
Abstract
Background and Aims:
ERAS protocols are widely used in colorectal surgery, yet their impact on outcomes in diverticular disease (DD) is unclear. The primary aim of this study was to compare postoperative complication rates after left-sided colon resections for either DD or left-sided colonic cancer within an ERAS pathway, the secondary aim was to assess ERAS protocol compliance.
Methods:
This retrospective multicenter cohort study used data from the Swedish ERAS® Interactive Audit System (EIAS) from 2010 to 2020. All participating centers consecutively register elective colorectal procedures in patients aged ⩾ 18 years. We included all adult patients undergoing elective left-sided colonic or sigmoid resection at participating centers, where all procedures are mandatorily registered within a standardized ERAS pathway, with no additional exclusions. ERAS protocol compliance (pre- and intraoperative items), postoperative symptoms, and postoperative complications were assessed according to ERAS® guidelines and compared between diagnostic groups. Associations between variables and outcomes were evaluated using logistic regression.
Results:
A total of 3774 patients were included (879 with DD and 2895 with cancer). Patients in the DD group were younger and had fewer comorbidities. ERAS compliance was similar between groups (86.3% for DD vs 86.7% for cancer). In multivariable analysis, there was no statistically significant difference in severe complications (Clavien–Dindo grade III–IV) between the DD and cancer groups (11.8% vs 13.1%; OR = 0.97, 95% CI = 0.87–1.09). However, DD was associated with a higher rate of overall complications (39.2% vs 36.5%; OR = 1.27, 95% CI = 1.07–1.52), particularly infectious complications (17.0% vs 12.1%; OR = 1.55, 95% CI = 1.23–1.97), including intra-abdominal abscesses (3.5% vs 2.3%; OR = 1.62, 95% CI = 1.01–2.60). In addition, DD patients were more likely to experience postoperative pain that delayed hospital discharge (5.2% vs 2.4%, OR = 1.78, 95% CI = 1.17–2.70).
Conclusions:
Despite similar adherence to the ERAS protocol, surgery for DD was associated with a higher overall rate of postoperative complications and similar rates of severe complications as surgery for colonic cancer. The considerable risk of complications should be carefully considered when counseling patients with DD for elective surgery.
Introduction
Diverticular disease (DD) is increasingly common in developed countries1,2 and may lead to serious complications such as perforation, abscesses, fistulas, bleeding, and peritonitis. 3
Recurrent or persistent inflammation as well as chronic complications like fistulas and stenoses can impair quality of life, and often prompt elective surgery. As in left sided colon cancer, typically a left-sided or sigmoid colon resection with primary anastomosis or a Hartmann’s procedure is performed.4,5 However, the decision to operate on DD remains controversial. Unlike colon cancer, where surgery is often lifesaving, the benefit of elective surgery in DD must be weighed against the significant risk of postoperative complications, especially in uncomplicated disease. Notably, studies specifically comparing surgery for diverticular disease and colorectal cancer report an anastomotic leakage (AL) rate of approximately 8%–9% in both groups.6,7 In DD, diverticula in the anastomosis, chronic inflammation and fibrosis may compromise tissue integrity and increase this risk.
The Enhanced Recovery After Surgery (ERAS) protocol 8 is a standardized, multimodal perioperative care program incorporating 25 evidence-based interventions. It has been shown to significantly reduce postoperative complications and length of hospital stay after major surgery.9–11 Patients undergoing elective colonic resections both for DD and for colon cancer have been systematically recorded in the Swedish branch of the International ERAS® Interactive Audit System (EIAS), which collects over 300 perioperative variables per patient. The registry provides an ideal framework for investigating surgical predictors and outcomes.
The primary aim of this study was to compare postoperative complication rates after surgery for diverticular disease and colon cancer; the secondary aim was to compare compliance with the ERAS protocol.
Methods
Study design, setting and participants
This retrospective multicenter cohort study included patients from all Swedish hospitals consistently reporting perioperative clinical data in EIAS. The participating institutions consisted of 5 University and 15 non-academic hospitals representing 20 out of 36 hospitals in Sweden regularly performing major colorectal surgery. 12 All adult patients undergoing elective resection for DD (ICD-coding K57.2, K57.3, K57.4, K57.5, K57.8, and K57.9) and left sided colon cancer (C18.6, C18.7, and C19.9) that underwent left sided colectomy or sigmoid resection with primary anastomosis or colostomy (Hartmann’s procedure) between 1 January 2010 and 31 December 2022 were included. Emergency operations and patients with local recurrence from colon cancer were excluded. Although ICD-10 codes were used to define diverticular disease, no stratification into complicated and uncomplicated diverticulitis was performed, as prior validation of the ERAS registry demonstrated limited concordance between ICD-10 coding and the actual clinical severity of diverticular disease documented in medical records.
