
Abstract
Background:
Superparamagnetic iron oxide (SPIO) nanoparticles are non-inferior as a tracer for sentinel lymph node biopsy (SLNB) detection in breast cancer patients compared to the standard radioactive tracer (technetium-99m, Tc99m) with or without blue dye (Patent blue V®, BD). Sentinel lymph node (SLN) detection has been successful using an ultra-low dose of 0.1 mL SPIO injected intradermally in patients with breast cancer, and this study aims to assess the potential reduction of SPIO-related skin discoloration and breast magnetic resonance imaging (MRI) artifacts at 6 and 12 months after breast-conserving surgery using the ultra-low dose of SPIO.
Method:
Skin discoloration and MRI artifact were pre-planned endpoints in the prospective MAGSNOW feasibility study. MRI follow-ups were scheduled 6 and 12 months after surgery, and MRI artifacts were classified into six grades. SPIO-induced skin discoloration was assessed at baseline, 1, 6, and 12 months by photography.
Results:
Thirty-six patients had 6- and 12-month MRI follow-up performed, revealing no MRI artifacts impairing breast assessment. At 12 months, 75.0% (27/36) of the patients had minimal MRI artifacts, primarily in the subcutaneous tissue, or <5 mm in the fibro-glandular tissue. At 12 months, 54% (27/50) of the patients had a skin discoloration with a median area of 0.79 cm2 (interquartile range (IQR) 0.14–1.41).
Conclusion:
An ultra-low dose of SPIO may offer a solution to the concerns of MRI artifacts and skin discoloration associated with the present recommended dose of 1–2 mL of SPIO.
Keywords
Introduction
Staging the axilla has a prognostic value for patients with breast cancer, and sentinel lymph node biopsy (SLNB) is currently the standard routine for nodal staging. 1 A common technique to identify the sentinel lymph node (SLN) is to use the combination of a radioactive tracer (technetium-99m, Tc99m) and a blue dye (Patent blue V®, BD). 2 The dependency of timely isotope delivery together with regulatory restrictions may, however, limit its use, and access in the global setting is challenging. In addition, Tc99m has a short half-life (6 h), which makes planning for surgery more challenging, 3 and BD has been linked to severe anaphylactic reactions reported in approximately 0.4% of the patients. 4
The SLN detection rate with Tc99m/BD is reported to be 98%–99% in patients with primary breast cancer. 5 Superparamagnetic iron oxide (SPIO) nanoparticles for SLN detection have been demonstrated to be non-inferior to the conventional Tc99m/BD technique.6,7 SPIO can be administered as an intradermal, peritumoral, subcutaneous, or subareolar injection in the breast.7,8 In addition, different timeframes for SPIO injection have been studied with successful detection of SLN more than four weeks after injection. 9 Two concerns have, however, been raised regarding using SPIO for SLNB, that is, skin discoloration and postoperative magnetic resonance imaging (MRI) artifacts in patients undergoing breast-conserving surgery (BCS).10–12 A recent systematic review and meta-analysis has suggested that an optimization of volume and injection site could potentially address the issue of staining and MRI artifacts. 13
The aim of this study was to evaluate if SPIO in an ultra-low dose of 0.1 mL administered intradermally can minimize SPIO-related skin discoloration and breast MRI artifacts following BCS. This report is a preplanned analysis of secondary endpoints from a previously reported prospective feasibility trial, which showed that SLNB was successful in all of the 50 included patients. 14
Methods
Study population and design
Fifty patients with histologically confirmed breast cancer and clinically node-negative axilla planned for BCS and SLNB were prospectively enrolled at Sahlgrenska University Hospital, Gothenburg, Sweden. All patients provided written informed consent. Exclusion criteria were age <18 years, body mass index (BMI) > 40 kg/m2, and contraindications for MRI, such as claustrophobia, metallic implants, internal electrical devices (e.g., pacemaker), and permanent makeup or tattoos, which, in the investigator’s opinion, might compromise the patient’s safety or imaging. Pregnancy or breastfeeding, iron overload disease, or known hypersensitivity to iron, dextran compounds, or BD were also contraindications. The study was approved by the Swedish Ethical Review Authority (dnr: 2021-02726) and the Swedish Medical Product Agency (dnr: 5.1-2021-41266), and a protocol synopsis was registered at clinicaltrials.gov (NCT05359783).
All patients received an intradermal injection of 0.1 mL SPIO within seven days of the day of surgery, either in the skin over the tumor or at the border of the areola, at the surgeon’s discretion. On the day of surgery, or the day before, Tc99m was injected peritumorally, whereas BD was optional to inject and was administered after the onset of anesthesia, but before skin incision, and the injection site was then separated from the SPIO injection. The protocol permitted the removal of discolored skin based on patient preferences.
