
Abstract
Background and aims:
The present study aimed to compare patients who underwent deep inferior epigastric perforator (DIEP) flap reconstruction with and without the implementation of the new optimized surgical recovery pathway. The new protocol aims to standardize and optimize perioperative management, shorten hospital stays, and lower complication rates for patients undergoing major surgical procedures.
Methods:
Consecutive patients who underwent immediate or delayed DIEP flap breast reconstruction were included in this study. Data regarding patient demographics, timing, laterality of reconstruction, hospital length of stay (LOS), and drain management were collected and compared for the pre-protocol group and the post-protocol group.
Results:
The pre-protocol group consisted of 65 patients, while the post-protocol group consisted of 68 patients. The two groups had similar total complication rates (pre-protocol 43.1% versus post-protocol 32.4%, p = 0.20). Between the two groups, there was a significantly lower rate of major surgical complications in the post-protocol group (pre-protocol 32.3% versus post-protocol 14.7%, p = 0.016). There were no significant differences between the groups regarding minor surgical complications (pre-protocol 7.7% versus post-protocol 17.6%, p = 0.086). In the pre-protocol group, the mean LOS was 6.1 days (range = 4–10, median = 6); in the post-protocol group, the mean LOS was 3.6 days (range = 3–10, median = 3; p < 0.00001). Majority of the post-protocol patients were discharged on postoperative day 3 (n = 47, 69.1%).
Conclusion:
Patients undergoing DIEP flap reconstruction can be discharged earlier without risking their safety by following the new protocol.
Keywords
Context and relevance
Breast reconstruction is an important chapter for many women recovering from breast cancer. In this study, we present a detailed examination of the implementation of the new optimized surgical pathway protocol in patients who underwent deep inferior epigastric perforator (DIEP) flap reconstruction, comparing outcomes with and without the new protocol. The new protocol aims to standardize and optimize perioperative management, shorten hospital stays, and lower complication rates for patients undergoing major surgical procedures. The length of stay and systemic complications reduced. No total flap losses. Understanding the potential benefits of the new optimized DIEP recovery pathway in this context could provide valuable insights into optimizing perioperative care and improving outcomes for patients undergoing DIEP flap breast reconstruction.
Introduction
Breast cancer is the most common type of cancer among women. Nowadays, women are more aware of the options for breast reconstruction, including autologous procedures, which are readily available alternatives to implants in many centers.1–4
The deep inferior epigastric perforator (DIEP) flap has become the golden standard among plastic surgeons due to its low donor site morbidity and natural aesthetic outcome. 5 DIEP flap reconstruction requires microsurgical facilities and skills as well as ample preoperative education and close and rather lengthy postoperative inpatient monitoring during the hospital stay. Nevertheless, major microsurgical complications are rare.6,7
A new protocol called “optimized DIEP recovery pathway” was introduced in the hospital unit with the aim of enhancing the previous patient care pathway (from here on referred to as the new protocol). This protocol focuses on standardizing and optimizing perioperative management for patients undergoing major surgical procedures. Keystone maneuvers support minimal preoperative fasting and early feeding, anesthesia methods that prevent postoperative nausea and vomiting, and better patient education before the surgery. These maneuvers also encourage early mobilization after surgery. The new protocol aims to achieve results consistent with those observed in similar practices worldwide. Specifically, it strives to reduce the hospital length of stay (LOS), lower the postoperative complication rate, and minimize opioid consumption.8,9
Various protocols and improvements have been developed over the years to optimize patient care and the surgical pathway across different surgical specialties. The Enhanced Recovery After Surgery (ERAS) protocol has demonstrated positive results in numerous procedures, including plastic surgery, colorectal, major abdominal, and orthopedic operations.10–14 In addition, other interventions have emerged to enhance patient care during DIEP flap surgery by reducing operating time and improving outcomes, such as complication rates and LOS. Examples of these interventions include the establishment of a 100-step surgical pathway and the development of team models designed to maximize results and minimize complications.15,16
The present study evaluated the impact of the new protocol on patients undergoing DIEP flap reconstruction. Specifically, this study compared key metrics, including LOS, complication rates, and readmission rates, of patients who underwent surgery prior to the adoption of the new protocol in Helsinki University Hospital and those treated after its implementation. Understanding the potential benefits of the new protocol in this context could provide valuable insights into optimizing perioperative care and improving outcomes for patients undergoing DIEP flap breast reconstruction.
Methods
In this retrospective observational analysis, the study population consisted of patients who underwent immediate or delayed microvascular breast reconstruction at the Division of Plastic Surgery of Jorvi Hospital. Jorvi Hospital is a subsidiary unit within the Helsinki University Hospital’s Plastic Surgery Department, located in Finland.
Patients were not selected for this study; instead, all individuals who underwent DIEP flap reconstruction during the study period were included in the analysis. The pre-protocol group consisted of patients operated on without the new protocol in 2018 and 2019. The post-protocol group consisted of patients who underwent operations under the new protocol between 2021 and 2022. Patients who had operations in 2020 were not included in this study due to the COVID-19 pandemic, which caused many changes in the patient care pathway that prevented adequate comparison between study groups.
Experienced plastic surgeons performed the DIEP flap reconstructions during the study period. In addition, plastic surgery residents received regular microsurgery training in this unit and were included in the operating team under the senior plastic surgeon’s supervision.
Care pathway
The hospital began implementing the new protocol in 2020 to optimize the care of patients undergoing DIEP reconstruction. The new care pathway is shown in Fig. 1.