All participating centers strive to treat their patients in accordance with the ERAS® Society Guideline for colonic surgery, which encompasses 25 evidence-based pre-, intra-, and post-operative interventions. 8 In 2021, a validation of the Swedish portion of EIAS showed near complete coverage (98.8%), with good data accuracy and few missing values. 13 All ERAS-affiliated centers consecutively and prospectively register all electively operated patients, ensuring that all these patients were included in the present study. Discharge from hospital is based on ERAS criteria, defined as adequate pain control (VAS score ⩽ 4 on oral analgesics), tolerance of oral intake, return of gastrointestinal function, independent mobilization, and absence of unresolved complications.
Data collection and variables
All data was collected from the EIAS database of the Swedish part of ERAS. Baseline characteristics included are described in Table 1.
Basic characteristics.
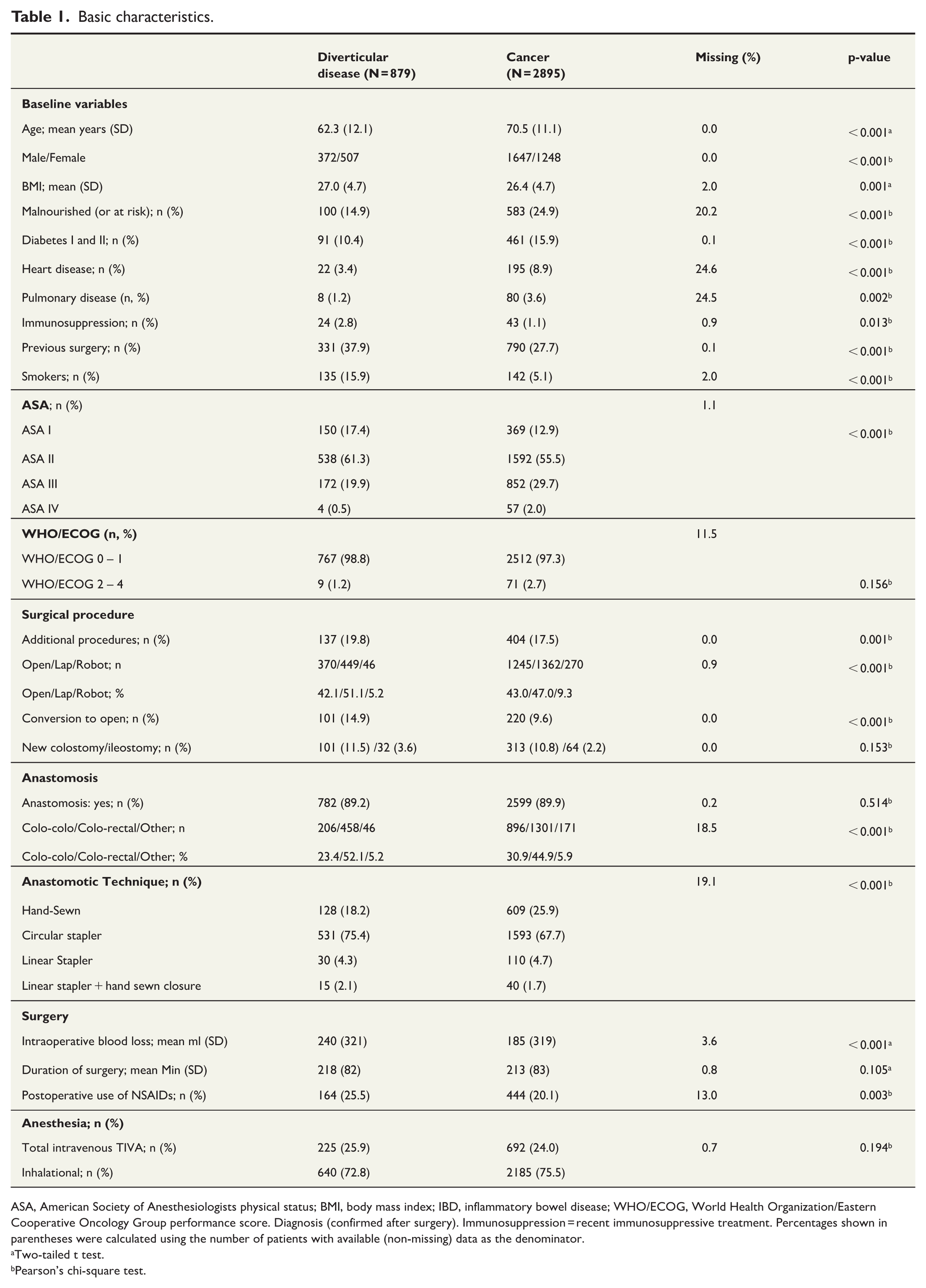
ASA, American Society of Anesthesiologists physical status; BMI, body mass index; IBD, inflammatory bowel disease; WHO/ECOG, World Health Organization/Eastern Cooperative Oncology Group performance score. Diagnosis (confirmed after surgery). Immunosuppression = recent immunosuppressive treatment. Percentages shown in parentheses were calculated using the number of patients with available (non-missing) data as the denominator.
