
Abstract
Background and Aims:
The purpose of this study was to compare the incidence of and treatment methods for Achilles tendon ruptures (ATRs) in public and private healthcare in Finland between 1997 and 2019.
Methods:
The Finnish National Hospital Discharge Register and the Finnish Register of Primary Health Care Visits were searched to identify all adults diagnosed with ATR in 1997–2019.
Results:
In the study period, 91% of patients with ATR were treated in the public sector. In public healthcare, the majority of patients were treated nonoperatively (10,997; 40% operative vs 16,303; 60% nonoperative), whereas in the private sector, the majority of the patients were treated operatively (2088; 80% operative vs 514; 20% nonoperative) (P < 0.001).
Conclusion:
The distribution of public and private treatment for ATRs remained consistent during the follow-up period from 1997 to 2019. In the public sector, treatment methods became significantly more nonoperative during the study period, while no such change was observed in the private sector.
Keywords
Introduction
The incidence of Achilles tendon ruptures (ATRs) has increased globally.1–4 Although most ATRs have been treated operatively, recent studies have revealed that nonsurgical treatments with early functional rehabilitation deliver comparable functional outcomes without the risk of surgical complications, such as infection or sural nerve injury, for the majority of patients.5–8 This has led to an increase in the nonsurgical treatment of ATRs.2–4,9,10
In Finland, every resident is entitled to public health services. According to the Constitution of Finland, public authorities shall guarantee adequate social, health, and medical services for everyone. In addition to these services, numerous private healthcare providers operate in Finland. Public hospitals are government owned and funded to provide universal access to healthcare, while private hospitals are privately owned and funded, often catering to individuals with private insurance or the ability to pay out of pocket. Because of the good coverage offered by private and employment-based health insurance, most occupational accidents and sports injuries are treated in the private sector. By the end of 2013, 22.7% of Finnish adults had some form of private health insurance. 11 This is evident as private health insurance is used to access private healthcare.
In Finland, the treatment of ATRs has become geographically more uniform. 12 However, variations in ATR treatment options between the public and private sectors have not yet been studied. Thus, the aim of this study was to compare the incidence of and treatment methods for ATRs in the public and private healthcare sectors in Finland in 1997–2019.
Methods
This study uses data obtained from the National Hospital Discharge Register (NHDR) and the Finnish Register of Primary Health Care Visits (PHCR), both of which are maintained by the National Institute for Health and Welfare. Data reporting to the NHDR, which was established in 1967, is mandatory for all public and private hospitals in Finland. The PHCR, which has been operational since 2011, collects data on every patient visit within Finland’s public primary healthcare system. Both registers include data on patient’ s age, sex, domicile, external cause of injury, type of injury, primary and secondary diagnoses, type of hospital (public or private), duration of hospital stay, and possible operations performed during the hospital stay. The NHDR has been found to have strong validity in terms of the coverage and accuracy of its data, especially for orthopedic traumas.13–15
Patients with ATRs were identified by searching both databases using the primary or secondary diagnosis code of S86.0—injury of Achilles tendon (International Classification of Diseases, 10th Revision (ICD-10)). To identify all operatively and nonoperatively treated patients, the NHDR was searched for all records with the procedural code NHL10, which refers to “suture or reinsertion of Achilles tendon” (Nordic Classification of Surgical Procedures). This was done to include only acute ruptures and exclude plastic repairs or tendon grafts of a chronic rupture. Following this identification process, all duplicates between the two registers were excluded, and the subsequent treatment sector was recorded. Notably, records with diagnosis code S86.0 were included in the operative incidence calculation only if the operation was performed within 30 days of the injury. This criterion was used to exclude other operations for Achilles tendon injuries, such as salvage of nonoperative treatment failures or reoperation. All pediatric patients (younger than 16 years of age) were excluded from the study. Since the NHDR and PHCR do not report injury laterality, only the first recorded injury was included. Data on patients’ age, sex, procedures performed during the hospital stay, and hospital district were collected. Cases in which information regarding the public versus private status of the healthcare provider was not available; thus, they were excluded (n = 231). The patient inclusion flowchart is shown in Fig. 1.