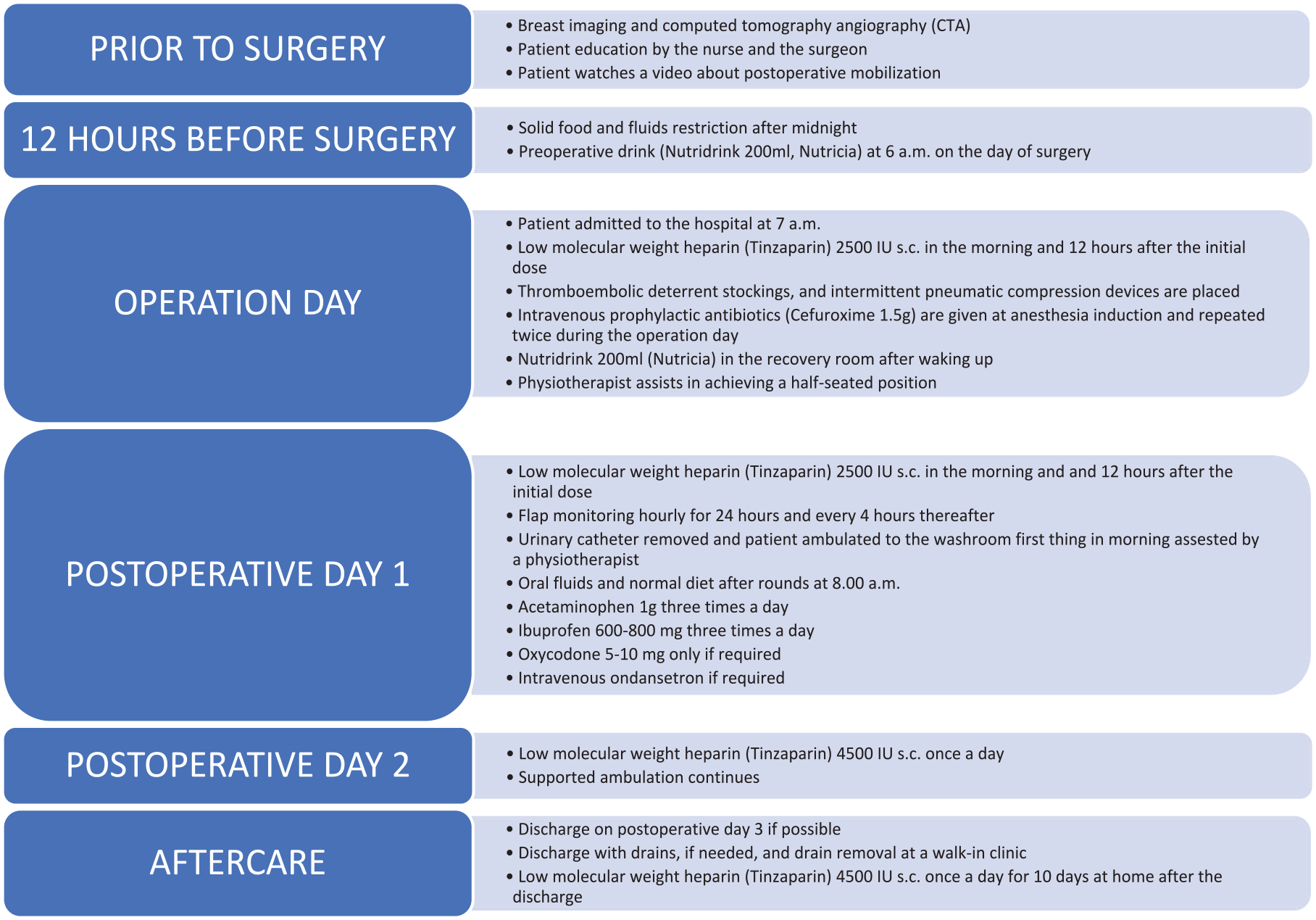
Care pathway.
An important step of the new protocol was patient education prior to surgery. Both surgeon and reconstruction nurse informed patients about the new protocol and particularly that it is safe to ambulate on the first postoperative day (POD) and be discharged on the third day after surgery, even with drains on when needed. In addition, patients received a video link from the physiotherapist, illustrating how to get out of bed protecting the donor site. Patients were encouraged to practice this prior to surgery. Patients were able to contact the hospital unit directly by phone if any questions or issues arose. A plastic surgeon was available around the clock to respond to inquiries and assess the situation should any problems occur.
All breast reconstruction patients arrived at the hospital on the morning of the surgery and received subcutaneous low molecular weight heparin (tinzaparin 2500 IU) at 7 am. The same dose was repeated 12 h after the initial dose. In addition, the patients received tinzaparin 2500 IU twice on POD 1 and thereafter 4500 IU tinzaparin once a day during the hospital stay and after discharging for 10 days at home.
Intravenous (IV) prophylactic antibiotics (cefuroxime 1.5 g IV) were administered at anesthesia induction and repeated twice unless contraindicated, in which case an alternative antibiotic suitable for the patient was selected. The first prophylactic dose was given during the morning of the surgery, second dose 3 h later, and a third dose on the evening of the surgery.
Patients were allowed a preoperative drink (Nutridrink 200 ml, Nutricia) at home on the morning of the surgery as well as after waking up in the recovery room as part of the new protocol. Oral fluids were distributed after rounds at approximately 8 a.m. on POD 1, with rapid progression to a normal diet, as tolerated.
Patients received multimodal analgesia, including regular acetaminophen (1 g three times a day), throughout the postoperative period. Ibuprofen of 600–800 mg was administered three times on POD 1 based on the new protocol. Since minimizing opioid use is a part of the new protocol, 5–10 mg of oxycodone were administered only on demand. Other analgesics such as pregabalin, gabapentin, or hydromorphone were not routinely used in our unit.
In addition, the unit started the use of topical tranexamic acid for contralateral breast and abdominal donor wound surfaces at the same time as the implementation of the new protocol to reduce postoperative bleeding. Although this was not an official element of the new protocol, its initiation happened to align with the implementation period of the new protocol.
During the surgery, drains were placed in the abdominal donor site and in the reconstruction breast. In cases where a symmetrizing procedure was performed, drains were typically not applied in the contralateral breast.