Two-tailed t test.
Pearson’s chi-square test.
The primary outcome measure was postoperative complications, and secondary outcome measures were symptoms delaying discharge and compliance with the ERAS protocol. Compliance was recorded in the EIAS database, along with all symptoms that delayed discharge and any complications occurring within 30 days postoperatively. Anastomotic leakage was defined according to EIAS as radiologically confirmed leakage, such as contrast extravasation, peri-anastomotic fluid collection, abscess or clinically evident leakage requiring intervention or reoperation.
Statistical analysis
All categorical variables are presented as frequencies and percentages, and continuous variables as means with standard deviations. Comparisons between groups were performed using Pearson’s chi-square test or Fisher’s exact test for categorical variables, as appropriate, and the independent samples t-test for continuous variables.
The analyses were exploratory and hypothesis-generating in nature. Although key outcome primary and secondary domains (Postoperative complications within 30 days, Symptoms delaying discharge and Compliance to the ERAS-protocol) were defined a priori based on data availability in the EIAS database, no single primary outcome or formally predefined secondary outcomes were specified. Consequently, no formal adjustment for multiple testing was applied. Reported p-values should therefore be interpreted descriptively and with caution.
Unadjusted associations between categorical exposures and outcomes were assessed using multivariable logistic regression models based on a predefined selection of clinically relevant intraoperative variables. Linear regression was used for continuous outcomes. All multivariable models were adjusted for age, sex, body mass index (BMI), ASA classification, smoking status, and surgical technique. The modeling strategy was prespecified based on clinical relevance rather than data-driven variable selection.
Missing data for variables included in the regression models were handled using listwise deletion; observations with missing data in any model variable were excluded from the respective analysis. Compliance rates were calculated by excluding missing data and estimating the mean compliance for each group. Given the low proportion of missing data and the consistent handling across analyses, no separate sensitivity analysis was performed, as alternative modeling approaches were not expected to meaningfully alter the observed associations.
Results are reported as odds ratios (ORs) with 95% confidence intervals (CIs) or p-values, as appropriate. A p-value < 0.05 was considered indicative of statistical significance, acknowledging the increased risk of type I error inherent in multiple comparisons. All statistical analyses were performed using STATA version 18.0 SE (StataCorp, College Station, TX, USA).
Results are reported according to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) checklist. Ethical approval was granted by the Regional Ethical Review Board in Stockholm (DNR 2020-00435 and DNR 2020-04708). Patients were informed of their inclusion in the database and were given the opportunity to opt out upon request.
Results
Basic characteristics and surgical technique
A total of 3774 patients underwent either left-sided colectomy or sigmoid resection for diverticular disease (n = 879; 23%) or for left-sided colon cancer (n = 2895; 77%). All baseline characteristics and surgical details are reported in Table 1. There were significantly more women in the DD group (58% vs 43%). Patients in the DD group were younger, less frequently malnourished, and had fewer comorbidities compared to patients with cancer. Open surgery was performed in 370 (42.1%) of the DD cases and in 1245 (43.0%) of the cancer cases. There were statistically significant differences between groups in the type of anastomosis and anastomotic technique. A higher proportion of DD patients received NSAIDs postoperatively. The overall rate of primary anastomosis was similar between groups. Among DD patients, 69 females (13.6%) compared to 28 males (7.5%) received an end colostomy, p < 0.01.
