
Abstract
Background and Aims:
The majority of neurogenic thoracic outlet syndrome (NTOS) surgery still involves removal of the first rib. A rib-sparing procedure has also been found to give a good result, but no meta-analysis has been published about this procedure. Also, from a financial point of view, it is important to know what kind of results have been obtained in the treatment of NTOS with rib-sparing surgery. Our opinion is that first-rib resection (FRR) surgeries, which contain more complications and require a longer recovery time, are performed too often these days, if the same result is achieved with rib-sparing surgery.
Methods:
We accomplished a systematic review and meta-analysis to find out the outcome of rib-sparing NTOS surgery, collecting studies on rib-sparing supraclavicular scalenotomy in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines using appropriate databases.
Results:
Of 1354 studies, 18 studies met our inclusion criteria. The mean study sample size was 58, and the mean patient age at surgery was 35.8 years. All studies reported long-term outcomes, with the mean follow-up time of 49 months. All reported fewer patient complaints after surgical TOS treatment. In our meta-analysis, improvement to Derkash’s excellent/good classifications was achieved in 71% (95% confidence interval (CI) = 64.4% to 76.4%, I2 = 73.0%). The heterogeneity noted in the systematic review showed no significant moderation by gender, age, or follow-up time. The studies included had a low risk of publication bias, with most failing to use validated evaluation methods.
Conclusion:
According to this analysis, the rib-sparing surgical treatment of NTOS is beneficial to most patients and relatively safe. Still, future studies should accommodate validated thoracic outlet scales.
Type of study / level of evidence:
Therapeutic IV
Introduction
Neurogenic thoracic outlet syndrome (NTOS) is the collective name for complaints caused by symptomatic compression of the brachial plexus. Because of the wide range of etiologies and lack of expert consensus for diagnostic testing, the true incidence of thoracic outlet syndrome (TOS) is difficult to discern. Illig et al. 1 estimated, based on a prospectively maintained database at their academic Thoracic Outlet Center, that the incidence of neurogenic thoracic outlet syndrome is approximately 2.5 per 100,000 population. In France, the incidence has been reported to be three to four cases per 100,000 people per year (Abraham et al. 2 ). Since NTOS symptoms often last for years despite treatment, it is obvious that the prevalence of NTOS is significantly higher. In fact, Edwards et al. 3 suggested a prevalence for TOS of at least 10 per 100,000 per year. NTOS especially affects young people with diverse pathologies and includes a range of symptoms related to the neck, head, and upper limbs. Patients may present with pain, weakness, numbness, and paraesthesia. An NTOS diagnosis may be demanding, as it is mainly based on patient history, physical examination, and provocative tests. Differential diagnosis is also crucial and may feature X-rays, Doppler ultrasounds, computed tomography (CT) and magnetic resonance imaging (MRI) scans, angiography, and electroneuromyography (ENMG). 4
For patients with NTOS, an initial period of nonsurgical treatment with physiotherapy often serves as the first line of treatment, as a considerable number of patients can be successfully treated conservatively. Physiotherapy is often beneficial, especially in mild forms of NTOS,5,6 but can also be ineffective. 7 Failure to improve often leads to surgical therapy, which consists of decompression of the thoracic outlet with or without rib resection. The three operative methods are scalenotomy or scalenectomy, resection of the first rib, and scalenotomy plus resection of the first rib.
The surgical management of NTOS has, among surgeons, been a controversial topic. Objective diagnostic and outcome criteria are lacking, and selection of patients with NTOS who will truly benefit from surgical management has been difficult. A dearth of clinical NTOS tests to serve as outcome predictors is also a problem. To date, Ghamari et al. 8 have used five generic outcome measures for NTOS patients to assess their intervention outcomes. Current clinical tests show good sensitivity but poor specificity, and they fail to reliably predict outcomes. 9 The new validated Thoracic Outlet Syndrome Index (TOSI) may prove useful for outcome measurement, however. 10 Although short-term results show the resolution of NTOS symptoms in as high as 90% of patients,8,11 long-term studies have shown a gradual deterioration in results over time to as low as 50% to 60%.12,13
The long-term results of differing NTOS treatment methods are especially rare. There remains a lack of consensus on the most appropriate surgical approach in NTOS management, 14 although many studies have compared the results of various operative methods.15–19 Objective critical data regarding the success of such treatments are conspicuously lacking, as well. 6 Notably, however, after supraclavicular release without rib resection in NTOS patients, pain, numbness, powerlessness, and daily harm have significantly decreased. 15 Povlsen et al. 20 similarly stated that evidence that transaxillary first-rib resection reduces pain more than does supraclavicular neuroplasty. Their data is of very low-quality, but no randomized evidence exists that demonstrates the superiority of surgery over no treatment. Reports on predicting preoperative or operative factors are particularly rare. One Cochrane review is available, but it only includes randomized or quasi-randomized trials. 20
We already adopted rib-sparing surgery decades ago 21 and thus aim to accomplish a systematic review and meta-analysis to ascertain the outcomes of supraclavicular rib-sparing surgery as NTOS treatment.
