
Abstract
Background and Aims:
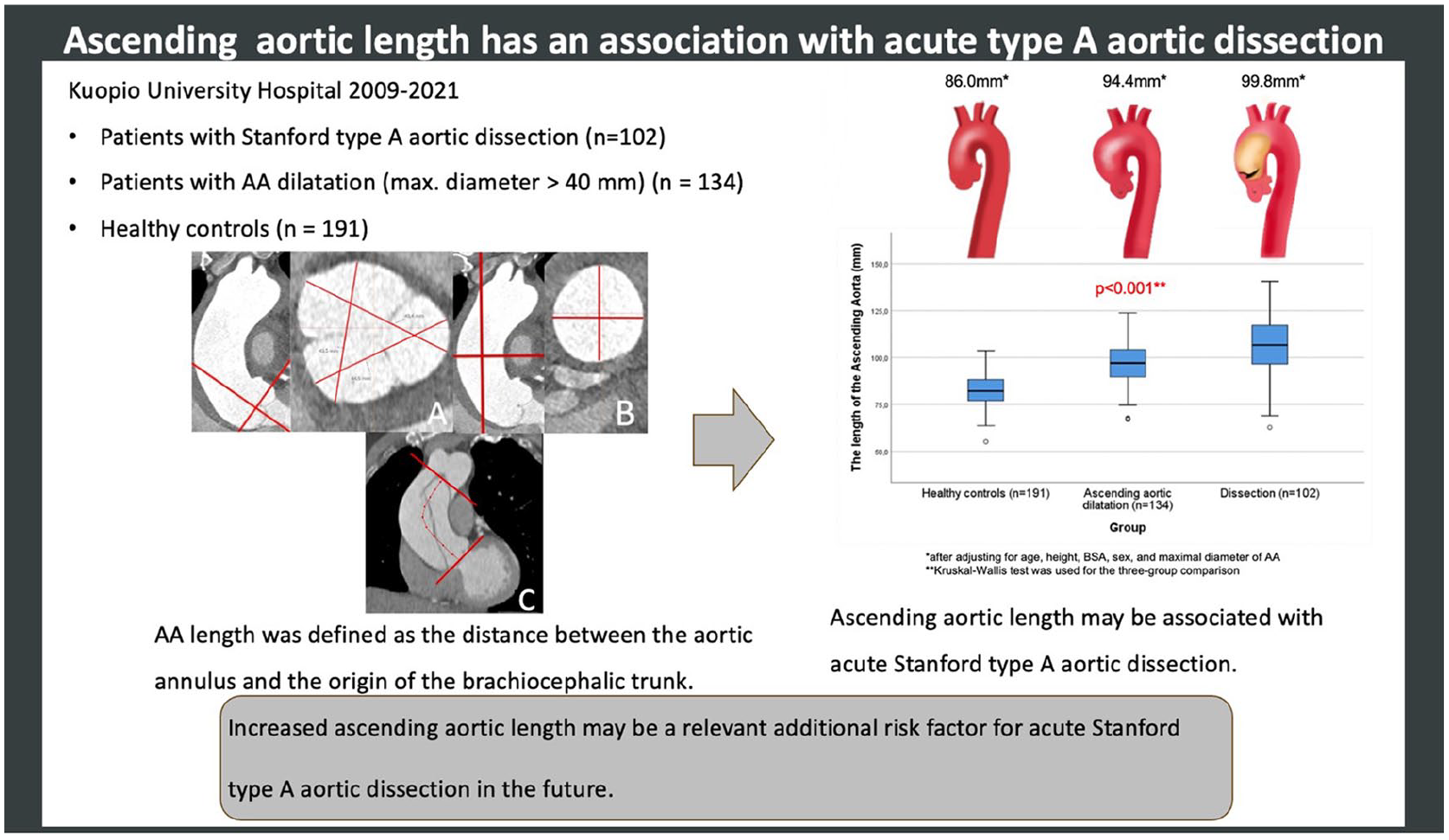
To investigate whether, alongside aortic dilatation, ascending aortic (AA) elongation is associated with the increased risk for aortic dissection.
