
Abstract
Background and Aims:
Evidence suggests that female surgeons achieve comparable or even more favorable outcomes than male surgeons. It is currently unclear what factors contribute to these potential differences. Possible explanations might be differences in personality traits, communication style, attitude, and risk-taking behavior. This cross-sectional study aimed to examine disparities in personality traits between male and female general surgeons in Sweden.
Methods:
The research was conducted as a cross-sectional study of personality traits. Between August 29, 2022, and December 15, 2023, Swedish specialists in general surgery were invited to participate in an online survey. The survey, assessed with the Big Five Inventory, collected information on self-reported surgeon gender, years in practice, employment data, and differences in personality traits.
Results:
The analysis encompassed responses from 223 Swedish general surgeons: 121 (54%) males and 102 (46%) females. In contrast to female surgeons, male surgeons were older and had longer surgical experience. A higher proportion of male surgeons were employed in rural hospitals. Higher mean scores were observed in all personality traits among female surgeons. The adjusted analysis showed significantly higher scores for conscientiousness (p < 0.001), extraversion (p < 0.001), agreeableness (p = 0.006), and neuroticism (p < 0.001); however, no such change was observed for openness.
Conclusion:
This cross-sectional study demonstrates that Swedish female and male surgeons differ in personality traits. The implications of these results could lead to a deeper understanding of the variations in surgical outcomes based on the gender of the surgeon.
Context and Relevance
Previous research suggests that female surgeons achieve comparable or even more favorable outcomes than male surgeons. It is still unclear what factors contribute to these potential differences. This cross-sectional study aimed to examine disparities in personality traits between male and female general surgeons in Sweden. It demonstrates that female and male surgeons exhibit distinct personality traits. Female surgeons tend to score higher in conscientiousness, extraversion, agreeableness, and neuroticism. Variances in personality traits between genders may elucidate differences in surgical outcomes and speciality selection.
Introduction
The medical field is witnessing a slow shift toward gender equality, as female students comprise more than half of the enrolment in medical schools in various countries.1,2 However, the underrepresentation of female surgeons persists globally, particularly in higher-ranking positions within surgical specialities. 1 Beyond numerical imbalances, several factors may contribute to different conditions in surgery. These factors encompass societal perceptions regarding the suitability of individuals to become surgeons, prevailing norms and the male-dominated culture within the field, varying quality of mentorship, the availability of relatable role models for younger surgeons, and the challenges associated with achieving work–life balance. 2
Despite the gender-based inequalities that female surgeons face during their training and in their work settings, recent evidence suggests that female surgeons may have more favorable outcomes in the short and long term.3–7 A recent large Swedish cohort study demonstrated a lower incidence of intraoperative complications when female surgeons performed cholecystectomies. 5 The reasons for these differences remain uncertain but hypotheses propose that surgical technique, attitude, communication style, and risk-taking behavior in the operating theater could influence outcomes.3–5 Differences in personality traits between the genders may help elucidate these differences.
Personality comprises subjective values encompassing behaviors, emotions, and thoughts, which pose difficulties in assessment. 8 Previous studies categorizing common personality-related adjectives have identified five main dimensions: openness, conscientiousness, extraversion, agreeableness, and neuroticism (OCEAN).8,9 These characteristics can be both positive and negative, depending on the context. 10 A recent review suggested that becoming or being a surgeon is associated with personality traits such as high conscientiousness and low neuroticism; however, regional- and country-specific differences may also exist. 11 While the ideal personality profile for a surgeon is unknown, the occupation requires a blend of emotional resilience, decisive decision-making, and technical skills. 12
Current evidence on these variations in personality traits between male and female surgeons is limited. Bridging this knowledge gap can enhance comprehension and resolution of gender disparities in medicine, particularly within the surgical context. This study aims to assess potential disparities in personality traits between female and male general surgeons in Sweden.
