
Abstract
Background and Aims:
Undetected cancers and fecal contamination in perforated diverticulitis may lead to failure of laparoscopic lavage. This study aimed to evaluate the diagnostic accuracy of preoperative computed tomography (CT) examinations and the interobserver agreement for detecting colonic malignancy and fecal contamination in patients with perforated diverticulitis.
Methods:
This study included 198 patients with suspected perforated diverticulitis from the SCANDIV trial, randomized to laparoscopic lavage or primary resection. CT examinations of all patients were independently reviewed by two specialists in abdominal radiology, and features of fecal contamination and colonic malignancy were registered and compared to the surgical reports.
Results:
At surgery, fecal contamination was described in 33 patients and was diagnosed on CT in 7 of those by both radiologists (sensitivity = 21%, specificity = 96%, positive predictive value (PPV) = 50%, and negative predictive value (NPV) = 86%) and in 25 patients by at least one of the radiologists (sensitivity = 76%, specificity = 63%, PPV = 29%, and NPV = 93%). Interobserver agreement between radiologists was 64% for fecal contamination (kappa = 0.18, SE = 0.05; p < 0.001). In 7 of 12 patients who turned out to have colon cancer, this was suspected at CT by at least one radiologist (sensitivity = 58%, specificity = 91%, PPV = 29%, NPV = 97%). Interobserver agreement between radiologists for suspected colonic malignancy was 92% (kappa = 0.46; SE = 0.12; p < 0.001).
Conclusion:
In this selected cohort of patients with suspected perforated diverticulitis, re-evaluation of CT scans proved unreliable for detecting malignancies and fecal contamination. This suggests that preoperative CT cannot replace follow-up colonoscopy or colonography following laparoscopic lavage.
Keywords
Context and Relevance
This study evaluates the diagnostic accuracies and interobserver agreement of CT imaging in perforated diverticulitis, using the operative report as the reference standard. The assessment focused on fecal contamination, abscess, and suspected colonic malignancy.
Introduction
Perforated diverticulitis is a common entity affecting 3–4 out of 100,000 individuals annually in Western countries.1 –3 About 30%−50% of these patients require emergency surgery, which carries a mortality rate of about 10%−20%.4 –6 Historically, emergency surgery has been the standard treatment for complicated diverticulitis with pneumoperitoneum. However, recent studies have shown that conservative management is often safe and feasible.7,8
Advances in computed tomography (CT) have improved the detection of small air bubbles outside of the colonic wall, which were previously missed, especially in patients with mild symptoms.9,10 Despite all improvements in radiology, the decision to operate is still primarily based on the clinical findings, with peritonitis or septicemia often being the decisive factors for emergency surgery.
The American Society of Colon and Rectal Surgeons has traditionally recommended emergency surgery for perforated diverticulitis with peritonitis,11,12 but the latest guideline allows for a conservative approach in highly selected, stable patients. 13 European surgeons, especially in Scandinavian countries, tend to use more conservative management for hemodynamically stable, immunocompetent patients.14,15
The SCANDIV trial was a multicenter randomized controlled study including patients from 21 centers in Norway and Sweden between February 5, 2010, and June 28, 2014. Patients requiring emergency surgery for perforated diverticulitis were randomized to either laparoscopic lavage (n = 101) or primary colonic resection (n = 98). 16 Of the 199 patients included, 25 were diagnosed with a hollow viscous perforation other than left-sided perforated diverticulitis upon abdominal inspection (six suspected colon tumor perforations, four perforated peptic ulcers, four benign right-sided colonic perforations, four unidentified perforations, two ischemic colitis, three small bowel perforations, one perforated appendicitis). The study revealed no statistical difference in severe complications at 90-day and one-year follow-ups.16 –18 However, the laparoscopic lavage group had higher early reintervention rates, and some sigmoid tumors were missed during laparoscopy.
The aim of this post hoc analysis was to assess diagnostic accuracy and the interobserver agreement of preoperative CT examinations compared to surgical findings in patients with perforated diverticulitis. The focus was particularly on detecting colon malignancy and fecal contamination.
Methods
Consent
The SCANDIV trial (clinicaltrails.gov nr: NCT01047462) and this post hoc explorative analysis was approved by the regional committee for medical and health research ethics in southeastern Norway (reference number 2009/177) and by the regional ethical review board in Stockholm, Sweden (protocol 2010/3:2, number 2010/113-31/3). Written, informed consent was obtained from all patients.
Patients
Patients older than 18 years with clinical and radiological signs of perforated diverticulitis needing surgical intervention were included in the SCANDIV trial. 16 As a part of the monitoring in the SCANDIV trial, all CT scans and operative reports were collected. This post hoc analysis included all patients with for whom the preoperative CT scan and the operative report were available.
Variables
Baseline characteristics included age, sex, body mass index (BMI), previous abdominal surgery, previous episodes of diverticulitis, comorbidity, risk factors, American Society of Anesthesiologists (ASA) physical score, and Charlson Comorbidity Index (CCI) score.
