
Abstract
Background and Aims:
Shared decision-making (SDM) is increasingly emphasized in clinical guidelines. For uncomplicated gallstone disease, both surgical and conservative strategies are considered safe, making patient preferences central to treatment selection. This study assessed the extent of patient involvement in decision-making regarding treatment for uncomplicated gallstone disease.
Methods:
In this prospective pilot study conducted at a surgical outpatient clinic in Norway, all referred patients with uncomplicated gallstone disease were invited to participate. Video-recorded consultations were independently evaluated by two expert raters. Surgeons, patients, and experts completed the MAPPIN-SDM questionnaire. The MAPPIN-SDM score is calculated as the mean of 11 items (0–4), with higher scores indicating greater SDM.
Results:
Of 34 eligible patients, 26 were included; 68% were women, and the mean age was 47.8 years (SD = 16.1). The overall mean MAPPIN-SDM score was 2.6 (SD = 0.48). Patients (mean = 3.5, SD = 0.48) and surgeons (mean = 2.9, SD = 0.56) rated the level of SDM higher than external observers (mean = 1.55, SD = 0.65; p < 0.001). Fourteen patients (54%) ultimately underwent surgery. Their average MAPPIN-SDM score was significantly higher than that of managed conservatively (2.89 versus 2.28, p < 0.001).
Conclusion:
This study demonstrates a moderate level of SDM in consultations for uncomplicated gallstone disease but reveals considerable discrepancies between patient/surgeon perceptions and observer assessments. Higher SDM scores were associated with the choice of surgery. These findings highlight the need for targeted strategies to improve the quality and consistency of SDM in the management of uncomplicated gallstone disease.
Context and relevance
Shared decision-making (SDM) is increasingly recognized as an essential part of good clinical practice. Prior to this study, data were limited on how SDM is practiced in the management of uncomplicated gallstone disease. This pilot study offers novel insight by objectively evaluating patient involvement using the MAPPIN-SDM tool. It reveals a moderate level of SDM, with significant discrepancies between perceived and observed patient involvement. These findings emphasize the need for SDM implementation and training to ensure patient involvement in treatment choices for uncomplicated gallstone disease.
Introduction
Gallstones increase gastrointestinal disease burden worldwide, 1 presenting in 5%–22% of patients. The prevalence varies across populations and increases with age. Most patients remain asymptomatic. 2 Risk factors for developing gallstones include female gender, age, physical inactivity, and obesity. 2 The only definite treatment for symptomatic gallstone disease is surgery, with laparoscopic cholecystectomy as the gold standard. Cholecystectomy is a commonly performed procedure with low peri- and post-operative morbidity. 3 The most common serious complication after cholecystectomy is common bile duct injury, occurring in <0.5% of patients. 4
Complications related to gallstone disease include cholecystitis, cholangitis, pancreatitis, and common bile duct stones. The term uncomplicated gallstone disease refers to patients with the presence of gallstones and episodic abdominal pain but without any of the complications developed yet. The standard treatment for gallstone disease with complications is cholecystectomy due to the high risk (30%–50% within 2 years) of recurrent complications.5,6 However, for patients with uncomplicated gallstone disease, conservative management with simple analgesics is considered a safe alternative to surgery to relieve symptoms, due to the low risk of future gallstone-related complications (3-5%).7–9
SDM is a process designed to support patients in making informed decisions. 10 Unlike informed consent, which merely documents information provision, SDM is a collaborative patient-centered communication process for arriving at informed and value-based decisions by the patients in the context of treating, screening, or preventing a health condition. 11 SDM is increasingly recognized as the essential communication model for medical decision-making, particularly in situations where there is a choice between multiple alternatives.12,13 However, a decade after the first systematic review in the field of SDM for surgical conditions, persistently low levels of patient-involvement behaviors remain, with only a marginal increase in overall scores.14,15 SDM is also viewed as a practical approach to evidence-based medicine, facilitating the integration of all relevant evidence into the clinical decision-making process.