Pre- and intraoperative compliance to ERAS protocol
Overall, the pre- and intraoperative compliance with the ERAS protocol was similar between the DD and the cancer groups (86.3% vs 86.7%). Although a few individual ERAS items showed statistically significant differences, overall clinical compliance with the individual elements was similar between the two groups. The only notable exceptions were the use of surgical drains and of postoperative nausea and vomiting prophylaxis, which both were significantly more common in the DD group, whereas bowel preparation was more frequently used in cancer patients (Table 2).
Compliance to ERAS interventions.
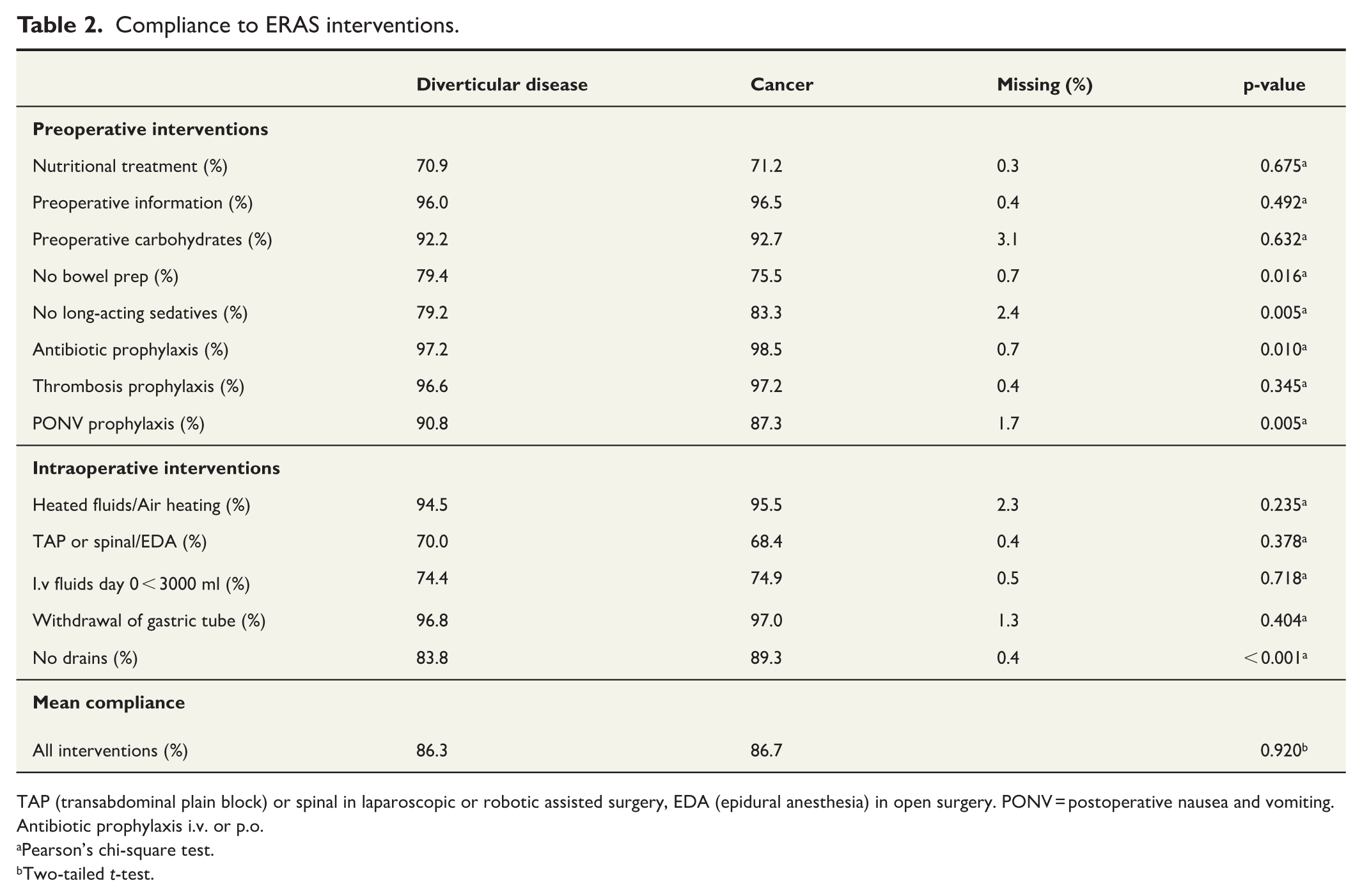
TAP (transabdominal plain block) or spinal in laparoscopic or robotic assisted surgery, EDA (epidural anesthesia) in open surgery. PONV = postoperative nausea and vomiting. Antibiotic prophylaxis i.v. or p.o.