On POD 1, patients engaged in supported ambulation in the inpatient unit, progressing to independent ambulation of increasing duration throughout their hospital stay. As part of the new protocol, patients typically had the urinary catheter removed and ambulated to the washroom on the postoperative morning after rounds. Most patients had their both drains removed during the hospital stay on POD 3 or 4, while others were discharged with their drains and had them removed by a nurse at a primary care facility within a few days. Ideally, the drains were removed during the hospital stay; however, the decision was made individually based on the drain output.
Data sources and collection
The research group collected data about the patients’ comorbidities, complications, and LOS from electronic patient record systems (Uranus from CGI and Apotti from Epic). The patients’ characteristics (age, body mass index (BMI), smoking status, comorbidities that required ongoing medication), surgical details (delayed or immediate operation and laterality of the reconstruction), prior adjuvant treatment, and drain management (whether the drains were removed during the hospital stay or after the day of discharge) were recorded. LOS was measured as PODs with the operation day designated as POD 0.
All complication data were collected by the first author and classified according to the Clavien–Dindo classification. 17 In addition, the Clavien–Dindo classification was independently verified by two plastic surgeons. In addition, any contralateral procedures (e.g. mastopexy and reduction mammaplasty) performed during the same operation were documented. Each patient’s Charlson comorbidity index score was calculated based on the diagnosis indicated in the patient’s electronic medical record using an online calculator (https://www.mdcalc.com/charlson-comorbidity-index-cci).
Statistical analyses
Categorical variables were expressed as frequencies and proportions and compared using the chi-square test or Fisher’s exact test, as appropriate. Continuous variables were expressed as mean and standard deviation or median and interquartile range (IQR) and compared using the two-tailed t-test or the Mann–Whitney U test, as appropriate. Ordinal variables were expressed as median and IQR and compared using the two-tailed Mann–Whitney U test. Kaplan–Meier analysis and the log-rank test were used for the estimation and comparison of reoperations. Statistical tests were performed using NCSS 2023 Statistical Software (NCSS, LLC, Kaysville, UT, USA, ncss.com/software/ncss).
Results
Patient demographics
The pre-protocol group (2018 and 2019) consisted of 65 patients, and the post-protocol group (2021 and 2022) consisted of 68 patients. There was one (1.5%) bilateral operation in the pre-protocol group and two (2.9%) in the post-protocol group. As such, there was a total of 136 flaps. All the bilateral operations in the study were delayed reconstructions. The groups were comparable in terms of laterality and timing of reconstruction (immediate/delayed) and symmetrizing surgery (Table 1).
Patient characteristics.
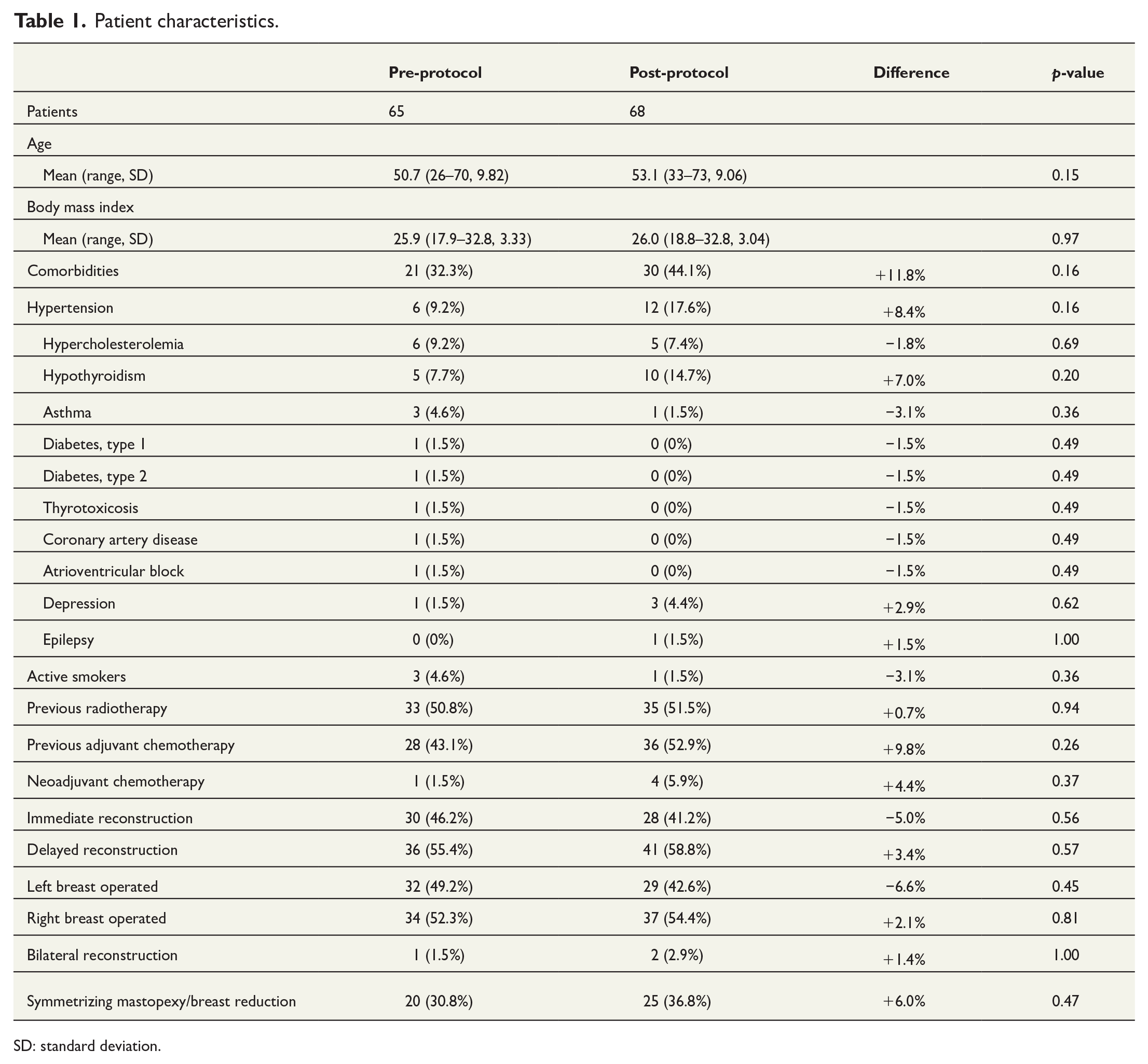
SD: standard deviation.