Persisting or new abdominal symptoms, often referred to as post-cholecystectomy syndrome, are common after cholecystectomy for uncomplicated gallstone disease (20%–40%).16,17 SDM in surgery seems to be associated with a greater patient satisfaction and value agreement, leading to decreased conflict and anxiety. 18 Moreover, anxiety can be linked to patients’ perception of pain after surgery.19,20 Enhancing SDM in the treatment of uncomplicated gallstone disease may potentially affect long-term pain outcomes. One previous study has evaluated SDM during consultations regarding cholecystectomy for uncomplicated gallstone disease. 21 This study included 30 patients and unilaterally reported SDM from the patient’s perspective with a semi-structured interview and a questionnaire. The primary aim of this exploratory study was to assess the extent of patient involvement in decision-making regarding treatment of uncomplicated gallstone disease, as evaluated by patients, surgeons, and observers. Secondary aims were to examine whether surgeons’ treatment preferences were associated with patient involvement and to compare SDM scores across patients, surgeons, and observers.
Methods
Design
This explorative cross-sectional study was conducted to evaluate the communication in consultations at a surgical outpatient clinic where treatment decisions for uncomplicated gallstone disease were discussed. The patient involvement was evaluated through the perspective of the patient, the surgeon, and an objective third person (observer).
Participants and setting
Patients referred by their general practitioner to the outpatient clinic at the Department of Gastrointestinal Surgery at Oslo University Hospital due to uncomplicated gallstone disease in April, May, June, and August 2023 were invited to participate. Uncomplicated gallstone disease was defined as gallstones present on ultrasound, Computer Tomography (CT), or Magnetic Resonance (MR) scan with concomitant/associated with abdominal pain attacks and the absence of complicated gallstone disease (cholecystitis, cholangitis, common bile duct stones, or pancreatitis). Patients not fit for surgery due to comorbidities or inoperable due to previous major surgery were excluded. Patients who did not speak fluent Norwegian or had other factors complicating the communication (hearing impairment, cognitive impairment, etc.) were excluded. The consultations were carried out on five different days with five different surgeons. The surgeons were all surgical residents with 2–7 years of experience, and all had Norwegian as their first language.
Measurements