Methods:
This retrospective study included patients treated for Stanford type A aortic dissection (n = 102) in Kuopio University Hospital between 2009 and 2022, patients with AA dilatation (maximal diameter > 40 mm) (n = 134), and healthy controls (n = 191). AA length and dimensions were measured from aortic computed tomography angiography (CTA) images. AA length was defined as the distance between the aortic annulus and the origin of the brachiocephalic trunk.
Results:
After adjusting the AA length to the patients’ age, height, body surface area (BSA), sex, and maximal diameter, the dissected aortas were 14 mm longer than in the healthy controls and 5 mm longer than in the dilated non-dissected aortas (p < 0.001). The dilated non-dissected aortas were 8 mm longer than in the healthy controls (p < 0.001). In the dissection cohort, 25/102 (25%) patients had maximal AA diameter < 55 mm and 16/102 (16%) patients had maximal AA diameter ⩾ 55 mm together with AA length > 110 mm. By combining 110 mm AA length and < 55 mm diameter, 58% of the dissection patients would have been identified instead of using solely AA diameter ⩾ 55 mm as a cut-off criterion, based on which only 33% patients met the indication for elective surgery.
Conclusion:
AA length seemed to have an association with acute type A dissection, and therefore, it could be an additional tool in identifying patients who may benefit from preventive aortic surgery.
Keywords
Context and Relevance
Currently, preventive ascending aortic (AA) replacement is indicated when the aortic diameter exceeds 55 mm in patients with no other aortopathies. However, the majority of AA complications occur before this threshold is reached. Therefore, new additional predictors are needed. We investigated a cohort of Stanford type A dissection patients treated in our hospital and compared them to non-dissected dilated aortas, as well as to healthy aortas. Based on our findings, increased AA length might play a considerable role in assessing the risk of type A dissection in the future.
Introduction
Along with ascending aortic (AA) aneurysm, acute Stanford type A aortic dissection (ATAAD) is a life-threatening complication of aortic dilatation that is challenging to prevent and predict. The incidence of ATAAD has been reported to be approximately 8.7/100,000 person-years, 1 and its prevalence is estimated to be 13.1/100,000 in men and 9.1/100,000 in women. 2
Without early surgical intervention, ATAAD is associated with poor prognosis. The total mortality rate is 73%, and pre-hospital mortality is up to 49%. 3 The European guidelines suggest prophylactic surgery only when the maximal diameter exceeds 55 mm. In cases with other comorbidities, such as a bicuspid aortic valve (BAV) combined with additional risk factors (e.g. hypertension, rapid increase in aortic diameter), a lower threshold of 50 mm is considered. 4 However, the majority of ATAADs have been shown to occur before the threshold for surgery is reached. Pape et al. 5 showed that 59% of patients with ATAAD enrolled in the International Registry of Acute Aortic Dissection had aortic diameters smaller than 55 mm. It is worth noting that in the moment of the ATAAD, patients have rarely had previous aortic imaging. In addition, when 343 dissected (Stanford type A) aortas were modeled to pre-dissection sizes by Rylski et al., 6 only 3% met the elective > 55 mm criterion for AA replacement. Therefore, new diagnostic predictors are needed to assess the risk before fatal complications occur.
AA elongation is often observed in dissected aortas, but the pathophysiological relationship between elongation and ATAAD is still poorly understood. However, it has been described that the tear of the intima layer of the aortic wall in ATAAD is often seen in a transverse direction, suggesting longitudinal stress on the aortic wall, which may be a consequence of aortic elongation. 7
Based on the previous findings, we assumed that the increased length of AA might have a considerable role in the development of ATAAD. The aim of the present study was to investigate the association between AA length and risk for ATAAD by comparing dissected AAs with non-dissected dilated AAs and healthy aortas in a selected patient population.
Methods
The Institutional Review Board (IRB) or equivalent ethics committee of the Kuopio University Hospital (200/2017) approved the study protocol and publication of data. Based on the IRB guidelines, the study met the criteria for exempting individual participant consent due to its retrospective database review.
Computed tomography angiography (CTA) imaging of the patients with ATAAD was performed before emergency surgery, and there was no need for repeated imaging related to this study. The groups of aortic dilatation and healthy controls were identified from prior studies of aortic dilatation (DilAo-Trial). 8
Study population
The patients’ risk factors for cardiovascular diseases (CVDs) and baseline characteristics were collected from their medical records. Of interest were the patients’ age, sex, weight, height, body surface area, hypertension, dyslipidemia, smoking, family history of CVD, diabetes, and aortic valve anomalies. Hypertension and dyslipidemia were defined if a patient was taking medication prescribed for hypertension or dyslipidemia. Smoking was defined if a patient was mentioned to be a current smoker or had quit smoking < 30 years ago. Family history was considered positive if the patient’s documents indicated a CVD in a first-degree relative.