MRI artifacts and follow-up
Imaging with MRI of the breasts was acquired on a 3 T MR scanner (Ingenia R5.7; Philips Healthcare, Best, The Netherlands) using a clinical routine protocol without intravenous contrast. Four sequences were generated: T1- and T2-weighted images derived from a turbo spin echo, fat-saturated T1-weighted high-resolution isotropic volume examination (THRIVE), and a short tau inversion recovery (STIR) sequence. The MRI artifacts in the operated breast were evaluated at 6 and 12 months (±1 month) after surgery. Artifacts extending into the fibro-glandular tissue (FGT) were evaluated in an axial plane, measuring from the subcutis to the deepest point in the FGT. Since no standard or validated scale is available to assess the extent of SPIO-related MRI artifacts, a six-level ordinal scale was created based on previous experience. The scale was developed through collaboration between two radiologists and three surgeons to ensure it was comprehensive, clinically relevant, and accounted for potential diagnostic limitations and practical constraints. Efforts were made to ensure the scale was straightforward to use in clinical practice or research settings while minimizing complexity without compromising diagnostic value.
Grade 0 = No artifacts
Grade 1 = Artifact visible in the subcutaneous tissue, good diagnostic quality
Grade 2 = Artifact <5 mm in FGT, good diagnostic quality
Grade 3 = Artifact 5–10 mm in FGT, readable with minimally impaired clinical assessment
Grade 4 = Artifact 11–30 mm in FGT, readable with a slightly impaired clinical assessment
Grade 5 = Artifact >30 mm in FGT, impaired clinical assessment
Intradermal injection technique
A very fine needle (26–35 gauge) was used with a 1 mL syringe loaded with 0.1 mL of SPIO. The target injection angle was 10°–20° to ensure accurate intradermal administration. Before the injection, the needle tip was positioned just beneath the skin surface (where the tip of the needle should be seen just under the skin), ensuring correct placement at the intradermal layer.
Skin discoloration and patient-reported outcomes
The size of the skin discolorations was measured and photo-documented at baseline, which is immediately after SPIO injection. Follow-up was scheduled at 1, 6, and 12 months after surgery. The potential skin discoloration was measured and photographed at each time point. The effect of a potential skin discoloration on patient-reported outcome was assessed by a non-validated modified version of the Skin Discoloration Impact Evaluation Questionnaire (SDIEQ) 12 months after surgery. 15 The survey contained a five-item skin discoloration impact evaluation questionnaire categorized into four levels (0 = not at all, 1 = a little, 2 = a lot, and 3 = very much) (Supplementary Information 1).
Residual magnetic counts
Residual transcutaneous magnetic counts at the breast injection site were measured postoperatively at 1, 6, and 12 months after surgery with a hand-held magnetometer (SentiMag®).
Statistical analysis
Descriptive values are reported as median, range, and interquartile range (IQR), or as numbers and percentages. The area of skin discoloration is provided in square centimeters (cm2). Chi-square test was performed to test the association between MRI artifact to the skin discoloration. Comparisons between skin discoloration at the different timepoints were conducted using the non-parametric Friedman’s test. If residual SPIO counts after surgery depended on whether the skin discoloration was removed or not was analyzed using Mann–Whitney U test.
Results
A total of 50 female patients with breast cancer were consecutively recruited from November 2021 to January 2023, with follow-up until January 2024. The median age was 63 years, and the median tumor size was 14 mm (Table 1). All patients received an ultra-low dose of 0.1 mL SPIO, a median of 4 days before surgery (range 1–9 days). Tc99m was used in all patients, and BD was injected in 26% (13/50) of the patients. No serious adverse events caused by Tc99m, BD, or SPIO were reported.
Patient and tumor characteristics in 50 women undergoing breast-conserving surgery and sentinel lymph node biopsy using 0.1 mL superparamagnetic iron oxide.
