
Abstract
Background:
In patients with renal hyperparathyroidism the choice of surgery varies between total parathyroidectomy with autotransplantation (TPTx + AT) and subtotal parathyroidectomy (SPT) with variable outcomes. The present study investigated the risk of extracervical recurrences in patients who underwent total parathyroidectomy with autotransplantation for dialysis patients with renal hyperparathyroidism.
Methods:
A retrospective cohort analysis of patients who underwent TPTx + AT for renal hyperparathyroidism between the years 2000 and 2023 at a tertiary referral hospital. Patient demographic profiles, biochemical and surgical data, incidence of recurrence and outcomes of intervention were collected.
Results:
Some 142 (71M:71 F) patients with a mean age of 58.6 ± 11.2 years underwent total parathyroidectomy and autotransplantation during the study period. The mean dialysis vintage was 6.3 ± 3.2 years. Extracervical recurrence was seen in 25 (17.6%) of 142 patients, after a mean follow-up of 9 (±4.2) years, with the common sites of recurrence being the deltoid autotransplant site (73.1%) and the mediastinum (11.5%), while 7.7% of recurrences were biochemical with no localized site. Of the recurrences, 19 of 25 (76%) underwent explant of the deltoid autotransplant, and two in the mediastinum underwent minimally invasive excision (one video assisted thoracic surgery and one robotic excision) of the parathyroid lesion. The median parathyroid hormone level at the time of recurrence was 109.4 pg/ml compared with 17.2 ng/L postexcision or explantation. The only factor predictive for recurrences in the cohort on multivariable analysis was postoperative serum PTH (p = 0.001). Log-rank test showed no statistically significant difference in survival between the two groups (p = 0.355).
Conclusion:
Extracervical recurrences in the autotransplant are not uncommon in the long-term following total parathyroidectomy and autotransplantation for patients with renal hyperparathyroidism. These recurrences need explantation or excision to reduce the PTH burden in patients who cannot avail a renal transplant.
Keywords
Context and relevance
Autotransplantation of the parathyroid gland is a well-established surgical technique, especially in the context of renal (secondary or tertiary) hyperparathyroidism following total parathyroidectomy with or without thymectomy.
Autotransplantation prevents permanent hypoparathyroidism, provides a controlled source of PTH post-op, and in the presence of recurrence the autograft is easier to resect than re-exploring the neck.
Recurrence of the autografts following autotransplantation is reported to be approximately 8% but literature in this regard is sparse.
Long-term extracervical recurrence following total parathyroidectomy and autotransplantation is not uncommon with an incidence of 18%.
Most recurrences are in the deltoid explant.
Elevated postoperative PTH well above the normal range is a predictor of long-term recurrence.
Explantation of the autotransplant is required to mitigate the severe hypophosphatemia and elevated PTH.
Not all cases of elevated PTH are due to recurrence, but may be due to prolonged dialysis after parathyroidectomy.
Long-term surveillance is necessary in patients following TPTX + AT for early detection of recurrence.
Introduction
Chronic kidney disease (CKD) is a common condition globally, affecting 5% to 10% of the population, with significant impact on health. 1 Worsening renal function over decades would eventually result in end-stage renal disease (ESRD), associated with increased serum parathyroid hormone (PTH), phosphorus and derangement of calcium, 25-hydroxyvitamin D (25(OH)D),1,25-dihydroxyvitamin D (1,25(OH)2D), fibroblast growth factor-23 (FGF-23), and growth hormone. Given the fact that patients with ESRD commonly develop mineral and bone disorders, known as CKD-MBD, this prompted Kidney Disease Improving Global Outcomes (KDIGO) to produce clinical guidelines for the management of this condition. 2 CKD-MB has a prevalence of about 55% as shown by a study from Singapore. 3
A manifestation of CKD-MB is renal hyperparathyroidism associated with elevated PTH and parathyroid gland hyperplasia. The mineral abnormalities and the increased PTH can be toxic to bone, heart muscle, and other organs. 4 Increased parathyroid hormone levels promote cardiovascular sequelae such as left ventricular hypertrophy, arrhythmias, and rates of incident heart disease. 5 In addition, the deranged bone and mineral metabolism has shown to be associated with extraskeletal calcification, especially in the vasculature.6,7 The treatment of CKD-MB generally involves medical therapy to control the levels of phosphate, calcium, vitamin D, and PTH levels. Common measures include administering phosphate binders, calcium and Vitamin D supplements, reducing phosphate intake and oral cinacalcet therapy. Patients who fail conservative therapy, require surgical parathyroidectomy.