Comorbidities
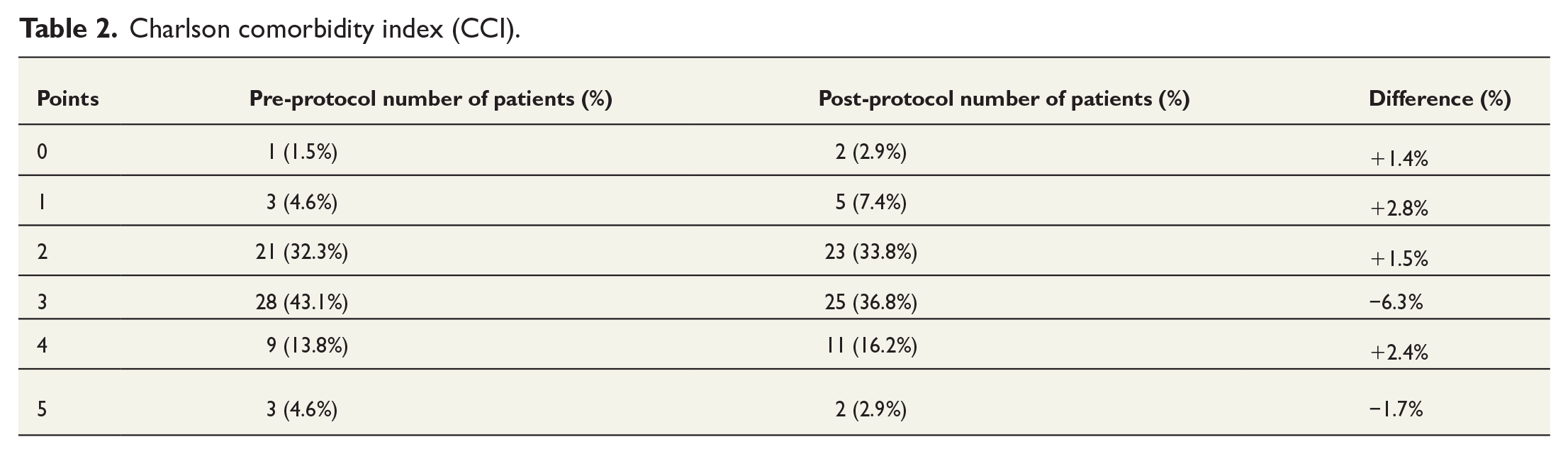
There were no significant differences in mean age, BMI, comorbidities, or adjuvant treatment between the groups. The patients’ demographics and Charlson comorbidity index scores are presented in Tables 1 and 2.
Charlson comorbidity index (CCI).
Complications
The complications are presented in Tables 3 and 4. Table 3 presents the total number of complications in the two patient groups, while Table 4 categorizes the complications according to the Clavien–Dindo classification, detailing their site of occurrence.
Complications.
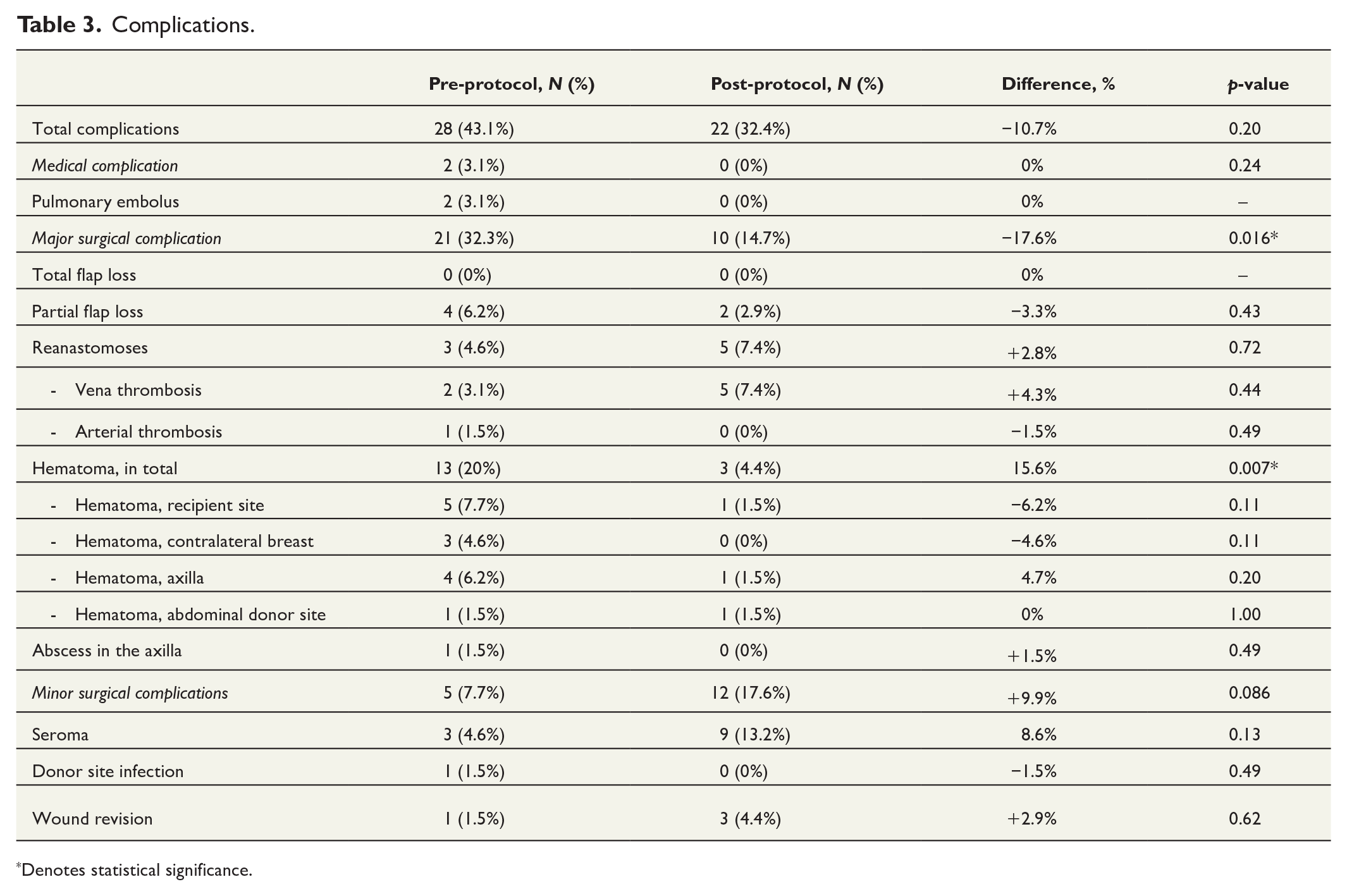
Denotes statistical significance.