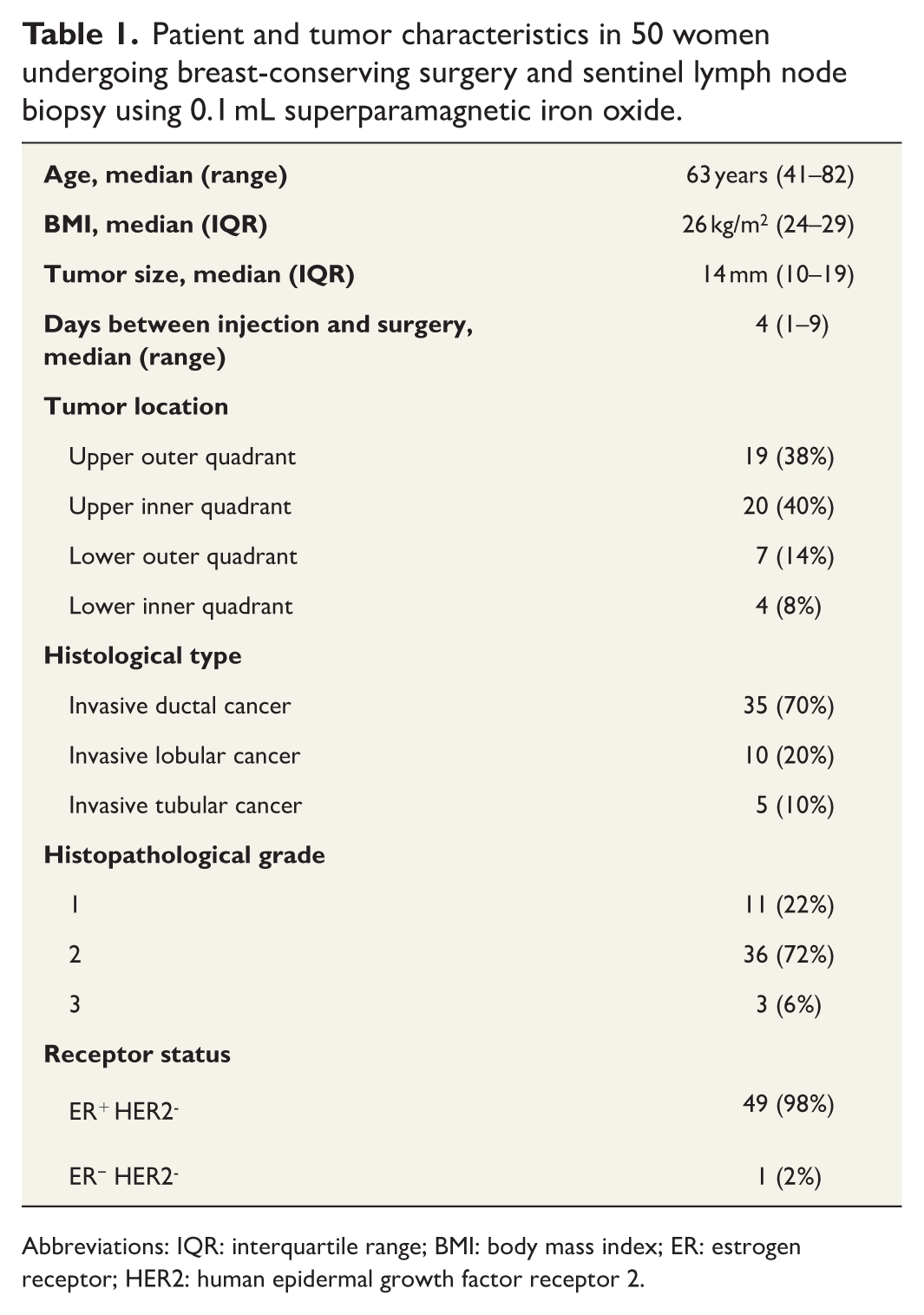
Abbreviations: IQR: interquartile range; BMI: body mass index; ER: estrogen receptor; HER2: human epidermal growth factor receptor 2.
MRI artifacts
The MRI follow-up was part of the secondary endpoint of the study. Among the 50 enrolled patients, 38 patients consented to MRI at 6 and 12 months after surgery. One patient participated in the 6-month MRI but, due to claustrophobia, did not take part in the 12-month MRI. Another patient was unable to take part in the 6-month MRI but underwent the 12-month MRI, leading to 37 MRI examinations at both timepoints. The MRI sequence showing the most pronounced artifacts within the FGT was THRIVE (T1); thus, this sequence was selected for measurements.
The frequencies of artifacts in T1-weighted MRI images were assessed in 36 patients who underwent MRI at both 6 and 12-month follow-ups. At both timepoints, 2.8% (1/36) of the patients had no MRI artifacts (grade 0), 72.2% (26/36) of the patients had artifacts visible only in the subcutaneous tissue or artifacts <5 mm in FGT (grades 1 and 2), and 25.0% (9/36) of the patients had artifacts measuring >5–10 or 11–30 mm in FGT with minimal to slight impaired clinical assessment (grades 3 and 4). There were no grade 5 MRI artifacts judged to impair the clinical assessment (Table 2). Similar results were found for T2-weighted MRI images (Table 2). MRI artifacts on T1-weighted and T2-weighted images are illustrated in Fig. 1.
The frequencies of artifacts after 6 and 12-month follow-up in T1- and T2-weighted MRI images.