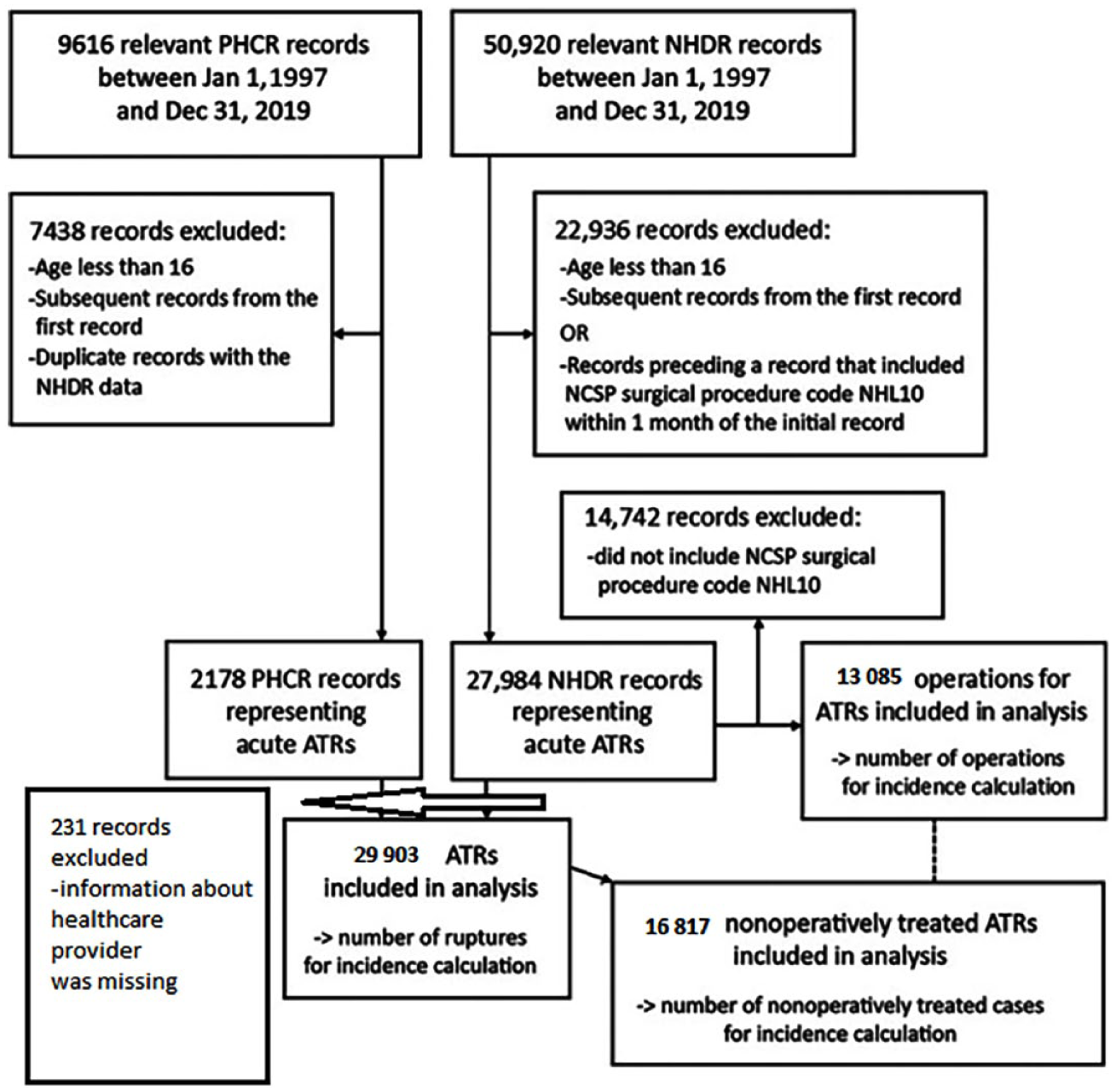
Patient inclusion flowchart.