Methods
Study design and setting
A cross-sectional study was performed, including general surgeons from public (rural, county, regional, and university) or private hospitals across Sweden. Data collection occurred in two phases: the first from August 29 to December 12, 2022 and the second from September 28 to December 15, 2023. The term gender is used throughout the manuscript to denote self-reported gender (female, male, or non-binary). The Swedish Ethical Review Authority deemed no ethical approval was needed due to the study’s cross-sectional design and the anonymous collection of surgeon characteristics (dnr 2022-02941-01). The manuscript adheres to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) reporting guidelines for cross-sectional studies. 13
Participants
Surgeons who had completed specialized training in general surgery and were currently practicing in Sweden were included in the study. Recruitment relied on a convenience sampling method. The study information and invitation were emailed to the heads of surgical departments listed by the Swedish Surgical Society and by personal invitations. The email included detailed study information with a direct hyperlink and QR code to the digital survey in Swedish.
Variables and data sources
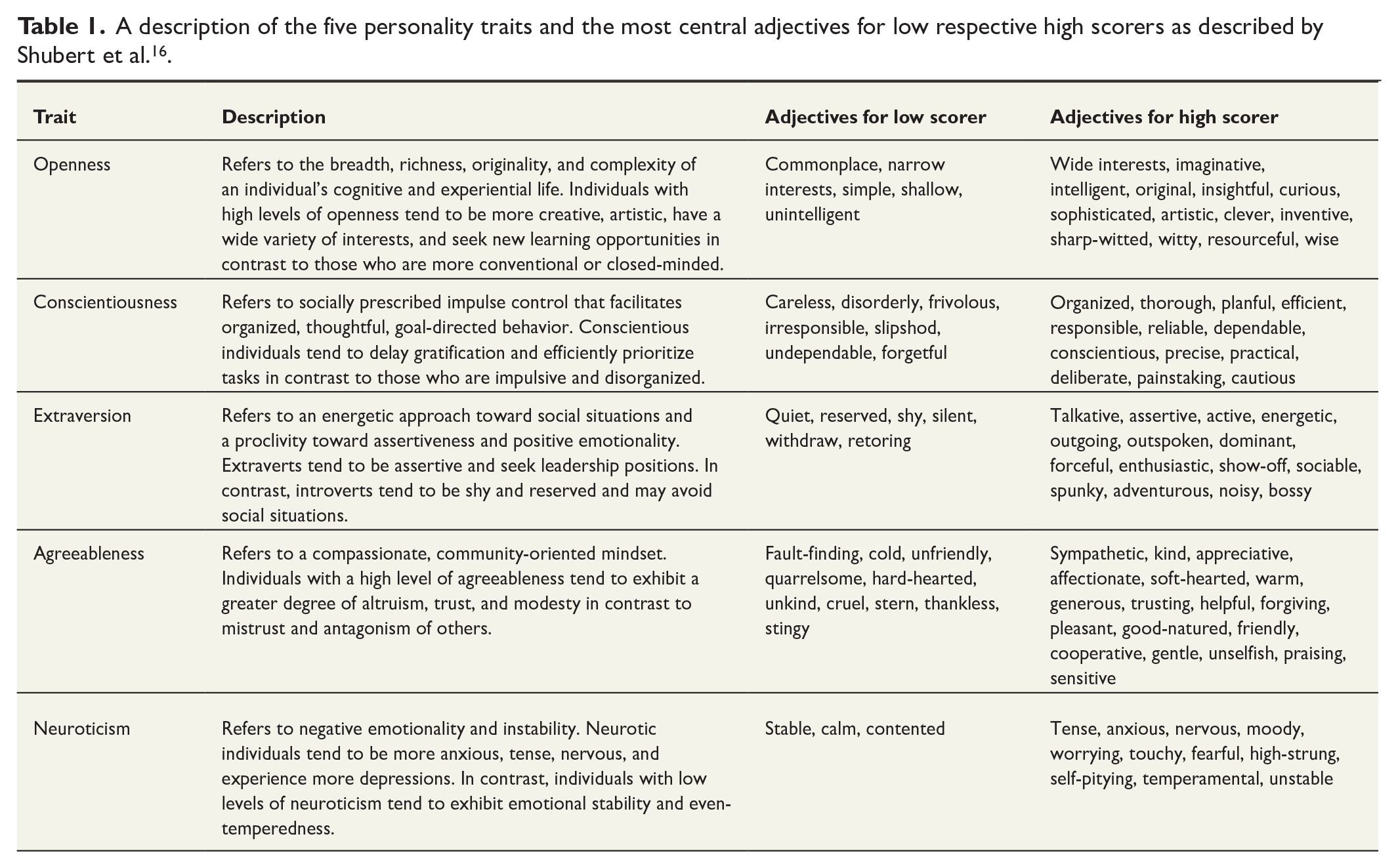
The online survey tool EasyQuest (EasyQuest, Oslo, Norway) was used for data collection. The survey covered self-reported questions concerning surgeon background, including age, gender, year of specialist certification, region of residency, and primary employment. In addition, participants responded to questions about personality traits as measured by the self-reported Big Five Inventory (BFI) scale. The BFI assesses the Big Five domains of personality (openness, conscientiousness, extraversion, agreeableness, and neuroticism).8,14 The participants ranked their level of agreement for 44 questions on a Likert-type scale ranging from “I strongly disagree” (1) to “I strongly agree” (5).14,15 Each personality trait was evaluated with 8–10 questions. The aggregate score for each trait was computed by summing the Likert-type scale scores. 14 Feasible scores (minimum and maximum) for each trait were: openness 10–50 points (p) (10 questions), conscientiousness 9–45 p (9 questions), extraversion 8–40 p (8 questions), agreeableness 9–45 p (9 questions), and neuroticism 8–40 p (8 questions). Table 1 provides a detailed description of the five personality traits, along with the most central adjectives defining low and high scores as described by Schubert et al. 16 The BFI has previously been used to address personality traits in surgeons. 12 The Swedish version of the BFI, validated in 2010, was used in the study. 14