The literature provides various instruments to measure patient involvement in decisions, each differing in purpose, data sources, and psychometric properties.22–25 Among these, the Multifocal Approach to the Sharing in SDM (MAPPIN-SDM) is notable for its comprehensive evaluation of patient involvement in decision-making from multiple perspectives.26,27 This multi-method approach is a key strength of MAPPIN-SDM, as it allows us to capture both the subjective experience of participants and objective observations of the interaction. MAPPIN-SDM is considered to cover the essential elements of SDM from a theoretical point of view. 12 This instrument has been previously utilized to assess patient involvement in surgical contexts.27,28 The MAPPIN-SDM inventory comprises three observational scales (surgeon, patient, and experts) and two corresponding questionnaires (surgeon and patient). All components are structured around an identical set of 11 indicators of patient involvement, although the measurement approach differs between observers and participants (Fig. 1). For observers, each indicator is rated on a scale from “0” to “4,” where “0” indicates “The behavior is not observed” and “4” indicates “The behavior is observed to an excellent standard.” For patients and surgeons, the same indicators are assessed through direct questions about their experience and understanding. In this study, consultations were recorded on video for analysis, with the unit of analysis being the decision sequence rather than the entire consultation. Two experts (“Observers”), who have previously demonstrated excellent inter-rater reliability in assessing SDM consultations, independently evaluated these video-recorded decision sequences using the MAPPIN-SDM observational scale. 27
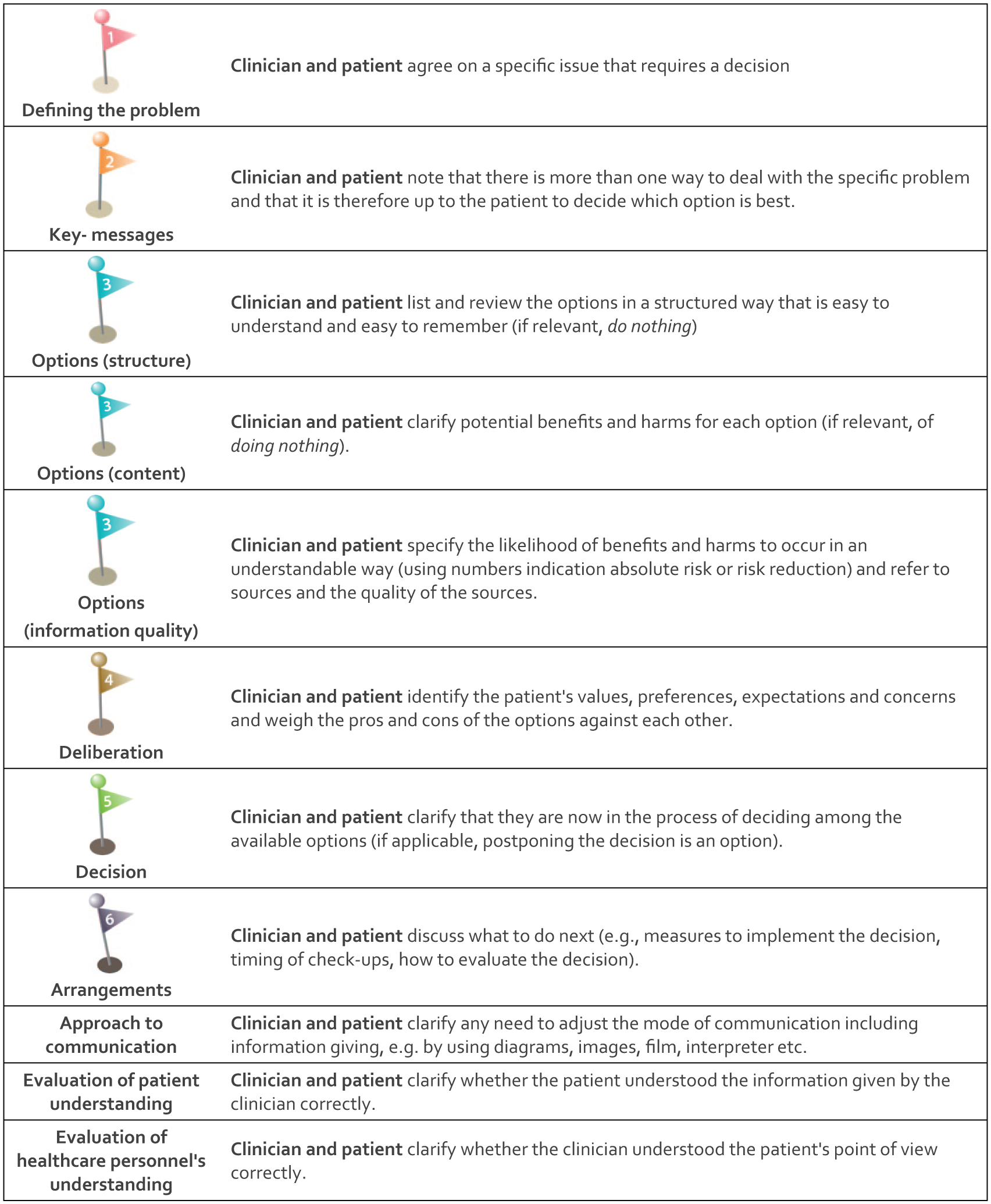
The MAPPIN-SDM inventory comprises the observer instrument, which consists of three harmonized scales for observation of patients, doctors, and both parties as a unit, along with corresponding questionnaires for patients and doctors. This table uses the phrasing from one of the observer scales. The questionnaires employ the identical criteria, but the phrasing is adjusted according to the perspective of the doctor or the patient.
The surgeons were asked to score their appraisal of the strength of an indication and their preference toward cholecystectomy on a scale from 1 to 10 for each patient as a part of the questionnaire after the consultation. One means “Weak indication and low preference for cholecystectomy” and 10 means “Strong indication and high preference towards cholecystectomy.”
