
Abstract
International and national guidelines recommend metabolic and bariatric surgery (MBS) as a treatment option for adolescents with severe obesity, but few countries offer MBS to adolescents in routine clinical care. This narrative review summarizes existing adolescent MBS guidelines and the available underpinning evidence. Two randomized trials and additional prospective studies have demonstrated efficacy and safety in adolescent MBS, and the health benefits appear to be similar or superior to outcomes in adults. However, there are specific challenges regarding the intervention during adolescence related to decision-making capacity and a peak in risk-taking behavior. Adolescents with severe obesity have—as a group—a mental health vulnerability, and specific nutritional concerns need to be addressed in relation to MBS. This review also describes how study findings can be translated into clinical care. We use Sweden as an example, where the National Board of Health and Welfare recommends MBS for selected adolescents with severe obesity aged 15 years or older. We present practical advice for implementing and integrating MBS in adolescents in the framework of multidisciplinary pediatric and adolescent care for obesity.
Context and Relevance
An increasing number of adolescents lives with severe obesity, which has profound effects on their lives and well-being.
Metabolic and bariatric surgery (MBS) has been assessed as a treatment option for adolescents in two randomized controlled trials and several prospective studies, and MBS is a recommended treatment for adolescents in recently published guidelines.
In this narrative review, we compile and compare the guidelines recommending MBS in adolescents and report the evidence that constitutes today’s knowledge about the safety and efficacy of adolescent MBS. We also discuss the implications for clinical practice.
Introduction
Bariatric surgery—often referred to as metabolic and bariatric surgery (MBS)—is an evidence-based, well-established, and effective treatment for adults with severe obesity. Long-term data demonstrate sustained weight loss, improvements in physical quality of life, reduction in incidence of type 2 diabetes and cardiovascular events (stroke and myocardial infarction), liver impairment, poly-cystic ovary syndrome and cancer, as well as reduced mortality.1,2
The physical and emotional burden of severe obesity adds another dimension to the transition from childhood to adulthood during adolescence, a journey which can be challenging in itself. In recent years, MBS has gained recognition as a valid treatment option in adolescents, sparking debates about its risks, benefits, and ethical considerations. Undergoing MBS can have a pivotal impact on the lives of young people navigating through adolescence with severe obesity and its associated effects on health.
New and emerging obesity management medications are attractive and reversible treatment options for young people living with obesity, 3 and evidence is urgently needed to define the respective roles of new medications and MBS in the treatment of adolescents with severe obesity. Nevertheless, MBS is a recommended treatment and should be considered in adolescents with severe obesity. In this article, we aim to summarize the evidence supporting the use of MBS in adolescents and explore the multifaceted aspects.
The regulatory aspects—Adolescents are eligible for MBS
Four guidelines have recently been updated and recommend MBS for adolescents with severe obesity, including the guidelines issued by the Swedish National Board of Health and Welfare 4 – 6 see Table 1 for a summary. All guidelines emphasize good safety and efficacy when using MBS in adolescents but reinforce the need for delivery in a comprehensive tailored multidisciplinary care. The surgical professional associations, as compared to the medical associations, appear to have fewer reservations and do not propose a lower age limit for MBS. 4 In the United States, the American Association of Pediatrics recommends MBS from the age of 13 and above, but stresses need for continuous research. 5 Guidelines in the United Kingdom opens for considering MBS in adolescents, however limited to “in exceptional circumstances.” 6
Guidelines on adolescent metabolic and bariatric surgery.
