
Abstract
Background and aims:
Current international guidelines recommend a center volume of at least 20 minimally invasive pancreatic procedures a year to perform laparoscopic left pancreatectomy. Iceland is a small, isolated country that is unavoidably low volume in terms of pancreatic surgery. To ensure good quality of care, there is a long tradition of surgeons training abroad, but this system has not been formally evaluated. The aim of this study was to evaluate the outcomes of laparoscopic and open left pancreatectomy over the last 20 years in Iceland.
Methods:
This was a national retrospective cohort study including all patients who underwent left-sided pancreatic resection in Iceland from 2003 to 2022.
Results:
A total of 244 patients underwent a pancreatic procedure during the study period. Eighty of these underwent left-sided resections, 41 of whom had a laparoscopic left pancreatectomy (LLP). Resection rates increased over the study period, and a significantly larger proportion of patients underwent LLP in the latter half of the study period. The laparoscopy group had statistically significantly lower rates of splenectomy (<0.001) and blood loss (<0.001) compared with open surgery. The morbidity rate of severe complications (Clavien–Dindo grade IIIa or higher) was 23%. The in-hospital and 90-day mortality rates were 1% and 4%, respectively.
Conclusions:
Overall, the operative and postoperative outcomes of left-sided pancreatic resections in a low-volume setting in Iceland were comparable to current reported studies from other Western countries.
Clinical trial registration number:
NCT06738914.
Keywords
Context and Relevance
This study describes the early implementation and use of laparoscopic and open left-sided pancreatectomy in a tertiary referral hospital in Iceland over the past two decades. Although the country is small and pancreatic procedures are by necessity few, operative and postoperative outcomes after left-sided pancreatectomy were comparable to those in other Western countries, and 65% of patients achieved an ideal outcome. The current system of training surgeons abroad in higher-volume centers therefore seems to be a good policy for pancreatic centers that are by necessity low in volume. Future efforts should focus on detecting and treating complications early, avoiding routine drains postoperatively, and being vigilant with the preoperative workup.
Introduction
Minimally invasive pancreatic surgery was first reported in the 1990s 1 and has since steadily increased in popularity. Minimally invasive left pancreatectomy has been shown to result in a shorter time to functional recovery, a shorter hospital stay, less blood loss, and a comparable complication rate to an open operation2,3 while being oncologically equivalent. 4
The question of volume in pancreatic surgery has been a growing topic over the last few decades, with many studies indicating an advantage in terms of the rate of resections, rate of radical resections, and short-term and overall mortality with increasing hospital volume.5–8 Current international guidelines in terms of training in minimally invasive pancreatic surgery recommend an annual hospital volume of at least 50 pancreatoduodenectomies and 10 left pancreatectomies (LPs) to enter a training program. 9 The recent Brescia international guidelines on minimally invasive pancreatic surgery recommend a center volume of at least 20 laparoscopic pancreatic procedures per year to perform these operations. However, they also acknowledge that a lower annual volume might be acceptable if there is a well-trained multidisciplinary pancreas team and if the center can demonstrate acceptable outcomes. 10
Iceland is a small and isolated country between the North Atlantic and Arctic Oceans, with a population of approximately 380,000 people. 11 Landspitali, the National University Hospital of Iceland, is the tertiary referral center performing all malignant gastrointestinal surgery in the country and faces the challenge of maintaining a good quality of HPB surgery while unavoidably being a low-volume hospital with respect to these procedures. To ensure good quality care and enough operative experience among surgeons, the country has a long tradition of training specialists overseas in northern Europe and North America. However, the outcomes of pancreatic surgery, particularly minimally invasive pancreatic surgery, in Iceland have not been published. The aim of this study was therefore to evaluate the outcomes of laparoscopic and open left-sided pancreatectomy (OLP) in Iceland over the past two decades.
Methods
Study design
This was a national cohort study in which all patients who underwent a left-sided pancreatic operation between 2003 and 2022 in Iceland were retrospectively studied. The data were obtained retrospectively from patients’ medical records. As all available patients were included, no power calculation was performed.
Variables
Postpancreatectomy hemorrhage (PPH), postoperative pancreatic fistula (POPF), and delayed gastric emptying (DGE) were defined using the International Study Group of Pancreatic Surgery definitions and included only grade B and C complications.12–14 Blood loss was obtained from the anesthesiology report from the operations when available and otherwise from the surgeon’s estimation. Severe complications were defined as those rated Clavien–Dindo grade IIIa or higher. 15 Ideal outcome was defined as the absence of severe complications, clinically relevant POPF, reoperation, readmission, in-hospital mortality, and a hospital stay over the 75th percentile in this study cohort. 16 The type of left-sided resection was defined according to van Ramshorst et al. 17
Statistical analyses
Statistical analyses were performed using SPSS Statistics 28.0 for Windows (IBM, Armonk, NY, USA). Numerical variables were compared using Student’s t-test or the Mann‒Whitney U-test, as appropriate. Categorical variables were compared using the χ2 test or Fisher’s exact test. Missing data were reported along with the results. A p-value <0.05 was considered significant.