Pearson’s chi-square test.
Two-tailed t-test.
Complications and mortality
Among patients with diverticular disease (DD), 345 (39.2%) experienced at least one complication within 30 days postoperatively, compared with 1057 (36.5%) patients undergoing surgery for cancer (adjusted OR = 1.27; 95% CI = 1.07–1.52). Infectious complications were more frequent in the DD group (17% vs 12%; adjusted OR = 1.55; 95% CI = 1.23–1.97), including intra-abdominal abscesses (3.5% vs 2.3%; adjusted OR = 1.64; 95% CI = 1.02–2.63).
There were no statistically significant differences between the groups in the rates of minor (Clavien–Dindo grade I–II) or major complications (Clavien–Dindo grade ⩾ III). Similarly, the incidence of anastomotic leakage did not differ between DD and cancer patients. In multivariable analyses, the type of anastomosis, surgical technique, and use of NSAIDs were not associated with an increased risk of anastomotic leakage.
The incidence of paralytic ileus (Table 3), wound infection, wound dehiscence, cardiovascular, cerebrovascular, respiratory, and other complications (data not shown) was comparable between the groups. Urinary tract injury occurred more frequently in the DD group; however, this difference was not statistically significant in either univariable or multivariable analyses. After adjustment for confounding factors, surgery for diverticular disease remained independently associated with a higher risk of urinary tract infection and intra-abdominal abscess formation (Table 3).
Postoperative outcomes.
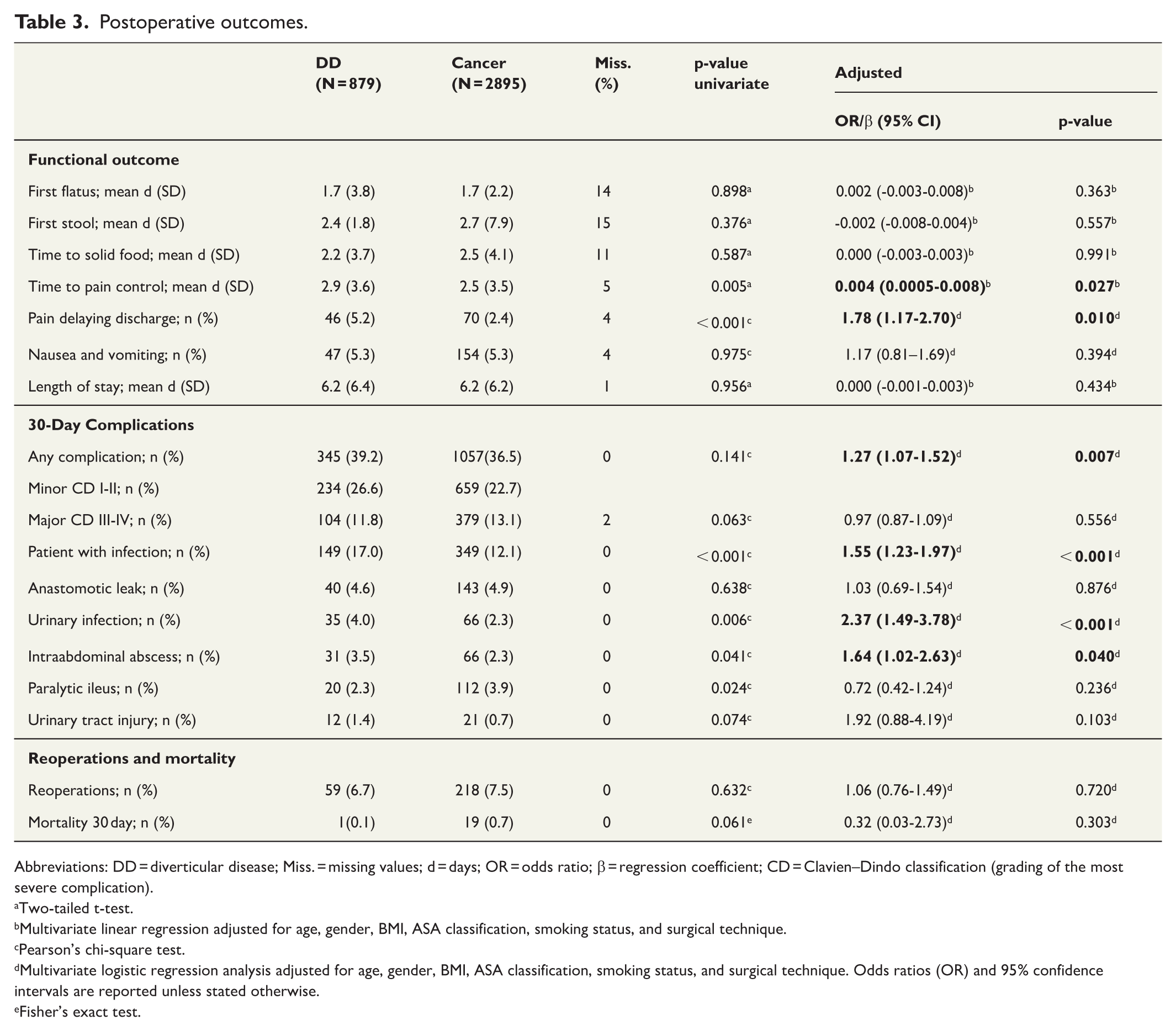
Abbreviations: DD = diverticular disease; Miss. = missing values; d = days; OR = odds ratio; β = regression coefficient; CD = Clavien–Dindo classification (grading of the most severe complication).
Two-tailed t-test.
Multivariate linear regression adjusted for age, gender, BMI, ASA classification, smoking status, and surgical technique.
Pearson’s chi-square test.
Multivariate logistic regression analysis adjusted for age, gender, BMI, ASA classification, smoking status, and surgical technique. Odds ratios (OR) and 95% confidence intervals are reported unless stated otherwise.
Fisher’s exact test.
Symptoms delaying discharge and length of stay
In terms of functional outcomes and symptoms that could delay discharge, there were no significant differences between DD and cancer patients with respect to nausea and vomiting, time to first flatus or bowel movement after surgery, and time to tolerating solid foods (Table 3). However, DD patients required more time to achieve adequate pain control and had a 78% higher risk of experiencing severe pain that delayed discharge (VAS > 4 on oral analgesics) (OR = 1.78, 95% CI: 1.17–2.70), as shown in Table 3. The reoperation rate and the mean length of hospital stay did not differ statistically significantly between the groups, with an average LOS of 6.2 days in both groups (Table 3).