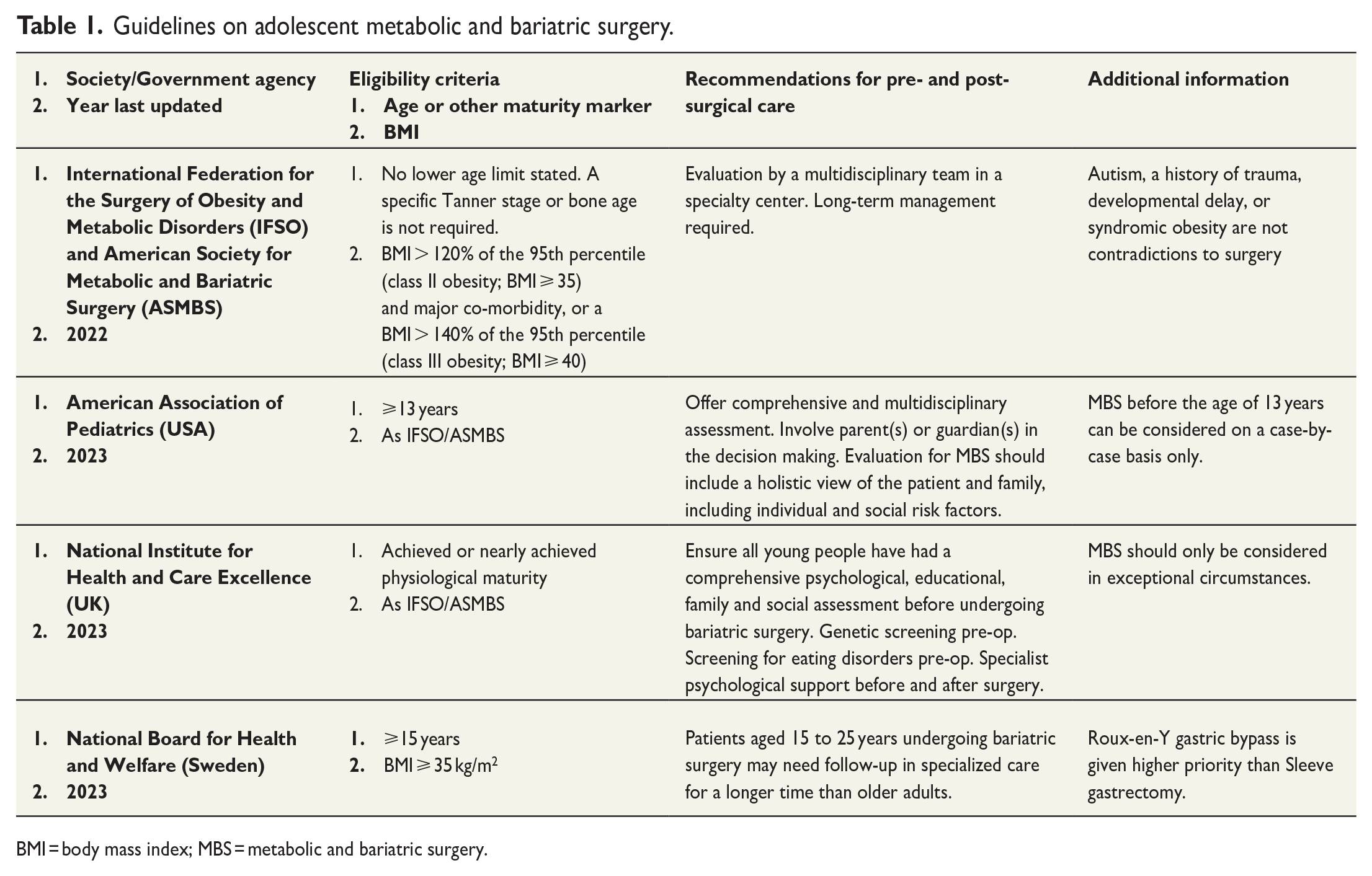
BMI = body mass index; MBS = metabolic and bariatric surgery.
A preoperative assessment by a multidisciplinary team with experience in the treatment of pediatric obesity is a prerequisite highlighted in all guidelines (Table 1). The need for evaluation beyond age and BMI is emphasized4,5 and an approach with an assessment of physical and psychosocial needs is recommended.
The Swedish guidelines addressing adolescent MBS
Authorities in Sweden have published two guidelines dealing with adolescent MBS. The Swedish national guidelines for the treatment of obesity were first published in 2022 to guide stakeholders and decision-makers and define priority for what interventions should be provided. 7 A treatment program for childhood obesity was published in 2023 as a practical treatment guide directed to healthcare professionals. The Swedish guidelines are generally well aligned with the international (Table 1), but the Swedish guidelines give Roux-en-Y gastric bypass a higher priority than sleeve gastrectomy based on existing evidence, whereas the other guidelines do not prioritize between surgical techniques. In Sweden, the costs for adolescent MBS are fully covered by the tax-funded national healthcare system.
Evidence supporting adolescent MBS
So far, two randomized controlled trials have been published investigating the safety and efficacy of MBS in adolescents. The first study was performed in Australia between 2005 and 2008, comparing gastric banding (a procedure in limited use today) to lifestyle treatment. 8 The second, Adolescent Morbid Obesity Surgery–2 (AMOS2), was performed in Sweden comparing MBS (predominantly gastric bypass) to intensive non-surgical treatment between 2014 and 2017. 9
In addition, there are several prospective studies evaluating adolescent MBS, where some studies have control groups with adolescents in lifestyle treatment. Table 2 presents high-quality published studies, several ongoing, in adolescent MBS and their respective outcomes. Below, we summarize the findings from adolescent studies and suggest how the findings can be translated to, and used, in clinical care.