This study was approved by the National Bioethics Committee in Iceland, number VSN-24-124, and the Scientific Committee of Landspitali University Hospital. As this was a retrospective cohort study and no individual cases could be identified in the results, it was not deemed necessary to obtain informed consent from the participants.
Results
During the study period, 244 patients underwent pancreatic surgery in Iceland, 97 of whom underwent left-sided pancreatic resection. After excluding patients who had undergone pancreatic tail resection as part of another operation, 80 patients remained in the study (Figure 1).
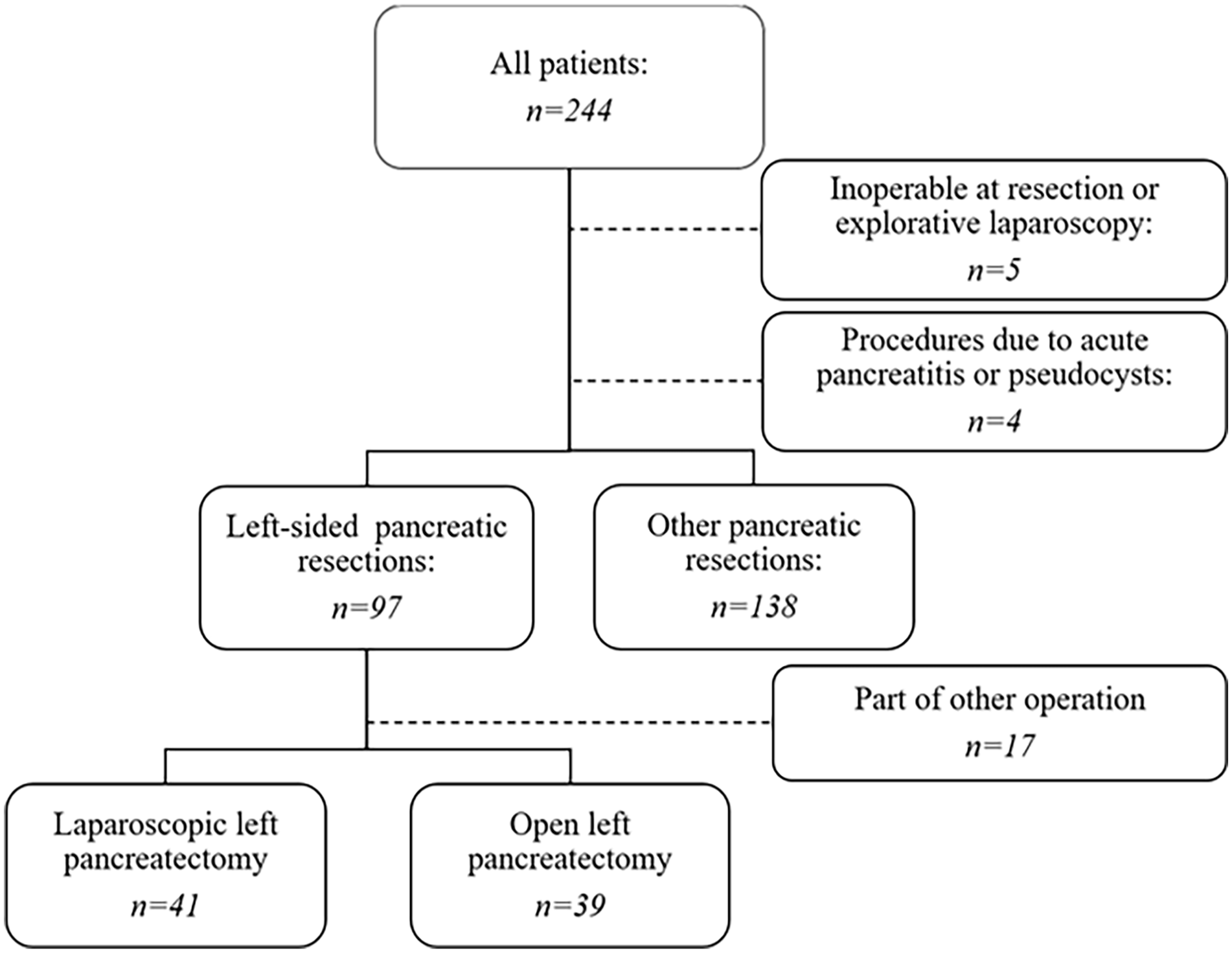
Flow chart of patients who underwent pancreatic procedures in Iceland from 2003 to 2022.