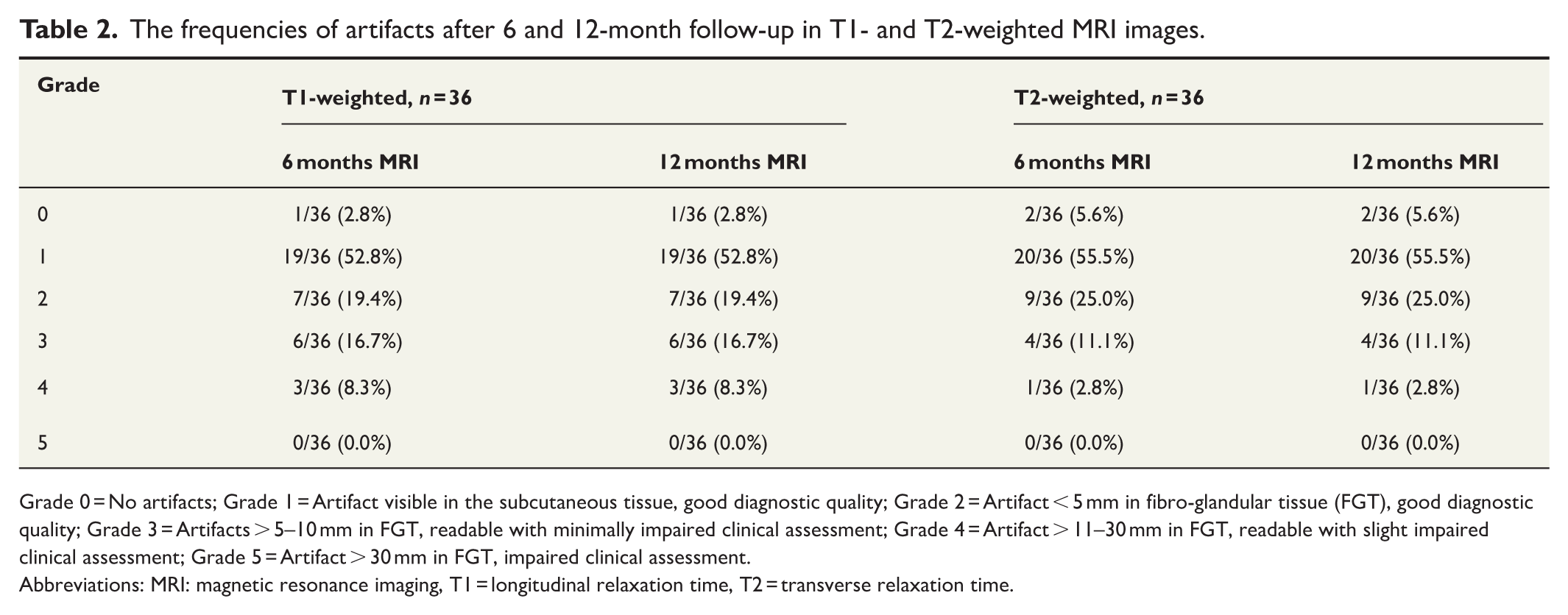
Grade 0 = No artifacts; Grade 1 = Artifact visible in the subcutaneous tissue, good diagnostic quality; Grade 2 = Artifact < 5 mm in fibro-glandular tissue (FGT), good diagnostic quality; Grade 3 = Artifacts > 5–10 mm in FGT, readable with minimally impaired clinical assessment; Grade 4 = Artifact > 11–30 mm in FGT, readable with slight impaired clinical assessment; Grade 5 = Artifact > 30 mm in FGT, impaired clinical assessment.
Abbreviations: MRI: magnetic resonance imaging, T1 = longitudinal relaxation time, T2 = transverse relaxation time.

MRI artifacts on T1-weighted and T2-weighted images.
Skin discoloration
At baseline 94% (47/50) of the patients were photographed and measured for skin discoloration, and 70.2% (33/47) had a skin discoloration with a median area of 0.20 cm2 (IQR 0.20–0.57). The discolored skin area was removed in 21 patients during surgery, but despite the removal of the skin at the injection site, 38.1% (8/21) of the patients had a remaining skin discoloration at the postoperative follow-up. All 50 patients were photographed and measured for skin discoloration at the 1-month follow-up, and 56.0% (28/50) of the patients had a skin discoloration with a median area of 0.72 cm2 (IQR 0.20–1.61). Of the 22 patients with no skin discoloration, 54.5% (12/22) of the patients had the discoloration removed during surgery. At the 6-month follow-up, the skin discoloration had disappeared in one patient, and 54.0% (27/50) of the patients had a remaining skin discoloration with a median area of 0.75 cm2 (IQR 0.14–1.77). At the 12-month follow-up, 54.0% (27/50) of the patients had a remaining skin discoloration with a median area of 0.79 cm2 (IQR 0.14–1.41) (Table 3).
Follow-up data in women with skin discoloration.