Discussion
In this large ERAS-based cohort, overall adherence to ERAS protocol elements was similar between patients operated on for diverticular disease (DD) and those undergoing surgery for colonic cancer. After adjustment for confounding factors, DD patients had higher risk to have any postoperative complication, particularly infectious complications, and reported more pain affecting discharge readiness. However, both severe complications and the length of hospital stay were similar between the groups.
There remains a notable paucity of data specifically examining surgical outcomes in patients with diverticular disease (DD). This is particularly relevant given that surgery for uncomplicated diverticular disease is primarily performed to improve quality of life, whereas surgery may be mandatory in the presence of complications such as fistula or severe stenosis to prevent sepsis or bowel obstruction. The Enhanced Recovery After Surgery (ERAS) protocol, 8 with over 300 pre-, intra-, and postoperative variables systematically recorded in the international EIAS database 12 provides an ideal framework for investigating surgical outcomes.
A previous large-scale study conducted outside the context of an ERAS protocol—using only outcome variables—reported a slightly lower anastomotic leakage (AL) rate for elective sigmoidectomy in DD patients (8.3%) compared to patients with colorectal cancer (9.2%). 6 However, patients with DD demonstrated a higher incidence of postoperative infections, including intra-abdominal abscesses (1.2% vs 0.4%), 6 which may be indicative of subclinical or minor leaks. In the present study, the anastomotic leakage (AL) rate was low in both groups, 4.6% among patients with DD and 4.9% among cancer patients. This finding may reflect contemporary perioperative care practices. Although adherence to ERAS-protocols could not be quantified across centers not using ERAS, restrictive intraoperative fluid strategies, most consistently achieved within ERAS frameworks, may have contributed to the observed low AL rates. 14 It is unlikely that these findings are due to inaccurate reporting. Anastomotic leakage was recorded based on clearly defined criteria within the EIAS database, which recently has demonstrated excellent concordance with hospital records. Interestingly, neither the type of anastomosis, surgical technique, nor the use of NSAIDs appeared to influence the rate of anastomotic leakage.