Approximately half of the patients underwent laparoscopic surgery. Resection rates increased in the latter half of the study period, when a larger proportion of patients also underwent surgery with a laparoscopic technique. A significantly greater proportion of patients in the open group had diabetes and preoperative weight loss. Otherwise, no significant differences were observed between the groups regarding preoperative comorbidities or the preoperative workup (Table 1).
Demographic data, comorbidities, and preoperative workup data.
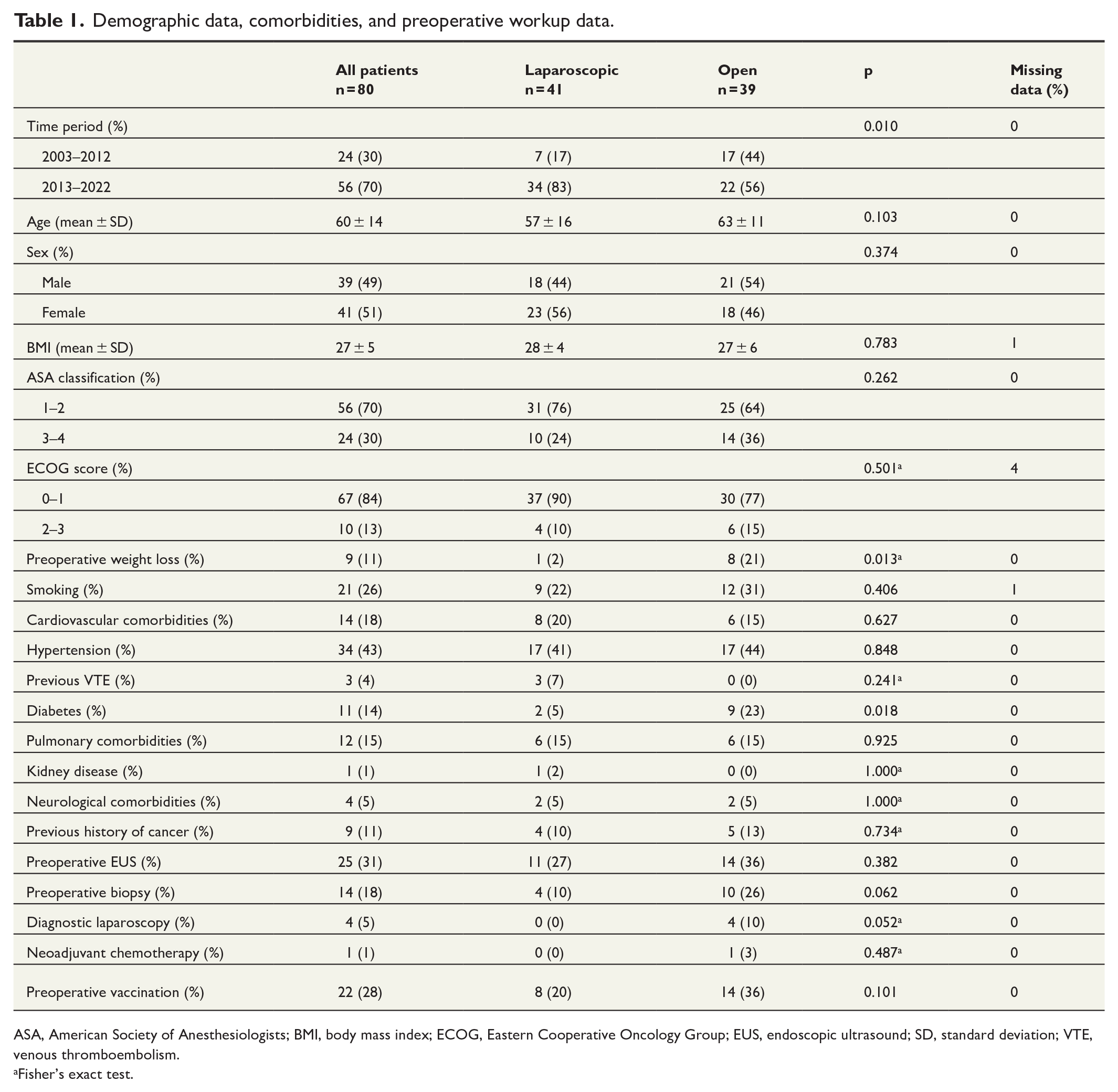
ASA, American Society of Anesthesiologists; BMI, body mass index; ECOG, Eastern Cooperative Oncology Group; EUS, endoscopic ultrasound; SD, standard deviation; VTE, venous thromboembolism.