Re-evaluation of operative reports
The operative reports were re-evaluated by two surgeons (J.K.S. and A.C.), and in case of discrepancies, arbitration was done by a referee (TÖ). All three are experienced colorectal surgeons with more than 15 years’ experience in colorectal surgery who participated in the SCANDIV study. The following parameters were recorded and classified: presence and location of macroscopic acute diverticulitis, visible hole in the colon at inspection, signs of obstruction, presence of fibrin exudate, presence and location of abscess, presence and distribution of free fluid or fecal contamination (localized if in one or two of the four abdominal quadrants or pelvis, and generalized if present in three or more of these five regions), and macroscopically suspected colonic malignancy. The original operative report did not have a structured form of reporting findings. Factors not mentioned in the operative report were interpreted as not present.
Re-evaluation of CT examinations
Two radiologists (L.T.B., A.T.) independently re-evaluated the preoperative CT examinations of the included patients. Both radiologists have more than 10 years’ experience in evaluating abdominal CT. Both were blinded to the initial radiological evaluation, clinical data, and operative outcome as well as to each other’s reports. The CT acquisitions were adapted to clinical presentation and according to local CT protocols in 21 different radiology units (9 in Sweden and 12 in Norway). The re-evaluation was performed according to a structured form which covered the following items: main tentative diagnosis (diverticulitis/cancer/other perforation), presence of colon diverticula, presence of inflamed diverticula, other signs of inflammation (wall thickening, fat stranding), presence of abscess and its location, presence and distribution of extraluminal air (“localized” if <5 cm from the inflamed colonic segment or “generalized” if >5 cm), presence and distribution of free fluid, fecal contamination (visible fecal matter outside the bowel), and signs of malignancy (suspected colon cancer, shouldering, obliteration of diverticula, suspected malignant lymph nodes).
Statistics
The sample size was given by the number of patients included in the SCANDIV trial with available CT scans and operative reports. A statistical analysis plan was made when designing the structured forms for re-evaluation of the CT examinations and the operative reports. All statistics were descriptive. The diagnostic accuracies of CT were calculated separately for each radiologist and for combinations of the two readers (“at least one” and “both”) with the arbitrated re-evaluation of the operative reports as the reference standard. Interobserver agreement was reported as Cohen’s kappa (κ) and percent agreement. Kappa values were interpreted according to Landis and Koch as “slight” (0–0.2), “fair” (0.21–0.40), “moderate” (0.41–0.60), “substantial” (0.61–0.80), and “almost perfect” (0.81–1.0). 19 The statistical analysis was done with IBM SPSS Statistics version 28.01.
Results
Of 199 patients included in the SCANDIV trial, one patient was erroneously included without written consent which left a total of 198 patients. The baseline characteristics including CCI and preoperative ASA score of the included patients are displayed in Table 1. The operative report was missing for three patients, as seen in Fig. 1.
Baseline characteristics of patients included in SCANDIV.
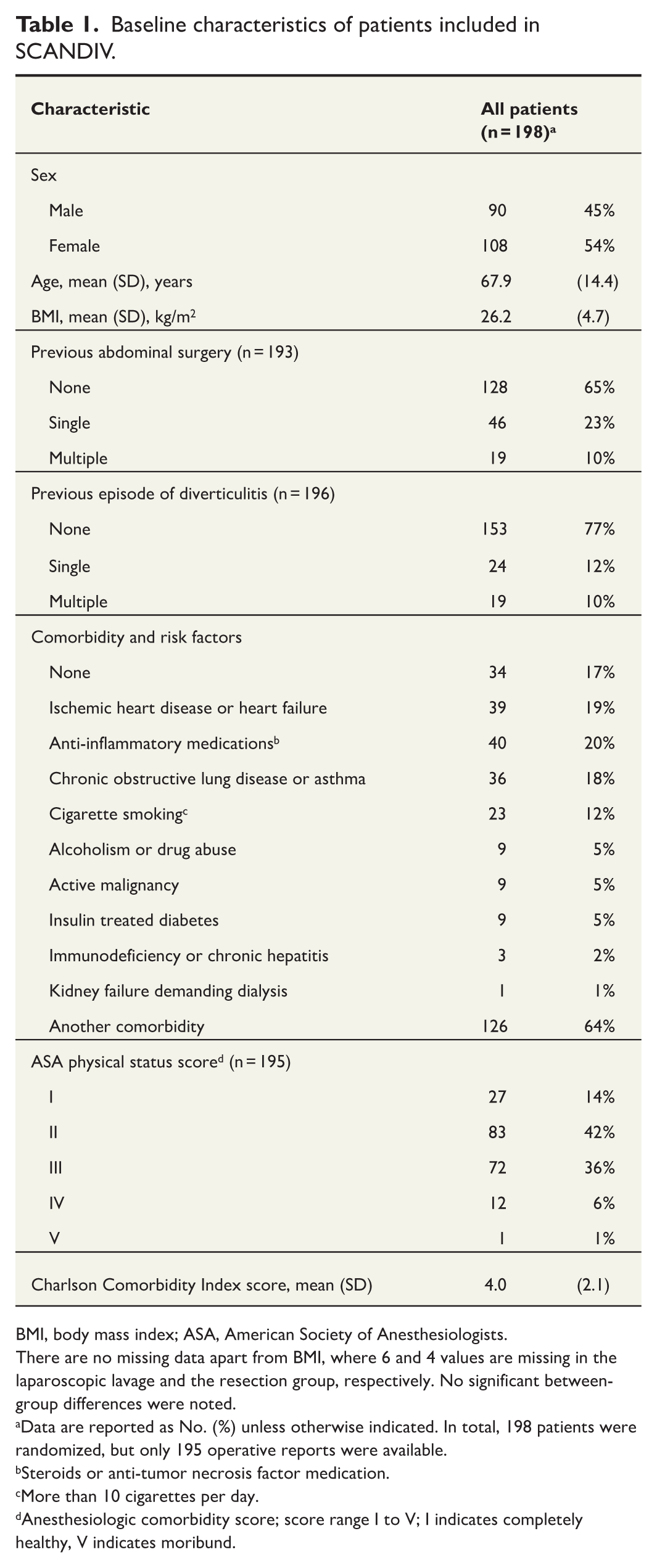
BMI, body mass index; ASA, American Society of Anesthesiologists.
