
Abstract
Dear Editor,
Colorectal cancer (CRC) is a leading cause of cancer-related mortality, with liver metastases being the most common site of distant metastases. Liver transplantation (LT) for colorectal liver metastases (CRLM) has demonstrated promising survival outcomes in recent trials, reporting 5-year overall survival (OS) rates between 60% and 83%. 1 However, organ scarcity remains a significant barrier to LT being implemented as a standard of care for selected patients. Living donor liver transplantation (LDLT), using segments 2 + 3 grafts using the RAPID technique, offers a potential solution with reduced donor risk. Since LDLT usually requires voluntary family donors, understanding their attitudes toward donation is critical.
A survey was conducted among three cohorts: (1) next of kin to patients who had undergone LT for CRLM within the SECA I-II LT trials, 1 (2) next of kin to CRC patients ineligible for LT or liver resection, and (3) healthcare workers with a healthy next of kin, instructed to answer as if their relative had CRLM. The original survey in Norwegian is included in the Supplementary Material (Supplement 1). Respondents answered questions regarding their willingness to donate and the minimum survival benefit required to justify donation. Statistical analyses were performed using chi-square tests, with a significance threshold of p < 0.05.
Eighty-two individuals participated: 32 from the SECA LT cohort, 20 from the ineligible CRC cohort, and 30 healthcare workers. All respondents expressed willingness to donate, with 78% (64/82) agreeing if donation extended survival by 6 months to 1 year (Fig. 1). A longer survival benefit of 5 years or more was required by only 5%.
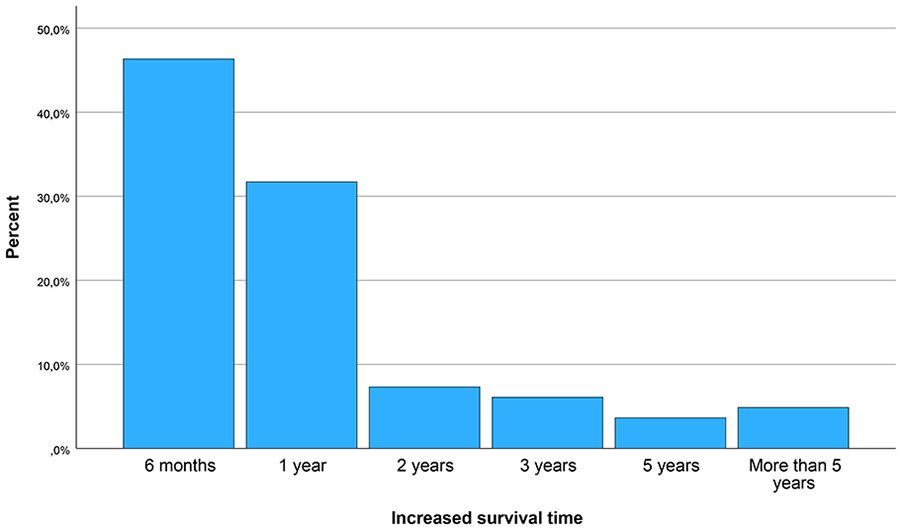
Bar chart showing the willingness of next of kin to donate liver segment 2 + 3 given the probability of the various expected increased survival times.
Children, siblings, or parents were significantly more likely (87%, n = 39) to accept a survival benefit of ≤1 year compared to spouses or partners (67%, n = 25, p = 0.038). No differences were observed regarding donor sex (p = 0.78), patient sex (p = 0.82), or patient age (above or under the median of 52 years, p = 0.31). The willingness to donate for an expected survival increase of 6 months to 1 year was similar across cohorts: 88% (28/32) in the SECA group, 70% (14/20) in the metastatic CRC group, and 73% (22/30) in healthcare workers (p = 0.10).
LT for CRLM has been primarily restricted to non-resectable disease; however, even patients with resectable disease and high tumor burden may benefit from LT compared to liver resection. Expanding LT for resectable CRLM would exacerbate donor shortages, making LDLT an attractive alternative. Traditional LDLT, involving right lobe donation, carries a donor morbidity rate of 30-35% and a mortality risk of 0.2%–0.3%. In contrast, segment 2 + 3 donation, especially via laparoscopic techniques, has a lower risk, comparable to kidney donation (mortality ~0.03%).2,3
The RAPID technique has demonstrated favorable donor safety, with 4.3% morbidity and no mortality in a cohort of 23 procedures. 4 Five-year OS rates of 70%–80% in selected LT recipients underscore the survival advantage over standard therapies, which has recently been shown in the randomized TRANSMET trial. 5 Cost-effectiveness analyses further support LT for CRLM when the median OS exceeds 3 years. 6
This study indicates that families are willing to donate even for a survival extension of only 6–12 months. However, this survival threshold is below what justifies LDLT, necessitating strict donor–recipient selection criteria. The international transplant oncology community generally considers a 5-year OS of ≥50% acceptable for LT for this indication.
Potential biases include self-selection, as those with negative views may have opted not to respond, and the influence of knowledge about LT benefits among SECA cohort families and healthcare workers.
The high willingness to donate suggests that LDLT is feasible for CRLM patients in Norway and also likely in other countries. These findings are crucial for designing future protocols for LDLT in selected CRLM patients; however, strict selection criteria must remain to ensure ethical and clinical justification.
Supplemental Material
sj-pdf-1-sjs-10.1177_14574969251335467 – Supplemental material for Assessing the attitudes of next of kin toward living donor liver transplantation for patients with colorectal liver metastases
Supplemental material, sj-pdf-1-sjs-10.1177_14574969251335467 for Assessing the attitudes of next of kin toward living donor liver transplantation for patients with colorectal liver metastases by Tor M. Smedman, Pål-Dag Line and Svein Dueland in Scandinavian Journal of Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Oslo University Hospital, the Norwegian Cancer Society, and the South-Eastern Norway Regional Health Authority.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki. Ethical review and approval were waived for this study due to the anonymity of the survey.
Informed consent
Informed consent statement was not applicable due to the anonymous nature of the survey.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.