Surgical treatment options for renal hyperparathyroidism includes total parathyroidectomy (TPTx), subtotal parathyroidectomy (STTPTx), and total parathyroidectomy with auto transplantation (TPTx + AT), with or without transcervical thymectomy.8,9 In patients who undergo TPTx + AT common sites for autotransplantation include the deltoid, brachioradialis and sternocleidomastoid muscles.10–12 AT help regulate the levels of parathyroid hormone and other minerals in the blood, and thereby alleviate the complications associated with low level of parathyroid hormones in renal hyperparathyroidism, seen in patients who undergo TPTx alone.8,13 However, despite the potential benefits of TPTx + AT, recurrences are not uncommon in the autograft.14,15 The aim of this study was to examine the outcomes of recurrences in patients on long-term surveillance following TPTx with deltoid autotransplantation.
Methods
This retrospective study evaluated all patients diagnosed with renal hyperparathyroidism who underwent total parathyroidectomy with deltoid autotransplantation between 2000 and 2022. The study adhered to the Declaration of Helsinki and was approved by the institution’s research ethics committee (IRB no 2022/00647). Variables extracted from the electronic medical records included clinical characteristics such as age at the time of the total parathyroidectomy, gender, race, dialysis vintage, tumor size, and thymectomy status. In addition, preoperative and postoperative biochemical indices—including serum calcium, parathyroid hormone, phosphate, and bone alkaline phosphatase levels—were reviewed.
Hospital medical records and prospectively maintained outpatient clinic records were examined to assess the incidence of postoperative hypocalcemia and hungry bone syndrome, as well as overall survival and recurrence. Recurrence data included the site, parathyroid hormone levels, and the management of recurrence. Recurrence was defined as initial decrease of serum PTH, followed by a subsequent increase in PTH, usually after 6 months or reappearance of elevated parathyroid hormone (greater than 6.8 pmol/L) and/or hypercalcemia (more than 2.6mmol/L) after a normalization or near normalization level post operative parathyroidectomy.16–19 All patients received a cervical ultrasound and a Sestamibi-scintigraphy prior to intervention. Overall survival was calculated as the time interval from the date of definitive surgery to mortality, regardless of the cause. The last follow-up date was December 2023. Patients with subtotal parathyroidectomy, cervical recurrences post total or subtotal parathyroidectomy and post renal transplant hyperparathyroidism were excluded from the study.
Data were recorded in Microsoft Excel (Microsoft Corp., Redmond, WA, USA). Patients were categorized based on recurrence status. Descriptive statistics are presented as mean (standard deviation), median (inter-quartile range), and frequencies (percentages) as appropriate. Continuous variables were compared using the student’s t-test or Mann–Whitney U test, while categorical variables were analyzed with the Chi-square test or Fisher’s exact test. The 5-year overall survival between the two groups was evaluated using the Log-Rank (Mantel-Cox) test and Kaplan-Meier survival curve. Univariate analysis of recurrence was performed using Cox regression analysis, with variables having a p-value < 0.2 included in the multivariable analysis. Hazard ratios and their 95% confidence intervals were calculated for each variable, with a p-value < 0.05 considered statistically significant. All statistical analyses were conducted using JASP version 0.18.3 (Netherlands) and IBM SPSS Statistics version 26 (IBM Corp., Armonk, NY, USA) for Windows.
Results
A total of 142 patients with renal hyperparathyroidism underwent total parathyroidectomy, comprising 71 males and 71 females (as shown in Fig. 1). The mean age of the patients was 58.3 ± 11.3 years. Of these, 25 patients (17.6%) experienced recurrence of hyperparathyroidism. The mean time to recurrence after index surgery was 5.1 years (± 2.4), with most of the recurrences prior to 2014 as shown in Fig. 2. There were no significant differences in the clinical profiles between the recurrence and nonrecurrence groups (Table 1). Preoperatively, only alkaline phosphatase was significantly higher in the no recurrence group (median 285 vs 107.5 (IU/L), p < 0.001). Serum calcium, PTH, and phosphate did not differ significantly between the two groups (Table 1).