Randomized controlled trials and prospective studies of adolescent metabolic and bariatric surgery.
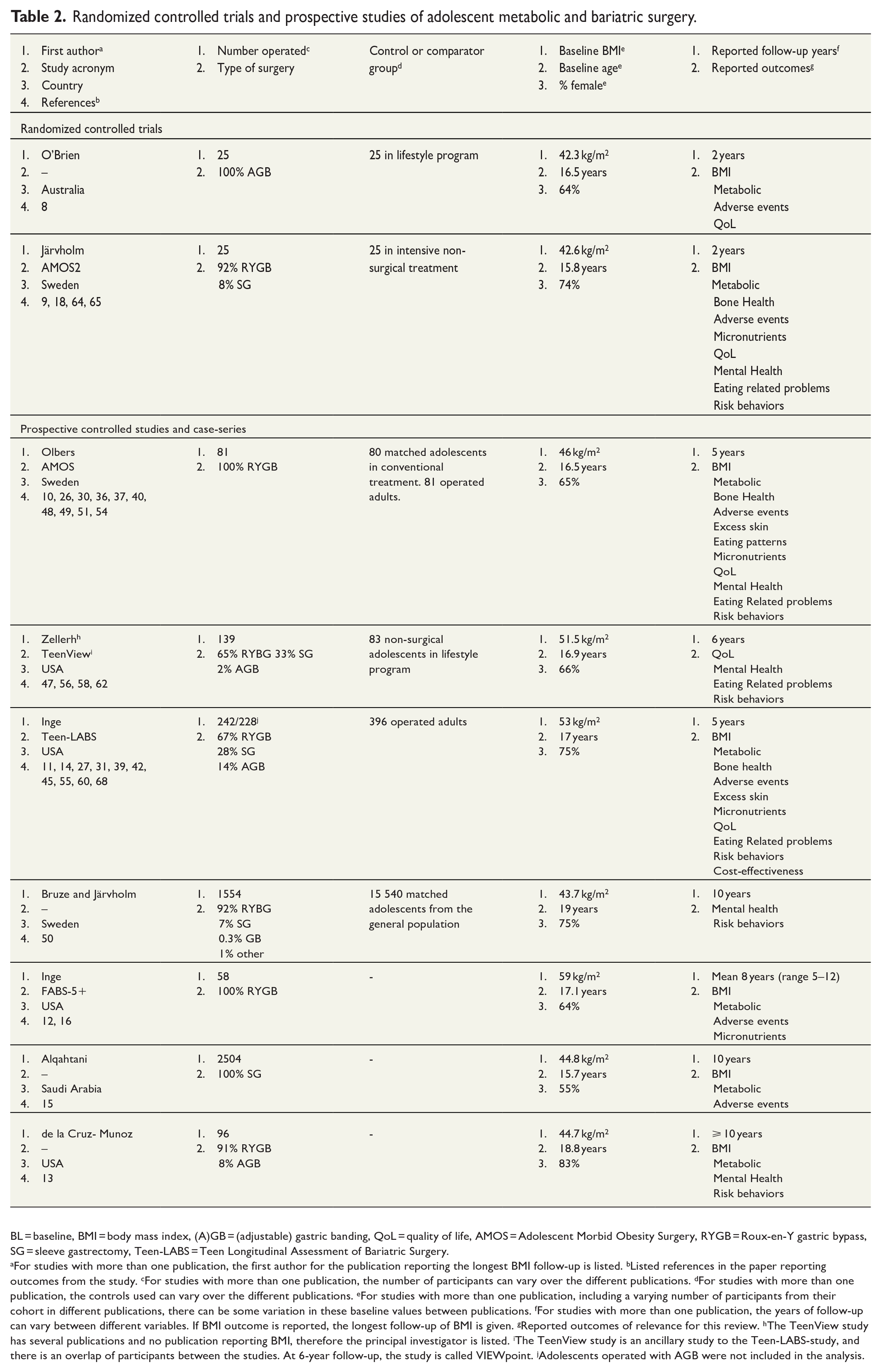
BL = baseline, BMI = body mass index, (A)GB = (adjustable) gastric banding, QoL = quality of life, AMOS = Adolescent Morbid Obesity Surgery, RYGB = Roux-en-Y gastric bypass, SG = sleeve gastrectomy, Teen-LABS = Teen Longitudinal Assessment of Bariatric Surgery.