Methods
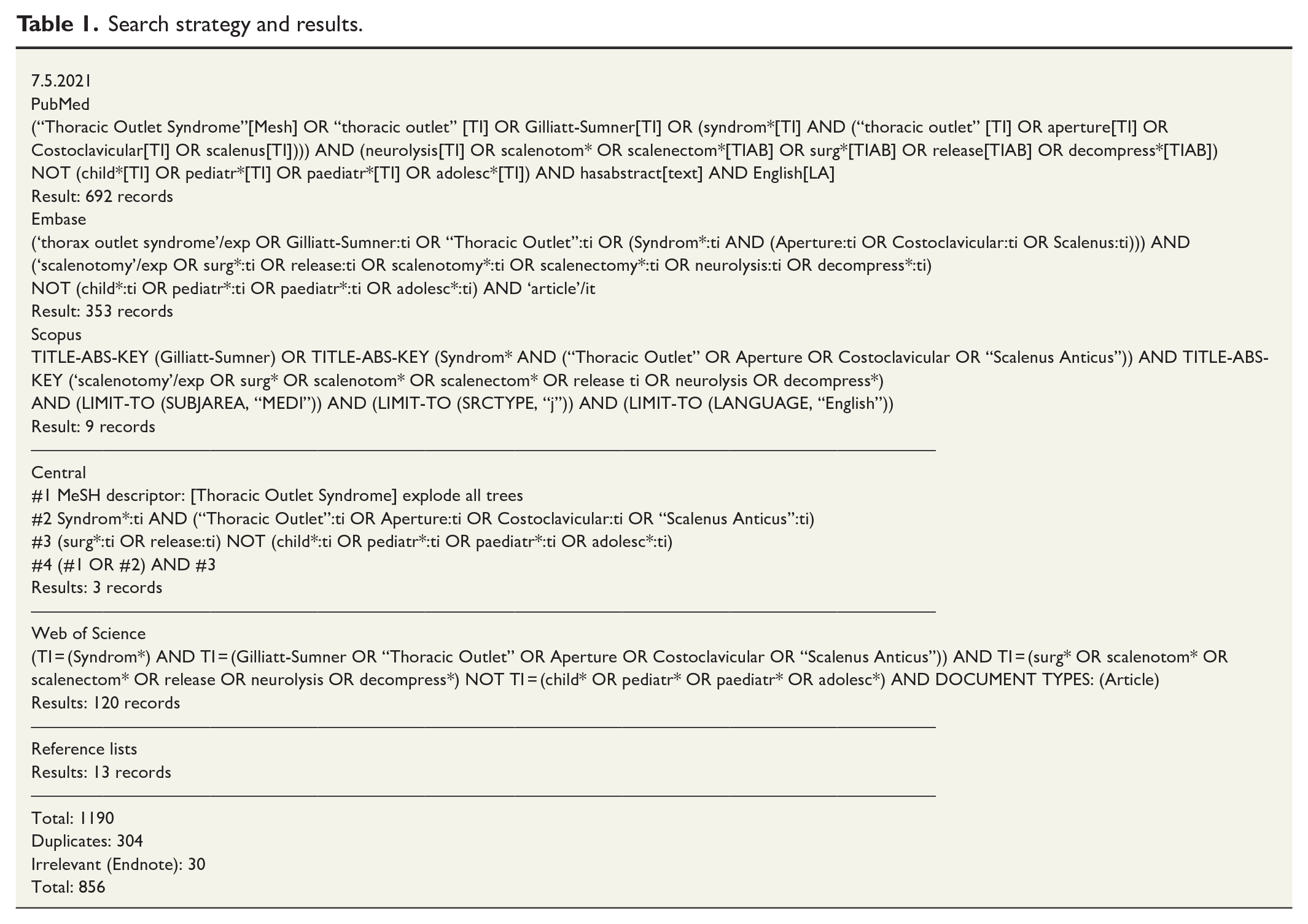
This report was written in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting systematic reviews and meta-analyses, 22 as well as being registered with PROSPERO (CRD42015026255). The PubMed, EMBASE, Web of Science, Scopus, and Central databases were reviewed for English-, Swedish-, or German-language human studies published between the databases’ inceptions and October 2022. The “related articles” function in PubMed and the reference lists of the initially retrieved articles also served to identify articles not found in the original search. The search strategy and results are in Table 1.
Search strategy and results.
Inclusion and exclusion criteria
The inclusion criteria were (1) being studies on rib-sparing supraclavicular scalenotomy; (2) published in English, Swedish, or German; (3) with postoperatively described subjective and possibly objective outcomes; (4) having a sample size of ≥10 patients; and (5) a mean follow-up duration of ≥1 year. The exclusion criteria were (1) an unavailable full text; (2) being pediatric research; (3) research concerning rib resection or endoscopic-assisted surgery; and (4) studies performed on nonhumans or cadaveric specimens. If the study concerned both scalenectomy and first-rib resection, the data of the separate outcomes had to be distinguishable. We accepted the diagnosis of NTOS by researchers in the studies included.
Data extraction and assessment
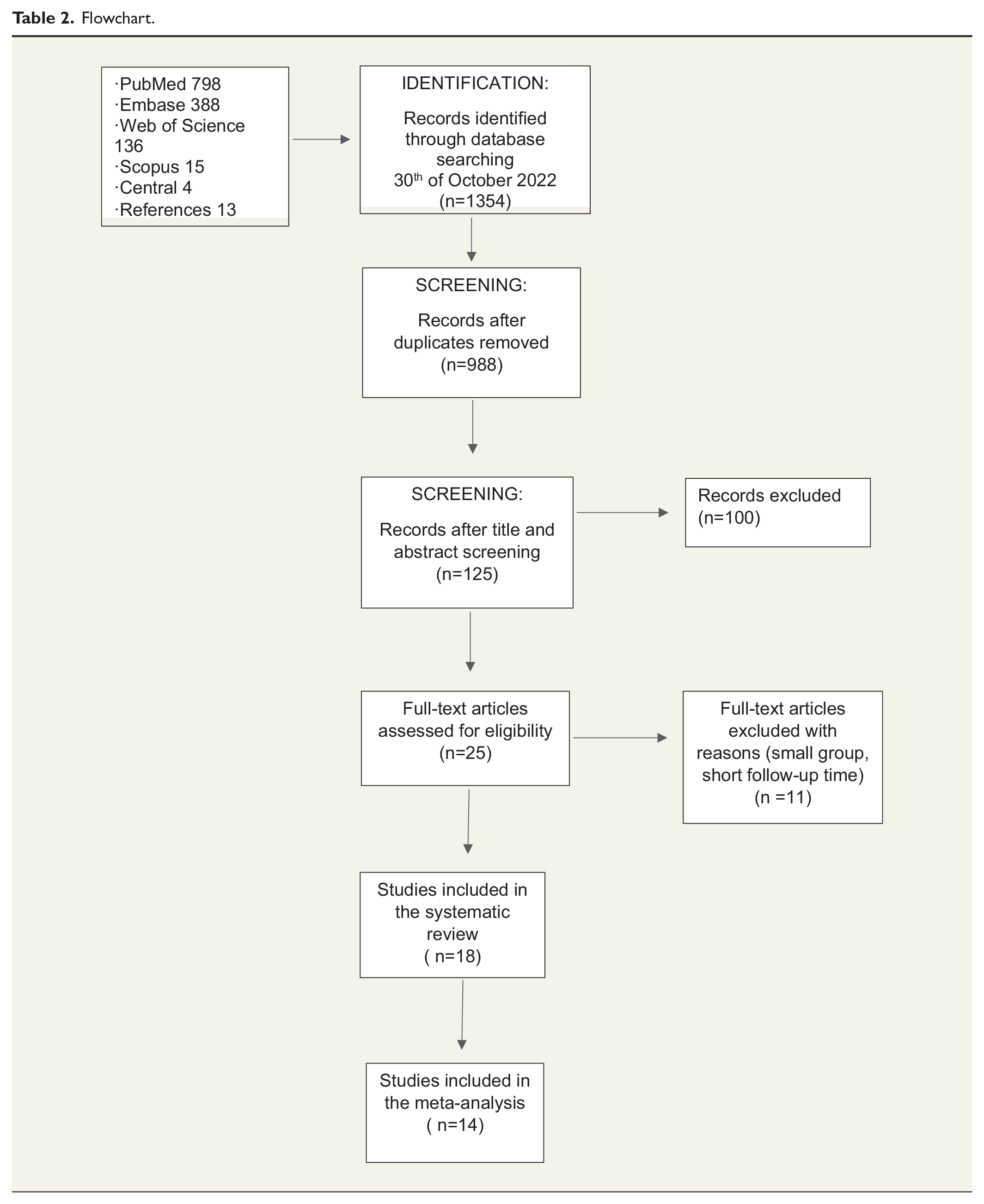
Two authors (M.V., H.V.) independently assessed all abstracts to determine their suitability, with full text analysis performed in case of uncertainty. The same two authors then independently extracted data from all the approved full texts. Discrepancies were resolved through discussion with the third author (N.R.). The data extracted were study design, lead author, publication year, population size, outcome measurements, type of intervention, complications, and follow-up data. Articles were excluded from the meta-analysis if the description of outcome data was unclear or if it was impossible to determine what percentage of patients had improved. Furthermore, if the study concerned both scalenotomy and first-rib resection, data on the separate outcomes had to be distinguishable. Table 2 presents a flowchart of the stages involved in the selection process.
Flowchart.
Statistical analysis
The pooled percentage of patients reported as having good or excellent surgical outcomes was estimated using a random effects model with double arcsine transformation. 23 The level of heterogeneity was examined by means of I2 statistics. If substantial heterogeneity (I2 > 50%) was observable, meta-regression served to test the moderating effect of sex, age, and disease duration. The risk of publication bias was also examined using funnel plots and Egger’s test for asymmetry. The meta-analysis utilized MetaXL version 5.3 (EpiGear International Pty Ltd, Sunrise Beach, Queensland, Australia), and the meta-regression, the SAS System for Windows version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Systematic analysis
Outcome measures