Fisher’s exact test.
The majority of patients underwent body and tail resection or tail resection only. Four patients, all in the open group, underwent neck, body, and tail resection, that is, division of the pancreas to the right of the superior mesenteric vein. 17 Two patients underwent additional organ resection (stomach and colon). The rates of splenectomy and amount of blood loss were significantly lower in the laparoscopic group. Fifteen percent of operations in the laparoscopic group were converted to open operations. The rate of pancreatic ductal adenocarcinoma (PDAC) was significantly lower in the laparoscopic group. Among the patients who underwent surgery for metastases, three had renal cancer, and one had colorectal cancer (Table 2).
Operation and diagnosis.
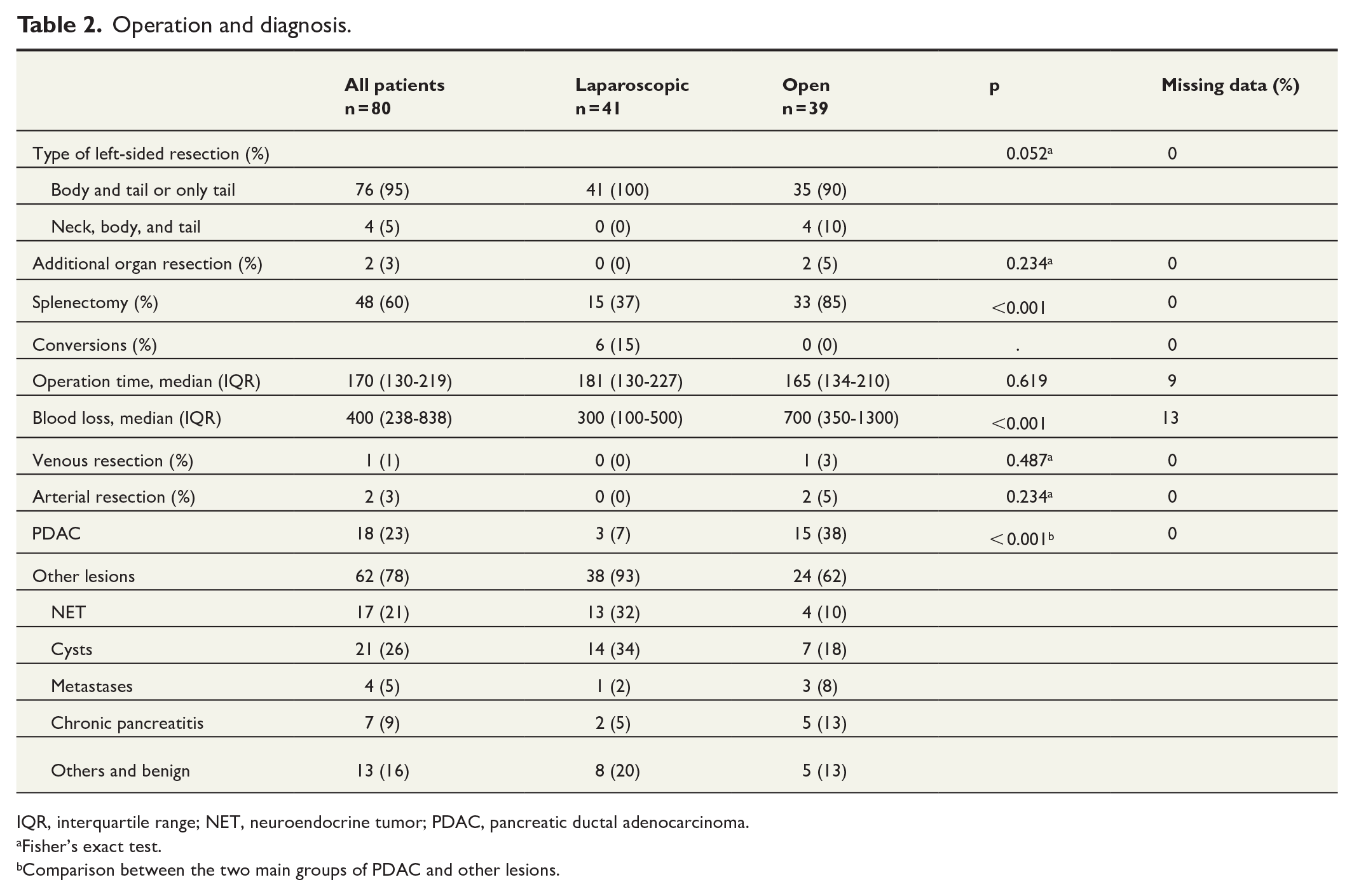
IQR, interquartile range; NET, neuroendocrine tumor; PDAC, pancreatic ductal adenocarcinoma.