There are no missing data apart from BMI, where 6 and 4 values are missing in the laparoscopic lavage and the resection group, respectively. No significant between-group differences were noted.
Data are reported as No. (%) unless otherwise indicated. In total, 198 patients were randomized, but only 195 operative reports were available.
Steroids or anti-tumor necrosis factor medication.
More than 10 cigarettes per day.
Anesthesiologic comorbidity score; score range I to V; I indicates completely healthy, V indicates moribund.
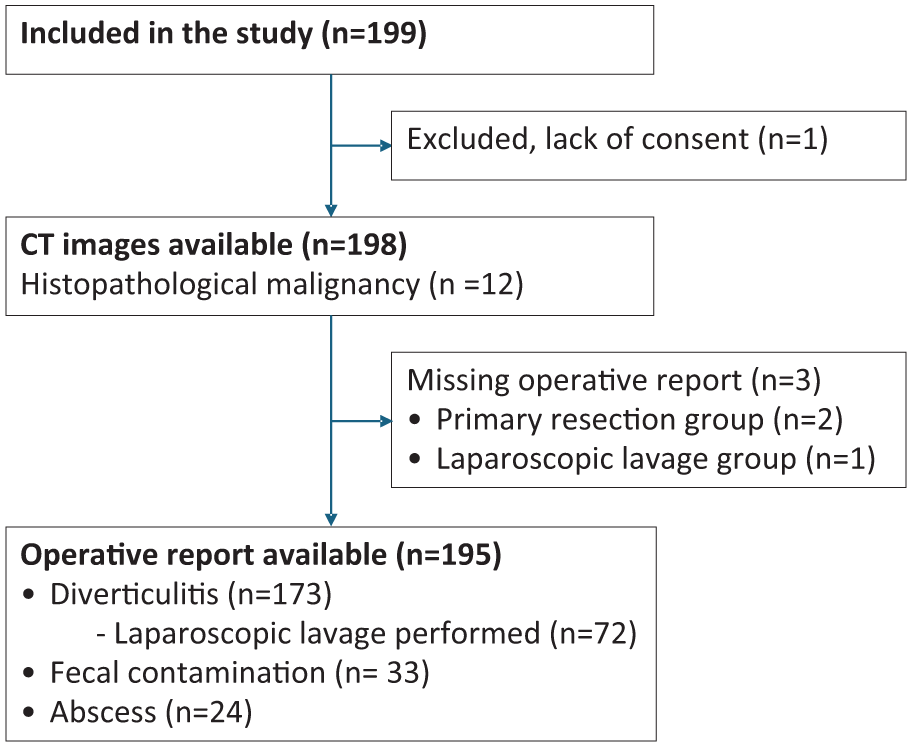
Flowchart of the cohort.
Comparison of the radiological findings with intraoperative and pathology reports
The diagnostic accuracies of each radiologist, at least one radiologist, and both radiologists are shown in Table 2.
Sensitivity, specificity, and positive and negative predictive values for the radiologists’ image interpretation.
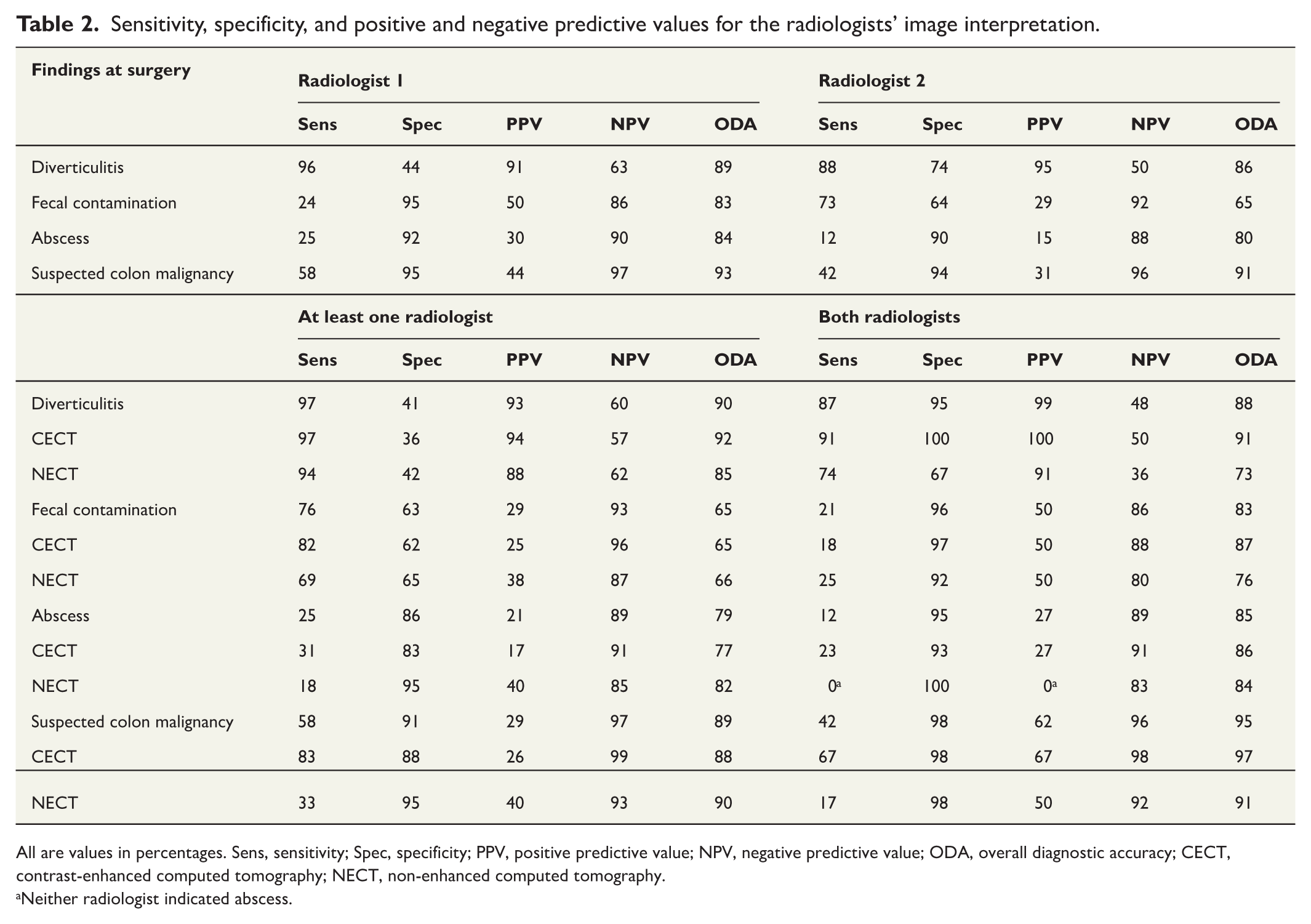