Clavien–Dindo classification of the complications between pre-protocol and post-protocol groups.
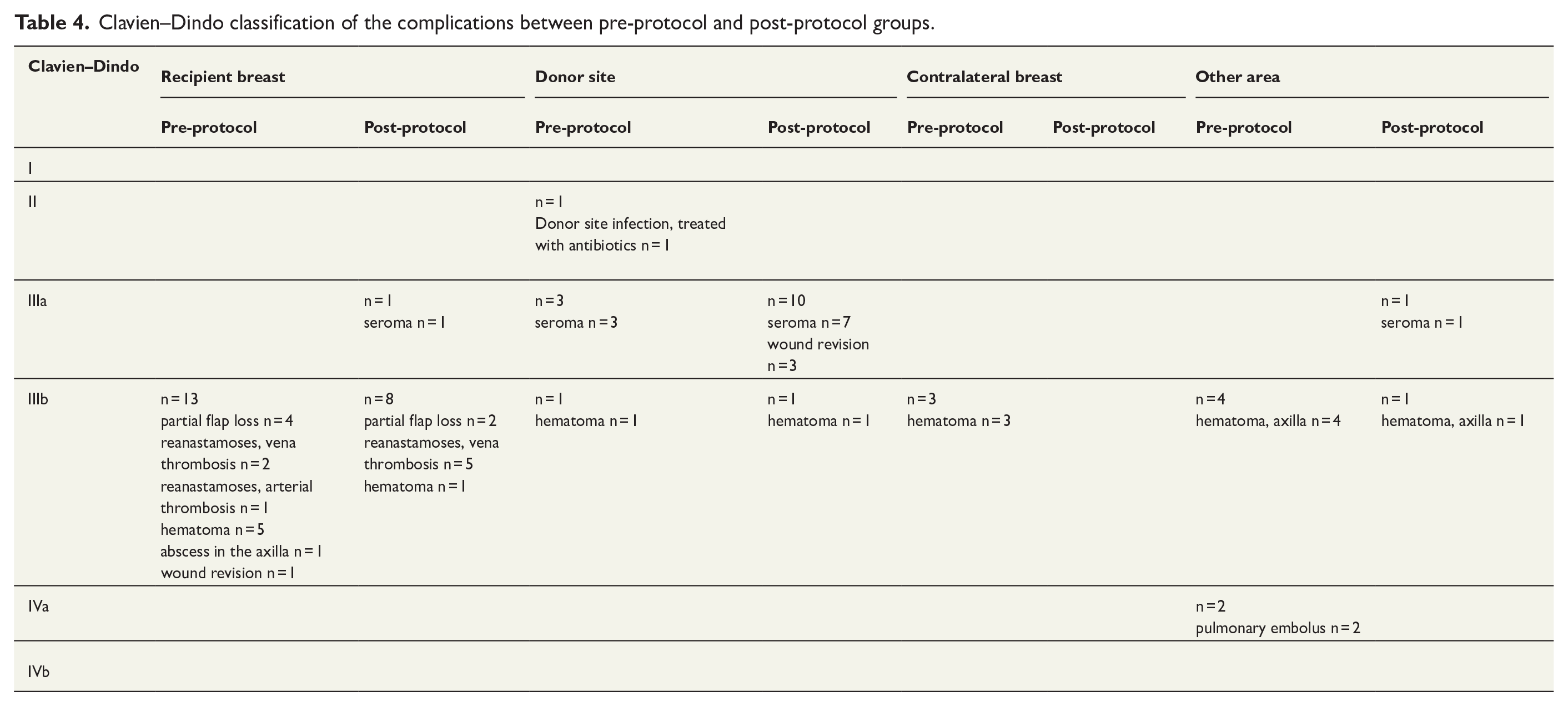
Total complications were similar between both groups (pre-protocol 43.1% versus post-protocol 32.4%, p = 0.20). Importantly, medical complications were minimal in both groups (pre-protocol 3.1% versus post-protocol 0%, p > 0.24). Both medical complications in the pre-protocol groups were pulmonary embolisms. Compared to the pre-protocol group, there was a significantly lower rate of major surgical complications in the post-protocol group (pre-protocol 32.3% versus post-protocol 14.7%, p = 0.016). There were no significant differences between the groups in terms of minor surgical complications (pre-protocol 7.7% versus post-protocol 17.6%, p = 0.086).