The database search yielded an initial 1 354 articles, of which 18 met the eligibility criteria. The full study characteristics detailed in Supplemental Table S1 include the number of patients, follow-up time and method, patient gender, outcome measures, quantitative outcome scores, patients’ subjective opinions, complications, and results.
The number of patients per study ranged from 11 to 179, with approximately 80% female. The mean study sample size was 58. Mean patient age at (the time of) surgery was 35.8 years. All studies reported long-term outcomes, with the mean follow-up time 49 months (range = 3–180 months). No study including scalenotomy was randomized. Several different surgical outcomes were indicated, with most of the studies reporting pain and numbness. Almost all studies reported patients’ self-assessed outcomes, later allowing us to perform a meta-analysis. The studies originated from the United States (9), Finland (4), Greece (1), the United Kingdom (1), Italy (1), Ireland (1), and Lithuania (1).
Ten of the studies featured questionnaires, three involved clinical research and four included both clinical and questionnaire methods. One study lacked clarity as to whether its estimation of results was clinical or by questionnaire. 24 We included one Likert-type II study, 24 nine Likert-type III studies,15,16,18,25–27,28–30 and four Likert-type IV studies.21,31–33
Studies using no quantitative validated outcome scores numbered 14. The other four comprised two using Visual Analogue Scale (VAS) (Ransom et al., 34 who also used The Single Assessment Numeric Evaluation (SANE), The Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH), Cervical Brachial Symptom Questionnaire (CBSQ), and Numerical Rating Scale (NRS), and Sheth and Campbell, 35 whereas Ruopsa et al. 36 used QuickDASH, CBSQ, and NRS, and Glynn et al. 37 used QuickDASH exclusively.
Patient subjective opinion and satisfaction were provided by 15 studies, and the life-time method which classifies results as excellent, good, fair, or poor by the other 3.15,16,18 The quality assessment results appear in Supplemental Table S2.
Nine studies reported patient TOS etiology,15,16,18,21,27–29,34,35 most of them highlighting trauma as a significant cause of TOS. Sanders et al. 16 reported that a history of trauma, mostly neck trauma, immediately preceded the onset of symptoms in 92% of 239 scalenectomy cases; those figures for Sanders and Pearce 15 were a similar 91% of 279 scalenectomies. Of note, the patients in these two articles were in part the same. Also reported to raise the risk for TOS was overuse. 34 Finally, Sanders and Pearce 15 found that of NTOS patients, 4.5% had a cervical rib.
The mean duration of symptoms was included in four studies and ranged from 2 months to 23 years. Nocturnal symptoms were estimated in only two articles.31,36 Jasinskas et al. 31 reported that postoperatively, headache disappeared in 43% of the patients and decreased in 31%, whereas dizziness disappeared in 56%. For their part, Ruopsa et al. 36 found that 57% of patients reported headache at least once per week before their scalenectomy, and at follow-up, this number fell to 30%. We found no studies reporting on the use of pre- and post-operative painkillers.