All are values in percentages. Sens, sensitivity; Spec, specificity; PPV, positive predictive value; NPV, negative predictive value; ODA, overall diagnostic accuracy; CECT, contrast-enhanced computed tomography; NECT, non-enhanced computed tomography.
Neither radiologist indicated abscess.
After arbitration, the operative report indicated an intraoperative diagnosis of diverticulitis in 173 of 195 patients (89%). The respective positive predictive values (PPVs) of the two radiologists were 91% and 95%.
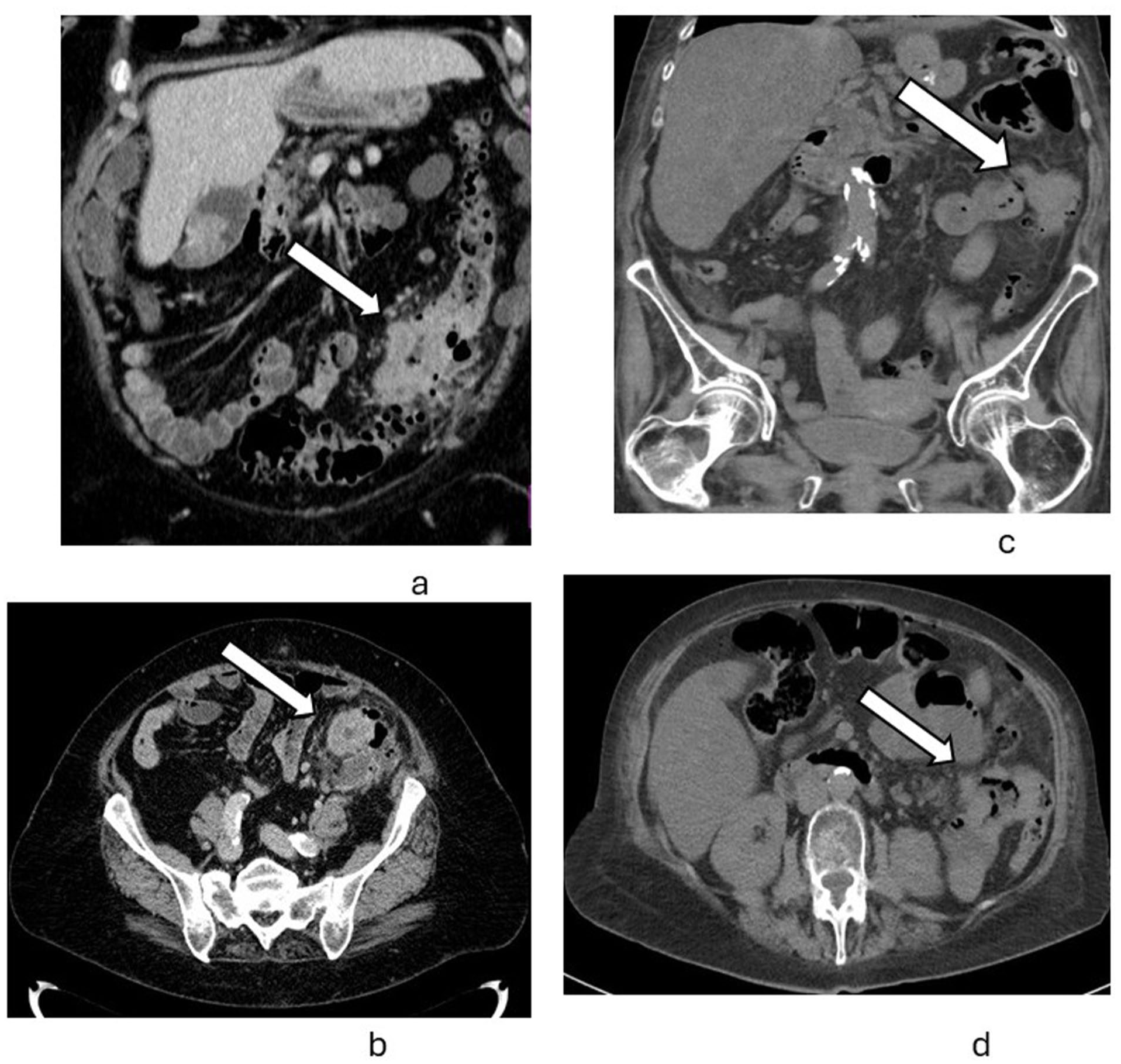
The operative reports indicated complications with fecal contamination in 33 and abscess in 24 patients (Table 3). For fecal contamination, the sensitivity was 24% and 73%, and the negative predictive values (NPVs) were 86% and 92%. For abscess, the sensitivity was 25% and 12%, and the NPVs were 90% and 88% for the individual radiologists. Fig. 2A, B (insert Fig. 2) shows a false negative CT for fecal contamination, and Fig. 2C, D shows a true positive. In 