For studies with more than one publication, the first author for the publication reporting the longest BMI follow-up is listed. bListed references in the paper reporting outcomes from the study. cFor studies with more than one publication, the number of participants can vary over the different publications. dFor studies with more than one publication, the controls used can vary over the different publications. eFor studies with more than one publication, including a varying number of participants from their cohort in different publications, there can be some variation in these baseline values between publications. fFor studies with more than one publication, the years of follow-up can vary between different variables. If BMI outcome is reported, the longest follow-up of BMI is given. gReported outcomes of relevance for this review. hThe TeenView study has several publications and no publication reporting BMI, therefore the principal investigator is listed. iThe TeenView study is an ancillary study to the Teen-LABS-study, and there is an overlap of participants between the studies. At 6-year follow-up, the study is called VIEWpoint. jAdolescents operated with AGB were not included in the analysis.
Summary of reported outcomes
Body mass index
Overall BMI and weight loss outcomes in adolescents are comparable to results in adults. As in adults, the mean long-term weight outcomes vary according to the type of surgical procedure. In the first randomized controlled trial with adolescents by O’Brien et al.,
8
a 2-year BMI change of –12.7 kg/m2 was reported in the gastric banding group compared to –
In observational studies, the 5-year total weight loss after gastric bypass was 28% and 26% in a Swedish and an American adolescent study, respectively, which represents a BMI reduction of 13 kg/m2.10,11 The long-term follow-up (mean 8, range 5–12 years) after gastric bypass in the FABS5+ study, reported a total weight loss of 29% and a corresponding BMI reduction of 16.9 kg/m2. 12 The longest follow-up so far (⩾10 years), have reported BMI outcomes in adolescents and young adults (median age of 19 years at baseline), where 91% (87/96) of them underwent gastric bypass. The mean total weight loss was 31.3%, corresponding to a BMI reduction of 14.5 kg/m2. 13
Over the first 3 years after sleeve gastrectomy, participants in the US Teen Longitudinal Assessment of Bariatric Surgery (Teen-LABS) study had a total weight loss of 27%, corresponding to a 13 kg/m2 BMI-reduction. 14 A large case series from Saudi Arabia reported outcomes in 2504 children, adolescents, and young adults (age 5–21 years) undergoing sleeve gastrectomy. The mean baseline BMI was 44.8 kg/m2, corresponding to a mean BMI z-score of 3.0 based on Saudi national growth charts. In this cohort, 37% were followed for at least 4 years, with a reported mean BMI reduction of 17.9 kg/m2, and 22% were followed over seven or more years with a mean BMI reduction of 16.3 kg/m2. 15 For the group followed at least 4 years, the BMI z-score was 1.7 at follow-up. For the group followed for at least 7 years, the BMI z-score was 1.9.
Comparative data (mainly from the use of gastric bypass, but also sleeve gastrectomy) demonstrate similar weight loss outcomes between adolescents and adults undergoing MBS up to 5 years after surgery.10,11 Even if the mean weight loss seen in adolescents mimics the results in adults, a greater variability in weight outcomes is generally seen in adolescents. 10 In the FABS5+ study, no dietary habits or physical activity assessed ⩾ 5 years after MBS were significantly related to adolescents’ long-term weight loss, but there was an association between greater weight loss and reporting better weight related quality of life. 16
Metabolic outcomes
Children with obesity often have high fasting insulin levels, impaired fasting glucose, and elevated liver enzymes, all of which reflect insulin resistance. Insulin resistance is considered a major driver of complications related to obesity in adolescents with obesity, such as type 2 diabetes, non-alcoholic fatty liver disease, and emerging polycystic ovary syndrome. 17 In AMOS2, none of the 50 patients had type 2 diabetes at baseline. 18 In the surgery group, 12/13 (92%) of adolescents with disturbed glucose homeostasis at baseline had normalized the impaired fasting glucose after 2 years, compared to 2/10 (20%) in the group randomized to intensive non-surgical treatment. 9
There is often an almost immediate improvement in insulin sensitivity in patients with type 2 diabetes or prediabetes after MBS despite not having lost any weight yet. 19 The phenomenon is likely mediated by the neuro-hormonal effects secondary to changes in gut anatomy but also to reduced caloric intake. The remission rates from type 2 diabetes after MBS seem higher for young patients than in adults. 11 A short duration of type 2 diabetes is associated with better chance of long-term remission. 20 During 5 years of follow-up, adolescents showed a higher probability of remission in cardiometabolic risk and physiological stress compared to adults. 11
Height and puberty after adolescent MBS
Children with obesity typically increase faster than expected in height in the years before puberty. In contrast, the growth spurt during puberty is blunted. The final height has not been shown to be affected by obesity or by surgical or non-surgical obesity treatment.15,21,22