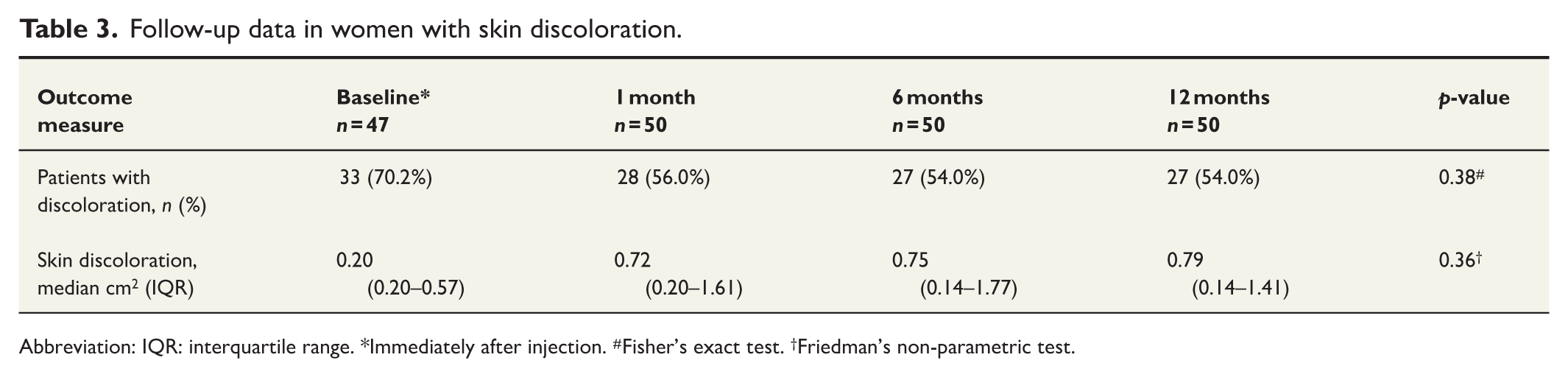
Abbreviation: IQR: interquartile range. *Immediately after injection. #Fisher’s exact test. †Friedman’s non-parametric test.
Correlation between MRI artifacts and skin discoloration
The MRI artifacts were correlated to the skin discoloration present on the baseline photography, and the patients were divided into two groups: (a) patients with skin discoloration and (b) patients without skin discoloration. The hypothesis was that patients without skin discoloration after SPIO injection had likely received a subcutaneous rather than a true intradermal injection.
At the 6-month follow-up, 24.3% (9/37) of the patients had a grade 3 to 4 MRI artifact. Among them, 44.4% (4/9) of the patients had a skin discoloration, and 55.6% (5/9) of the patients did not have any skin discoloration. At the 12-month follow-up, 27.0% (10/37) of the patients had a grade 3 to 4 MRI artifact. Among them, 40.0% (4/10) of the patients had a skin discoloration, and 60.0% (5/10) of the patients did not have any skin discoloration. However, when comparing the distribution of artifacts depending on the presence of a skin discoloration at baseline, this was statistically significant only for T1-weighted MRI sequences at 6 months follow-up (Table 4).
The frequencies of MRI artifacts at 6- and 12-month follow-up based on skin discoloration at baseline photography.
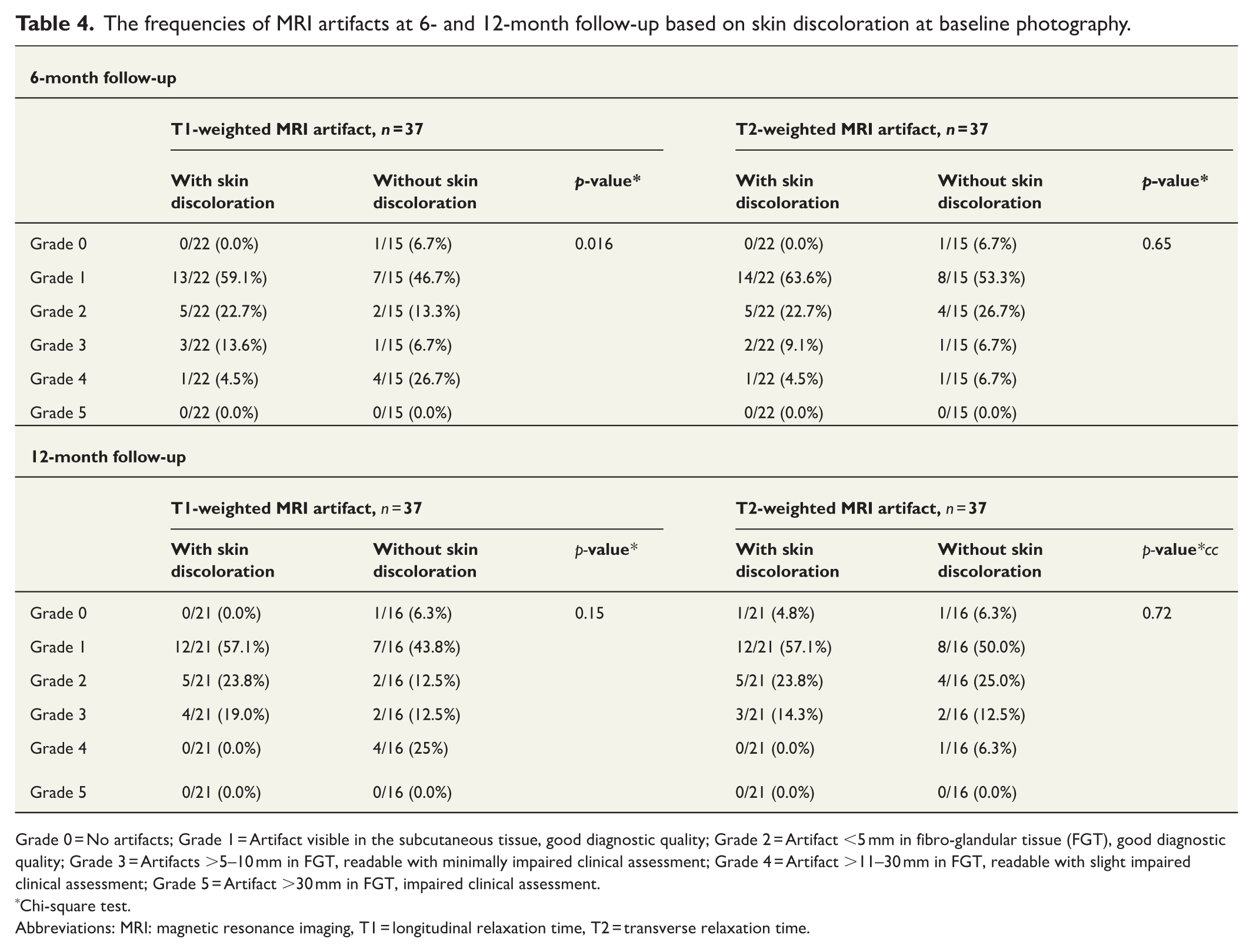