Surgical findings
Six studies reported surgical findings. Of these, Baltopoulos et al. 33 reported hypertrophy of the scalenus anticus muscle and one fibrous extension of the first rib. As for pathological findings, Cheng et al. 29 encountered the following complications during TOS surgeries: anterior and middle scalene anomalies, scalenus minimus, fibrous bands, scarring, long C7 transverse process, and abnormal first rib. Among 88 surgeries, Ruopsa et al. 36 found 12 normal, 20 large, and 38 tendinous scalenus anticus muscles, as well as 18 muscles with tight posterior fascia. Those researchers also stated that the space between the first rib and the clavicle was wide in 58 patients, somewhat narrowed in 17, and narrow in 3 cases. Estimated plexus compression was obvious in 71 cases and probable in 8.
Ciampi et al. 30 found that 15 patients (30%) were affected by anterior scalene muscle anomalies, 11 of which had hypertrophic muscles, and 4 a falciform insertion; one patient (2%) was affected by an anomalous band (type 3 according to Roos’s (1976 classification)), and 4 (8%) were affected by perineural fibrosis; these 4 patients also had a history of cervical trauma. Dellon 27 found scarring of the brachial plexus proximally and superficially to the deep cervical fascia and the fibrous edges of the scalenus anticus; scarring of the lower trunk and the C8 and T1 roots to the most posterior aspect of the first thoracic rib; and scarring of the T1 root to the medial aspect of the first rib, the suprapleural fascia, and the proximal juncture of the C8 and T1 roots. According to Ransom, 34 the most common surgical findings included pleural bands in 74% of the patients, tight scalene muscles in 64%, and tethered brachial plexus in 48%.
Return to work and retirement
Patients’ estimated return to work was a feature of four studies. Notably, Cheng et al. 29 found that, after scalenectomy, 63% of patients returned to work. Gockel et al. 21 found that those retired at follow-up a mean 4.1 years after surgery comprised 33% of patients; the retirement frequency in this patient population during the follow-up period also increased from 6% to 33% and was the highest among factory workers. Ruopsa et al. 36 reported that at follow-up, a mean 13 years after surgery, those still working full time were more than 50% of the women and 79% of the men. Sheth and Campbell 35 found that patients who were not working before surgery were after surgery, unlikely to return to work.
Factors affecting surgical outcome
Factors that affect surgical outcome were areas of study in five articles.18,29,32,36,37 According to Cheng, 29 the only important factor that determined clinical outcome in primary supraclavicular TOS decompression was the duration of symptoms before surgery. Some 83% of patients who had symptoms for less than 2 years had successful results compared with only 68% in those who had symptoms longer than 2 years (p < 0.05). In contrast, (the) length of symptom duration did not correspond to surgical result in Kallio and Rokkanen’s article. 32 Ruopsa et al. 36 found no significant preoperative (plexus tenderness, Roos’s Elevated Arm Test) or intraoperative factors (condition of the scalenus anterior muscle, width of the first rib-clavicle space, or estimated plexus compression) that predict surgical outcome. Earlier, Sanders et al. 16 had found that a scalene muscle block was an important factor in determining clinical outcome after supraclavicular scalenectomy: a good response to scalenectomy occurred in 80% of their patients, all of whom had good responses to a scalene muscle block. In contrast, only 32% of their patients had good improvement following surgery if they had had a negative response to the scalene muscle block. Glynn et al. 37 reported significant improvements in post- versus pre-operative DASH scoring for TOS patients without a history of trauma, and postoperative DASH scores were significantly lower than preoperative scores for those who did not smoke. Sanders 18 stated that patients with work-related TOS had poorer postoperative results.
Complications
Only two studies indicated no complications at all,33,35 but complications were evident in 10 studies.15,21,26,28–31,34,36,38 There was no operative mortality specified in any of the 18 articles.
Cheng et al. 29 noted many complications among their 43 scalenectomies, including intraoperative pleural injury (40%), pneumothorax (7%), pleural effusions/atelectasis (2%), long thoracic nerve injury (5%), Horner syndrome (5%), lymphatic injury (5%), wound infection (1%), and re-exploration (2%). Ruopsa et al. 36 reported that among 89 scalenotomies, physician-reported complications occurred in five patients (6%): transient phrenic nerve palsy, levator scapulae muscle pain for 4–5 days, dissection of a ventriculoperitoneal shunt inserted 30 years earlier, and edema around the neck which caused problems with head movement and temporary serratus palsy. There also emerged 13 self-reported complications, such as problems with subcutaneous stitches which had absorbed very slowly. Three patients had problems with breathing after surgery, but no permanent phrenic nerve or serratus palsies emerged. Sanders et al. 16 indicated that among their 239 scalenectomies, 7% of patients had temporary and 0.5% had permanent phrenic nerve palsies, and 1% experienced needle aspiration of the pneumothorax. Sanders et al. 15 also found that among 279 scalenectomies, temporary phrenic nerve palsy occurred in 6% of patients, venous injury in 0.4%, pleura opening without pneumothorax in 1.4%, and pneumothorax requiring a tap in 0.4%. Of note, the patient data of these last two articles were partly overlapping.
Of Ciampi et al.’s 30 20 patients studied in 2011, one developed neuropraxia which resolved completely after 1 month. The researchers also observed neither major complications nor wound infections. Among Jasinskas’ 77 patients reported in 2017, 31 only one postoperative complication was determined: a suppuration of the operative wound (1%), which was treated by applying conservative measures.
Woods 28 published on complications among 90 patients. In five, (6%), temporary dyspnoea developed due to trauma to the phrenic nerve at the time of surgery, and wound infection occurred in two patients (2%); local hemorrhage necessitating operative hemostasis occurred in one. Ransom et al. 34 reported, among 54, complications in three patients (4.9%), which included pneumothorax in one (1.6%) and Horner syndrome in two (3.3%). Baltopoulos et al. 33 reported two cases of transient brachial plexus injury (infection and mild overstretching, with complete resolution of the symptoms in a respective 2 and 3 weeks), but no other intraoperative or postoperative complications.