Dissection population
The present study included a cohort of 102 patients who were admitted to surgery due to ATAAD in Kuopio University Hospital, Heart Center between 2009 and 2022. Pre-operative CTA imaging studies were utilized to measure the length and maximal diameter of AA. All patients admitted to the hospital for ATAAD during the above-mentioned time period were included in the study. Patients with missing weight and height information or insufficient CTA imaging data were excluded.
AA dilatation population and healthy controls
Altogether, 134 patients with AA dilatation and 191 healthy controls (no aortic diseases such as dilatation or prior dissection) who had been imaged with aortic CTA in Kuopio University Hospital between 2014 and 2020 were included. AA was determined as dilated if its maximal diameter exceeded 40 mm at any level. 4 Imaging of the aorta was performed according to routine clinical indications, such as pre-operatively before aortic valve replacement or other heart surgeries in suspicion of aortic dissection or in newly diagnosed (<1 month) aortic aneurysm or dilatation. The detailed exclusion criteria were described in a prior publication. 8
CTA
In the imaging process, electrocardiogram gating and iodinated contrast agent (Omnipaque, GE Healthcare, Chicago, IL, USA) were utilized. CTA images were recorded during peak systole, and the tube voltage (80–120 kV) was set semi-automatically following the patient’s size. The images were scanned from the base of the skull to the level of the groin, with the patient lying in a supine position.