A description of the five personality traits and the most central adjectives for low respective high scorers as described by Shubert et al. 16 .
Study size
In 2021, there were 1536 active specialists in general surgery in Sweden: 502 (32.7%) female and 1034 (67.3%) male surgeons. 17 To ensure a sufficiently large sample size with the ability to detect a significant difference between genders, with 90% power at the p < 0.05 level, 88 male and 81 female surgeons would be required. The sample size calculation was determined based on an estimate of 1000 male and 500 female surgeons.
Statistical methods
Demographics of the participating surgeons were presented as numbers, proportions, or mean values with standard deviations (SD). Differences in mean personality scores between male and female surgeons were assessed using analysis of variance (ANOVA) and analysis of covariance (ANCOVA) through general linear modeling. Bonferroni corrections were applied in the ANCOVA to address the issue of multiple comparisons. Effect sizes were estimated using Cohen’s d. Results were presented as mean values with corresponding 95% confidence intervals (CIs) and p values. Crohnbach’s alpha was calculated for the items. A two-sided p value of ≤0.05 was considered statistically significant. SPSS version 29 (IBM Corp, Armonk, NY, USA) was used for statistical analysis.
Results
Participants
An invitation was extended to surgeons from 46 departments in Sweden, resulting in a survey response rate of 225 specialists in general surgery. Following the exclusion of two surgeons over the age of 70 years who were no longer in active clinical service, the final cohort comprised 223 surgeons. In total, 121 (54.3%) males and 102 (45.7%) females were included in the analysis (no surgeons were identified as non-binary). The captured responses correspond to 14.5% (223 of 1536) of all active general surgeons in Sweden. 17 Among the 223 surgeons in the analysis, 107 (59 males and 48 females) responded in the first phase of the survey in 2022, while 116 (62 males and 54 females) responded in the second phase in 2023. Notably, 55% of those who initiated the survey successfully completed it.