12 patients, a histologically verified colon malignancy was found either at the index operation or at reoperation. For colon malignancy, the sensitivities of the two radiologists individually were 58% and 42%, the specificities were 95% and 94%, the PPVs were 44% and 31%, and the NPVs were 97% and 96%, respectively. Fig. 3A, B shows a true positive CT for malignancy diagnosed with preoperative CT by both radiologists. Fig. 3C, D shows a false negative CT for malignancy not found radiologically but intraoperatively. In seven out of twelve patients who turned out to have a histologically verified colon cancer, this was suspected by at least one radiologist (sensitivity = 58%, specificity = 91%, PPV = 29%, NPV = 97%).
Operative report, interobserver agreement.
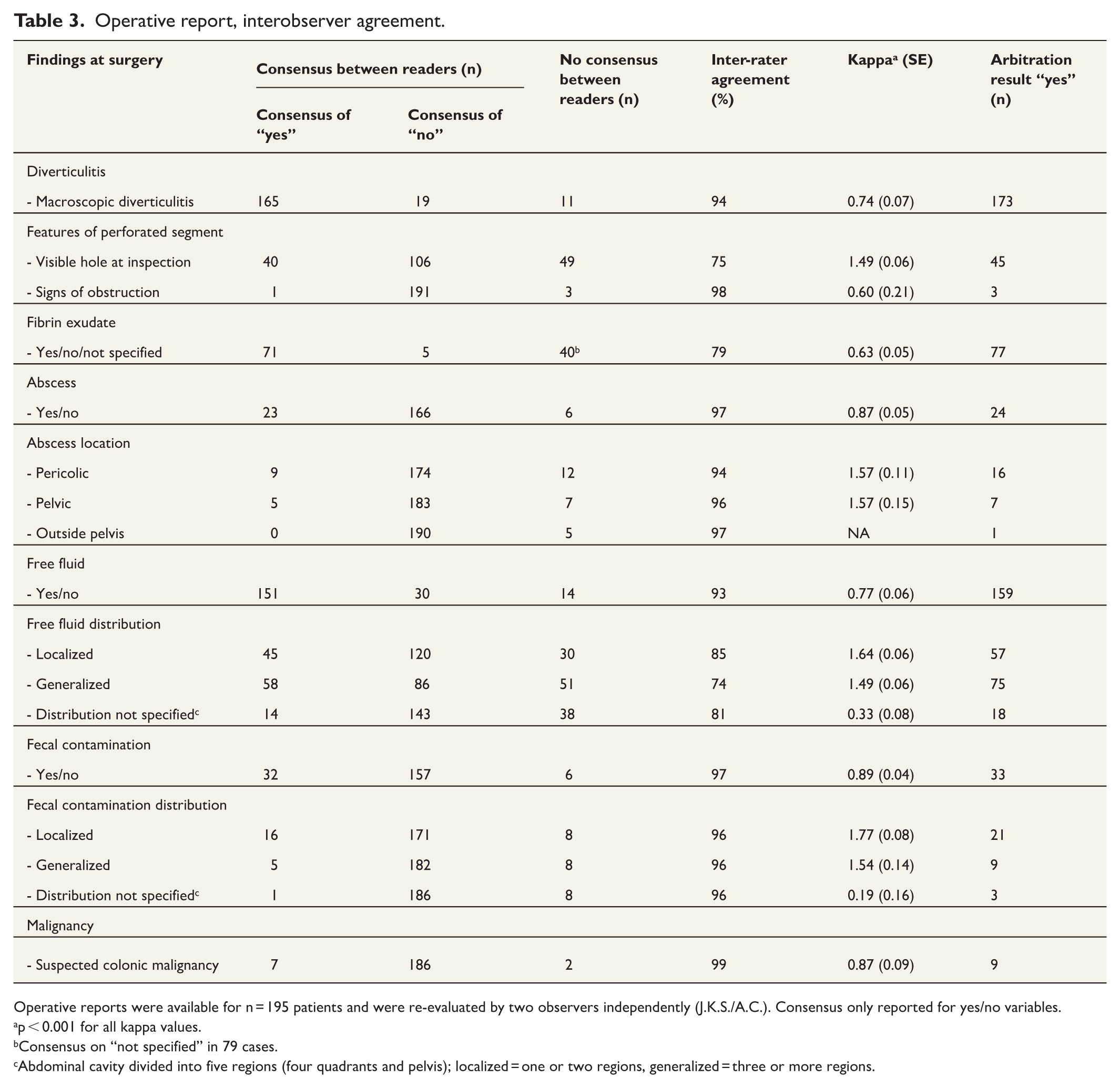
Operative reports were available for n = 195 patients and were re-evaluated by two observers independently (J.K.S./A.C.). Consensus only reported for yes/no variables.