Data collection and assessment of CTA images
Measurement of the AA diameters and length
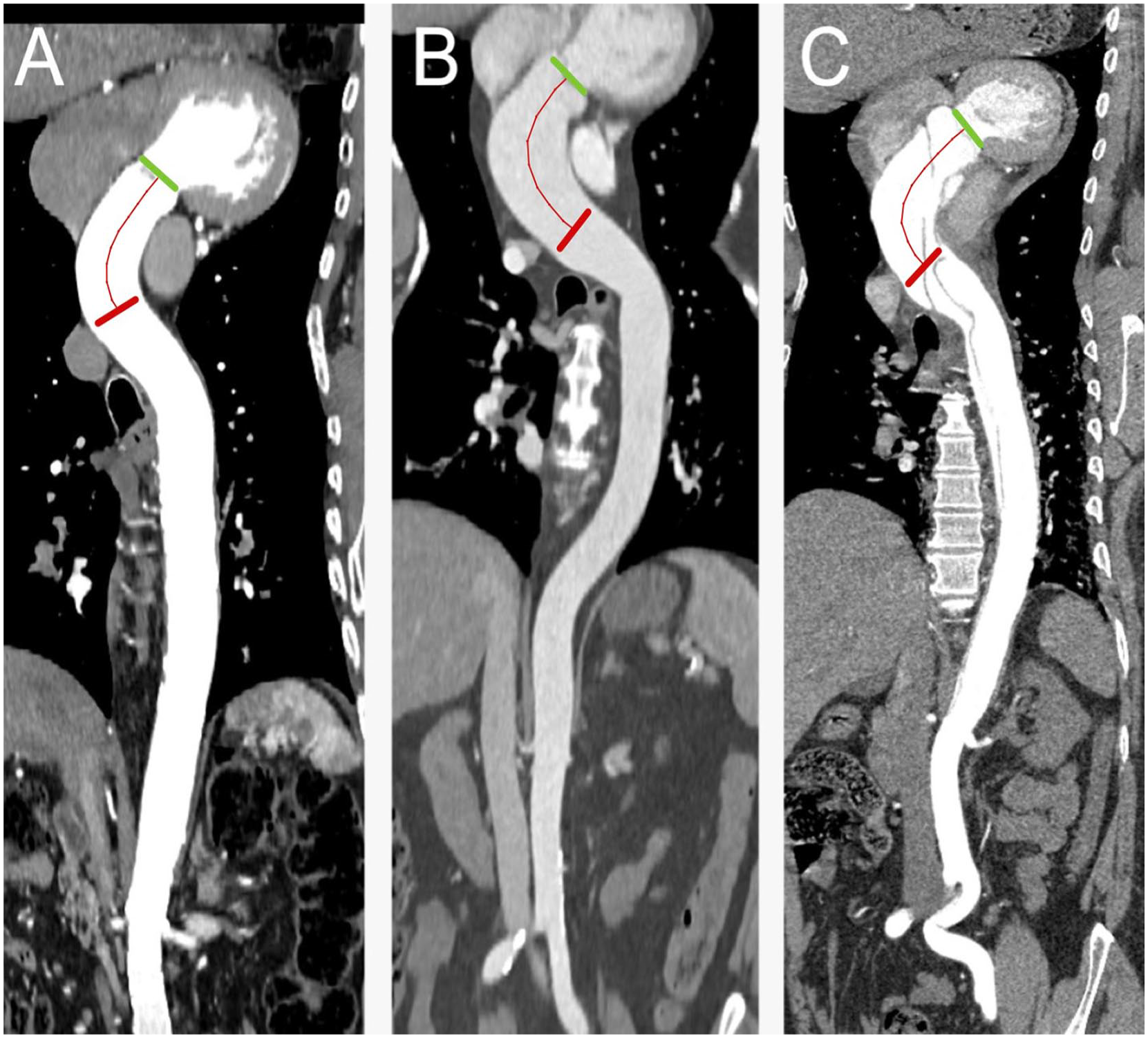
Observer 1 (T.K.) retrospectively performed the data acquisition of 102 dissection patients’ aortic diameters from the CTA images with the IDS7 (version 17.3.6; Sectra Imtec, Linköping, Sweden) diagnostic workstation. The diameters of the AA dilatation group and healthy controls were measured previously by Observer 3 (P.K.). In each group, the diameters of AA were measured according to the international recommendations4,9 by adjusting the measurement points at the outer vascular walls perpendicular to the center of the AA. The AA diameter was measured in two planes: in the sinus of Valsalva and in the middle AA. In the sinus of Valsalva, measurement was made in three different directions from sinus to sinus using multiplanar reconstruction (Fig. 1A). In the middle AA, two measures were taken perpendicular to each other in the direction of flow using multiplanar reconstruction (Fig. 1B). In both planes, only the largest diameter was registered.
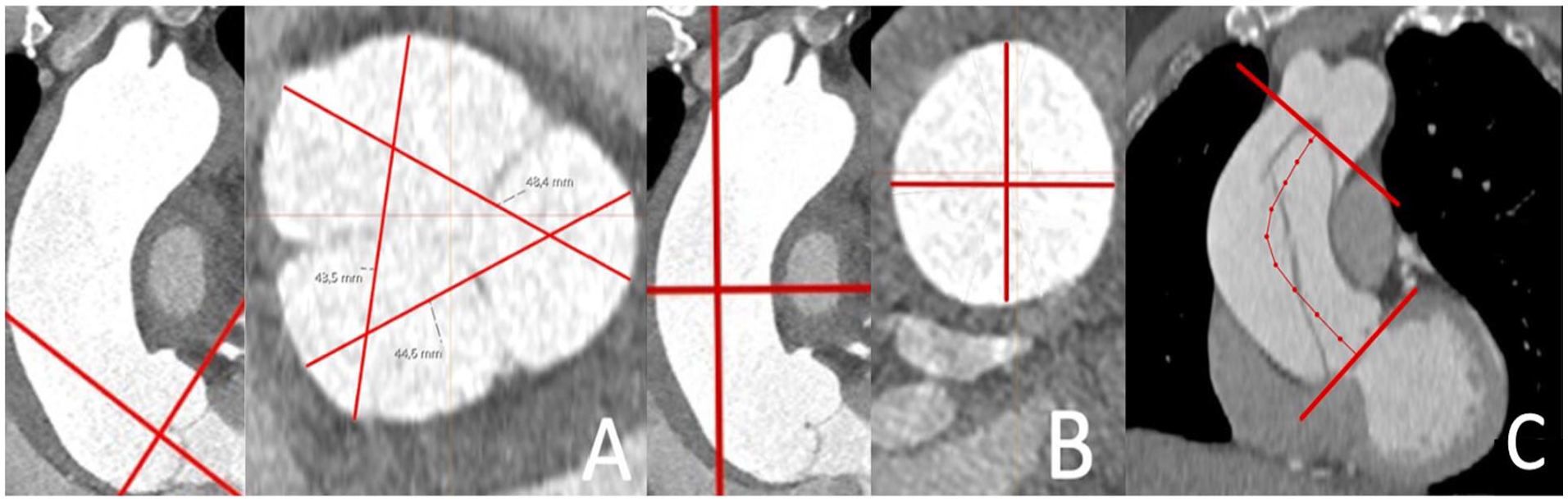
The diameters of the AA were measured from the sinus Valsalva (A) and middle-AA (B) planes. The starting points were placed on the outer vascular wall according to the ESC guidelines. 4 Three measurements were made in the sinus Valsalva and two in the middle AA, and the largest diameter was recorded. The AA length was defined in centerline as the distance between the aortic annulus and the origin of the brachiocephalic trunk (C).