Statistics
Continuous variables were summarized with means, standard deviations, and ranges. Incidences with 95% confidence intervals (CIs) were calculated based on the annual adult population (persons aged ⩾ 16 years), as obtained from Statistics Finland (www.stat.fi). 16 Cis were calculated using Ulm’s 17 method and the R software package epiR (version 2.0.80). 18 Differences in treatment methods and sex distributions between public and private hospitals were analyzed using Fisher’s exact test. Age differences between public and private hospitals were assessed using Welch’s t-test with a 95% CI. Incidence calculations and other statistical reports were conducted using R software version 4.3.0 (R Core Team) and the ggplot2 R software package (version 3.5.1) to produce graphics.
Ethics, data sharing, funding, and disclosures
Ethical approval for the study was granted by the Finnish National Institute of Health and Wellness (study permit number THL/2266/5.05.00/2019), and we received research funding from the Finnish government. The data supporting the findings of this study are available from the corresponding author upon request. A complete disclosure of interest according to the International Committee of Medical Journal Editors (ICMJE) is available upon request.
Results
A total of 29,902 ATRs were identified, of which 16,817 (56%) were treated nonoperatively and 13,085 (44%) were treated operatively. A total of 27,300 (91%) ATRs were treated in the public healthcare system, and 2602 (9%) were treated in private healthcare settings. Throughout the study period, the mean ATR incidence was 27.3 (CI = 26.9–27.6) per 100,000 person-years in the public sector and 2.6 (CI = 2.5–2.7) per 100,000 person-years in the private sector, with a combined incidence of 29.9 (CI = 29.5–30.2) per 100,000 person-years. The annual number of ATR patients increased toward the end of the study period; in 2019, the combined incidence was 32.3 (CI = 30.7–34.0) per 100,000 person-years. The introduction of the PHCR in 2011 also coincided with an increase in cases treated in public healthcare (Fig. 2). In public healthcare, the majority of patients were treated nonoperatively (10,997; 40% operative vs 16,303; 60% nonoperative), whereas in the private sector, the majority of the patients were treated operatively (2088; 80% operative vs 514; 20% nonoperative) (P < 0.001). Patients with ATRs received treatment from 65 different private healthcare providers and 264 different public healthcare providers during the study period.
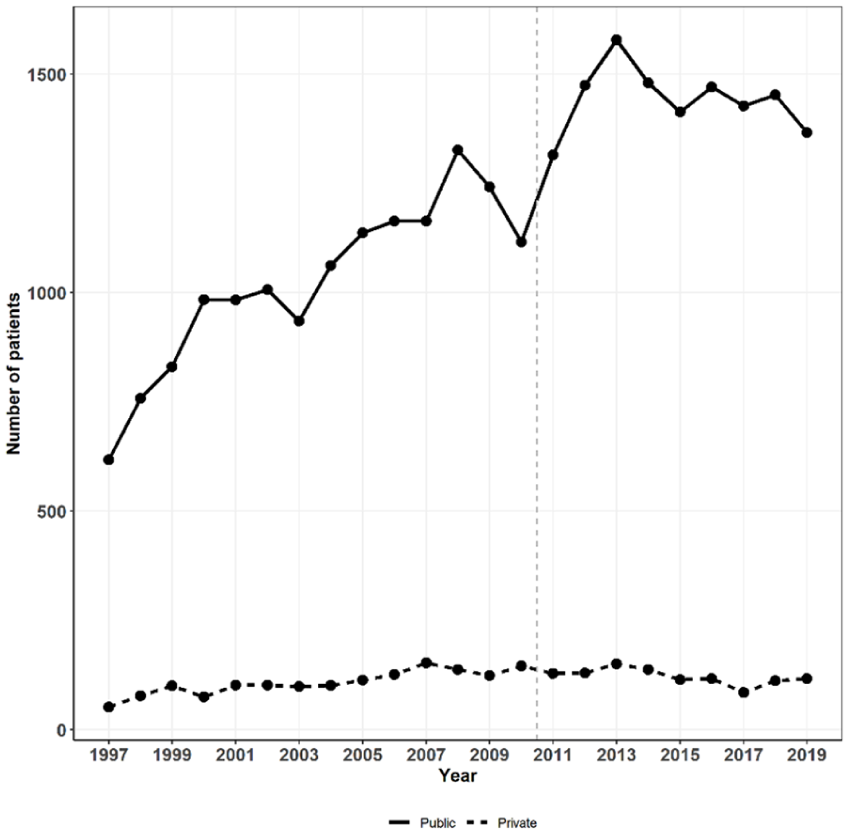
Publicly and privately treated patients by year.