Grade 0 = No artifacts; Grade 1 = Artifact visible in the subcutaneous tissue, good diagnostic quality; Grade 2 = Artifact <5 mm in fibro-glandular tissue (FGT), good diagnostic quality; Grade 3 = Artifacts >5–10 mm in FGT, readable with minimally impaired clinical assessment; Grade 4 = Artifact >11–30 mm in FGT, readable with slight impaired clinical assessment; Grade 5 = Artifact >30 mm in FGT, impaired clinical assessment.
Chi-square test.
Abbreviations: MRI: magnetic resonance imaging, T1 = longitudinal relaxation time, T2 = transverse relaxation time.
Modified SDIEQ
Between 6 and 12 months after surgery, 76.0% (38/50) of the patients answered the SDIEQ at one timepoint (either at 6 or 12 months). Out of the 27 patients with a skin discoloration, only one patient reported “a lot” to “very much” discomfort in all five different aspects. The size of the discolored skin in this patient measured 0.55 cm2, ranking as the 18th largest discoloration within the group, with the remaining skin discolorations.
Residual magnetic counts
The injection site in the breast was measured for transcutaneous residual magnetic counts, with a median magnetic residual count of 9999 (IQR 4575-9999) immediately after surgery, 8020 counts (IQR 3400–9999) at 1 month follow-up, 4038 counts (IQR 1450–9999) at 6 months, and 1400 counts (IQR 589–3900) at 12 months. The transcutaneous residual magnetic counts were lower in patients when the skin discoloration had been removed (Table 5).
The residual SPIO counts after surgery depending on whether the skin discoloration was removed or not.