AA length was determined in the centerline as the part of the vessel between the level of the aortic annulus and the origin of the brachiocephalic trunk (Fig. 1C) in the postprocessing diagnostic workstation (Syngo.via; Siemens, Erlangen, Germany). For the AA length measurement, an automated centerline of flow reconstruction was used, also for the dissection patients, and corrected manually if necessary.
Intra- and inter-observer analyses
To assess intra- and inter-observer reproducibility, the AA dimensions and length of the dissection population were measured twice by Observer 1 (T.K.) and by an independent Observer 2 (E.S.). For the AA dilatation group and healthy controls, reproducibility measurements were performed previously during a prior study by Observer 1 (T.K.) and Observer 3 (P.K.).
Statistical analyses
Statistical analyses were performed with IBM SPSS Statistics (version 27, Chicago, IL, USA). Statistical significance was defined as p < 0.05 and high significance as p < 0.001. Abnormally distributed parameters were presented as median and interquartile range and normally distributed parameters as mean ± standard deviation (SD).
The normality of the aortic dimensions and AA length was analyzed by drawing a histogram and visually assessing the distribution of the parameters in collaboration with a biostatistician. Statistical significances for normally distributed parameters were tested using an independent-samples T-test. To estimate statistical significances between the three groups, the chi-square test was used for class-scaled parameters and the Kruskal–Wallis test for continuous parameters.
Correlations between AA length and the patients’ height, weight, BSA, and aortic diameters were tested using the Pearson correlation test. The r-values were defined as 0.0–0.30 (negligible correlation), 0.30–0.50 (moderate correlation), and 0.50–1.0 (strong correlation). Parameters associated with AA length in univariate analysis were used to adjust a multivariable linear regression model for the AA length. To assess the correlations with class-scaled parameters and AA length, their means were compared.
The presence of a systematic error in the intra- and inter-observer analysis was tested with a paired samples t-test. Intra- and inter-observer reproducibilities were estimated using the intraclass correlation coefficient (ICC) with a two-way mixed-effects model and absolute agreement. The guideline designed by Koo et al. 10 was followed: under 0.50 (poor), between 0.50 and 0.75 (moderate), between 0.75 and 0.90 (good), and above 0.90 (excellent).
Results
Study population
The dissection cohort (n = 102) had the youngest mean age (63 ± 13 years), and the majority were male (n = 70, 69%). Approximately 63% of the dissection patients had a diagnosis of hypertension. Only three (3%) patients had BAV.
The mean age of the AA dilatation cohort (n = 134) was 69 ± 11 years, with mostly men (n = 101, 75%), and 56% were hypertensive. BAV was found in 11 (8%) patients.
The mean age of the healthy controls (n = 191) was 65 ± 16 years, and the majority were female (n = 109, 57%). Hypertension was noted in 52% of the patients, and four (2%) represented BAV.
There were no significant differences in cardiovascular risk factors (hypertension, diabetes, dyslipidemia, or smoking) between the groups (p > 0.05). Positive family history for CVD differed significantly (p = 0.002) within the groups and was most frequent in the aortic dissection group. In the entire study population, there were no diagnosis for connective tissue syndrome. The detailed patient characteristics are presented in Table 1.
Baseline characteristics of the study population.