Halfway through the study period, a significant change in the prevailing treatment method occurred in the public. The proportion of nonoperatively treated patients surpassed that of those treated operatively 2009 onward (Fig. 3A). No such change was observed in the private sector, where operative treatment remained dominant throughout the entire study period (Fig. 3B). This did not alter the overall trend in treatment modality, as the majority of patients are treated within the public sector (Fig. 3C).
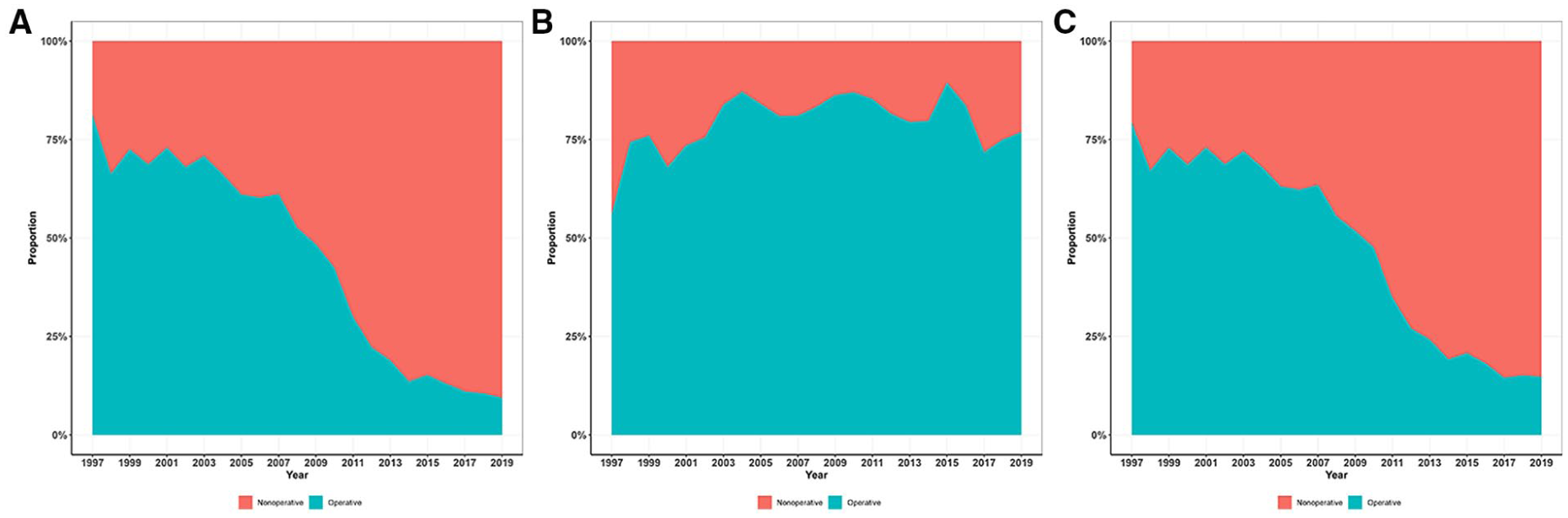
(A) Proportion of nonoperative versus operative treatment in public healthcare by year, (B) proportion of nonoperative versus operative treatment in private healthcare by year, and (C) proportion of nonoperative versus operative treatment in Finland by year.