Ethics
All eligible patients were reached out to by phone before the consultation to inform verbally about the study. Written information and formal signed consent were obtained before the consultation from both patient and surgeon. All patients and surgeons knew that they were recorded before the consultation. Patients not consenting to participate in the study received usual care. The local data protection officers had no objections related to the study (23/04665). The need for ethical approval was waived by the Regional Ethical Committee.
Statistical analyses
Statistical analyses were performed using SPSS Statistics 28 (IBM Corp, Armonk, NY, USA). The total SDM score (SDM-mass) was derived from the mean of the patient, surgeon, and observer scores for each patient. 29 Categorical variables were reported as counts and percentages. Continuous data were presented as mean (standard deviation). Statistical significance of differences between SDM scores from patient, surgeon, and observer was assessed using the Student’s t-test. Pearson correlations were calculated between SDM scores achieved from administering three different MAPPIN-SDM scales. The correlation between the strength of surgeons’ preference and SDM score was explored with linear regression and expressed with the Pearson correlation coefficient.
Results
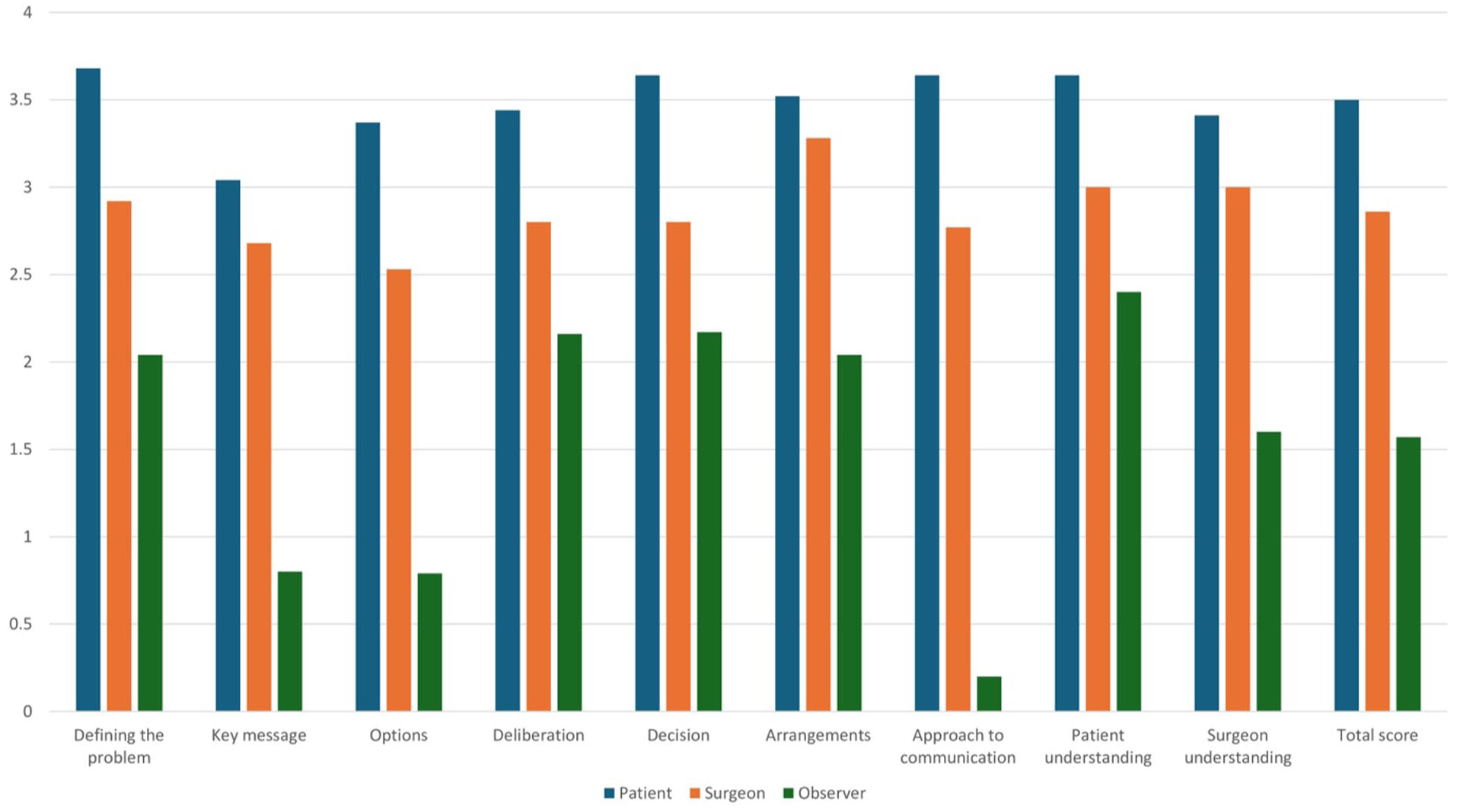
Among 34 eligible patients, 26 fulfilled the inclusion criteria and consented to participate in the study (Fig. 2). Of these, 23 (68%) were women, with a mean age of 47.8 years (SD = 16.1). None of the patients had previously undergone major abdominal surgery. There was no correlation between SDM score and age (p = 0.420) or sex (p = 0.821). The surgeon’s preference toward cholecystectomy scores was as follows: <3, 8 (29%) patients; 4–7, in 5 (18%) patients; and >7, in 15 (54%) patients. The time spent on the decision-making sequence in consultations ranged from 7 to 23 min, with a mean of 13.6 min. The overall mean MAPPIN-SDM score was 2.65 (SD = 0.48). The mean score for patients was 3.50 (SD = 0.48); for surgeons, it was 2.90 (SD = 0.56), whereas the observer score was 1.55 (SD = 0.65). The observer score was significantly lower than patient-reported scores (p < 0.001). The lowest MAPPIN-SDM scores were reported for the domains “key message,” “alternatives,” and “meta-communication” (Fig. 3).
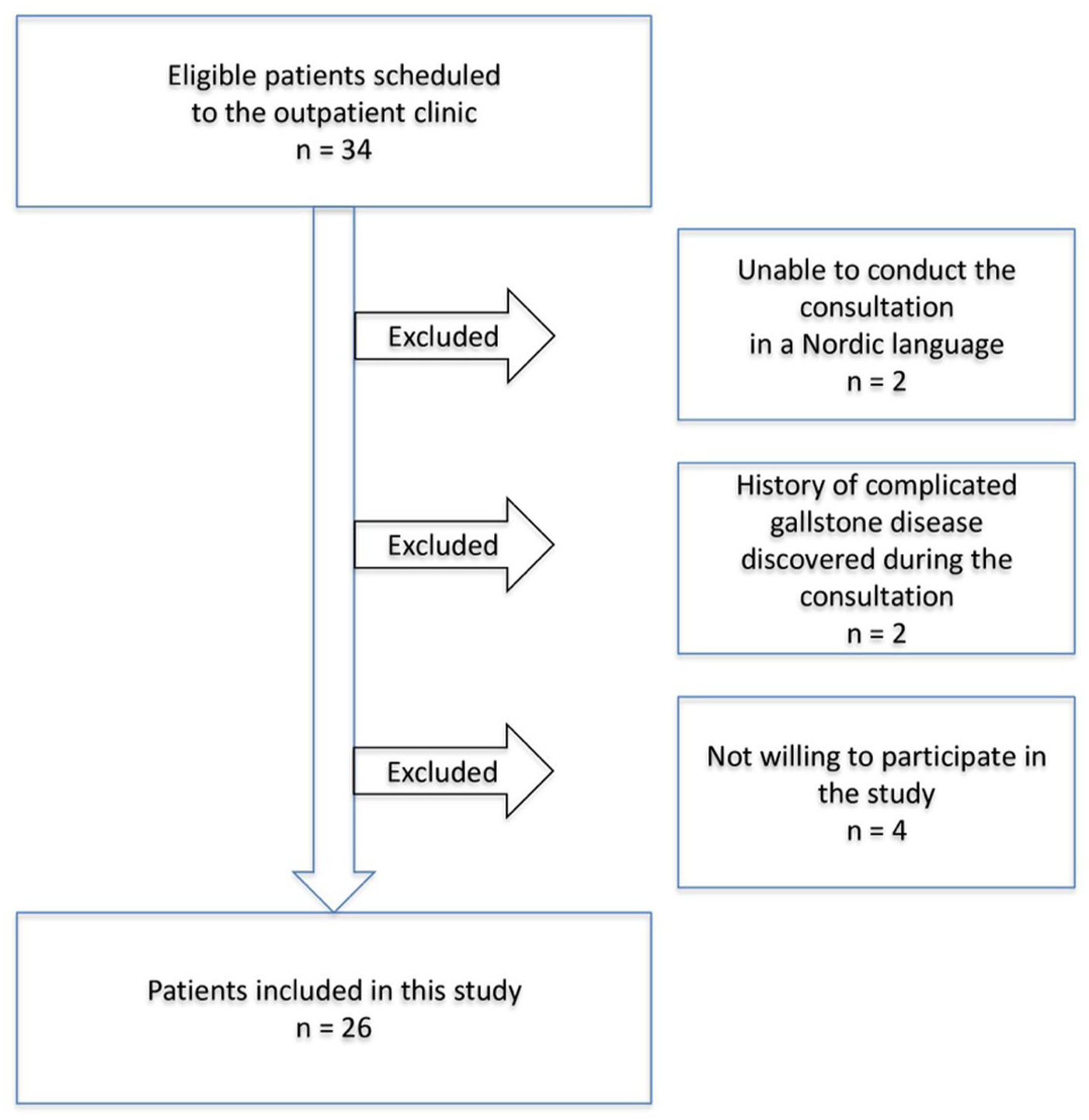
Flowchart of included and excluded patients in a cross-sectional pilot study of shared decision-making for establishing the indication for cholecystectomy for uncomplicated gallstone disease.