Fisher’s exact test.
Comparison between the two main groups of PDAC and other lesions.
Postoperatively, the only variable that differed significantly between the groups was the length of hospital stay, which was shorter in the laparoscopic group. The rate of clinically relevant pancreatic fistulas was non-significantly greater in the laparoscopic group, whereas the rates of severe complications according to the Clavien–Dindo classification, DGE, unplanned intensive care, and medical complications were non-significantly higher in the open group. Sixty-five percent of patients achieved an ideal outcome, and the in-hospital and 90-day mortality rates were 1% and 4%, respectively (Table 3).
Postoperative course.
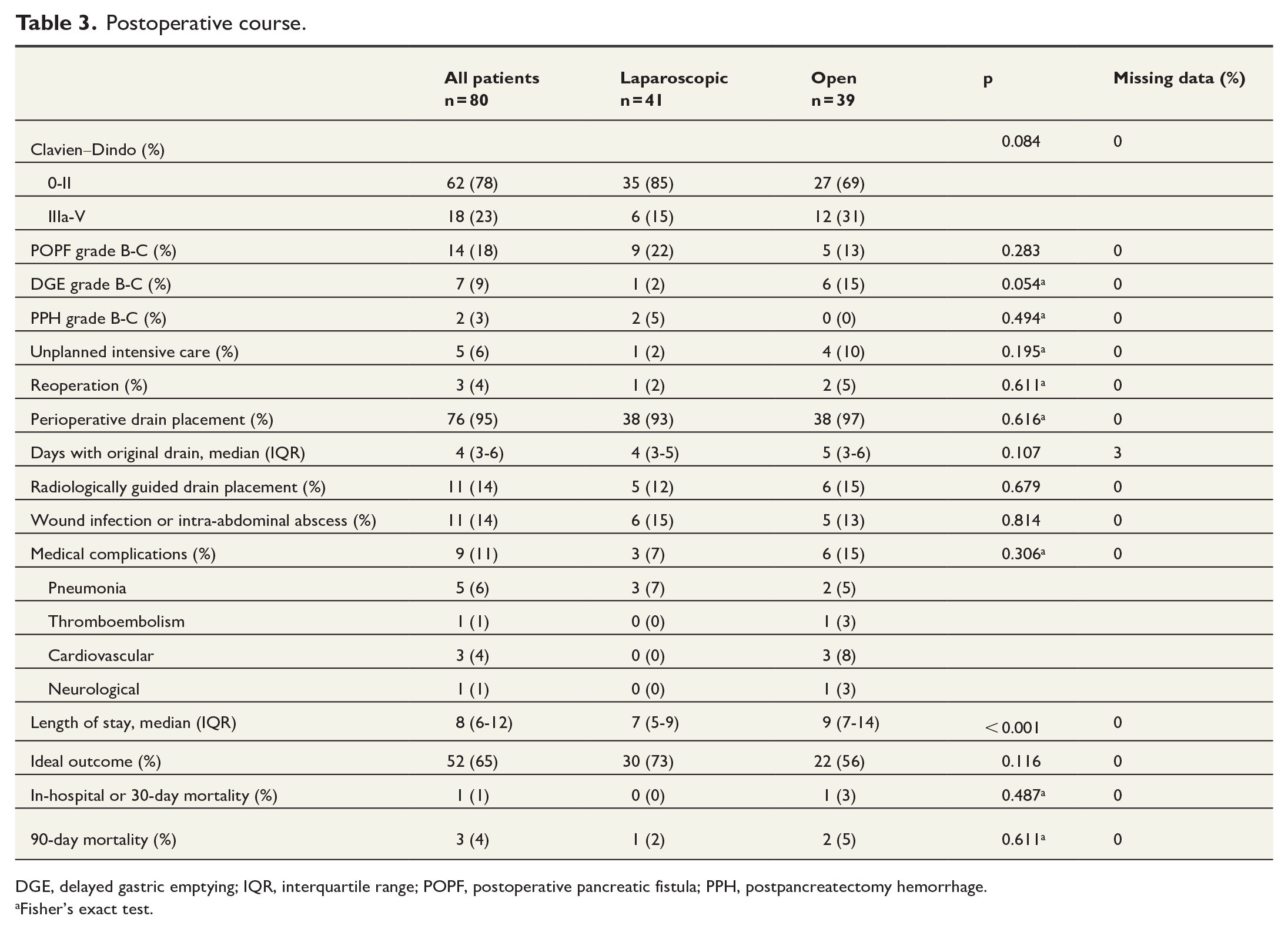
DGE, delayed gastric emptying; IQR, interquartile range; POPF, postoperative pancreatic fistula; PPH, postpancreatectomy hemorrhage.