Descriptive data
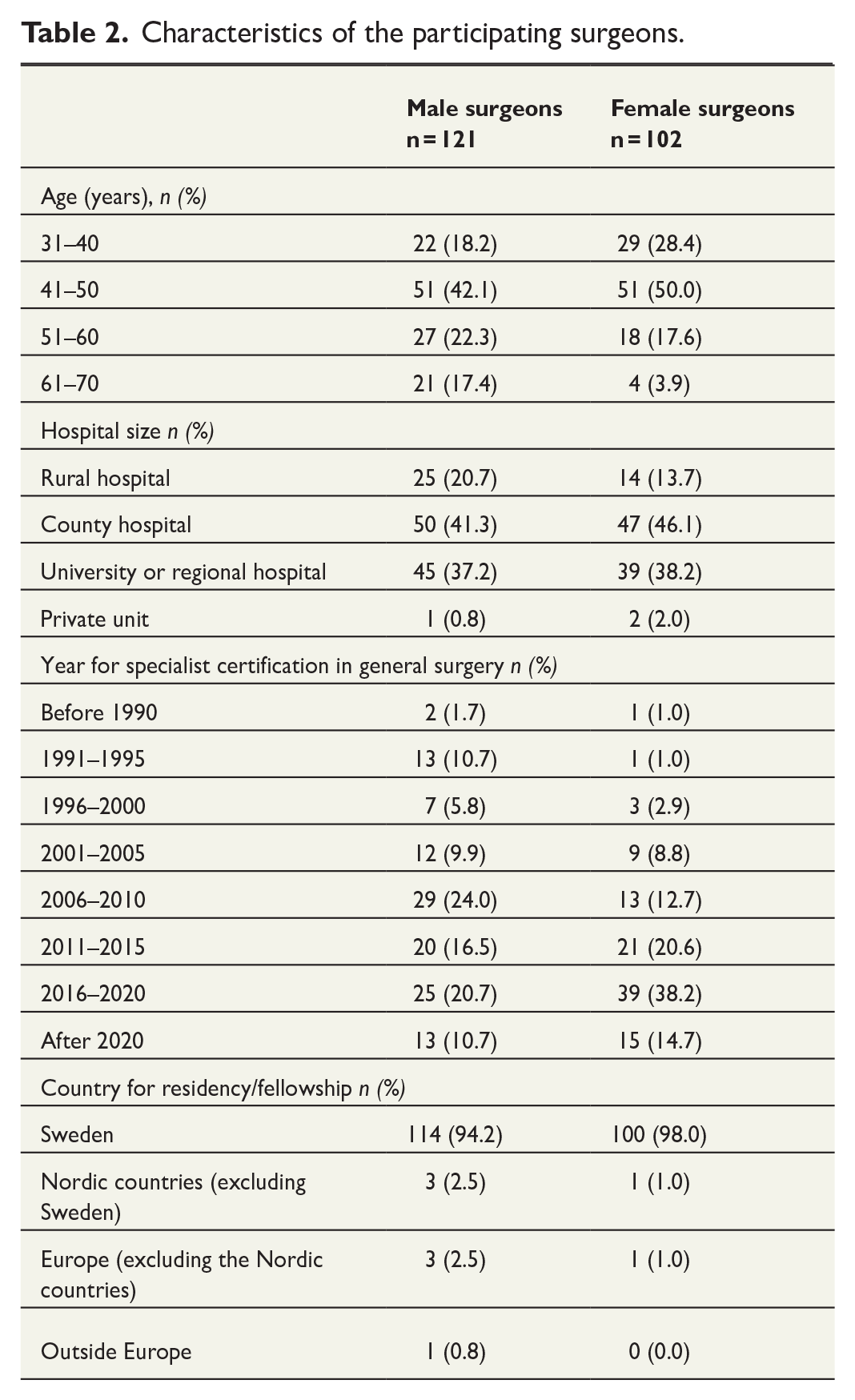
Male surgeons who responded to the survey were older than their female counterparts and had longer clinical experience at the specialist level (Table 2). Minor differences were noted in the geographical distribution of the residency programs among surgeons, with a higher proportion of male surgeons completing their residency requirements in countries other than Sweden. In addition, subtle variations in primary employment settings were seen, where a larger percentage of male surgeons were predominantly employed in rural hospitals (Table 2).