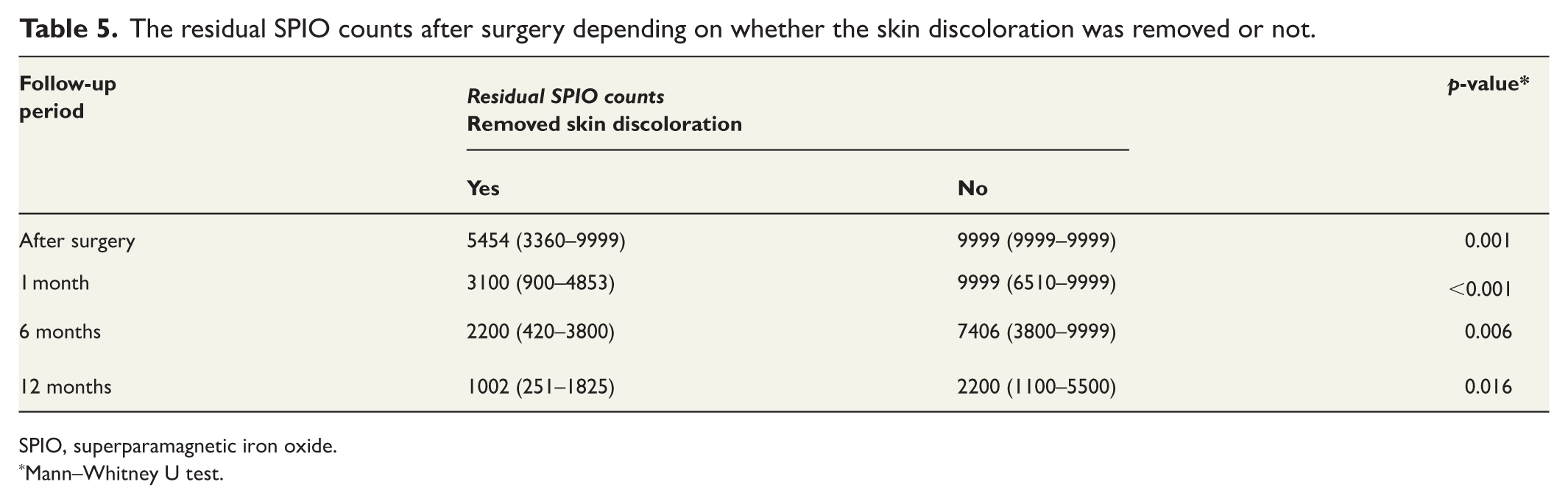
SPIO, superparamagnetic iron oxide.
Mann–Whitney U test.
Discussion
In the first report of the MAGSNOW trial, SLN detection was feasible in all 50 patients using an intradermal ultra-low dose of 0.1 mL SPIO. 14 In the present pre-planned follow-up of the secondary endpoints, MRI artifacts and skin discoloration were evaluated. None of the patients showed MRI artifacts deemed to be of any major impact on the radiological assessment of the breast gland. The skin discolorations after the intradermal injections were small and remained similar in size during the 12-month follow-up Fig. 2. Importantly, even if there was a remaining skin discoloration, this did not have an impact on the patient-reported experience.

Follow-up of typical skin discoloration in a woman after 0.1 mL intradermal SPIO injection.
Previous studies that have used 2 mL of SPIO injected in the glandular tissue have reported MRI artifacts of a greater extent compared to our results.10,11,16,17 In patients undergoing BCS and SLNB, Aribal et al. reported that 48.8% of the patients had MRI artifacts that impaired the assessment with signal void within the FGT. 17 Also, compared to our results, Krischer et al. presented three times more MRI artifacts (76.5%) after a mean of 42-month follow-up in a subgroup of patients treated with BCS. 10 Similar observations as ours were made in another study presenting less frequent MRI artifacts using 0.l mL SPIO injected intratumorally in six patients; however, an intratumoral injection seemed to result in a lower detection rate. 11 A recent prospective observational study using a 1 mL peritumoral SPIO injection reported a weighted prevalence rate of 20.9% for SPIO-related artifacts in the breast parenchyma in patients undergoing BCS, which aligns with our findings of a 25% frequency of artifacts affecting the breast parenchyma. 18 However, different MRI scale was used in these studies. Therefore, it is challenging to draw direct parallels between the studies, especially considering that we investigated different doses and injection sites.
We, however, noticed during the analysis that 29.8% of the patients did not have any skin discoloration immediately after SPIO injection and thus hypothesized that these patients had received a subcutaneous injection instead of a true intradermal injection. Interestingly, the present findings indicate that patients with a skin discoloration had reduced MRI artifacts, which underlines the importance of a good injection technique if using an intradermal injection so that SPIO does not enter the subcutaneous tissue. A correct intradermal injection will, however, result in a small skin discoloration that can have cosmetic implications, but this discoloration can, on the other hand, be removed during surgery. If the SPIO injection is placed in the same area as the skin incision for the tumor removal, it is even easier to remove the small staining by excising a small amount of skin. For most patients, an additional scar from the removal of the injection site in the periareolar region is minimal and can effectively be hidden when aligned with the areolar border. The final cosmetic result, however, depends on individual healing and the precision of the surgical technique, which has to be taken into consideration. Furthermore, the removal of the skin discoloration during surgery is also associated with significantly lower residual SPIO counts over time, suggesting that the surgical removal reduces SPIO retention in patients. Since the drainage process is activated immediately after the SPIO injection, it is important to note that even after the removal of the skin discoloration, SPIO in the deeper tissue may later migrate back to the surface. This may explain the remaining skin discoloration in eight out of 21 patients (38.1%) at the postoperative follow-up, despite the removal of the skin at the injection site during surgery. Therefore, it is important that patients are informed about the potential skin discoloration and how this is associated with the risk for MRI artifacts. These findings underscore the need for further refinement of this method, where the injection technique is one of the many considerations.