Fisher’s exact test.
Among the patients with pancreatic cancer, the majority had stage II tumors, followed by stage I tumors. Ten patients received adjuvant chemotherapy. The median overall survival among patients with PDAC was 1.2 years, and the disease-free survival was 0.7 years (Table 4). Among patients with neuroendocrine tumors, the majority were grade 1 (Table 5).
Histopathological data, chemotherapy use, and survival among patients with pancreatic ductal adenocarcinoma.
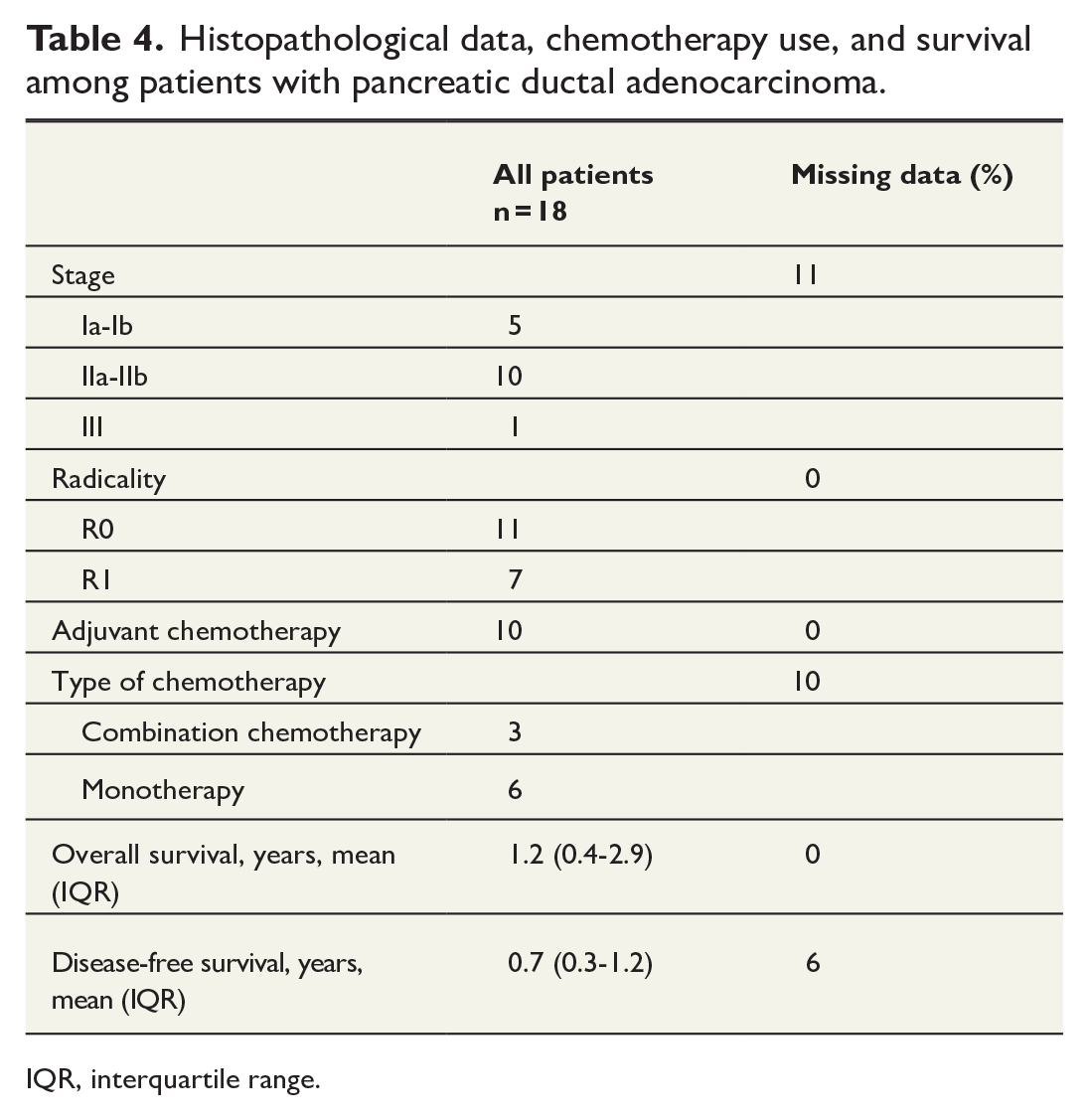
IQR, interquartile range.