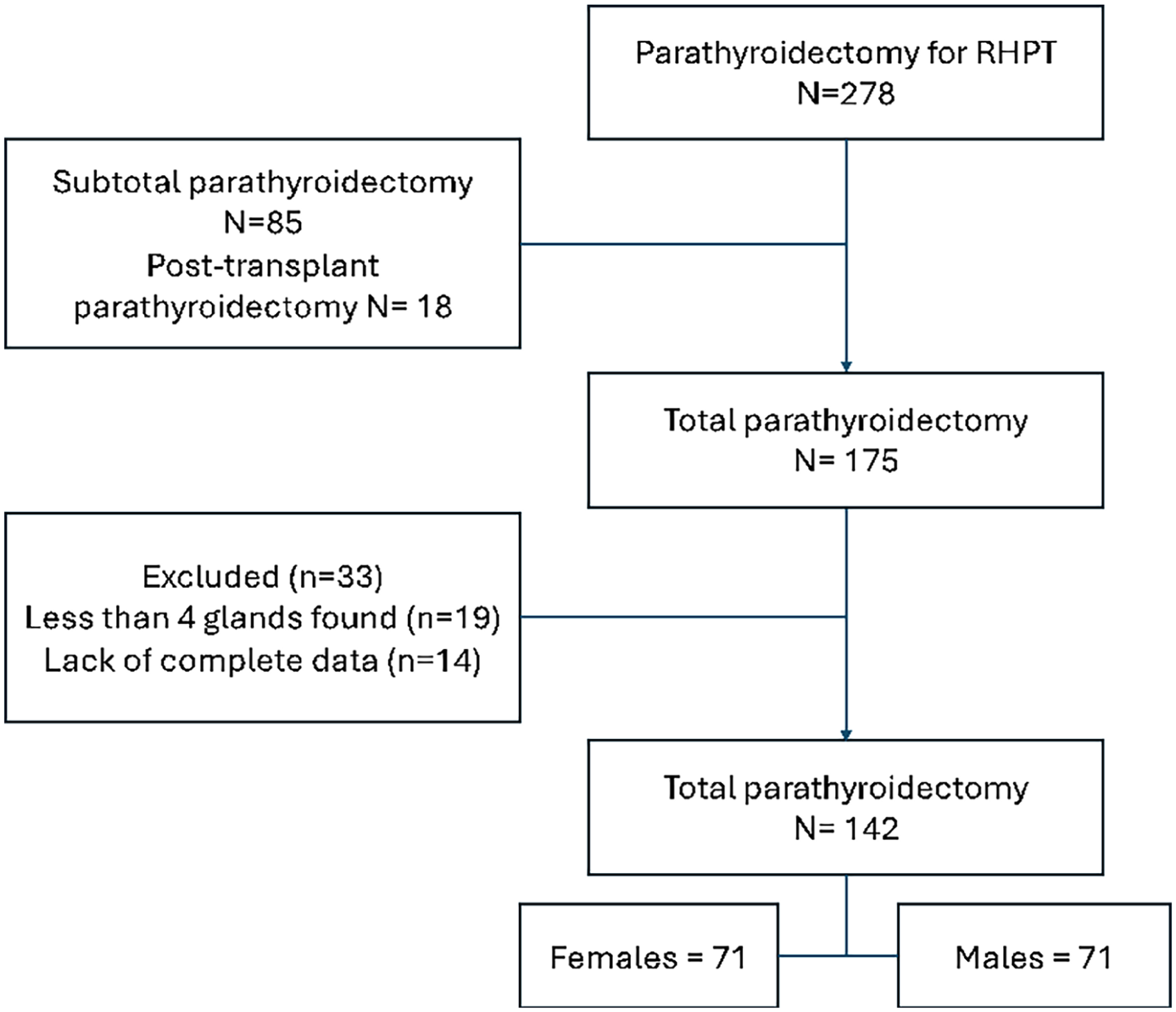
PRISMA of the study cohort.
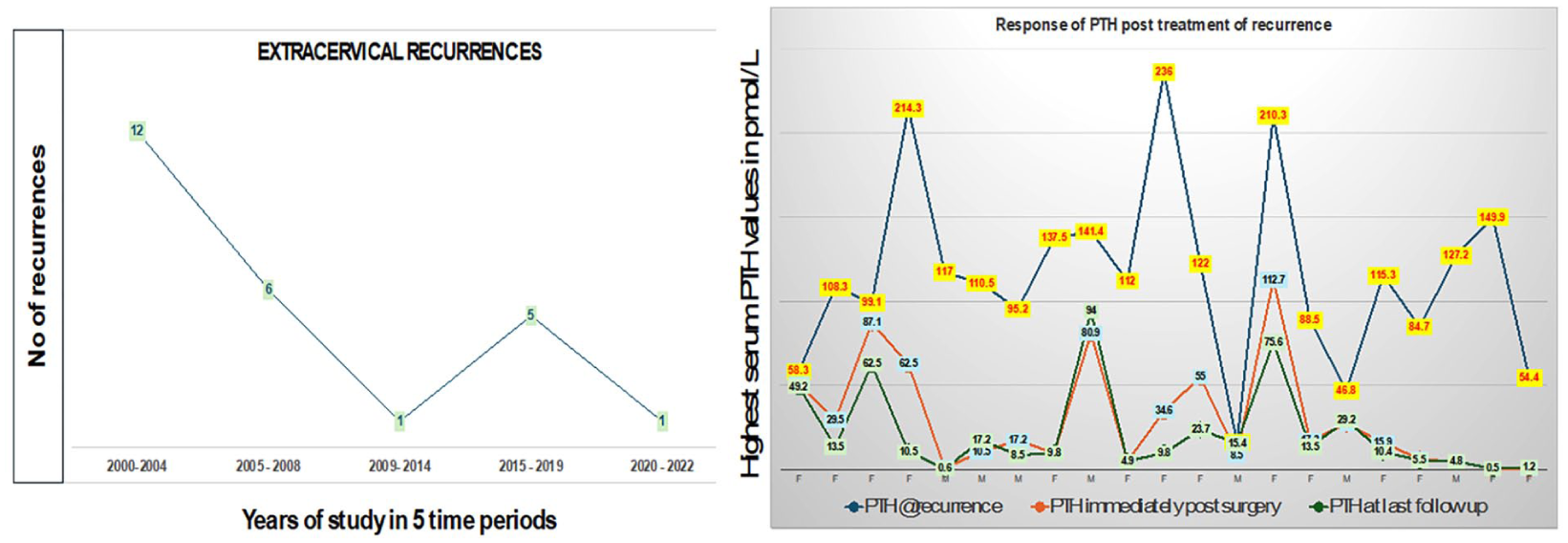
Number of recurrences over the period of study showing a higher recurrence rate prior to 2014, and change in PTH after treatment of recurrences in 21 