No total flap loss was observed in either group. Furthermore, there were no differences in the partial flap loss rates between the groups (pre-protocol 6.2% versus post-protocol 2.9%, p = 0.43). Partial flap loss was defined to occur when less than 20% of the flap’s skin island and underlying fat turned necrotic and had to be removed. There was a significantly higher rate of hematomas in the pre-protocol group than in the post-protocol group (pre-protocol 20% versus post-protocol 4.4%, p = 0.007).
Reoperations
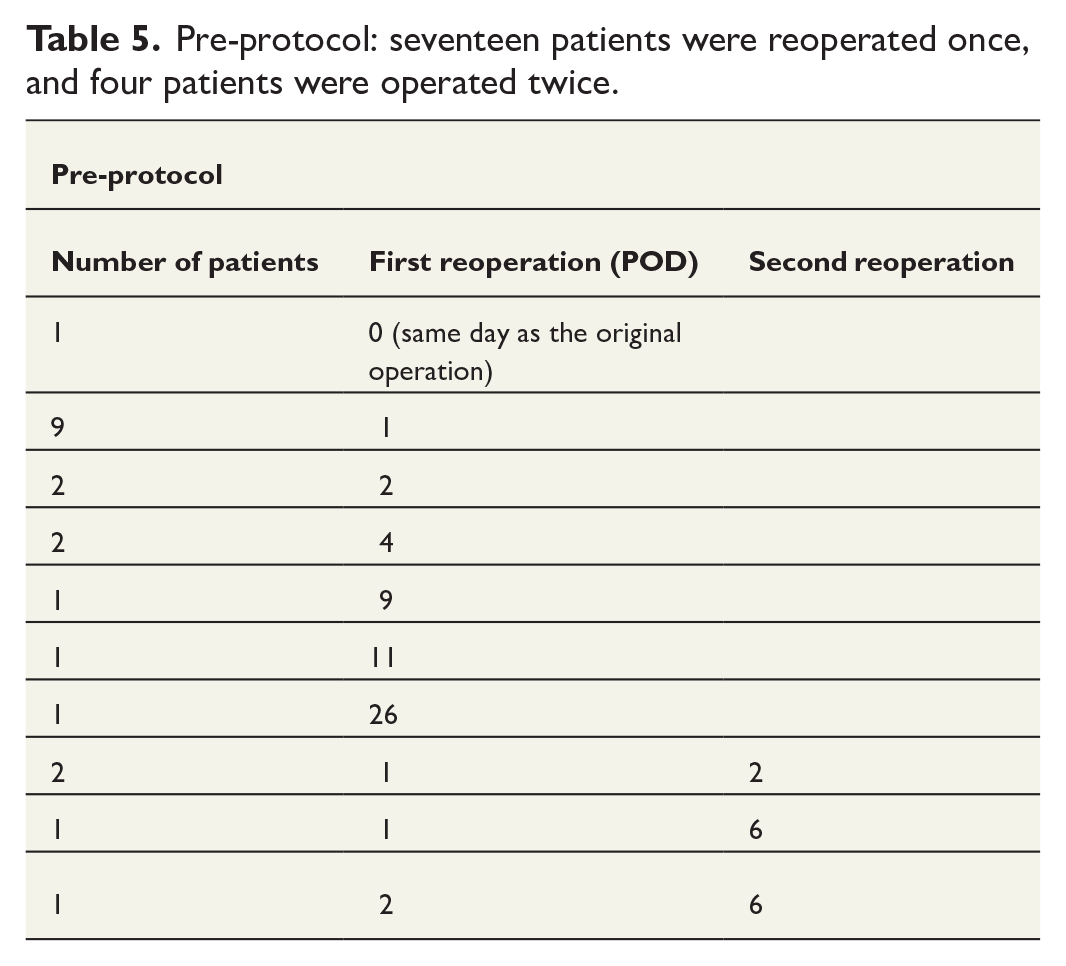
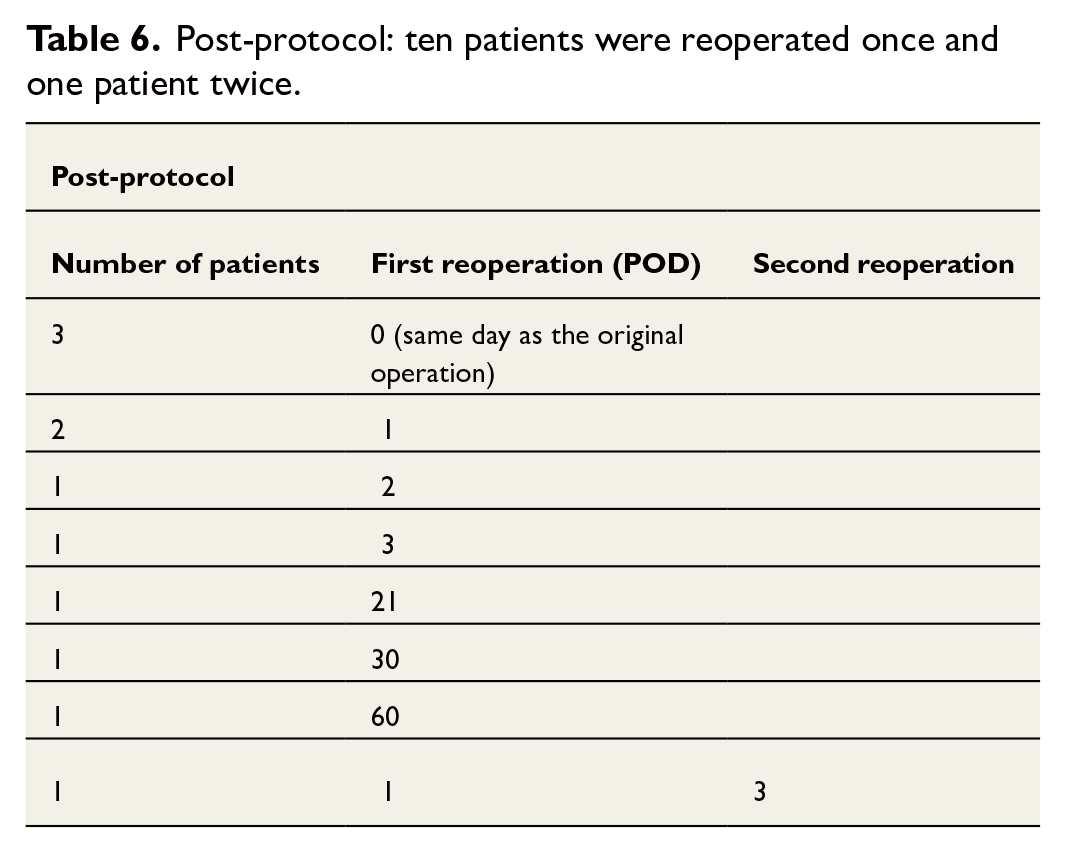
Reoperations and the timing of the first and/or second reoperations are presented in Tables 5 and 6. Reoperation time was defined as the number of PODs compared to the initial DIEP operation.