There has been a concern of affecting pubertal development and growth spurt in adolescents undergoing MBS, and a common inclusion criterion has been a Tanner pubertal stage 3. 18 Over time, this precautionary principle has been challenged, and a guideline issued by two surgical associations has no age or pubertal stage limit (Table 1). 23
Weight loss after MBS appears to be beneficial for pubertal development. In boys, less testosterone is converted to estrogen in the adipose tissue, and in girls, the improved insulin sensitivity and reduced androgen levels improve the menstrual cycle. Hence, both sexes are normalizing levels of sex hormones following MBS.24,25
Bone health
Generally, children and adolescents with obesity have a higher-than-normal bone mass with high density compared to normal-weight peers as assessed with dual-energy x-ray absorptiometry (DXA). 26 In the randomized AMOS2 study, the operated adolescents had a steep decrease in bone mineral density over 2 years, but they remained in the normal range. The bone mineral density in the control group in AMOS2 was unchanged. 9 In a study from the United States, adolescents 5 to 11 years after MBS had a somewhat lower bone density compared to an age and weight matched non-operated group. 27
Surgical complications and adverse events
Adverse events after MBS in adolescents are nowadays less frequent and milder than in previous observational studies. 10 In the first randomized study, using gastric banding, 48% of the operated participants had an adverse event, and 28% needed a reoperation during the 2 years of follow-up. 8 In the randomized AMOS2, conducted almost a decade later and using predominantly gastric bypass, adverse events were few and mild. One participant (4%) underwent cholecystectomy during the 2 years of follow-up. 9 Improvements in surgical technique 28 and the use of prophylaxis for gallstone formation during the rapid weight loss phase likely explain this decrease.
In an American study comparing adolescents and adults over 5 years after MBS, the adolescents had significantly more reoperations than the adult patients. The authors found no apparent cause for this finding and suggested that the difference in reoperations could be due to closer monitoring of the adolescents, a lower threshold to intervene in adolescents compared to adults or recall bias. 11
An increased long-term risk of chronic gastro-esophageal reflux in at least in 1/3 of patients and development of Barrett’s esophagus has been reported after sleeve gastrectomy. 29 Total or partial small bowel obstruction is the commonest major complication after gastric bypass (risk up 5% in recent series). 28 Overall, more “simple” surgical techniques (e.g. gastric banding and sleeve gastrectomy) have a lower risk of early surgical complications which should be weighed to a likely greater need for revisional surgery due to, for example, weight regain over long term.
Dumping syndrome (e.g. palpitation, sweating, unwellness, abdominal pain and nausea after eating) has not been systematically assessed after MBS in adolescents. However, comparative data in non-operated adolescents regarding gastro-intestinal symptoms and eating quality are reassuring. 9
Excess skin
Despite better skin elasticity and plasticity in youth, studies demonstrate that adolescents express substantial complaints about excessive skin after MBS. The excess skin has also been objectively verified, and 88% of participants being assessed in the AMOS-study desired body contouring surgery. 30 In Teen-LABS, 70% reported that they wanted skin-reducing surgery during the first 5 years after MBS, most commonly at the abdomen and arms. 31
Eating patterns
MBS, especially gastric bypass surgery, involves anatomical gastrointestinal changes that lead to altered gut hormone response, neural responses, and gut bacterial diversity. 32 These alterations help to limit food intake and promote weight loss by reducing hunger, increasing satiety, and preventing a reduction in energy expenditure. 33 Changes in dietary intake are predominantly seen during the first year after MBS and include a reduction in energy intake. 34 Recent findings have challenged previous conclusions about changed food preferences after MBS, as patients in rigorous studies tend to eat the same food but in smaller quantities after surgery. 35
Long-term dietary intake in adolescents after gastric bypass is characterized by a decreased portion size. 36 Over 5 years in the AMOS study, macronutrient distribution did not differ between operated adolescents and controls. 37 An adequate intake of protein may support the preservation of muscle mass in adolescents. 37
Supplementation adherence and micronutrient deficiencies
Micronutrient deficiencies involving iron, vitamin D, and vitamin B12, are prevalent in adolescent with severe obesity. 38 Multiple deficiencies have been reported in 10%–98% in adolescent MBS candidates, with a very high BMI associated with higher risk.38,39
Micronutrient deficiencies might persist or deteriorate long term after MBS in adolescents. 38 Deficiencies to look for in adolescents after MBS are iron, vitamin D, and B12.38 –40 Type of surgery, female sex, dark skin, adherence to supplementation, weight regain, and pregnancy are factors associated with increased risk for micronutrient deficiencies after MBS. 39 Iron and B12 deficiencies appear to be more common after gastric bypass compared to sleeve gastrectomy, despite similar weight loss. 39