patients (19 deltoid explants and 2 mediastinal excision of hyperplastic glands).
Clinical and biochemical profile of patients (n = 141) with total parathyroidectomy and autotransplantation.
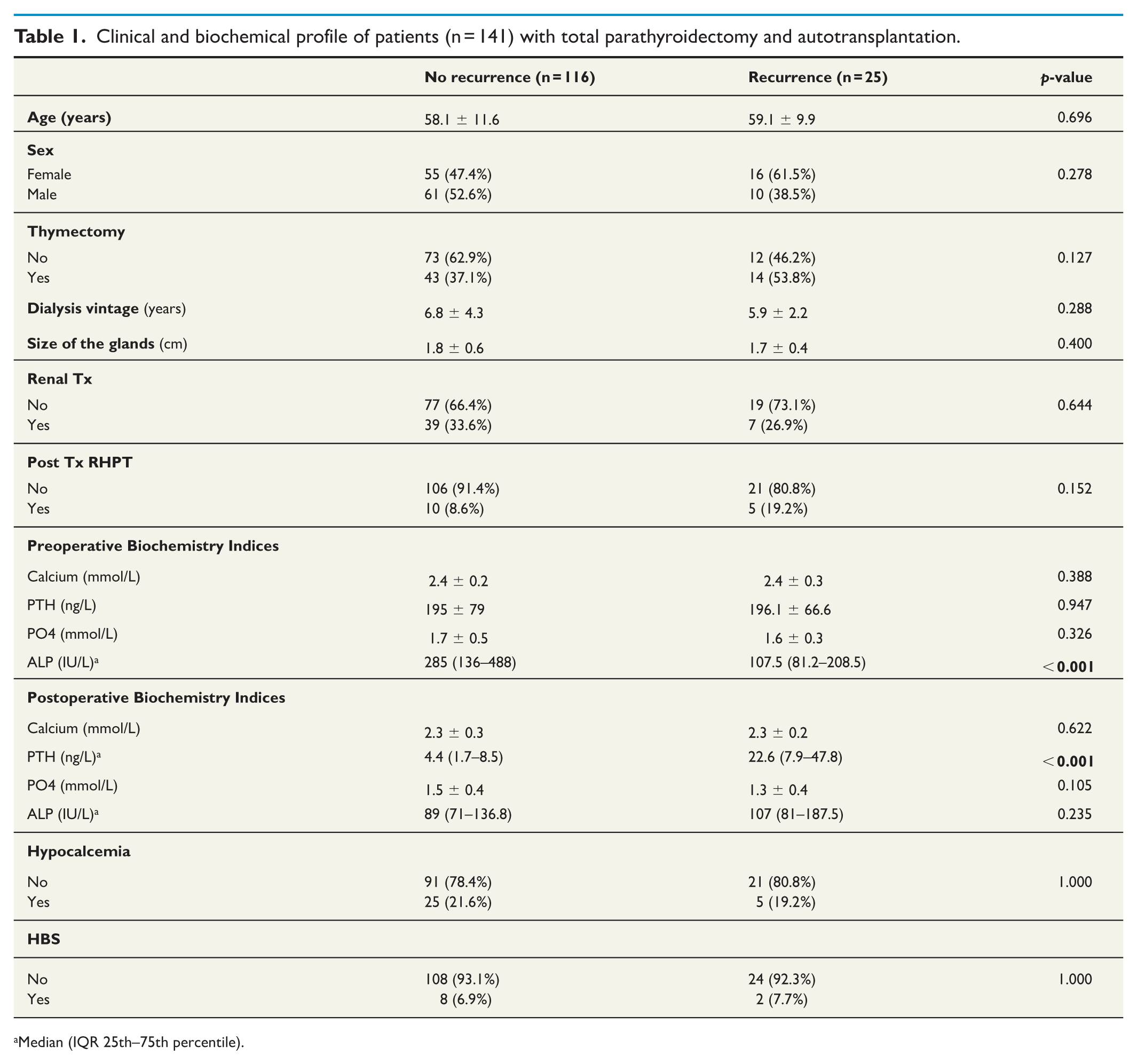
Median (IQR 25th–75th percentile).