MAPPIN-SDM mean scores (0–4) for each of the nine domains and total score reported by the patient (n = 26), surgeon (n = 5), and observer (n = 2).
SDM scores showed a weak correlation between patients and observers (r = 0.37, p = 0.04), a moderate correlation between patients and surgeons (r = 0.60, p = 0.001), and a strong correlation between surgeons and observers (r = 0.70, p < 0.001).
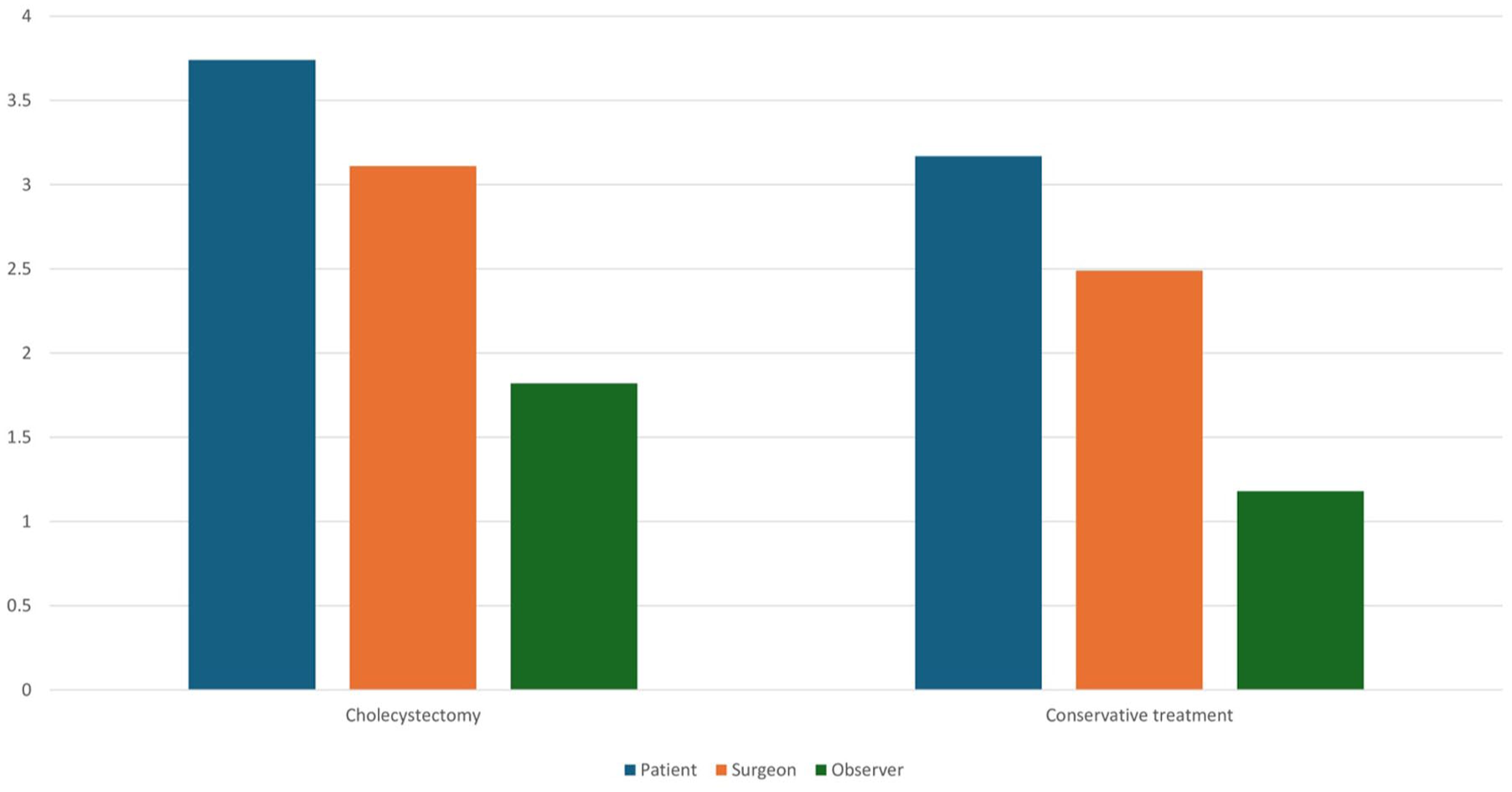
Patients who underwent surgery (14 participants, 54%) had a higher total mean MAPPIN-SDM score compared to those who did not (2.89 versus 2.28; p < 0.001) (Fig. 4). In addition, greater patient involvement was positively correlated with the strength of the surgeon’s preference toward cholecystectomy (r = 0.67; p < 0.001).
MAPPIN-SDM mean scores (0–4) among patients undergoing cholecystectomy (n = 14) and conservative treatment (n = 12) scored by the patient, surgeon, and observer.
Discussion
The main finding of this cross-sectional pilot study was that although patients and surgeons reported a high level of SDM, the expert observers reported a low level of patient involvement in decision-making about treatment of uncomplicated gallstone disease. The only previous study evaluating SDM in this population used patient reports with questionnaires and semi-structured interviews. 21 Patients reported a high level of SDM when responding to questionnaires. However, in interviews, they indicated a lower level of SDM. This supports our finding that patients may overestimate their involvement when assessing SDM through questionnaires. Based on this and the previous study on this topic, SDM appears to be low in consultations for uncomplicated gallstone disease when assessed with an expert observer or interviews. 21 However, the evidence is still too limited to draw any firm conclusions.
In this study, the lowest SDM scores were for the domains “key message,” “alternatives,” and “meta-communication,” highlighting specific targets for improvement. These findings suggest that implementation of SDM training should focus on areas such as explicitly articulating the key message and providing the patient with a clear invitation to participate. Information support aids could be useful to help present the treatment alternatives. 30 In addition, increased SDM awareness and knowledge among surgeons could be useful to increase patient involvement in the treatment of uncomplicated gallstone disease.