No adolescent-specific nutritional guidelines after MBS have been presented and best practice guidelines in adults can be used. Daily supplementation of vitamin D and B12 and Iron and calcium along with a multivitamin and mineral supplement is recommended. 41 Adherence to supplementation is low in adolescents without focused strategies. 42 In the AMOS study, approximately 50% of the adolescents took the supplements at least three days per week. 40 Self-reported supplementation in adolescents seems reliable as studies show convergence between self-reported adherence and biochemistry.40,43 Capacity, including both personal awareness and external support, has been identified as a critical factor for adherence in adolescents, 43 whereas forgetfulness and difficulties swallowing tablets have been reported as barriers. 42
Quality of life
Adolescents with severe obesity commonly report an impaired quality of life.44,45 Quality of life improves after MBS, at least in a short-term perspective, without significant differences between surgical procedures. 46 The greatest improvements are reported 1 year after surgery, with a gradual decline over time. Still, improvements have been demonstrated up to 6 years after adolescent MBS. 46
The main improvements are seen in the physical aspects of quality of life,9,10,47 and these improvements are sustained at least over 5 years, 10 while improvements in mental quality of life seem less sustainable. In the randomized AMOS2 study, MBS was not superior in improving mental quality of life compared to intensive non-surgical treatment over 2 years. 9 Prospective studies also report short term improvements in the mental aspects of quality of life after surgery, 48 that erode over time. 49
Obesity-specific quality of life improves after MBS, and sustained improvements have been demonstrated in adolescents until 5 years after surgery. 10 However, in the randomized AMOS2-study, obesity-specific quality of life improved similarly in the operated and the non-surgical treated group over 2 years, indicating that improvements in obesity-specific quality of life does not necessarily require weight-loss. 9
Mental health
As a group, adolescents that are eligible for MBS have a high burden of mental health problems compared to peers.9,50 In the randomized AMOS2 study, there was an improvement in mental health in the operated adolescents during the first year after surgery not seen in the adolescents in non-surgical treatment. However, this difference vanished during the second year of follow-up, and MBS was not superior to intensive non-surgical treatment for improving mental health over 2 years. 9 In line with this finding, prospective short-term studies demonstrate improvements in self-reported mental health, such as reduced symptoms of depression and anxiety after surgery that may represent a post-bariatric “honeymoon.” 51 , 52
An improved self-esteem was reported 5 years after MBS compared to baseline in the AMOS study, however no improvements in overall mood were found. 49 In comparison to the control group, adolescents in AMOS had more specialized psychiatric treatment after, but not before, MBS. 49 The most common registered diagnoses after surgery were depressive episode, unspecified and emotionally unstable personality disorder. 49 A register-based study following almost 1500 operated adolescents (<21 years) in Sweden up to 10 years after MBS, showed that the adolescents had a continued increase in psychiatric treatment and psychotropic drugs over the years following MBS. 50 For all investigated mental health variables, except substance use disorder, the psychiatric care and drug use continued along the pre-surgery trajectories, indicating that MBS neither improve nor deteriorate mental health in adolescents. 50
Eating-related problems
Few adolescents presenting for MBS fulfil the criteria for an eating disorder. However, a substantial proportion report some degree of loss of control over eating or binge eating.54,55 However, eating related problems before surgery, does not seem to impair weight outcome after MBS49,54 or affect dietary intake after gastric bypass. 36
In the randomized AMOS2 study, binge eating, and uncontrolled eating were significantly more improved in adolescents undergoing MBS after 2 years compared to adolescents in non-surgical intensive treatment. 9 Prospective studies have also reported substantial and sustained improvements in eating related problems up to 5 years after MBS in adolescents. 49
Of note, eating-related problems reported after surgery are associated with less weight loss at both 2, 54 5, 49 and 6 years 56 after adolescent MBS. Most adolescents with eating-related problems after MBS have had such problems already before surgery, but there are a few patients with new onset after MBS.49,54 Those having eating-related problems at 6 years reported more often lower self-worth, greater internalizing symptoms, and higher weight-related teasing at baseline. 56 More self-reported binge eating, uncontrolled eating, and emotional eating in adolescents 5 years after MBS were associated with unhealthy dietary traits postoperatively, whereas higher self-reported cognitive restraint at 5 years was associated with a healthier dietary pattern. 36
Risk behaviors
Engagement in risk behaviors begins, and sometimes peak, during adolescence. 57 Thus, MBS in this stage of life takes place during a period when risk taking is at its highest or will peak in the years following surgery.