Postoperatively, the parathyroid hormone level was significantly higher in the recurrence group (median of 22.6 vs 4.4 ng/L, p < 0.001). Other postoperative parameters, including serum calcium, phosphate, alkaline phosphatase levels, as well as the incidence of hypocalcemia and hungry bone syndrome, were similar between the two groups (Table 1). The most common sites of recurrence were the deltoid (73.1%) and the mediastinum (11.5%), while 7.7% of recurrences were biochemical with no localized site. The median parathyroid hormone level at the time of recurrence was 109.4 ng/L. Among the 25 patients with recurrence, 80.8% underwent explantation of the deltoid autograft, with a median parathyroid hormone level of 17.2 ng/L postexcision or explantation (Table 2). Four patients (one with mediastinal, one forearm recurrence, and two with biochemical hyperparathyroidism) chose not to have any revision surgery for the recurrences. The two patients with persistent biochemical elevation of PTH had negative imaging on both US of the neck, deltoid and Sestamibi scans.
Recurrent renal hyperparathyroidism outcomes and management.

Median (IQR 25th–75th percentile).
In the 19 patients with deltoid autograft who underwent explantation and two patients with mediastinal excision, the change in PTH is shown in Fig. 2. Of the 19 patients, four continue to have very elevated PTH (more than five times the upper limit of normal) despite surgical intervention and of these two patients had previous thymectomy performed at index surgery. The mediastinal recurrence in two patients was treated with VATS approach (n = 1) and robotic surgery (n = 1). In terms of complications, symptomatic hypocalcaemia was seen in two (4%) and hungry bone syndrome in one (2%) of the patients with recurrent surgery.
Univariate Cox regression analysis revealed that postoperative PTH (HR = 1.049, 95% CI: 1.035–1.064; p < 0.001) were associated with recurrence. Multivariable analysis confirmed that only postoperative PTH remained a strong predictor of recurrence (HR = 1.043, 95% CI: 1.027–1.060; p < 0.001) (Table 3). The 5-year overall survival rate was 92.9% for patients with recurrence and 84% for those without recurrence. However, the log-rank test showed no statistically significant difference between the two survival rates (p = 0.355). The mean overall survival time was 204.5 months for the recurrence group and 211.1 months for the nonrecurrence group (Fig. 3).
Uni-and multivariable Cox regression analysis for recurrence total parathyroidectomy and autotransplantation.
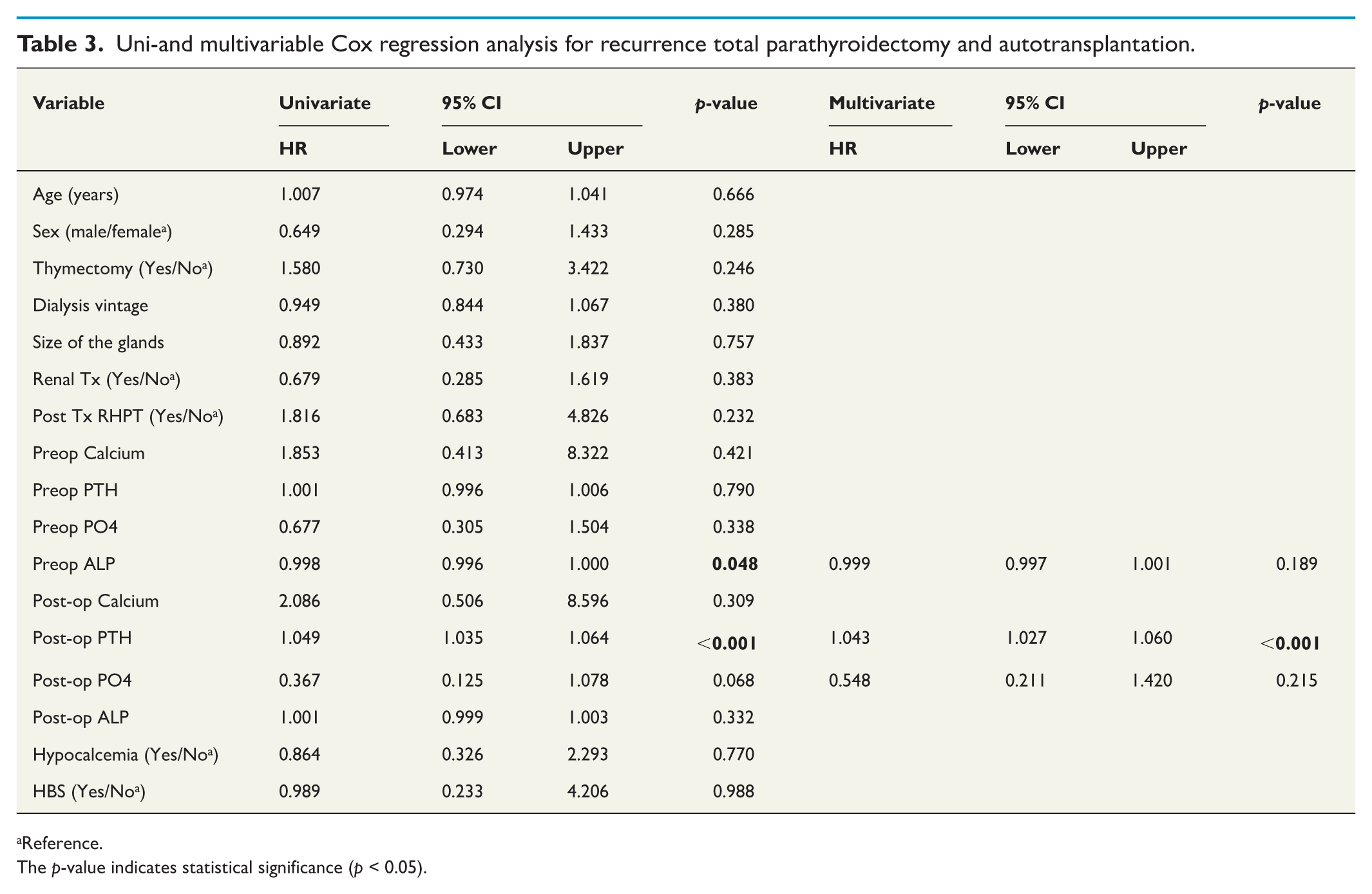
Reference.
The p-value indicates statistical significance (p < 0.05).
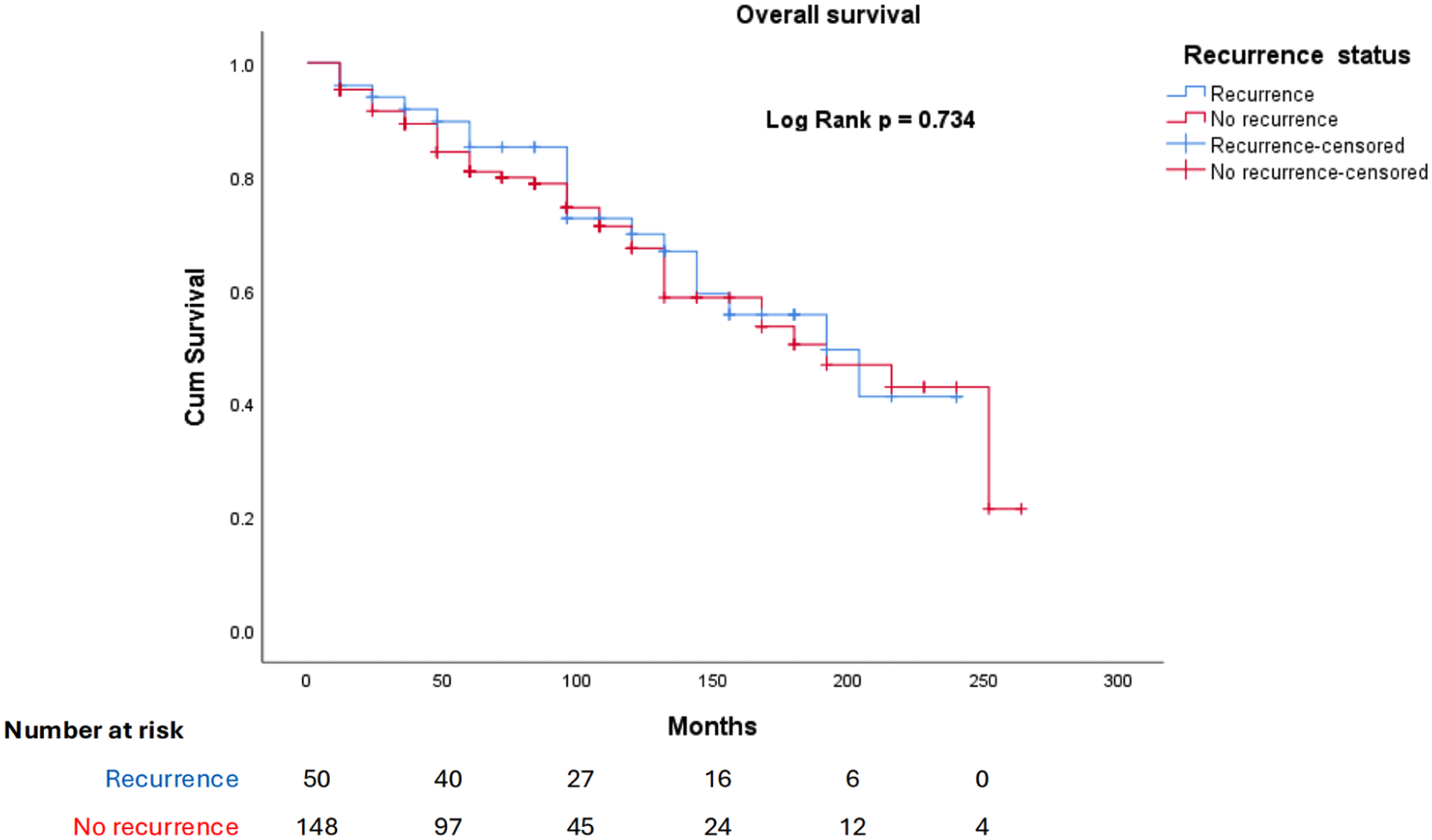
Overall survival between the recurrence and no recurrence groups after total parathyroidectomy for renal hyperparathyroidism.
Discussion