Characteristics of the participating surgeons.
Outcomes
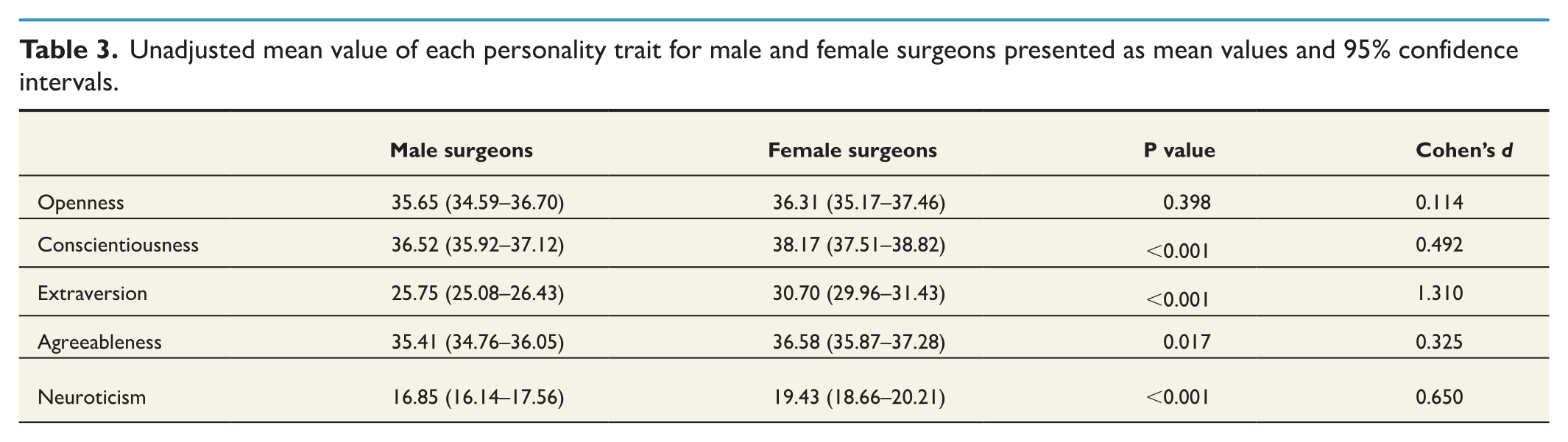
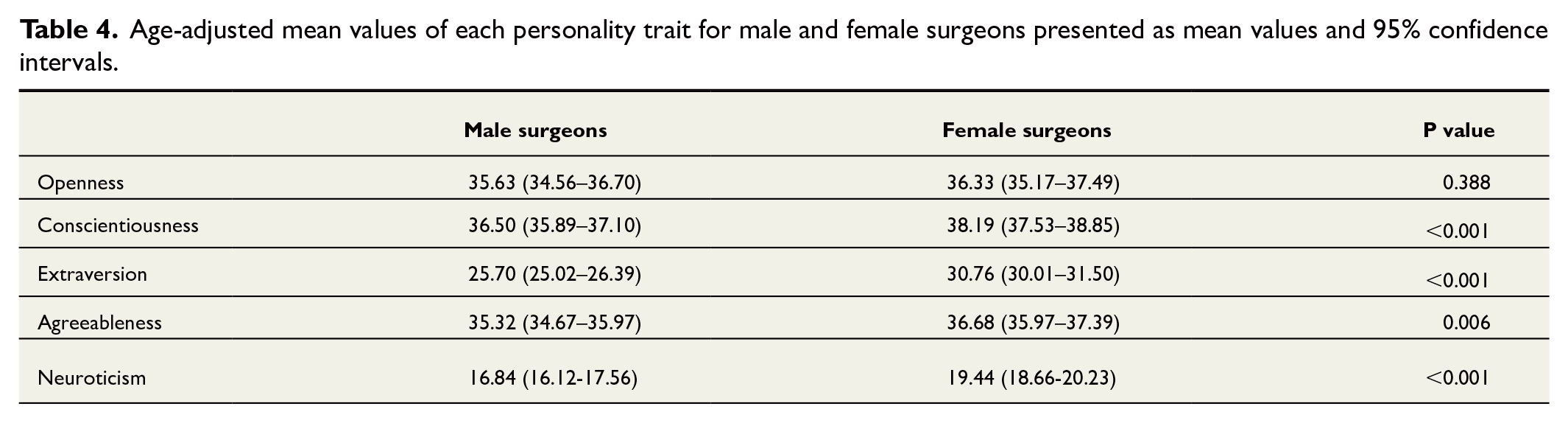
Female surgeons reported higher mean values across all assessed personality traits (Table 3). The non-adjusted analysis revealed statistically significant gender differences in conscientiousness (p < 0.001), extraversion (p < 0.001), agreeableness (p = 0.017), and neuroticism (p < 0.001). No statistically significant disparities were noted for openness (p = 0.398). After adjusting for age, female surgeons maintained significantly higher mean values for conscientiousness (p < 0.001), extraversion (p < 0.001), agreeableness (p = 0.006), and neuroticism (p < 0.001), but not for openness (p = 0.388) (Table 4 and Figure 1).
Unadjusted mean value of each personality trait for male and female surgeons presented as mean values and 95% confidence intervals.
Age-adjusted mean values of each personality trait for male and female surgeons presented as mean values and 95% confidence intervals.
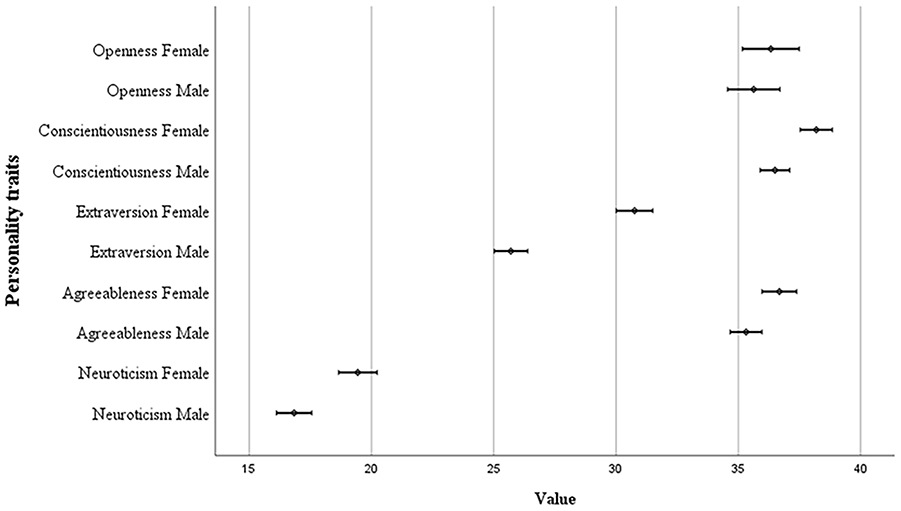
Forrest plot for all personality traits presented as adjusted mean values with 95% confidence intervals.
Reliability
Crohnbach’s alpha was calculated for all 44 items, yielding an overall value of 0.70, with individual item values ranging from 0.68 to 0.72. The values correlate with the results from the Swedish validation study. 14
Discussion
The results of this cross-sectional study suggest that there are contrasting patterns of personality traits among male and female surgeons in Sweden. Female surgeons scored higher in four of five dimensions of personality, demonstrating significantly elevated levels of conscientiousness, extraversion, agreeableness, and neuroticism. No significant difference was observed for openness.
Despite Sweden’s position as the fifth most gender-equal country globally, only 32.7% of the general surgeons were females in 2022.17,18 Still, the percentage of consultant female general surgeons in the United Kingdom was only 17.5%. 19 In Sweden, a surgical specialization requires 5–6 years of surgical residency. This period of specialist training has traditionally been preceded by the successful completion of a 5.5-year medical program and an internship with basic training and practical rotations for a minimum of 18 months across various medical specialities, including surgery. A transition to a 6-year medical school program is currently being introduced.