META-ANALYSIS for operation success
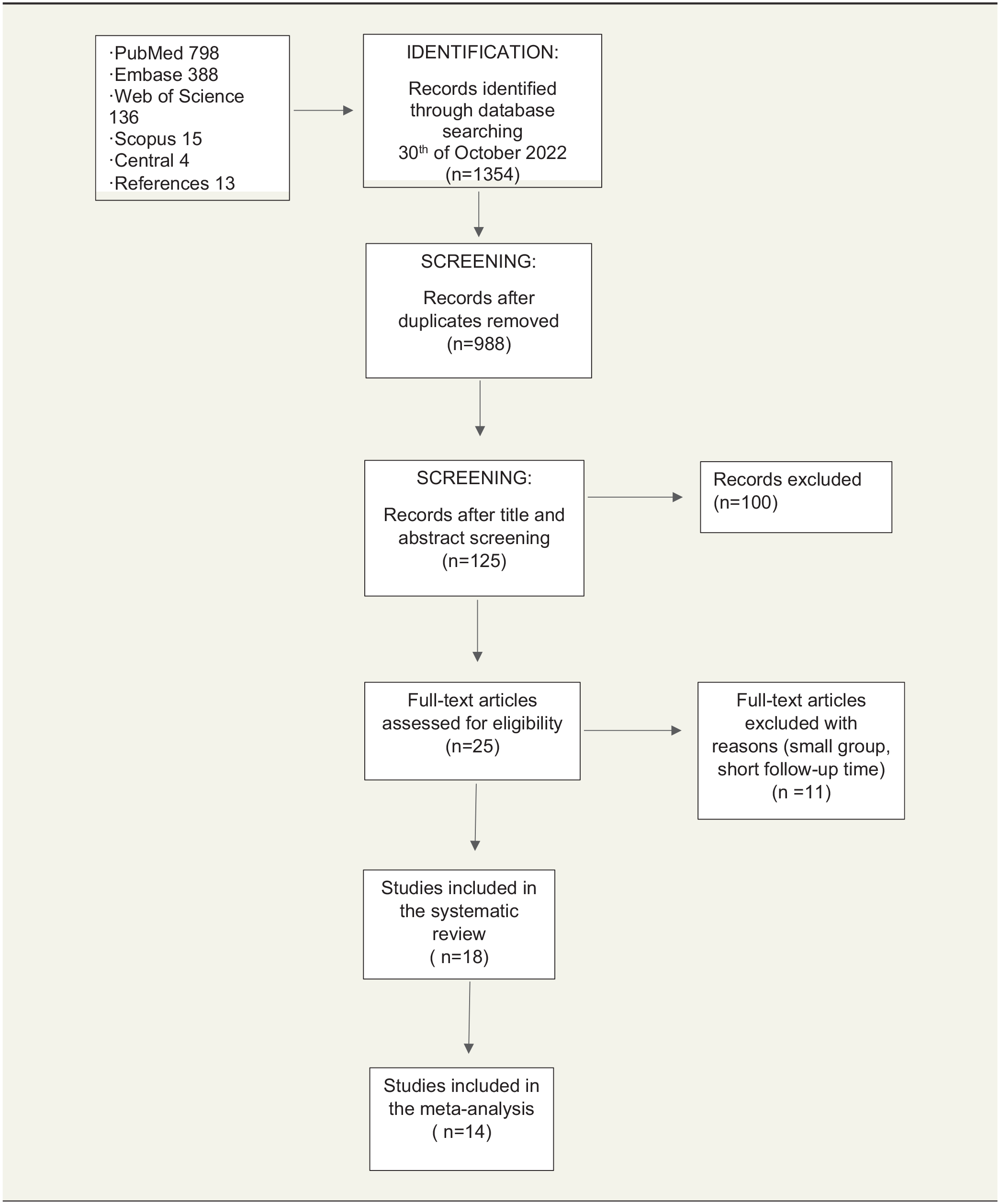
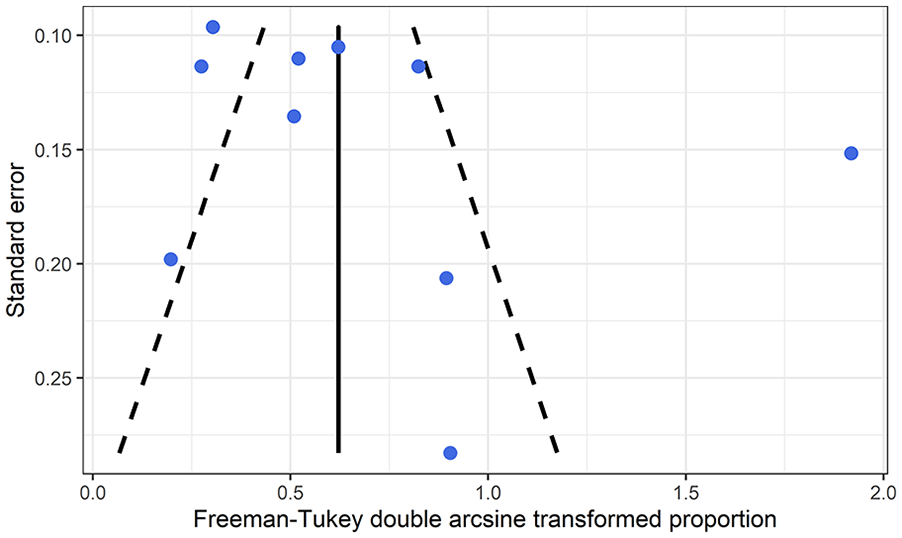
Fifteen studies gave excellent/good patient-reported outcomes, a sufficient number to allow performance of a meta-analysis. Other outcomes were only reported in a few studies.34,37 Another article only concerned young athletes’ NTOS and was excluded from the meta-analysis, because those patients represented a limited group. 33 Three articles34,37,35 did not use the same conversion variable, so they were excluded from the meta-analysis, as well (for meta-analysis data, see Figs 1 and 2). The pooled estimate for operation success was 71% (95% confidence interval (CI) = 64.4% to 76.4%, I2 = 73.0).