The incidence of long-term extracervical recurrence following TPTx + AT is about 18%, with nearly three quarters of them in the deltoid autograft, and mediastinum. In such extracervical recurrences, interventions like deltoid parathyroid explant or mediastinal exploration may be required to render the patients euparathyroid. This long-term study shows a higher incidence of autografted hyperplasia with continuing severe CKD, though with no impact on mortality. The predictors of long-term recurrence in this study include higher postoperative PTH levels and longer duration of CKD. The findings from the study align with previous research that there is a continued high secretion of PTH following TPTx. 20
Patients with CKD have hyperplasia of the parathyroid glands and usually require removal of all the glands and the choice of nature of the parathyroid surgery depends on a few factors. Subtotal PTx is the preferred choice of surgery in patients with tertiary hyperparathyroidism post renal transplantation where only one or two glands may be hyperplastic.21,22 TPTx + AT is preferred in patients with co-existent thyroid pathologies that may require further interventions, medical comorbidities precluding safe general anesthesia or surgery, or previous neck surgeries. 23 Review of articles published in the literature comparing outcomes of TPTx + AT with subtotal PTx showed superior benefits in terms of recurrence with TPTx + AT.13,14,24–27 In a previous study we had shown superior outcomes in the short term TPTx + AT in our institution, with subtotal PTx being preferred in transplanted patients with tertiary hyperparathyroidism. 14
Following total parathyroidectomy for refractory secondary or tertiary hyperparathyroidism, a small amount of viable parathyroid tissue is often ectopically implanted to maintain controlled parathyroid hormone (PTH) production and prevent permanent hypoparathyroidism. The Wells’ method is the most employed technique, involving transplantation of parathyroid tissue into the forearm muscle (typically brachioradialis).12,28 This approach offers a surgically accessible site for potential future re-excision and facilitates PTH monitoring from the graft site via selective blood sampling. However, the technique is not without drawbacks, with a common concern being potential interference with vascular access. To address these concerns, minimally invasive alternatives have been proposed, including subcutaneous injection or Intramuscular injection of finely minced parathyroid tissue, which are the techniques employed in our institution.10,11,29
While parathyroid autograft is effective in preventing permanent hypoparathyroidism following total parathyroidectomy, it is not without potential complications. One notable concern is the development of autograft hyperplasia, the incidence of which is reported to be approximately 8%, and the risk appears to be closely linked to the selection of the reimplanted parathyroid tissue.15,16,30 Reimplantation of hyperplastic, nodular, or otherwise diseased tissue can lead to recurrent or persistent