Research on gender differences in personality traits exists across various domains, yet little evidence is found within medicine, particularly in surgery. A study on the normative Swedish population unveiled that women demonstrated greater warmth, emotional variability, and meticulousness than men. 14 Internationally, women attain higher scores in neuroticism compared to men. 8 According to a Dutch study in the medical field, surgeons, surgical residents, and medical students interested in surgery displayed elevated levels of openness, conscientiousness, extraversion, agreeableness, and reduced levels of neuroticism compared to their normative population. 12 Another study comparing surgeons and internists found higher conscientiousness, extraversion, and agreeableness among internal medicine physicians. 20 Gender differences were not explored in this study. A study conducted with members of the Royal College of Surgeons of England revealed that surgeons scored higher in openness, conscientiousness, agreeableness, and neuroticism compared to individuals outside the field. Among the respondents, female surgeons, who were over-represented in the survey with 43% of the responses compared to 10% of the eligible participants, scored higher in openness and extraversion. 21 A large study involving 2837 Finnish physicians, including 229 surgeons, found that higher conscientiousness, along with lower agreeableness and neuroticism, was associated with a tendency to specialize in surgery. 22 A global survey of 127 colorectal surgeons revealed that compared to the general population, these surgeons exhibited higher emotional stability, lower agreeableness, extraversion, and openness while maintaining similar levels of conscientiousness. In addition, female surgeons demonstrated lower levels of openness. 23 Personality development is a lifelong process influenced by age and significant life events. The OCEAN personality traits have been observed to follow an inverted U-shaped trajectory, reaching their peak in the age group 40–60 years. However, only conscientiousness shows a consistent increase in stability. 24 In our study, female surgeons scored significantly higher in all personality traits, except for openness.
The projected effects of personality traits on the professional performance of male and female surgeons are expected to have implications for both short- and long-term patient outcomes. However, the available literature fails to provide a clear understanding of how personality traits specifically affect these outcomes. Surgical outcomes in specialized fields are influenced by a lot of factors, such as decision-making, technical proficiency, teamwork dynamics, efficient intra-team communication, and patient-related factors. According to previous studies,3–7 female surgeons have demonstrated comparable or more favorable outcomes in the short and long run. Several factors have been suggested as contributing to this positive association, including a communication style that prioritizes the individual and variations in the selection process for elective surgery patients.3–5,14 Female physicians have also been shown to provide more preventive services to their patients. 25 However, higher frequencies of intraoperative complications observed for male surgeons in cholecystectomies, including major bleedings, bile duct injuries, and visceral perforations, suggest that differences in surgical technique, attitudes, and risk-taking behavior may also influence outcomes. 5 In addition, studies indicate practice pattern variations between male and female physicians at the group level, with females showing greater adherence to clinical guidelines and evidence-based practice. 26
In a study focusing on cardiothoracic surgeons, lower extraversion was associated with better outcomes while higher openness was linked to worse outcomes. However, the sample size included only two female surgeons out of a cohort of 53 surgeons. 27 The authors found no significant correlation between the remaining personality traits. Moreover, high extraversion has been identified as a protective factor against burnout in surgical residents, while elevated neuroticism scores elevate the risk. 28 The uncertainty surrounding the significance of the higher levels of extraversion observed among female surgeons in our study suggests either a potential presence of essential qualities for surgeons or the necessity for high extraversion to counterbalance the selection factors encountered by female physicians when entering the field of surgery. 29 The higher conscientiousness scores among female surgeons may give insights into the observed variances in intraoperative complications and help account for the slightly longer operating times noted in previous research.4,5 In addition, a higher neuroticism score might lead to heightened apprehension for bleeding and potential complications, thus prompting a more meticulous surgical approach and a willingness to consult a colleague for assistance. Conscientiousness and neuroticism may influence patient selection, pre-surgery optimisation, and postoperative follow-up. Higher scores may influence teamwork dynamics and communication within the surgical team regarding agreeableness. The association of personality traits and surgical outcomes merits further study to fully understand their impact on surgical performance.