This study revealed important differences in how SDM is perceived in uncomplicated gallstone disease consultations. Patients reported significantly higher levels of involvement than documented by expert observers. Notably, surgeons’ ratings aligned more strongly with expert observations (r = 0.70) than with patients’ ratings (r = 0.37). This pattern aligns with findings from a comprehensive systematic review of SDM in surgery; self-reported SDM levels were high for patients (93%), while the objective assessments showed significantly lower scores of 7% to 39%. 31 Patients may rate their involvement more favorably due to social desirability bias or limited understanding of what constitutes SDM or optimal SDM. MAPPIN-SDM is not specifically validated for patients with gallstone disease. The high patient scores may reflect a ceiling effect in the MAPPIN-SDM patient reports for this population. A ceiling effect occurs when mean scores are so high that the instrument cannot effectively distinguish between high and low scorers. 32 In contrast, external observers, using standardized quality criteria, often identify gaps in the SDM process that may not be apparent to the direct participants. The expert observations are more likely to give an accurate description of SDM. This study should encourage the development of questionnaires that measure patient-reported SDM more accurately, specifically addressing the ceiling effect.
This study showed increased SDM among patients undergoing surgery compared to those continuing with conservative treatment. In addition, the extent of patient involvement was positively associated with the strength of the surgeon’s preference toward cholecystectomy. This is contrary to previous reports, often reporting a tendency toward less invasive treatment choices when patients are involved in the decision. 30 In a systematic review and meta-analysis of a variety of surgical procedures, 8 of 12 studies reported reduced surgery rates with increased SDM. However, the meta-analysis reported no significant difference. 18
We have no explanations for this based on the data in this study. However, we can speculate that both surgeons’ and patients’ expectations and preferences can play a role. This should be in the scope of future studies on SDM in consultations for uncomplicated gallstone disease.
The main strengths of this study were the use of patient, surgeon, and expert observers; validated questionnaires; and the high participation rate (87%). Our study has important limitations. The small sample size of both surgeons (n = 5) and patients (n = 26), combined with recruitment at a single center, limits the generalizability of our findings. This sampling approach might have selected more motivated participants, potentially overestimating SDM implementation in routine clinical practice. Moreover, the inclusion of consultations from only five surgeons with varying experience levels (2–7 years) over five specific days may also limit generalizability. While this variation reflects real-world clinical settings, future studies should include more surgeons over a longer period to better account for individual differences in consultation style and SDM implementation. Awareness of being video recorded during the consultations might have altered natural communication patterns between surgeons and patients, potentially inflating SDM behaviors. Unfortunately, this method was necessary to enable objective assessment of SDM implementation through external observation. Moreover, observation without patient consent would be ethically unacceptable. Given the relatively low observer-rated SDM scores, we believe this Hawthorne effect/observer effect did not substantially impact our findings. 33 Social desirability bias in self-reported measures represents another limitation. Participants may have reported higher SDM engagement than they experienced, as evidenced by the discrepancy between self-reported and observer-rated scores.26,34 As previously discussed, this is a common challenge in SDM research. To mitigate its impact, we used anonymous questionnaires and validated measurement tools. Finally, other patient characteristics not included in the study may have influenced surgical decision-making, although most likely not to a greater extent, as serious morbidity excluded patients from being considered for surgery.
Conclusion
This study revealed important differences in how SDM is perceived in uncomplicated gallstone disease consultations. Patients reported higher levels of SDM compared to expert observers. These findings highlight the need for structured SDM implementation and training in clinical practice and the development of questionnaires that measure patient-reported SDM more accurately.
Footnotes
Acknowledgements
A special thanks to Eva Milch and the rest of the staff at the outpatient clinic at Oslo University Hospital for making this study possible. Thanks to all the participants.
Author contributions
M.A.T., S.K., T.F., M.F., T.G., T.M., and J.K. contributed to the conceptualization and study planning.
M.A.T., S.K., and J.K. contributed to the data collection.
M.A.T. contributed to the statistical analysis.
M.A.T., S.K., T.F., M.F., T.G., T.M., and J.K. contributed to the data interpretation.
M.A.T. and S.K. contributed to drafting the manuscript.
T.F., M.F., T.G., T.M., and J.K. contributed to the revision of manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
All participants obtained informed written consent, and the study was approved by the local data protection had no objections related to the study (23/04665).