hyperparathyroidism originating from the graft site. To mitigate this risk, it is recommended that the reimplanted tissue be carefully selected intraoperatively, ideally using the most normal looking gland in size and architecture, and confirmed, when possible, by frozen section analysis. In addition, dividing the tissue into multiple small fragments implanted into separate pockets within the muscle can help reduce the likelihood of overgrowth and facilitate targeted re-excision if necessary. The institutional practice for the last 15 years has been to use about 30-40 mg of the most normal looking parathyroid and mince it before implanting into the deltoid and this has been shown to be very effective maintaining the PTH levels.10,11
Several factors can contribute to the recurrence of hyperparathyroidism following parathyroidectomy in patients with renal hyperparathyroidism and include incomplete removal of the parathyroid glands during the initial surgery, the presence of supernumerary or more than four glands or ectopic parathyroid glands, and the development of new hyperplastic glands over time. In the study reported here, long-term recurrence in the deltoid autotransplant was seen in nearly 10% of the cohort, similar to that reported by Tominaga et al. 30 in their series of 2669 patients requiring deltoid explant in 9.3%. Supernumerary glands in the neck and mediastinum were seen in 12 (6%) of patients, with half of them requiring surgical intervention. Numano et al. 31 reported the presence of supernumerary glands in their cohort of 870 patients, with 12 (2%) requiring reintervention for recurrent/persistent disease. Where deltoid autograft is the site of recurrence, en bloc resection of autograft with surrounding muscle is required. 30
Thymectomy along with subtotal or total PTx would decrease persistent or recurrent disease due to the presence of supernumerary or thymic parathyroids. Supernumerary parathyroid glands have been reported in over 10% of random autopsies, and in 30% of patients with renal hyperparathyroidism usually located in the neck in the retroesophageal grove or carotid sheath, and extracervical in the thymus and mediastinum. 32 In this study, three parathyroids were localized in the superior mediastinum, of whom two patients underwent re-exploration and were cured. A similar study showed intrathymic parathyroids at recurrent surgery in 28% of patients, found to be ectopic in 17 (63.0 %) patients and supernumerary in eight (29.6 %). 33 Thus, routine transcervical thymectomy should be performed where possible in patients on permanent hemodialysis with no potential for renal transplantation to decrease this risk of recurrent disease and reoperative morbidity.32–35