p < 0.001 for all kappa values.
Consensus on “not specified” in 79 cases.
Abdominal cavity divided into five regions (four quadrants and pelvis); localized = one or two regions, generalized = three or more regions.

False negative fecal contamination (A and B) and true positive fecal contamination (C and D).
True positive malignancy (A and B) and false negative malignancy (C and D). Images A and B show a contrast-enhancing wall thickening in the sigmoid colon, and colon malignancy was suspected by both radiologists. In the initial clinical workup, this tumor was missed by the radiologist, and the lesion in the gallbladder was flagged as a tumor. Surgery revealed no tumor in the gall bladder but a tumor in the sigmoid colon. (C) and (D) show a tumor in the left colon that was missed by both radiologists in this non-enhanced CT.
Contrast-enhanced CT versus non-enhanced CT
Contrast-enhanced CT (CECT) was performed in 128 patients and non-enhanced CT (NECT) in 67 patients. In the Norwegian part of the cohort, 80 out of 104 CT examinations (77%) were CECT compared to 48 out of 91 (53%) in the Swedish part of the cohort. On CECT, five out of six cases of colon malignancy (83%) were suspected by at least one radiologist compared to two out of six cases (33%) on NECT. At surgery, abscess was found in 24 patients. Four out of thirteen cases of abscess (31%) were diagnosed by at least one radiologist on CECT compared to two out of 11 cases (18%) on NECT. Fecal contamination was found in 33 patients at surgery. In total, 14 out of 17 cases (82%) of fecal contamination were detected by at least one radiologist on CECT, compared to eleven out of 16 (69%) on NECT.
Operative report, interobserver agreement
As shown in Table 3, the interobserver agreement between surgeons 1 and 2 for evaluation of all variables in the operative report ranged from slight to almost perfect (κ: 0.19–0.89, agreement: 74%−99%). An almost perfect agreement was seen for presence of abscess (κ: 0.87, agreement: 97%), presence of fecal contamination (κ: 0.89, agreement: 97%), and macroscopically suspected colonic malignancy (κ: 0.87, agreement: 99%). Variables with substantial agreement were the presence of macroscopic diverticulitis (κ: 0.74, agreement: 94%) and free fluid (κ: 0.77, agreement: 93%). There was generally higher agreement on the presence of free fluid, fecal contamination, and abscess, than their distribution or location.
Radiological findings, interobserver agreement
The interobserver agreement between radiologists 1 and 2 ranged from slight to substantial (κ: 0.08–0.74, agreement: 58%−99%), as shown in Table 4.
Radiological data with consensus between readers on yes/no values.