Karakatsanis et al. identified that patients who received a peritumoral injection of 2 mL SPIO had a lower risk of developing a skin discoloration compared to a periareolar injection, with 20.5% compared to 79.5% of the patients having a skin discoloration after 15 months. 19 Similarly, Wärnberg et al. evaluated skin discoloration depending on the injection site (retro-areolar compared to peritumoral) after injection of 2 mL SPIO, demonstrating that skin discolorations were less frequent with peritumoral injection (37.8%) compared to retro-areolar injection (67.3%), with two of the patients depicted in Fig. 3 for reference. 9 The mean size of the discoloration was 16.3 (range 2–100) cm2 after a retro-areolar injection compared to 6.8 (range 1–100) cm2 after a peritumoral injection. 9 Also, Rubio et al. addressed skin discoloration in a randomized trial comparing 1, 1.5, and 2 mL SPIO injected subareolarly on the day of surgery. 12 The 6-month follow-up showed significantly less skin discoloration in the 1 mL group compared to the other two groups. Our study did not demonstrate any significant reduction in skin discoloration over time. Compared to other studies, our results showed a minimal skin discoloration with a median size of 0.79 cm2 that has not been reported before.9,12,19

Follow-up of skin discoloration in a woman after injection of 2 mL SPIO diluted with 3 mL saline injected in the periareolar area.
In this study, only one woman among the 38 patients answering the SDIEQ reported concerns regarding skin discoloration. Patient-reported outcomes considering skin discoloration have been addressed before.3,12,19,20 In the MONOS study, Karakatsanis et al. reported that 97% of the patients had no complaints after 10 months. 19 Furthermore, Wärnberg et al. noted better patient-reported outcomes in patients who received peritumoral injection. 9 In the SUNRISE trial, Rubio et al. reported no cosmetic complaints regarding the discolored skin in 70% of the patients. 12 In accordance with the previous findings, our data showed discomfort in one of 38 (2.6%) patients after surgery. These results imply that a potential skin discoloration is not considered a problem for most patients. This study marks the first use of a standardized questionnaire to assess patient-related outcomes concerning skin discoloration.
This study has limitations as it is a non-randomized, single-center, prospective analysis within a framework of a feasibility study, restricted by a small sample size, resulting in low statistical power. The external validity and the generalizability could be affected due to the small sample size, and due to that, the trial was performed at only one center. Moreover, the 0.1 mL SPIO is not yet approved for clinical use, and our results would be applicable in the future only if the dose is approved. This underscores the need for larger, multicentre trials to further validate the present results. A strength of the study is the prospective design, with MRI artifacts and skin discoloration being predefined endpoints with predefined definitions. A limitation is also that the grading of the MRI artifact and the skin discoloration impact evaluation questionnaire was not validated. Selection bias is also a factor to be considered, as patients who consented may not be representative of those concerned about skin discoloration or future MRI artifacts caused by SPIO. The clinical routine at the time of the trial was to use 1.0 mL SPIO, potentially causing even larger artifacts and discolorations. Despite these limitations, the insights gained contribute information to the existing literature concerning the effects of MRI artifacts and skin discolorations using an ultra-low dose of SPIO in patients undergoing BCS and SLNB.
This study shows that an ultra-low dose of 0.1 mL SPIO injected intradermally appears to minimize MRI artifacts to an extent that it does not compromise the diagnostic interpretation of breast MRI in the vast majority of patients undergoing BCS. Furthermore, this ultra-low dose of SPIO creates only a minor skin discoloration that can potentially also be removed during surgery. The efficacy in SLN detection was also recently demonstrated in a larger multicentre prospective phase II trial, including 216 patients, where the ultra-low dose of 0.1 mL SPIO injection was non-inferior to Tc99m and BD. 21
Supplemental Material
sj-docx-1-sjs-10.1177_14574969251387495 – Supplemental material for Impact of an ultra-low dose of superparamagnetic iron oxide on postoperative breast MRI artifacts and skin discoloration in patients with breast cancer
Supplemental material, sj-docx-1-sjs-10.1177_14574969251387495 for Impact of an ultra-low dose of superparamagnetic iron oxide on postoperative breast MRI artifacts and skin discoloration in patients with breast cancer by Nushin Mirzaei, Fredrik Wärnberg, Pontus Zaar, Micael Oliveira Diniz, Andreas Karakatsanis, Henrik Leonhardt and Roger Olofsson Bagge in Scandinavian Journal of Surgery
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.