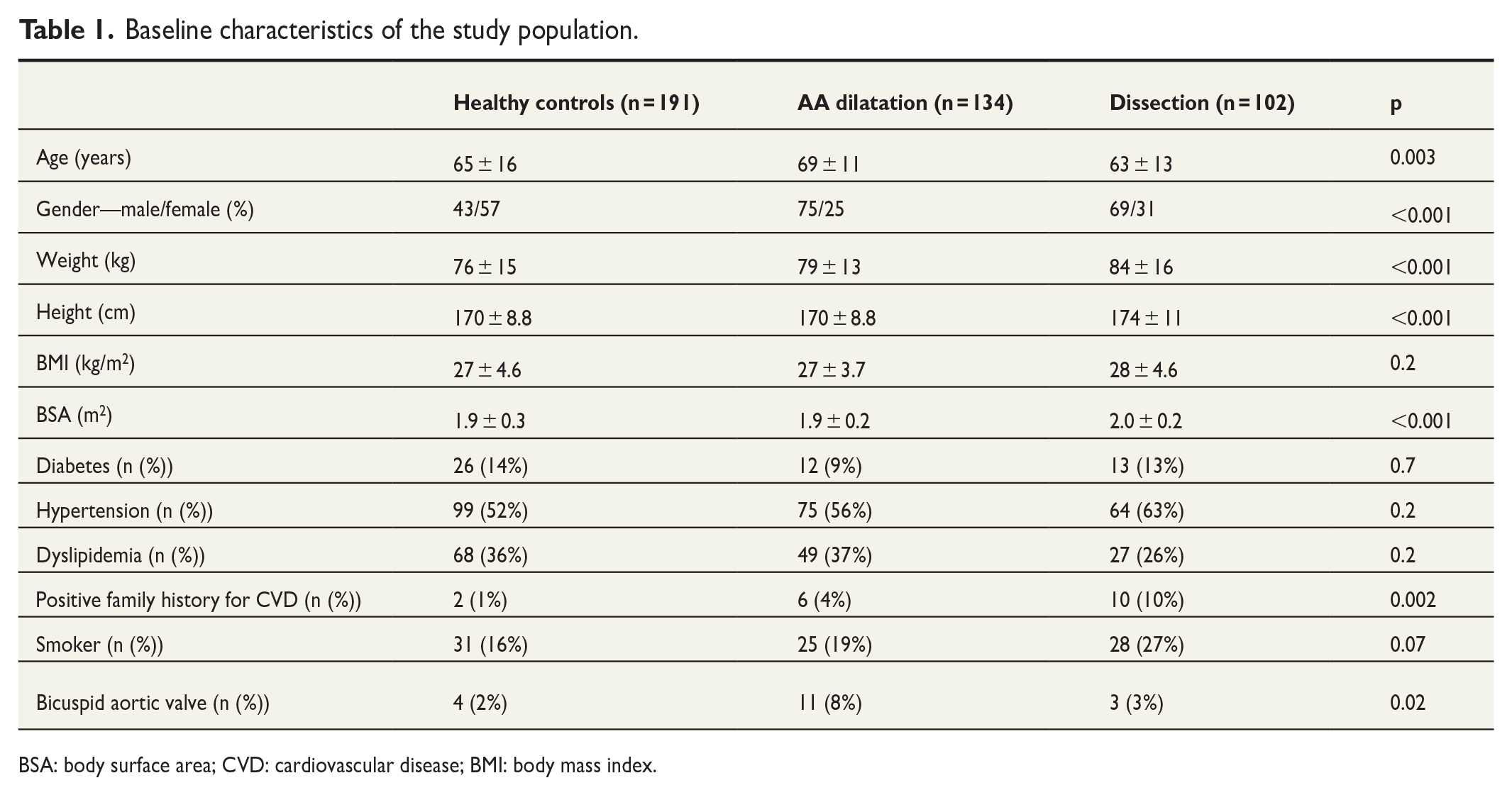
BSA: body surface area; CVD: cardiovascular disease; BMI: body mass index.
Aortic diameters in dissected and non-dissected aortas
In the healthy controls, the AA diameter was 36 ± 3 mm in the sinus of Valsalva plane and 34 ± 3 mm in the mid-AA plane. After establishing the mean largest diameter of the healthy controls, a diameter of 36 ± 3 mm was recorded.