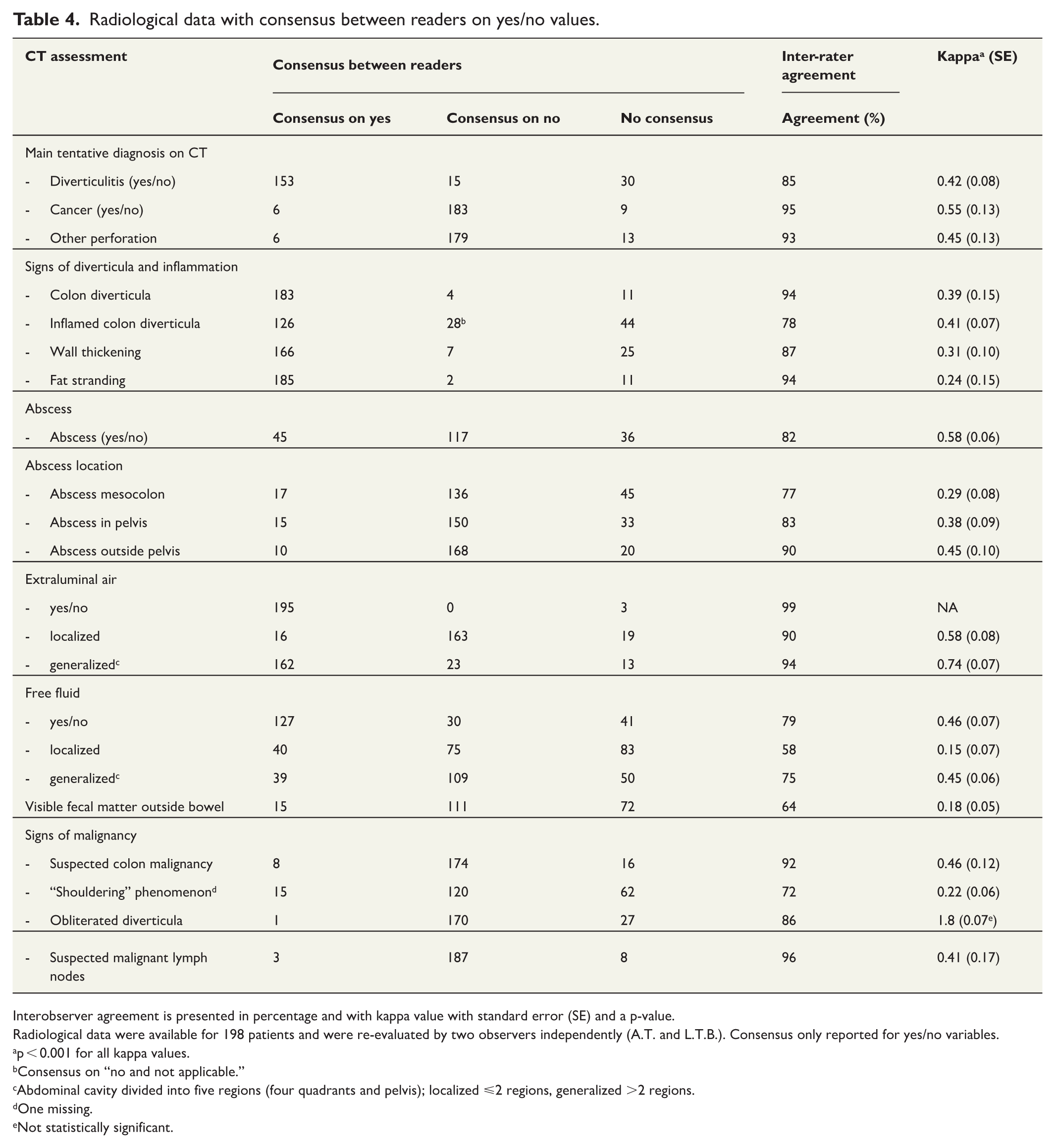
Interobserver agreement is presented in percentage and with kappa value with standard error (SE) and a p-value.
Radiological data were available for 198 patients and were re-evaluated by two observers independently (A.T. and L.T.B.). Consensus only reported for yes/no variables.
p < 0.001 for all kappa values.
Consensus on “no and not applicable.”
Abdominal cavity divided into five regions (four quadrants and pelvis); localized ⩽2 regions, generalized >2 regions.
One missing.
Not statistically significant.
Interobserver agreement was moderate for the main diagnosis: diverticulitis (κ: 0.42, agreement: 85%), cancer (κ: 0.55, agreement: 95%), and other perforation (κ: 0.45, agreement: 93%). There was moderate agreement for presence of abscess (κ: 0.58, agreement: 82%), free fluid (κ: 0.46, agreement: 79%), and for suspected colon malignancy (κ: 0.46, agreement: 92%). Interobserver agreement for visible fecal matter outside of bowel was slight (κ: 0.18, agreement: 64%).
Reoperations within index admission
A total of 72 patients underwent with laparoscopic lavage. Of these, 10 required reoperations within 90 days of index operation due to septic complications, such as secondary peritonitis, abscess, or drainage failure. In four of these cases, at least one radiologist noted visible fecal matter outside the bowel, and in one case, the presence of an abscess was indicated.
Abscess and risk of colonic malignancy
There were 12 cases of colonic malignancy in our cohort of 198 patients, suggesting a 6% risk of colon malignancy in perforated diverticulitis. In a group of 11 patients, in which both radiologists indicated the presence of abscess, there were two colonic malignancies, suggesting a risk of 18% (2 out of 11) in diverticulitis with abscess. In the remaining 187 patients, who had no abscess or no consensus of abscess, there were 10 cases of colonic malignancy, suggesting a risk of 5% in this group.
Discussion
In this explorative post hoc study of the SCANDIV trial, we evaluated 198 CT scans and corresponding operative reports from 195 patients. Independent interpretations by two experienced radiologists showed the overall diagnostic accuracy on the suspicion of colon malignancy was >90% with moderate agreement (κ: 0.46, agreement: 92%). For fecal contamination, there was low overall diagnostic accuracy for both readers (65% and 83%, respectively) and only slight agreement (κ: 0.18, agreement: 64%).
With the increasing reliance on CT scans in modern practice and advancement in radiological technology, there is a tendency to expect intraoperative findings to closely match radiological interpretations.19 –21 Although CT technology may have advanced since the initial patients were included in this trial, we believe the scanners and acquisition protocols used are representative of current clinical practice. In this study, we found a moderate overall diagnostic accuracy of CT for diagnosing fecal contamination, which varied considerably between radiologists (65% vs. 83%). Consequently, the readings of the CT scans alone could neither have been relied upon to guide the decision between conservative or operative management, nor to anticipate intraoperative findings.