Smoking
Only the TeenView study has thoroughly reported on smoking behaviors in adolescents undergoing MBS. They found that smoking habits were similar in adolescents undergoing MBS or lifestyle treatment with a similar frequency as among normal weight peers. 58 To the best of our knowledge, no study has assessed other forms of tobacco or nicotine use in adolescents undergoing MBS.
Alcohol
An increased risk of developing substance use disorders, mainly alcohol, has been demonstrated in adults after MBS, with higher risk in younger patients. 59 In a Swedish study an increased risk for healthcare visits listing alcohol use disorder was found over the 10 years following MBS in patients <21 years compared to a reference population. 50 At 7 years after MBS, the proportion receiving treatment for a substance use disorder (of which > 95% alcohol) stabilized around 5%, while the corresponding number in the reference population remained below 1%. 50 In a US study without controls, using a questionnaire to assess alcohol use disorder, approximately half of the cohort reported a new-onset of at-risk alcohol use, alcohol a new-related harm, or alcohol-related problems 8 years after adolescent MBS. 60
Drugs
In adults, gastric bypass is associated with an increased risk of non-alcohol substance use disorder. 61 In the Swedish AMOS2-study, including adolescents aged 13 to 16 years, questionnaire data revealed little drug use among adolescents at inclusion and over two after MBS or non-surgical intensive treatment. 9 In other adolescent studies, substance use beyond alcohol has rarely been systematically assessed, but has still been brought to the researchers’ attention. In the AMOS study, five patients (5.2%, three girls and two boys) reported excessive use of addictive substances (drugs and alcohol) at the follow-up 2 years after MBS, 48 and in the American Teen-LABS study, two of three deaths before the 5-year follow-up were related to drug overdoses. 11
Sexual health and pregnancy
Most data on sexual health after adolescent MBS concern women. In the randomized AMOS2 study, two cases of unintended pregnancies were reported in the MBS group and none in the intensive non-surgical treatment group during 2 years of follow-up. 9 In the non-randomized TeenView study, girls undergoing MBS or lifestyle treatment were followed across 4 years, and pregnancies were more common in the surgical group (25%; n = 21) compared to the conventionally treated group (8%; n = 4). 62 In AMOS, there was one unintended pregnancy in a 16-year-old girl during the first 2 years after MBS, 48 and in Teen-LABS, seven participants reported pregnancy at the 3-year follow-up (of in total 173 participants including both males and females). 14
Low adherence to vitamin and mineral supplementation in adolescents after MBS40,42 may be a risk factor for adverse pregnancy outcomes. Generally, guidelines for adults recommend that pregnancy should be avoided until weight stabilization or 12–24 months after surgery. 41 An American case series including 47 female adolescents (<19 years), a high pregnancy rate was found, as seven pregnancies in six females were reported. Six pregnancies were conceived within 10–22 months after surgery and one 36 months after. All pregnancies resulted in healthy term deliveries. 63
Special considerations in adolescent MBS
The decision process
An inability to understand the potential risks and benefits is normally a contraindication for MBS and is a special concern in adolescents. The adolescent’s autonomy and capacity to make informed consent about their health should be evaluated before MBS. A substantial proportion of adolescents with obesity have concomitant neuropsychiatric problems, mainly characterized by problems in line with ADHD 64 and a substantial proportion has cognitive impairments. 65 Thus, information should be tailored to meet the needs of adolescents with a limited attention span and limited capacity to understand complex information. Pictograms to support the conversation can enable conversation in cases of lowered verbal capacity. 65 Deciding to undergo MBS is not an emergency decision, and information about the intervention should be given on several occasions.
Still, a limited autonomy should not be an absolute contraindication. Ethical expertise suggests that in adolescents where MBS should be a preferred treatment option otherwise due to medical risk, it should also be offered to adolescents with limited decision capacity by using the ethical principle of non-discrimination.
MBS in a family context
The parents or other caregivers should be involved in the decision process as well as in the pre- and post-bariatric care. Their support is supposed to partly compensate for the adolescent’s limited maturity. Parents are indeed seen as an important resource for support by adolescents before and after MBS, but adolescents also report experiences where parents are source of criticism and unsupportiveness. 66 Patients and parents need to work on strategies to optimize their collaboration before and after MBS, a process that may need support from health care providers.