Pre-protocol: seventeen patients were reoperated once, and four patients were operated twice.
Post-protocol: ten patients were reoperated once and one patient twice.
Hospital LOS
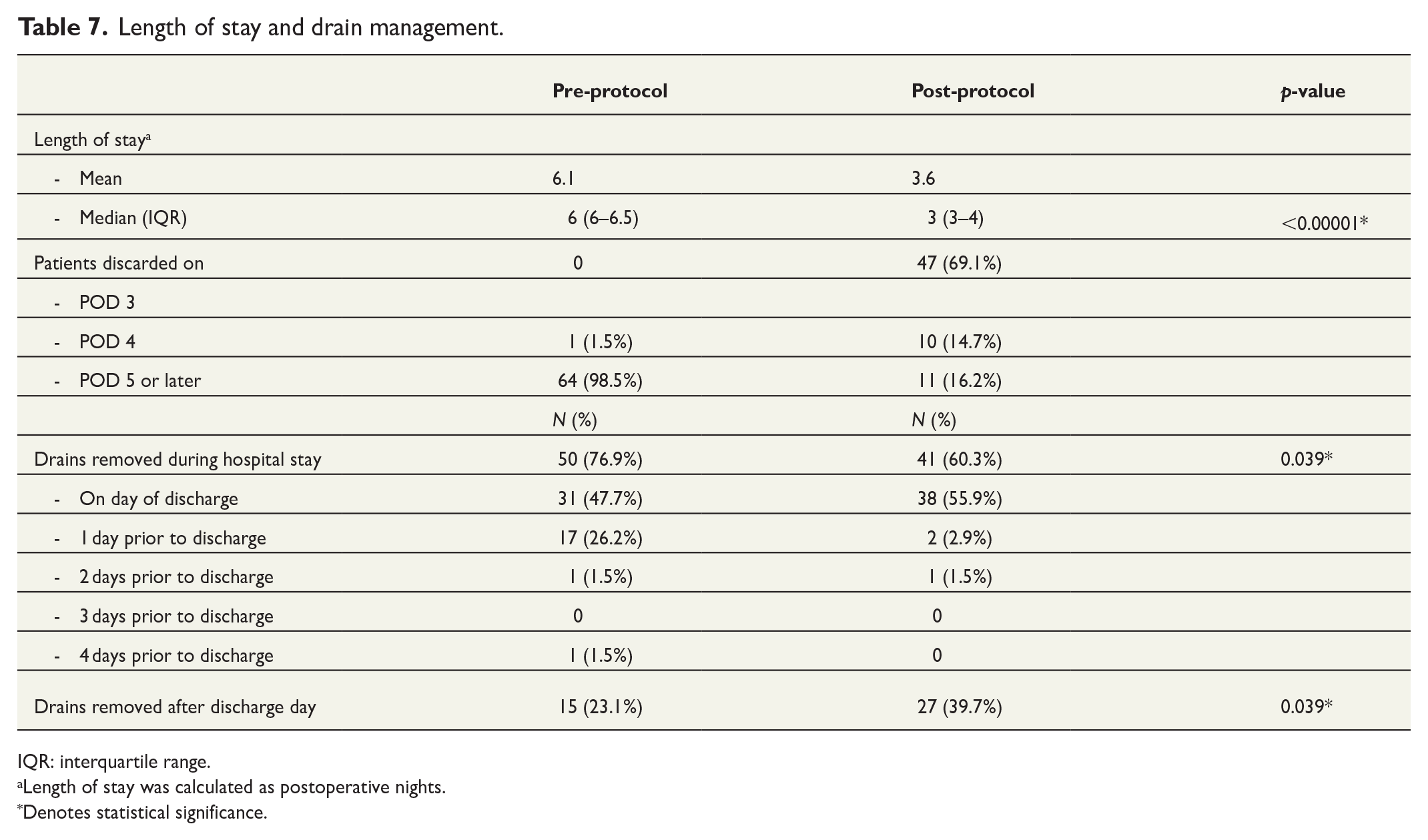
In the pre-protocol group, the mean LOS was 6.1 days (range = 4–10 days, median = 6), while in the post-protocol group, the mean LOS was 3.6 days (range = 3–10 days, median = 3; p < 0.00001). Majority of the post-protocol patients were discharged on POD 3 (n = 47, 69.1%) and the others on POD 4 (n = 10, 14.7%) or POD 5 or later (n = 11, 16.2%). In the pre-protocol group, no patients were discharged on POD 3 (n = 0, 0%). On POD 4, one patient (n = 1, 1.5%) was discharged and the rest of the patients on POD 5 or later (n = 64, 98.5%). The length of stay is detailed in Table 7.