The findings from this study align with existing literature on the predictors and outcomes of recurrent renal hyperparathyroidism (rHPT) posttotal parathyroidectomy (TPTx). Previous research identified higher preoperative parathyroid hormone (PTH) levels and longer duration of renal disease post parathyroidectomy as significant predictors of recurrence, mirroring this study’s conclusions. 20 A recent meta-analysis showed a strong correlation between intraoperative parathyroid hormone (ioPTH) levels and early postoperative PTH measurements, indicating that ioPTH monitoring is a reliable intraoperative marker during parathyroidectomy (PTX) for renal hyperparathyroidism (rHPT). 36 In patients where there is no significant drop at 20 min with IOPTH may require closer PTH monitoring looking for persistent or recurrent disease. This is reinforced by the findings of Xu et al. 37 who emphasized that elevated PTH levels immediately after surgery are indicative of recurrence risk. However, not all biochemical PTH elevation post parathyroidectomy can be attributed to treatment failure or recurrence, after parathyroidectomy, as continued PTH secretion occurs in response to the uremic stimulus, and early hypocalcaemia. These studies collectively highlight the necessity of early surgical intervention and vigilant biochemical surveillance to mitigate the risk of recurrence and manage patient outcomes effectively. In this study, biochemical elevation of high PTH was seen in four patients, despite intervention to explant the deltoid autograft.
Management of recurrence following total parathyroidectomy can be troublesome. Our findings indicate that while recurrence is a relatively common occurrence, it does not significantly impact overall survival in this patient population. Improved surgical techniques and postoperative care may have contributed to effective outcomes in our cohort. However, patients experiencing recurrence had a significantly longer follow-up duration, suggesting they may require more intensive monitoring and management. This longer follow-up period (9.4 years for the recurrence group vs 7.3 years for the nonrecurrence group) underscores the need for vigilant long-term surveillance to detect and manage potential complications early.
Conclusion
In the long-term, extracervical recurrence is not uncommon following total parathyroidectomy and autotransplantation for renal hyperparathyroidism. When recurrences are detected, explantation of the autotransplant may be required to mitigate the severe hypophosphatemia and elevated PTH. Not all cases of elevated PTH are due to recurrence, but may be due to prolonged dialysis after parathyroidectomy, and in such cases continued medical therapy is required with long-term follow-up.
Footnotes
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Dan Cortes, Sujith Wijerethne, James Lee, Ngiam Kee Yuan, and Rajeev Parameswaran. Statistical analysis was performed by Ralph Victor Yap. The first draft of the manuscript was written by Dan Cortes & Sujith Wijerethne and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study adhered to the Declaration of Helsinki and was approved by the institution’s research ethics committee (IRB no 2022/00647).