It is common that parents to adolescents presenting for MBS, have personal experiences of MBS. 18 This is generally positive, as the parents can use their experience and knowledge to support. However, health care providers need to secure an autonomy in the adolescent’s decision to undergo MBS.
Cost-effectiveness
Simulation-based cost-effectiveness analyses of MBS versus no surgery performed in adolescence have reported an incremental cost per quality-adjusted life year (QALY) of about £2000 over a lifetime horizon in the UK 67 and $155 000, $114 000 and $91 000 over a 3-, 4- and 5 year time-horizon, respectively, in the US. 68 Both studies showed large simulated QALY gains in the surgery versus the no surgery group, where QALY gains were modeled primarily by using the relationship between BMI and quality of life from other data sources rather than actual quality of life experienced by patients treated or not treated with MBS. The authors of the shorter-term US analysis, which used model input data from the Teen-LABS study, underscored the need for long-term clinical trials that capture costs and QALY endpoints to be used for cost-effectiveness analyses.
The Swedish experience of adolescent MBS
Adolescent MBS is currently centralized to a few university hospitals in Sweden, and approximately between 30 and 40 operations are carried out in patients < 18 years each year. The pre-surgical evaluation assesses existing comorbidities, previous treatment, and longitudinal BMI charts. In addition, adolescents eligible for MBS undergo a psychological assessment including an evaluation of mental health, binge eating symptoms and other eating-related problems, as well as the adolescent’s decision-making capacity and process. Similar predefined questionnaires are used at all Swedish centers offering MBS. At present, the Beck Youth Inventories and the Eating Disorder Examination- questionnaire are used to screen for symptoms of mental health problems and eating disorders. The assessment additionally reviews the social situation of each patient with the aim of securing proper support before, during, and after MBS. A multidisciplinary team including (but not necessarily limited to) a pediatrician, surgeon, psychologist, dietitian, and pediatric nurse, is formed around the adolescent.
In our clinical experience, MBS seems to work best for adolescent patients with a daily structure, a supportive family and an ongoing successful lifestyle modification treatment, including physical activity. Therefore, we aim to strengthen all these factors both before and after MBS.
Starting through research collaborations, a Swedish national advisory network was established bringing together pediatricians, psychologists, surgeons, nurses, and dietitians treating children and adolescents with severe obesity.9,10 Today, the network meets for monthly web-meetings, where anonymized cases that may be eligible for MBS and obesity management medication, are discussed and given non-mandatory recommendations.
Long-term follow-up in clinical care is a challenge after adolescent MBS, as the patients normally transfer from pediatric to adult care at the age of 18 years. With more operated adolescents and young adults, there is a need for long-term follow-up care tailored to the needs of this age group. Today, long-term follow-up in Sweden is delivered in primary care and patients need to remember to schedule yearly appointments, a routine that is hard to establish also for middle aged adults. 69 Some healthcare regions can offer follow-up in specialist care until the age of 25, 70 which is in line with the recommendation from the National Board of Health and Welfare. Due to the mental health vulnerability and risk profile of younger MBS patients, it is particularly important to establish a routine to monitor mental health and substance abuse during long-term follow-up.
Summary
MBS is an effective and well-tolerated option that should be considered for adolescents with severe obesity when lifestyle treatment and/or obesity management medications do not provide sufficient effect. For physical health outcomes, MBS is at least as effective in adolescents as in adults. Previous concerns about interfering with puberty and height have been reassured by data showing normal development after MBS. Adolescents are, however, generally more vulnerable than adults from a mental health and risk behavior perspective, which needs to be considered.
Defining the optimal time-point for MBS in an adolescent’s life is pivotal. Data suggest that postponing surgery leads to further weight gain, deterioration in health, and social isolation that eventually may hinder the adolescent from ever entering an independent adult life. Therefore, much is at stake for the individual, the family, and the society.
The future of adolescent MBS
There is a rapid development in treatment options for young people living with severe obesity with new safe and effective obesity management medications. 3 However, in our experience, the pharmacological treatment may be insufficient for some patients in the higher BMI-ranges, and in Swedish current clinical practice, obesity management medications are often used as a bridge to surgery. Long-term follow-up is needed, and future studies should define optimal roles for pharmacological treatments and MBS, and how the treatment options can be optimally combined. Health care providers need to upgrade their ambitions of using all available options in providing effective and safe treatments to adolescents with severe obesity.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Local principal investigator in a global phase III study of a GLP-1 agonist for children: L.S. (part of clinical work). Lecturing fees from industry: K.J. (reimbursement to clinical institution). T.O. (reimbursement to academic institution). Advisory board for industry: T.O. (reimbursement to academic institution).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.