In the present study, patients with diverticular disease (DD) were significantly younger than those with colorectal cancer, which is expected given that the need for treatment of symptomatic DD typically arises around the age of 6015,16 whereas the median age for colorectal cancer diagnosis is approximately 70 years . 17 Younger age is often associated with fewer comorbidities. Nevertheless, patients with diverticular disease experienced a higher incidence of infectious complications, such as urinary tract infections and intra-abdominal abscesses. This observation should be interpreted with caution, as the ERAS database does not allow reliable stratification between complicated and uncomplicated diverticulitis. Importantly, a substantial proportion of patients undergoing elective surgery for diverticular disease may have complicated disease, including fistula formation or persistent abscesses, for which surgery is indicated to prevent ongoing infection or further complications. In this context, the higher rate of infectious complications likely reflects disease severity rather than age or baseline health status. Chronic inflammation and fibrosis can distort tissue planes, making dissection more difficult and potentially longer. These changes may also impair local perfusion and healing, increasing the risk of minor or subclinical leaks that present as postoperative infections. Together, these features provide a plausible explanation for the elevated infectious complication rate in DD patients.
The rate of primary anastomosis among DD patients was 89%, which is low compared to previous smaller studies reporting rates as high as 98%. 18 This, and the notably lower rate of primary anastomosis among female patients is difficult to explain and may reflect a culture of surgical caution rather than evidence-based decision-making aimed at minimizing complications. While the overall risk of ureteral injury was low in both groups, the incidence was twice as high among patients undergoing surgery for diverticular disease compared to those treated for cancer. Pelvic inflammation commonly seen in diverticulitis can obscure visualization of the left ureter, thereby increasing the risk of injury. This is an important consideration in the surgical planning for DD patients, as ureteral injuries are serious and can result in long-term complications. Careful preoperative planning, including review of cross-sectional imaging, anticipation of distorted anatomy, and selective use of ureteral identification techniques, may help reduce the risk of ureteral injury in these patients.
The strengths of the present study include its multicenter design, large sample size, and the inclusion of over 300 consecutively recorded variables from the ERAS database. The detailed collection of these variables enables a comprehensive evaluation of the entire care pathway. In addition, there was a high level of compliance with the ERAS protocol during both the preoperative and intraoperative phases for patients with diverticular disease and those with cancer. However, as a retrospective cohort study, several limitations must be acknowledged—most notably the potential for selection bias. Moreover, certain unmeasured confounders, such as differences in surgeon experience or perioperative antibiotic protocols, may have influenced postoperative outcomes. Furthermore, as data was collected over a 10-year period, several time factors may have influenced the results. This includes evolvement of anastomotic techniques and minimally invasive surgery as well as changes in adherence to the ERAS protocol throughout the study period.
In conclusion, adherence to the ERAS protocol was similar between the groups. Surgery for diverticular disease was associated with a higher overall rate of postoperative complications compared with surgery for colonic cancer, while rates of both minor and severe complications were comparable between groups. Given the substantial risk of postoperative complications, careful consideration and thorough patient counseling are warranted when elective surgery for diverticular disease is contemplated.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969261431953 – Supplemental material for Enhanced recovery after surgery in diverticular disease: A multicenter comparison with colorectal cancer
Supplemental material, sj-docx-1-sjs-10.1177_14574969261431953 for Enhanced recovery after surgery in diverticular disease: A multicenter comparison with colorectal cancer by Mahmood Wael Mahmood, Mirna Abraham-Nordling, Anna Löf-Granström, Ali Kiasat, Fredrik Hjern and Ulf O. Gustafsson in Scandinavian Journal of Surgery
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sigurd and Elsa Goljes Memorial Foundation.
Clinical trial registration
N/A.
Data availability statement
Due to Swedish legal restrictions and the current ethical approval for the study, data is not publicly available to share, but the research group can provide descriptive data in table form.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.