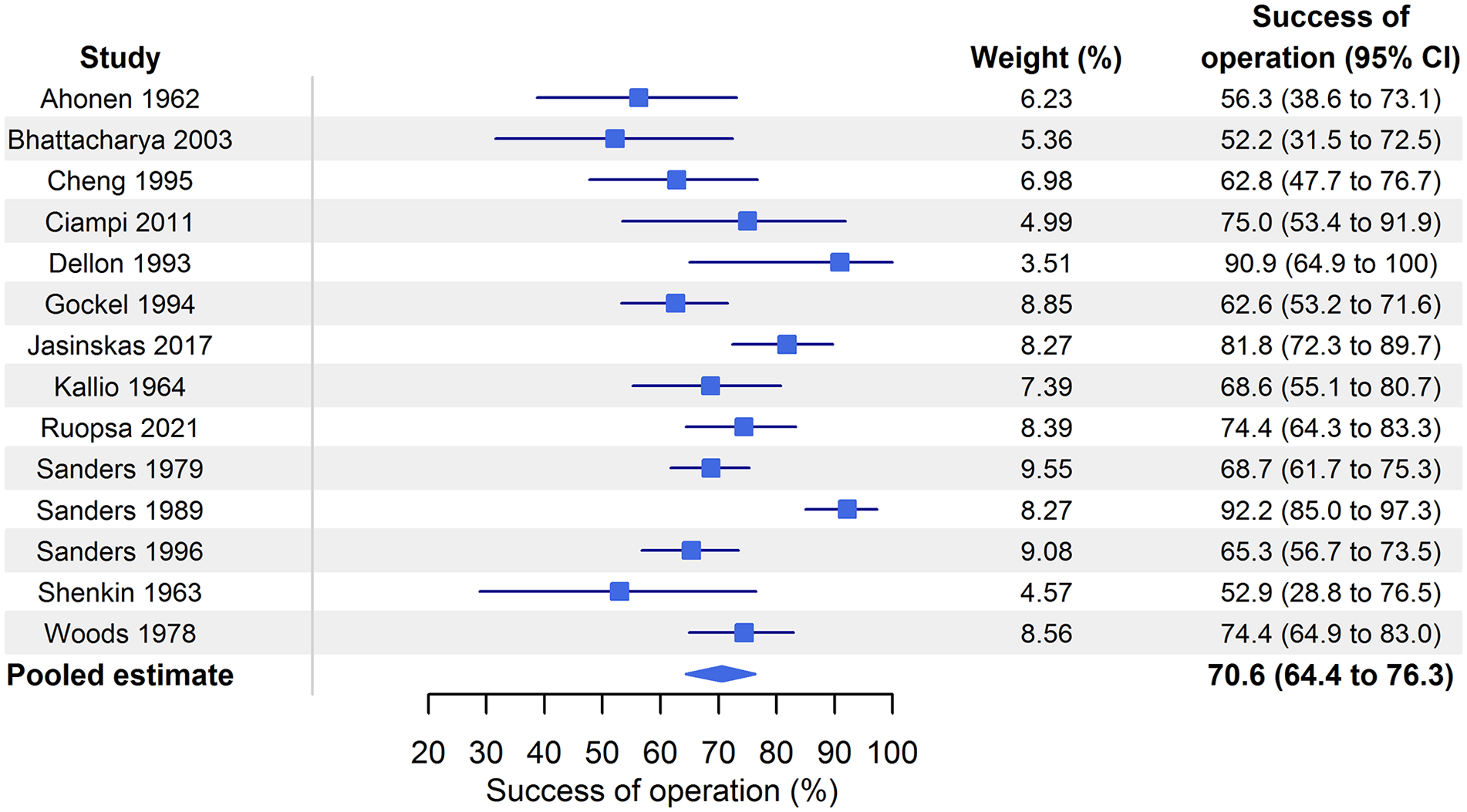
Forest plot.
Funnel plot.
Meta-regression analysis served in the examination of whether sex, age, or disease duration had a moderating effect-on-effect size (e.g. if younger patient age explains the higher percentage of surgical success). Sex (for transformed effect size β = −0.035, 95% CI = −2.145 to 2.075, p = 0.971), age (for transformed effect size β = −0.005, 95% CI = −0.052 to 0.042, p = 0.816), and disease duration (for transformed effect size β = 0.001, 95% CI = −0.005 to 0.006, p = 0.820) were not statistically significant moderators, meaning these factors did not explain the heterogeneity (Figs S1–S3). The funnel plot in Fig. 2 did not suggest any publication bias (Egger regression, p = 0.802).
In the sensitivity analysis, which excluded one study (Sanders et al.), the results remained similar, with no substantial heterogeneity detectable (pooled estimate for operation success: 68.5%; 95% CI = 63.8% to 72.9%, I2 = 46.1%).