Length of stay and drain management.
IQR: interquartile range.
Length of stay was calculated as postoperative nights.
Denotes statistical significance.
Drain management
There was a significant difference in drain management between the groups. Details on drain management are presented in Table 7. The pre-protocol group had a higher rate of drain removal during the hospital stay than the post-protocol group (pre-protocol 76.9% versus post-protocol 60.3%, p = 0.039) because LOS was higher for the patients in the former group. The post-protocol group had a higher rate of drain removal after discharge than the pre-protocol group (pre-protocol 23.1% versus post-protocol 39.7% p = 0.039) due to the earlier discharge overall.
Discussion
The purpose of this study was to analyze whether the implementation of the new protocol in a middle-sized plastic surgery unit had an impact on complications and LOS. The findings showed that LOS decreased significantly in the post-protocol group, and most patients in this group were discharged on POD 3. Similarly, other studies have demonstrated a reduction in LOS by 1–3 days following the implementation of an improved surgical recovery pathway.18–23 Bonde et al. 24 showed that 80% of patients can be discharged on POD 3, which is in line with our results. Despite the decrease in LOS following the implementation of the new protocol, there was no increase in the overall complication rate between the two groups. This finding is in line with other studies.14,18,19,21,22,25–30
Our findings suggest that the keystones for earlier discharge are more accurate preoperative patient education and early mobilization. Nowadays, patients are discharged from hospitals more quickly than before, challenging the previous notion in Finland that prolonged hospitalization and monitoring are needed after complex surgeries. Our study complements and extends the findings of previous studies, which concluded that patients can be sent home on POD 3 without risking their safety. Due to the positive results in both LOS and overall complication rates after the implementation of the new protocol in this study, this practice is now an integral part of the standard care in the Jorvi subunit.
In a meta-analysis, Tan et al. 23 found that several studies reported higher flap loss rates after the implementation of the ERAS protocol. In contrast, no increases in total or partial flap loss were found in this study despite of the integration of the new protocol in our unit. However, the definition of partial flap loss and the line between partial and total flap loss may vary in different centers, which, as Tan et al. noted, 23 could make it difficult to compare the results of different studies.
Hematomas occurred more often in our study than in other studies that used improved surgical recovery pathway.22,25,29 Significant reduction in the number of hematomas in the post-protocol group was observed, providing a positive outcome for this study. One reason could be surgeons’ increased awareness of the hematoma occurrence, potentially resulting in more precise execution of hemostasis during surgery. Another contributing factor may be the introduction of topical tranexamic acid for contralateral breast and abdominal donor site wound surfaces at the same time as the implementation of the new protocol. This decision in the unit was influenced by the positive findings of Ausen et al., 31 who demonstrated a reduction in hematoma occurrence with tranexamic acid use in their study.
The prevalence of hematomas in DIEP breast reconstruction surgery necessitates a nuanced exploration of contributing factors and optimal management strategies. Tranexamic acid effectively reduces hematoma formation, while low-molecular-weight heparin administration, despite its potential to increase hematomas, remains necessary.22,31 It is crucial to balance the risk of minor pulmonary embolisms with appropriate anticoagulant therapy. 32 While anticoagulants play a vital role in preventing thrombotic events, the delicate balance between thrombosis prevention and hemorrhagic complications requires further research and evidence-based guidelines on dosing in microsurgery.
Unlike other studies, we observed an increase in minor surgical complications, especially in terms of seromas, in the post-protocol group.22,24,26,28 This may be since in the majority of post-protocol patients drains were removed during their hospital stay. It is notable that post-protocol patients were also discharged significantly earlier, with most being discharged by POD 3, whereas in the pre-protocol group, discharge typically occurred around POD 5 or later, during which time drains were also often kept in place for a longer duration. In addition, we closely tracked also minor complications up till 90 days after the surgery, while many studies recorded complications for 30 days after surgery. This could partially explain the high number of seromas observed in our study since some of the seromas tracked in this study appeared after 30 days of the operation. Since no standard criteria have been set for outcome measures of the different improved surgical recovery pathway protocols, it is challenging to compare our results with those of other studies.
The result of this analysis was that the new protocol led to a shorter fasting period, early mobilization, and shorter LOS. As such, the protocol had a purely positive impact on patients and caregivers, and the unit has no reason to go back to a more conservative care pathway. Furthermore, when comparing our findings to other enhanced surgical pathway protocols, it is noteworthy that similar components, for example in the ERAS protocol—such as minimizing opioid use and maintaining normotension and warmth in patients perioperatively—were already integrated into the hospital’s treatment guidelines. This prior alignment facilitated a more seamless implementation of the unit’s new protocol by the team.
In our opinion, this new protocol can be generalized to other similar centers that perform DIEP reconstructions. It is applicable to all patients, as we did not select specific individuals but instead analyzed all consecutive patients who underwent DIEP procedures.
The limitations of this study were the relatively small number of patients and its retrospective nature. We acknowledge the benefits and importance of continuously monitoring the effects of applying a new protocol in several centers globally. In addition, the new protocol does not include the use of tranexamic acid, which may have affected the complication rates observed in our study. Therefore, we employed a critical approach when comparing our outcomes to those studies that did not involve the use of tranexamic acid.
Conclusion
Our conclusion is that patients can be discharged earlier without risking their safety after the implementation of the new protocol. The LOS was shorter in the post-protocol group without an increase in the number of total complications.
Footnotes
Authors’ contributions
All authors contributed to the conception and design of the study. Material preparation, data collection, and analysis were performed by Ina Korpiola, Elena Surcel, Päivi Merkkola-von Schantz, Susanna Kauhanen, and Maiju Härmä. The first draft of the manuscript was written by Ina Korpiola, and all authors commented on the previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
A standard institutional research permit was approved for this study.