During the whole study period, the mean age of patients with ATRs was 49 years (SD = 16, range = 16–101) in public healthcare and 45 years (SD 14, range = 16–89) in private healthcare, with an estimated difference of 4.1 years (CI = 3.5–4.6; Table 1). The overall proportion of female patients was 23% in public healthcare (20% operative vs 26% nonoperative) and 20% in private healthcare (19% operative vs 26% nonoperative). Male patients demonstrated a higher likelihood of seeking private treatment (male 9.0% vs female 7.8%; P = 0.001), particularly in the second half of the study period (2009–2019; male 8.7% vs female 6.6%; P < 0.001; Fig. 4).
Mean ages of patients treated in public versus private healthcare.
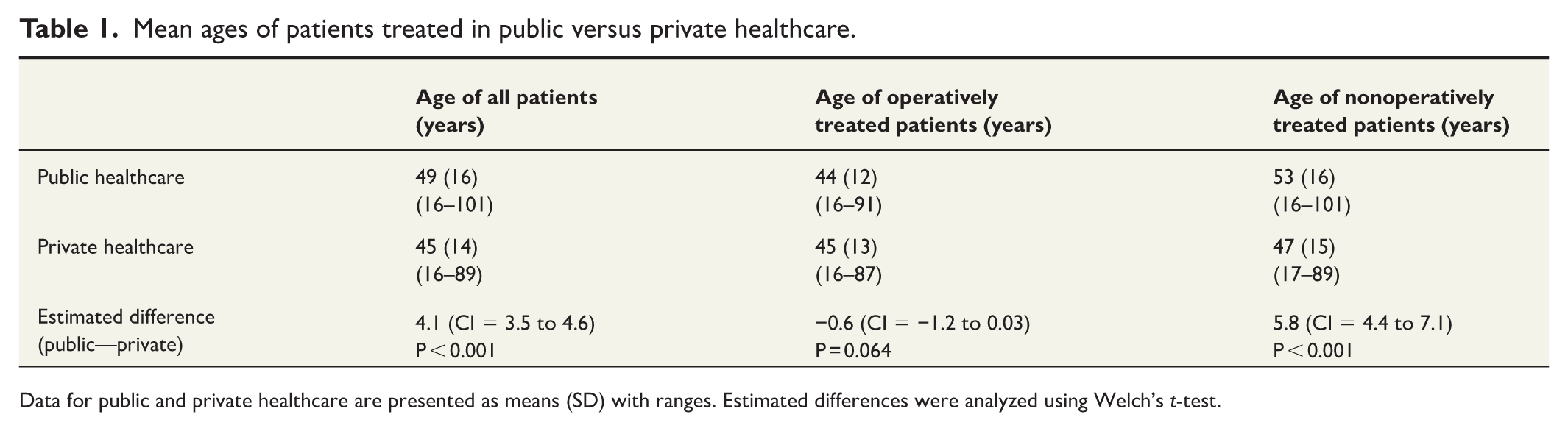
Data for public and private healthcare are presented as means (SD) with ranges. Estimated differences were analyzed using Welch’s t-test.