In our cohort, 12 patients (6%) turned out to have a colon malignancy. In a retrospective study of 633 patients with diverticulitis, Sallinen et al. 20 reported that 16 out of 17 cases of colon malignancy were found in patients with concomitant abscess, indicating an 11.4% cancer risk in this group. In comparison, we found an 18% (2 out of 11) cancer risk associated with abscess, but the majority of cancers were found in patients without abscess, with a cancer risk of 5% (10 out of 187) in this group. Our radiologists identified 5 and 7 out of the 12 colon malignancies, respectively. Although they achieved relatively high diagnostic accuracies (> 90%) for colon malignancy compared to the previously reported 67%, their sensitivity was low (42% and 58%, respectively) and the interobserver agreement was moderate (κ: 0.46, agreement: 92%).20,21 In our opinion, these results underpin the recommendation of a colon examination following all episodes of conservatively treated complicated diverticulitis.13,14,22
Radiological signs such as the “shouldering phenomenon,” obliterated diverticula, or enlarged locoregional lymph nodes may suggest malignancy. Agreement between the radiologists was fair for shouldering phenomenon (κ: 0.22, agreement: 72%), slight for obliterated diverticula (κ: 0.08, agreement: 86%), and moderate for suspected malignant lymph nodes (κ: 0.41, agreement: 96%). This highlights the complexity of differentiating between diverticulitis and malignancy in acute settings, as even these radiological findings are unreliable. The difficulties in differentiating tumor from diverticulitis were also demonstrated in a previous study by Grahnat et al. 21 who identified only one out of six cancers on CT and had a false positive rate of 67% (2 out of 3). Valletta et al. 21 demonstrated that CT colonography (virtual colonoscopy) might aid in distinguishing between diverticular disease and malignancy in patients with chronic diverticular disease. 22 However, this technique is usually discouraged in emergency settings due to the risk of bowel perforation from the gas insufflation.
In the SCANDIV trial, the CT examinations were performed in multiple hospitals, with varying acquisition protocols. NECT was generally more common in Sweden (47%) compared to Norway (23%). We found a considerably lower sensitivity and NPV on NECT compared to CECT for suspected colon malignancy and abscess, although the results for fecal contamination were less clear. These results indicate that a surgeon should not put too great emphasis on an NECT excluding these conditions, even though the differences in overall diagnostic accuracy were less convincing (Table 2). Hence, it is our opinion that CT performed for suspected diverticulitis should be contrast enhanced to better rule out these conditions, unless there is a compelling reason to abstain from contrast media.
This study has several limitations. It was not designed to evaluate the general diagnostic accuracy of abdominal CT in emergency settings due to the highly selected study population. Thus, the diagnostic accuracy measures are only applicable to patients with suspected perforated diverticulitis and free air on a CT scan. Despite independent re-evaluation by two experienced colorectal surgeons, the low kappa values for several items, such as distribution of free fluid and fecal contamination (Table 3), suggest that many operative reports may be incomplete or difficult to interpret, partly due to the lack of standardization. Standardized reporting of surgical procedures could improve the content of operative reports for both clinical work and research. 23 Another limitation is the retrospective re-evaluation of the operative reports and CT examinations. It is unclear how the retrospective evaluation of CT examinations may have influenced diagnostic performance compared to initial radiology reports. However, it was impossible to extract the necessary data from the original CT reports since they did not follow a structured template. Hence, an independent retrospective evaluation by two radiologists was our best option. One could argue that a structured CT report should have been part of the main study. There is evidence from other diagnoses that structured CT reporting has the potential to improve diagnostic accuracy. 24
The main strength of the SCANDIV trial is its randomized design, including patients with perforated diverticulitis in emergency settings. As CT was part of the inclusion criteria, all patients were examined with CT, and nearly all CT scans and operative reports were available for re-evaluation. Another strength is the multicenter design, providing a realistic picture of current medical practice.
In this explorative post hoc study in a selected cohort of patients with suspected perforated diverticulitis, re-evaluation of CT scans proved unreliable for detecting malignancies and fecal contamination. This suggests that preoperative CT cannot replace follow-up colonoscopy or colonography following laparoscopic lavage.
Footnotes
Acknowledgements
We thank all participants in the SCANDIV study group and all previous co-authors of the SCANDIV publications for their previous involvement, which made this study possible.
Author contributions
J.K.S. and J.S. were co-authors and had full access to the data in the study and took responsibility for the integrity of the data and accuracy of the data analysis. All authors contributed to the conceptualization, methodology, and writing of the manuscript, as well as the review and editing. L.T.B. and A.T. were part of the investigation and data curation. P.M.L. and T.Ö. supervised the project. All authors approved of the manuscript before publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The original SCANDIV study was funded with a fellowship to Johannes Kurt Schultz by the South-Eastern Norway Regional Health Authority (PNR 2719011) and additional research funding from Akershus University Hospital in Norway for running expenses (PNR 2619041, 2629038, and 2649054). The current post hoc study received no external funding.
Ethics approval statement
The SCANDIV trial and this post hoc analysis were approved by the regional committee for medical and health research ethics in southeastern Norway (reference number: 2009/177) and by the regional ethical review board in Stockholm, Sweden (protocol 2010/3:2, number 2010/113-31/3).
Patient consent statement
Written, informed consent was obtained from all patients.
Permission to reproduce material from other sources
Not applicable.