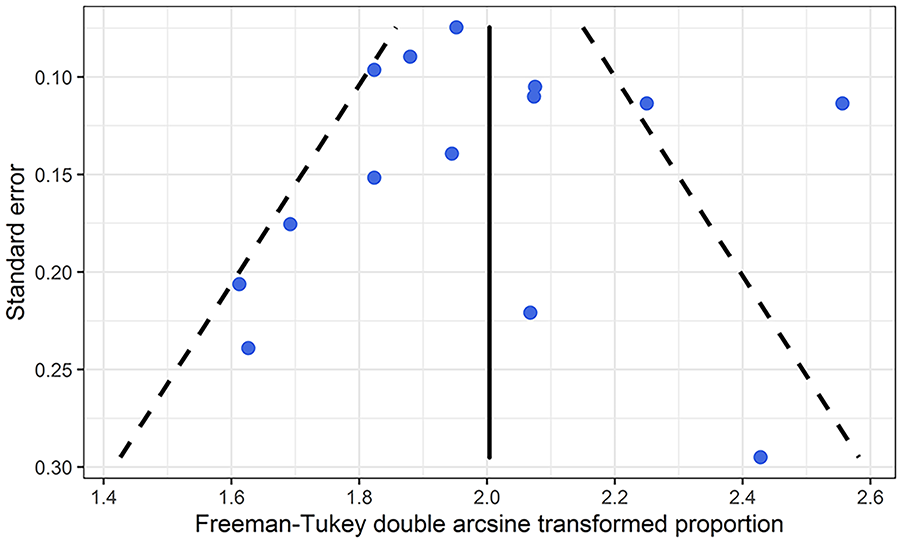
Meta-analysis for complications
Ten studies gave complication rate outcomes, a sufficient number to allow performance of a meta-analysis. The pooled estimate for complication was 10.6% (95% CI = 3.1% to 33.2%, I2 = 91.5%) (Figs 3 and 4).
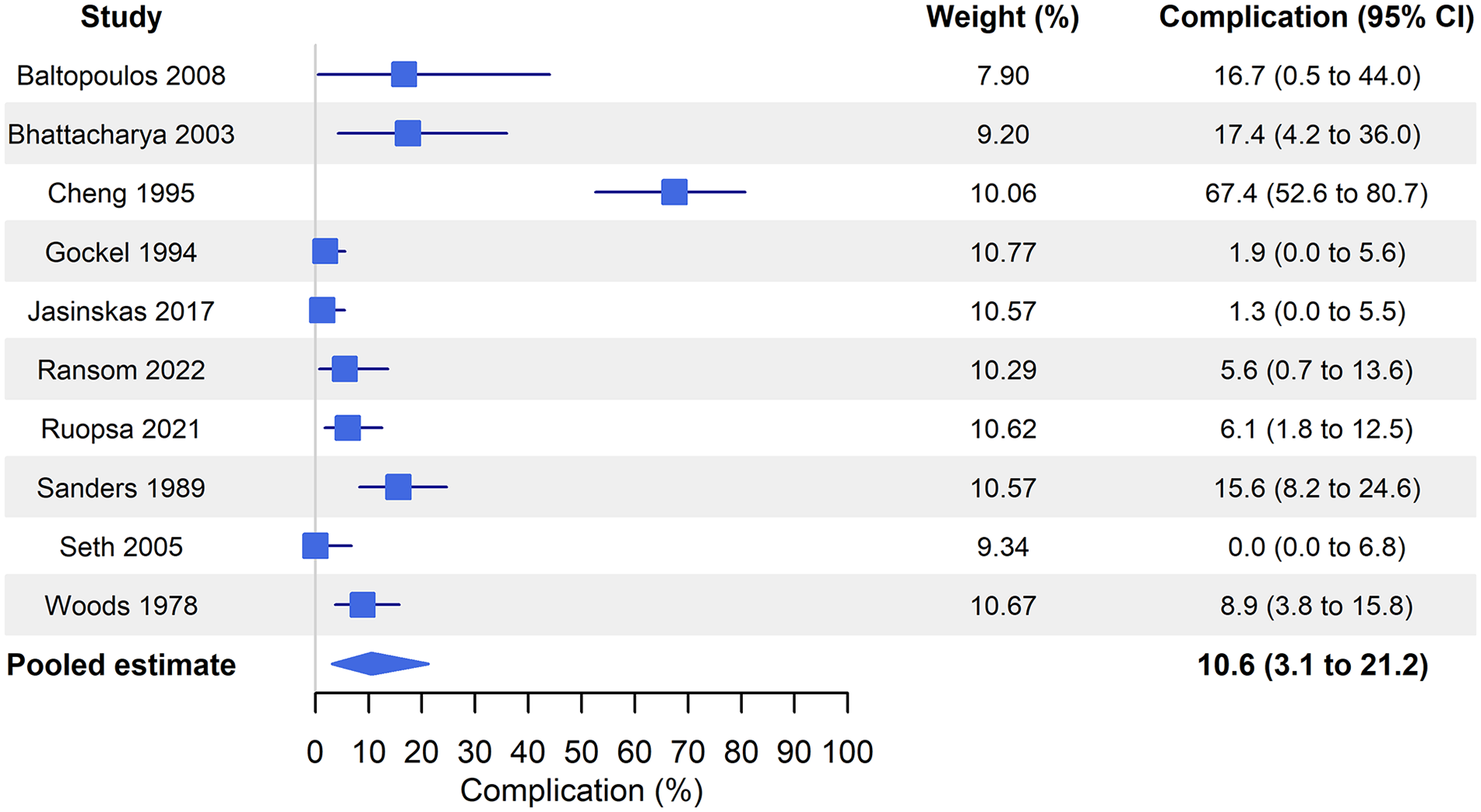
Forest plot.
Funnel plot complications.
In the sensitivity analysis, which excluded one study (Cheng et al.) with exceptional high complication rate, the pooled estimate for the complication rate was 6.7% (95% CI = 3.2% to 11.2%, I2 = 68.7%).
Risk of bias
Risk of bias was estimated using traffic light method (Supplemental Figs S4 and S5). Risk of bias due to missing outcome data raised some concerns. In six studies, there were no dropouts at all, in two studies, that was not reported, and in the others, the dropout percentage varied between 8% and 58%, with the mean of 27%. However, risk of bias concerning other domains, deviations from the intended interventions, the measurement of the outcome, and the selection of the reported result, was low.
Discussion
Our systematic literature review showed that rib-sparing surgical treatment of neurogenic TOS was safe and beneficial in most patients. Our meta-analysis further confirmed that the majority of patients achieved good or excellent results without significant side effects. The fairly low percentage of complications across these studies implies that supraclavicular rib-sparing scalenotomy/scalenectomy is a safe procedure in the treatment of neurogenic TOS.