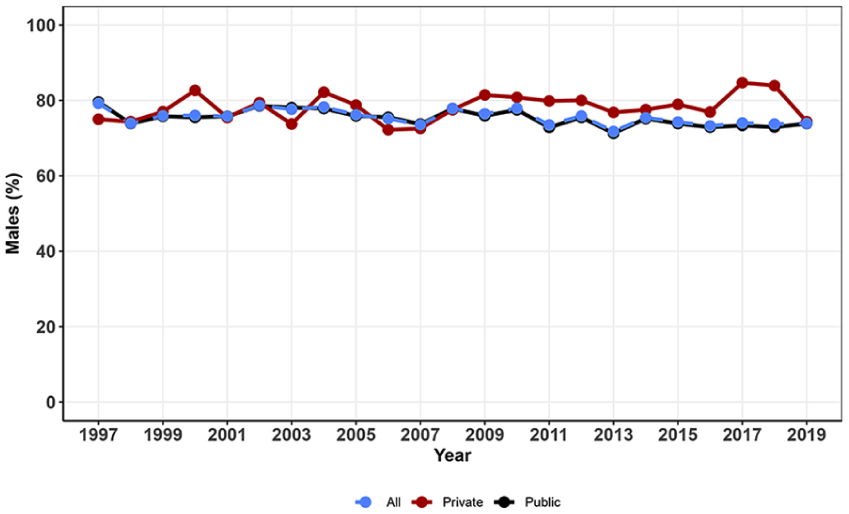
Proportion of male ATR patients during the study period.
Information about the external cause of injury was available for 65% of patients treated publicly and 42% of patients treated privately. This information was not available for any cases in the first 2 years of the study period (1997–1998), after which the data were increasingly reported and available. In publicly treated cases, the most common causes were sports (39%) and recreational injuries (37%), while privately treated cases had the highest proportion of undefined injuries (33%), followed by sports injuries (27%) (Table 2).
The causes of injury of patients treated in public versus private healthcare.

Discussion
In Finland, between 1997 and 2019, the incidence of ATR increased in the public sector but remained relatively stable in the private sector. Over this study period, public healthcare has seen a clear shift toward more nonoperative treatment methods, whereas no similar change was observed in the private sector.
A clear trend toward nonoperative ATR treatment was observed. Recent studies have shown that nonoperative treatment with early functional rehabilitation of acute midsubstance ATR offers similar functional outcomes while avoiding the risks associated with surgery, such as infections or sural nerve damage.5–8 Nonoperative treatment has been associated with a slightly higher risk of rerupture; however, with early functional rehabilitation, this increased risk has not been observed.8,19 Also, operatively treated ATRs have been found to recover plantar flexion strength 10%–18% better than nonoperatively treated ATRs. 20 The clinical significance of this is ambiguous but should be recognized when treating professional athletes and other patients with high physical demands. In both public and private healthcare, the risks and benefits of surgery of ATR should be individually assessed and discussed with the patient in a collaborative decision-making approach. In light of current literature, ATR surgery, at least for patients without high physical demands, might even be defined as a low-value procedure, in that it is harmful or produces little or no benefit to the patient. 21 In Finland, this has led to a nonoperative shift in treatment approach for ATRs. 3 In the present study, we observed a difference in treatment strategy, with public healthcare clearly shifting toward nonoperative options while operative treatment remained predominant in the private sector. Patients treated in the private sector were found to be slightly younger than those who received public healthcare treatment (45 vs 49), which may have contributed to this difference in treatment approaches. Ponkilaineno et al. 22 noted a decline in the incidence of some low-value orthopedic procedures in the private sector in Finland in recent years. The main factors of variation in low-value surgeries are the beliefs held by surgeons and patients regarding the effectiveness of the procedure.21,23 Reimbursement models and surgeon incentives may also influence the use of specific procedures. 23 Despite vast evidence supporting nonoperative treatment methods, there still seem to be differing opinions between the public and private sectors regarding treatment strategies for ATRs in Finland. One potential explanation may be that the uptake of research evidence is not as quick in the private sector as in public healthcare. Exposure to research may also vary from surgeon to surgeon. In the private sector, treatment decisions are solely made by the individual surgeon, meaning that their personal beliefs and preferences can significantly influence clinical choices. Furthermore, patients with health insurance who prefer surgical interventions may be more likely to seek care in the private sector. In addition, athletes’ licenses include insurance that covers treatment in the private sector, which naturally directs athletes to private care. This patient group is more likely to require surgical treatment due to their extremely high physical demands of their profession.