Strengths and limitations
One notable aspect of the study is its acceptable participation rate, as 14.5% of all active general surgeons in Sweden, from both public and private hospitals, contributed. However, several limitations should be acknowledged. First, the study employed a self-reported digital survey to gather data from a targeted cohort of surgeons in Sweden. A further constraint arises from using convenience sampling, which carries the risk of introducing sampling bias. Another limitation is that the survey was distributed to the heads of surgical departments without confirmation of whether the survey was forwarded to the employed surgeons. Consequently, responses from some regions might be missing, potentially limiting the generalizability of the findings. Survey bias depends on the response and completion rates, with the latter being correlated to the survey’s length. While there is no defined benchmark for what constitutes an adequate response rate in surveys, our study shows a completion rate of 55%. However, this number is still high, considering the extensive survey with 50 questions. 30 A somewhat uneven response rate was observed, deviating from the gender distribution for all general surgeons in Sweden: 54.3% of males and 45.7% of females responded to the survey. This gender-related disparity could potentially introduce selection bias, compromising the generalizability of the results. We opted for a completely anonymous survey to maximize the reliability of the collected responses. However, anonymity increases the likelihood of receiving duplicate or non-specialist responses regarding general surgery in Sweden.
The foundation of this study lies within the context of a Swedish surgical population. Generalizing findings related to personality traits in health care is challenging due to the potential influence of cultural differences, societal norms, and variations in health care structures, all of which may impact outcomes. Hence, it is crucial to exercise prudence when evaluating the potential application of these outcomes in other countries.
Implementation and clinical significance
The literature highlights female surgeons’ challenges compared to their male counterparts. Female physicians are more likely to experience gender-based discrimination, sexual harassment, marginalization, and gender-based disparities in pay. 2 Prospective physicians are influenced by a variety of factors when making the decision to specialize in their final years of medical school. Females may encounter discouragement when pursuing certain specializations (e.g. surgery), primarily due to prevailing workplace cultures. At the same time, men may be deterred by knowledge areas or a wish to align their professional paths with predominant male role models. 31 In surgical education, it is important to acknowledge gender differences in personality traits. Despite the rise in the number of female students entering medical schools, it is unlikely that gender equality in residency or higher academic positions will be achieved in the near future. 32 Given the general interest in personalized or adaptive learning and the recognized barriers women face when pursuing surgical careers, it becomes imperative to incorporate an awareness of personality trait disparities into the design of speciality training programs.
Conclusion
The study found that Swedish female general surgeons demonstrated significantly elevated levels of conscientiousness, extraversion, agreeableness, and neuroticism compared to their male counterparts. The implications of these findings are significant, as they have the potential to shed light on the topic of gender diversity within surgical specialties.
Footnotes
Acknowledgements
The authors thank Dr Leslie Shaps for proofreading the manuscript. The study was not preregistered in an independent, institutional registry.
Author contributions
M.B. contributed to Data curation, Formal analysis, Funding acquisition, Project administration, Resources, Validation, Visualization, Investigation, Writing—original draft preparation, review & editing. A.M. contributed to Investigation, Methodology, Supervision, Validation, Writing—review & editing. S.M. contributed to Conceptualization, Investigation, Methodology, Supervision, Validation, and Writing—review & editing. P.J. contributed to Conceptualization; Data curation; Formal analysis; Funding acquisition; Methodology; Validation, Visualization, Resources; Software; Writing—review & editing.
Data availability statement
All data collected for the study can be obtained from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by grants from the Research Fund at Skaraborg Hospital, Sweden (grant no. VGSKAS-980298) and the Center for Clinical Research, Falun, Sweden (grant no. CKFUU-963291). Dr Leslie Shaps was compensated for their work with funds from grant VGSKAS-980298. The funding sources were not involved in the study’s design and conduct, including data collection, analysis, interpretation of data, writing of the report, or in the decision to submit the paper for publication.