Previous NTOS meta-analyses have studied both scalenotomies and rib resections. For instance, Peek et al., 38 analyzing the outcomes and major complications of arterial, venous, and neurogenic TOS, found that all their included articles showed improvements in complaints after surgical treatment. Lingyun et al. 39 provided a meta-analysis of NTOS outcomes after scalenotomy or rib resection based on Derkosh’s classification. Their meta-analysis showed that both supraclavicular neuroplasty of the brachial plexus (SNBP) and transaxillary first-rib resection (TFRR) are effective for NTOS treatment, although SNBP is better in improving Derkash’s classification in the long term. Yin et al. 40 reported that scalenotomy had a high probability of a success rate >70%, but only a low probability of a success rate >80%. These positive findings suggest that resection of the first rib is not necessary in the surgical treatment of NTOS.
Our review also summarized evidence of the effectiveness of scalenotomy in the treatment of NTOS. We used databases extensively. All articles that we included demonstrated, after scalenectomy, improved symptoms. Patient-reported outcome was the only outcome reported in 15 studies, although this number was sufficient to perform a meta-analysis. We found moderate heterogeneity between patient outcomes.
Our research does have several limitations. First, most of the included studies were retrospective, and there were no randomized controlled trial studies, which raises the risk of bias. Retrospective small series cases may be heavily biased. The included papers probably are from a highly selected patient population. From 988 studies, we only included and evaluated 18 studies in the review. This number of relevant studies is low, and of them, only three featured more than 100 patients. Some of the studies provided no clarification of how the patients had been examined or even of how the results were estimated. Quantitative validated outcome scores were only used in four studies, apparently because no validated scores existed at that time, and some of the studies were of moderate-to-poor methodological quality as well. Therefore, the overall quality of the available evidence may be low, with a high risk of bias. Moreover, the results focused on patient reports of improved symptoms; only a few studies included objective data, and the various data chosen for use were not comparable. On the contrary, the articles included in the meta-analysis described the end result of the surgery in the same way, so a meta-analysis was possible. Thus, because no other variables were available to study, we could only investigate the subjective success of each surgery. A comparison utilizing more objective evaluation criteria such as TOSI and QuickDASH would make the outcome data more convincing.
In conclusion, this systematic literature review and meta-analysis show that rib-sparing scalenotomy is effective in the treatment of NTOS. However, additional high-quality and multicentered research will be crucial to confirm these findings. To yield more comparable studies, we also recommend the use of a validated universal TOS-related outcome tool, one such as TOSI, for both pre- and post-operative evaluation of TOS surgery.
Supplemental Material
sj-tif-1-sjs-10.1177_14574969251332910 – Supplemental material for Rib-sparing scalenotomy in thoracic outlet syndrome treatment: A systematic review and meta-analysis
Supplemental material, sj-tif-1-sjs-10.1177_14574969251332910 for Rib-sparing scalenotomy in thoracic outlet syndrome treatment: A systematic review and meta-analysis by Niina Ruopsa, Heidi Vastamäki, Tero Vahlberg, Martti Vastamäki and Leena Ristolainen in Scandinavian Journal of Surgery
Supplemental Material
sj-tif-2-sjs-10.1177_14574969251332910 – Supplemental material for Rib-sparing scalenotomy in thoracic outlet syndrome treatment: A systematic review and meta-analysis
Supplemental material, sj-tif-2-sjs-10.1177_14574969251332910 for Rib-sparing scalenotomy in thoracic outlet syndrome treatment: A systematic review and meta-analysis by Niina Ruopsa, Heidi Vastamäki, Tero Vahlberg, Martti Vastamäki and Leena Ristolainen in Scandinavian Journal of Surgery
Supplemental Material
sj-tif-3-sjs-10.1177_14574969251332910 – Supplemental material for Rib-sparing scalenotomy in thoracic outlet syndrome treatment: A systematic review and meta-analysis
Supplemental material, sj-tif-3-sjs-10.1177_14574969251332910 for Rib-sparing scalenotomy in thoracic outlet syndrome treatment: A systematic review and meta-analysis by Niina Ruopsa, Heidi Vastamäki, Tero Vahlberg, Martti Vastamäki and Leena Ristolainen in Scandinavian Journal of Surgery
Supplemental Material
sj-xlsx-4-sjs-10.1177_14574969251332910 – Supplemental material for Rib-sparing scalenotomy in thoracic outlet syndrome treatment: A systematic review and meta-analysis
Supplemental material, sj-xlsx-4-sjs-10.1177_14574969251332910 for Rib-sparing scalenotomy in thoracic outlet syndrome treatment: A systematic review and meta-analysis by Niina Ruopsa, Heidi Vastamäki, Tero Vahlberg, Martti Vastamäki and Leena Ristolainen in Scandinavian Journal of Surgery
Supplemental Material
sj-xlsx-5-sjs-10.1177_14574969251332910 – Supplemental material for Rib-sparing scalenotomy in thoracic outlet syndrome treatment: A systematic review and meta-analysis
Supplemental material, sj-xlsx-5-sjs-10.1177_14574969251332910 for Rib-sparing scalenotomy in thoracic outlet syndrome treatment: A systematic review and meta-analysis by Niina Ruopsa, Heidi Vastamäki, Tero Vahlberg, Martti Vastamäki and Leena Ristolainen in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors thank Carol Norris, PhD, for language revision, and Mikhail Saltychev, MD, PhD, for help in planning the study, and Leeni Lehtiö, Information Specialist, for help with the data search.
Author contributions
NR: Study design; patient examination; draft writing.
LR: Statistics; study design; draft checking.
MV: Study design; draft writing.
HV: Study design; draft writing.
TV: Statistics; draft checking.
Authors’ note
All ICMJE Ethical Committee of the University hospital district approved the study (no. 1118/2019). Each author certifies that his or her institution approved the human protocol for this investigation that all investigations were concluded in conformity with ethical principles of research, and that informed consent for participation in the study came from each participant. This work was performed at the Research Institute Orton, Helsinki, Finland.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The institution of the authors has received, during the study period, funding from Orton EVO grants from the Ministry of Social Affairs and Health, Finland.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.