Several factors may contribute to patients opting for private care, including reduced waiting times, expedited access to specialized care, and the prioritization of faster interventions. In the context of occupational accidents, insurance companies frequently refer patients to private healthcare for treatment—in Finland, employers have a legal obligation to insure their staff. In addition, about one-fifth of Finnish adults have private health insurance, 11 which is most likely associated with the use of private healthcare. Paloneva et al. 24 identified a significantly increasing trend in rotator cuff repair surgeries in the private sector between 1998 and 2011. They proposed that there was a rise in the number of patients opting for private care to address shoulder conditions but did not determine the proportion of patients managed nonoperatively. Contrary to Paloneva et al.’s 24 study, the current study did not provide evidence of an increase in the use of private healthcare for ATRs. We hypothesize that, excluding insured athletes, individuals with post-injury walking difficulties tend to seek immediate care at always-open public emergency departments on short notice rather than determining whether they have adequate insurance to cover recreational injuries.
We found no significant differences in the causes of ATR between public and private healthcare settings. Sports injuries were most common in both public and private healthcare (20% vs 27%), and the proportions of patients receiving public or private treatment due to an occupational injury were also similar (7% vs 5%). Unfortunately, the reported external causes of injury were partially incomplete in our study, as information was available for 65% of patients treated publicly and 42% of patients treated privately. In addition, imprecise diagnosis codes, such as “undefined” and “other injuries,” were used. The ICD-10 coding system was implemented in Finland in 1996, which could explain the incomplete coding in the following years. However, the coding increased toward the end of the study period, probably due to the advancement of the electronic patient record system, which made the coding of external causes of injury mandatory.
This was an observational study based on administrative databases, and the results described how the incidence of and treatment approaches for ATRs have changed from 1997 to 2019 in the public and private healthcare sectors in Finland. Our aim was not to compare the results of different treatment methods or to provide recommendations for how ATRs should be treated.
We note several limitations in our study. First, the study was based on registry data and, therefore, retrospective, which introduces a risk of bias. For instance, it is possible that some patients treated in the private sector may have been in better health and possessed higher functional demands compared to those treated in the public sector. Second, we did not obtain data about functional outcomes or the length of sick leaves, meaning that we were unable to assess treatment outcomes between operatively and nonoperatively treated patients, although this was not an aim of the study. Furthermore, the ICD-10 classification does not have its own code for rerupture, avulsion, or partial rupture of the Achilles tendon. Although we did not believe that reruptures would be a significant course of bias in the study, we tried to minimize this risk by only including records with operative treatment within 30 days since the injury. It is possible that the 30-day window included some unsuccessful conservative treatments; however, this would not introduce bias to the comparison of public and private healthcare, as it applied to the entire study population. The data might have included cases with avulsions and partial ruptures. However, as avulsions are almost always treated operatively and partial ruptures nonoperatively, we did not believe that this would introduce bias in the operative versus nonoperative comparison.
Conclusion
The distribution of public and private treatment for ATRs remained consistent from 1997 to 2019. In the public sector, ATR treatment methods became noticeably more nonoperative over time, while no such change was observed in the private sector. In addition, patients treated in the private sector were found to be slightly younger, which may have contributed to this difference in treatment approaches.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A complete disclosure of interest according to the ICMJE is available upon request.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received research funding from the Finnish government.
Ethical approval
Ethical approval was obtained from the Finnish National Institute of Health and Welfare (permit no. THL/2266/5.05.00/2019).
Informed consent
Not needed for a register study.