Histopathological data and survival among patients with neuroendocrine tumors.
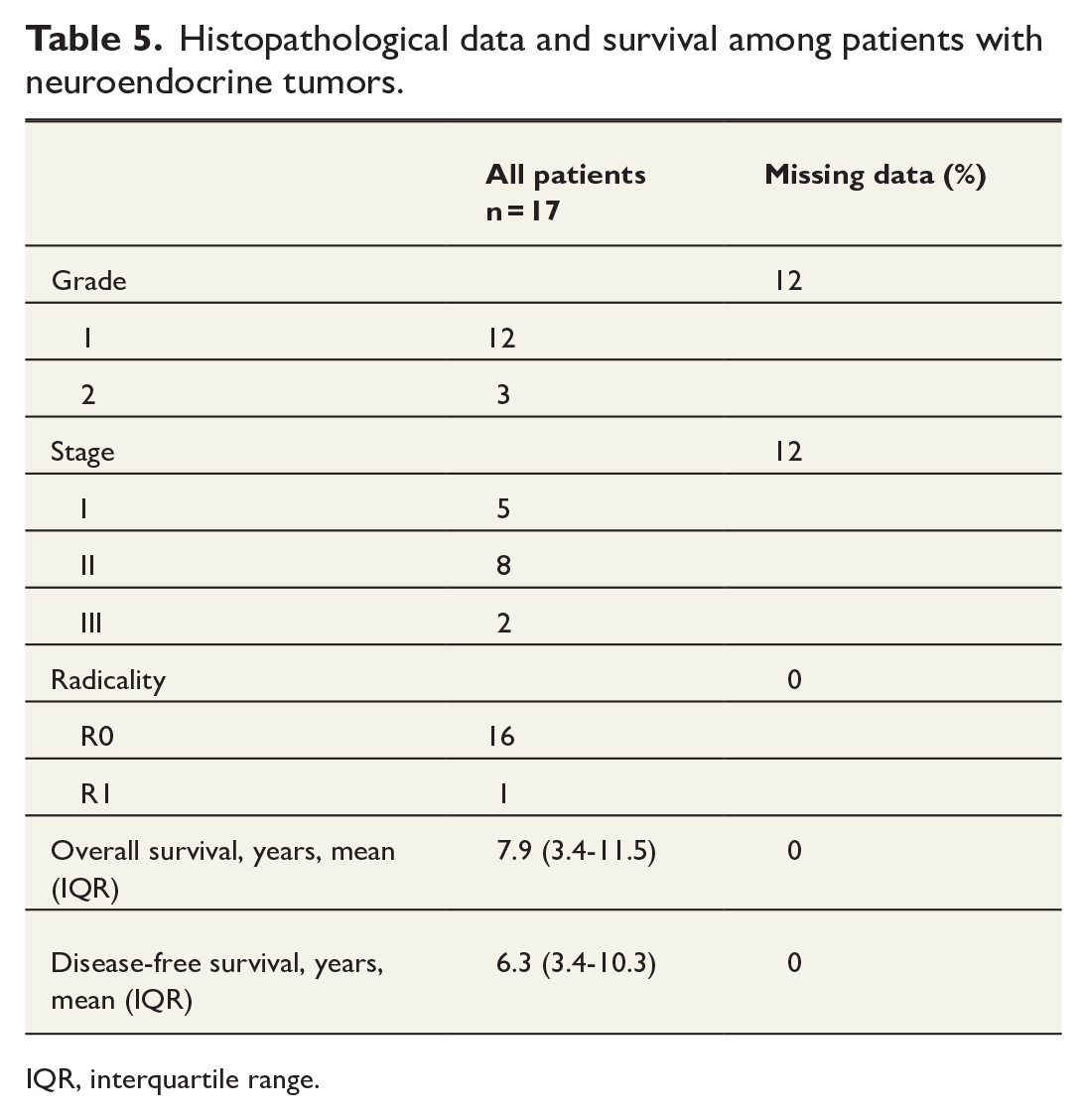
IQR, interquartile range.
Among the three patients who died within 90 days, all had poorly differentiated adenocarcinoma of the pancreas, two of whom experienced early recurrence after the operation that was discovered only 4 and 16 days postoperatively, respectively. The third patient died of postoperative complications.
