultrasound-based monitoring and those undergoing symptom-based monitoring. The null hypothesis is that the mean IPSS is equal between groups (
Statistical analyses
The primary analysis will be carried out on an intention-to-treat basis. A secondary analysis of the population will be made on a per-protocol basis. Missing data exceeding 5% will be imputed using appropriate methods, and intercurrent events will be managed individually, with participants experiencing such events censored at the time of the event.
The primary outcome is IPSS 3 months after the surgery. The difference between the groups will be evaluated by Welch’s T-test. We will calculate the mean value for the difference between the groups and report it with its 95% confidence interval. The primary outcome will also be analyzed adjusting for IPSS before surgery, age, and sex. All primary analyses will be conducted using a two-sided test with a significance level of 0.05.
The secondary outcomes are IPSS at 12 months, 15D, and urinary complications questionnaires (3 and 12 months). The primary analysis will be a crude analysis, and the secondary analysis will be covariate-adjusted similar to the primary outcome. Results at 12 months will be analyzed in a similar manner as those at 3 months. Results will be analyzed with R statistical software (RStudio 4.x).
Ethics and dissemination
The study protocol was accepted by the Ethics Committee of the Wellbeing Services County of Central Finland (1U/2020, 20.2.2020). The trial will be conducted in compliance with the Declaration of Helsinki. All data are handled in accordance with current Finnish legislation and the EU General Data Protection Regulation (GDPR). Participation is voluntary, and patients may withdraw their consent at any time without providing a reason and without any impact on their clinical care.
The risks for the patient inflicted by participation in the study are deemed minimal. Participating in the study does not affect the timing of the surgery, anesthesia, surgical technique, or hospital discharge as it only affects the method of monitoring postoperative urinary retention. In the ultrasound group, urinary retention is monitored according to current practice with an ultrasound scanner, and the patient is catheterized if either the residual exceeds 800 mL or the patient is symptomatic. The optimal threshold for catheterization is unknown, but 800 mL is safe after arthroplasty (9). Patients are informed to urinate just before the onset of the spinal anesthesia. Normal diuresis is 0.5–1.0 mL/kg/h. In the symptoms monitoring group the maximal follow-up time is 10 h before the patient is catheterized if spontaneous urination has not occurred. With an example patient of 70 kg, the bladder volume should be around 350–700 mL after 10 h. Previous studies report that urinary retention over 1000 mL becomes a risk factor for future urologic complications. 20 It is also possible that chronic urinary retention can cause bladder overdistension, impairing its contractility and effective urine expulsion. Persistent overdistension may damage the bladder wall and reduce its function, increasing the risk of renal insufficiency due to backpressure on the kidneys. Prolonged bladder outlet obstruction can lead to vesicoureteral reflux, where urine flows backward into the ureters and kidneys, causing recurrent infections and renal parenchymal damage, potentially resulting in chronic kidney disease (CKD). In addition, urinary retention increases the risk of urinary tract infections (UTIs) due to stagnant urine and incomplete bladder emptying. 21 However, considering that the duration of the intervention is only 10 h, this should not pose a significant risk to patients.
There are also risks related to PRO questionnaires, such as: (1) Response bias: patients may provide responses that are not fully accurate or may be influenced by social desirability, recall bias, or their current mood, potentially affecting the reliability of the data; (2) Interpretation challenges: Variability in how patients understand and interpret questions can lead to inconsistent or unclear results, making it difficult to compare responses across different individuals; (3) Burden on patients: Filling out PRO questionnaires can be time-consuming or challenging, particularly for patients with severe symptoms; (4) Data privacy: There is a risk of sensitive personal health information being exposed or mishandled, which underscores the need for secure data management practices; and (5) Limited scope: PRO questionnaires may not capture all relevant clinical or physiological information, potentially overlooking aspects of health that are not covered by the questionnaire. 22
Consequently, after a thorough assessment of the study’s parameters and potential risks, it has been determined that the study is considered safe to proceed. The evaluation confirms that the safeguards and protocols in place sufficiently mitigate any potential risks, ensuring that conducting the study will not pose significant safety concerns for participant.
Full reports of this study will be submitted to peer-reviewed journals within the fields.
Discussion
The UREA study can offer crucial novel monitoring strategies for POUR patients undergoing TKA. POUR is a common problem, and it is important to closely monitor this following total arthroplasty because it raises infection risk. To our knowledge, this is the first study to evaluate the safety of symptoms-only monitoring compared with ultrasound monitoring of urinary retention after TKA. Symptoms-only monitoring might decrease the need for catheterization lowering the risk of UTI and hematogenous infection of the prosthesis. A previous study has shown that a catheterization threshold of 800 mL compared to 500 mL after total arthroplasty significantly reduced the need for postoperative urinary catheterization, without increasing urological complications. 9 However, it is unknown whether there is a need for a specific catheterization threshold. Thus, the study could determine whether patients can be safely monitored solely based on their symptoms.
The rationale behind symptoms-only monitoring is that a universal catheterization threshold may not be suitable for all patients hypothesizing that patients can be safely monitored based on their symptoms without increasing the need for postoperative catheterization. Safety will be analyzed by IPSS and complemented with the urinary complication questionnaire. Quality of life will be analyzed using the 15D-questionnaire and is expected to be similar between the two groups.
There are some potential limitations in the trial. First, for practical reasons, it is not feasible to blind patients. The lack of blinding could in theory affect the results, particularly patient-reported outcomes, as awareness of group allocation may influence responses. However, blinding was deemed impossible for pragmatic reasons, and both groups otherwise received identical perioperative care, which should reduce the risk of systematic bias. Second, the recruitment of patients can be slow, because this is a single center trial. However, TKA is one of the most common surgical procedures in our center, and the speed of recruitment should be adequate. Another limitation is that perioperative medications, such as analgesics or drugs for benign prostatic hyperplasia, were not systematically recorded. These medications may influence the risk of urinary retention, but randomization should help distribute any such differences evenly between the groups mitigating this risk of bias.
The strengths of the study are the pragmatic nature of the study and randomized clinical trial design. The interventions are conducted in a clinical setting enhancing the potential future implementation of retention monitoring in healthcare systems potentially reducing equipment costs and optimizing personnel resources.
In summary, the UREA trial is a randomized controlled study comparing ultrasound and symptoms-only monitoring of urinary retention after TKA. The study offers novel information to determine the safety of monitoring TKA patients without a specific catheterization threshold.
Footnotes
Acknowledgements
We are grateful to all the faculties and funding sources whose support has been essential in designing this research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is financed by Finnish State Competitive Research Funding (Erityisvaltionosuus, EVO). The funders have no role in analysis of the data, drafting of the manuscript, or the decision to submit the manuscript for peer review.
Trial registration
ClinicalTrials.gov (NCT04707001).