Discussion
In this national cohort study of laparoscopic and open left pancreatectomy in a small-volume hospital over the past two decades, Iceland was shown to have implemented laparoscopic surgery very early and had a marginal majority of operations performed as laparoscopic operations during the study period. This is remarkable compared with recent figures from the Global Audits on Pancreatic Surgery Group (GAPASURG) collaboration encompassing data from the Netherlands, Sweden, Germany, and North America, where only the Netherlands had a majority of resections performed as minimally invasive resections over a study period from 2014 to 2020. 18
When examining quality indicators such as operation time, conversion, and spleen preservation, the results of the current study were comparable to those of more recent studies from other Western countries.2,4,18,19 Blood loss was higher than expected, with a median of 400 mL for the entire cohort, which is greater than what has commonly been reported elsewhere.2–4 The high number could be an effect of the study period beginning in 2003, as it is comparable to other reports from the early 2000s. 20 In addition, there is considerable diversity among studies in terms of how blood loss is estimated, which might also have affected the results. 21
In terms of postoperative outcomes, 65% of the patients in this study had an ideal outcome, non-significantly greater in the laparoscopic group. The ideal outcome is a relatively new composite outcome measure in pancreatic surgery and has been argued to be a more accurate measure of postoperative outcomes than individual factors such as mortality or complications. 16 In a recent study based on the GAPASURG collaboration mentioned above regarding ideal outcome after minimally invasive and OLP among over 20 000 patients, an overall rate of 59% was reported, significantly higher in the minimally invasive group. 22
Among postoperative complications, the rate of severe complications was comparable to that reported in other Western countries in recent years,2,4 but the rate of clinically relevant pancreatic fistulas was on the lower side.2,19 As shown very elegantly in the recently published PORSCH trial, early diagnosis of and intervention in complications after pancreatic surgery results by definition in a higher rate of Clavien–Dindo ⩾III and clinically relevant POPF but ultimately benefits the patients, as shown by lower rates of bleeding requiring intervention, organ failure, and mortality. 23
When comparing laparoscopic and open operations, this study reported less blood loss and a shorter length of stay in the laparoscopic group, which is in line with results from randomized studies.2,3 The results in this study showed a lower rate of splenectomy in the laparoscopic group as well. The rate of perioperative drain placement in this study was very high at 95%. While there have been previous publications casting doubt on the necessity of placing perioperative drains in patients undergoing left-sided pancreatectomy, 24 the recently published, binational PANDORINA randomized controlled trial clearly revealed that routine drain placement leads to a higher rate of overall complications as well as pancreatic fistulas without conferring any advantages. 19
In terms of mortality, one patient died within 30 days, which seems to be on par with other studies from Western countries.2,18 However, three patients died within 90 days, resulting in a 90-day mortality rate of 4%, which is higher than the figures reported elsewhere.4,19 In these patients, the cause of death was purely related to complications in one patient, whereas the other two patients experienced early disease recurrence in combination with postoperative complications. This suggests a need to be more vigilant with preoperative investigations to avoid unnecessary surgery in patients who will not benefit from it. Importantly, in the earlier part of the study period, patients were not as a rule discussed at a multidisciplinary meeting before surgery.
This study had several limitations. First, this was a retrospective study, and the data were collected from medical records, which make it slightly more uncertain than prospectively collected data. Second, the patient cohort was small, which made the analyses quite underpowered when comparing the two operation methods. However, as the main aim of the study was to evaluate outcomes in this small available cohort in comparison with international figures from high-volume centers, the methodology was deemed adequate.
Conclusion
In this national study evaluating 20 years of laparoscopic and open left-sided pancreatectomies in Iceland, a high rate of laparoscopic resections was shown, even compared with more recent data from other Western countries. Operative and postoperative outcomes were generally similar to those reported in other countries, and the proportion of patients with ideal outcome was high. This finding indicates that the current system of training surgeons overseas is an effective way for small-volume hospitals to ensure high-quality pancreatic surgery. In the future, important improvements can be achieved by avoiding routine placement of drains after left-sided resections, focusing on detecting and treating complications early, and being vigilant with the preoperative workup among PDAC patients to avoid unnecessary operations.
Footnotes
Author contributions
K.J.: Concept and design; data collection, analysis and interpretation; drafting of the article; approval of the final version before publication.
G.B.: Interpretation of data; critical revision of the article; approval of the final version before publication.
K.H.H.: Concept and design; interpretation of data; critical revision of the article; approval of the final version before publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.