In the dissection cohort, the diameters of the sinus Valsalva were similar compared to the AA dilatation cohort (44 ± 8 mm vs 43 ± 4 mm; p = 0.2). However, in the mid-AA plane, the diameters differed significantly (51 ± 10 mm vs 40 ± 6 mm; p < 0.001). When comparing the largest diameters between dissection and AA dilatation patients, the difference was significant (52 ± 10 mm vs 44 ± 4 mm; p < 0.001). The AA diameters in both dissection and AA dilatation patients were significantly larger than in the healthy controls (p < 0.001).
In the dissection group, 68 of 102 patients (67%) had the largest AA diameter < 55 mm. Thus, only 33% of the dissected aortas met the criterion for elective surgery. On the contrary, in the AA dilatation group, 5 of 134 patients (4%) had the largest diameter ⩾ 55 mm, with no signs of ATAAD.
Aortic length in dissected and non-dissected aortas
Both dissection and AA dilatation cohorts had significantly longer AAs compared to the healthy controls (p < 0.001). In addition, between the dissection and AA dilatation cohorts, the AA length differed significantly (110 ± 15 mm vs 97 ± 11 mm; p < 0.001). The mean AA length in the healthy controls was 83 ± 8 mm. Detailed AA dimensions, lengths, and ratios are presented in Table 2.
AA lengths, maximal diameters, and ratios between AA length and patient’s height, AA length and patient’s BSA, and AA maximal diameter and AA length.
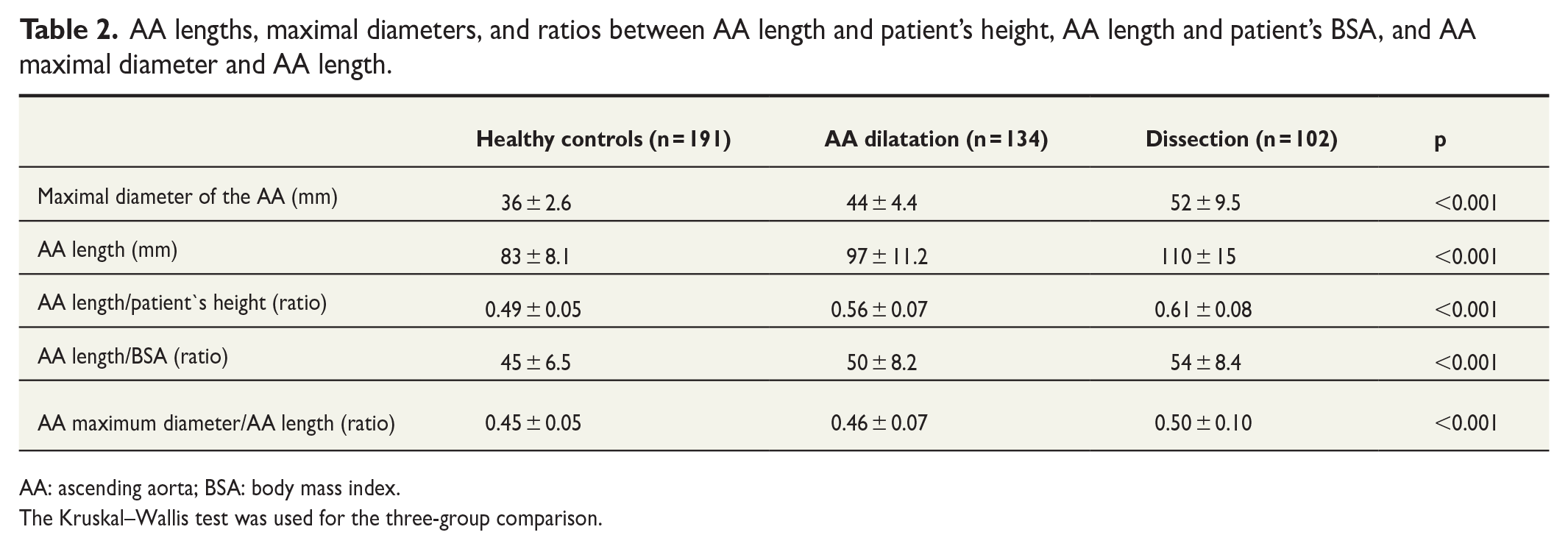
AA: ascending aorta; BSA: body mass index.
The Kruskal–Wallis test was used for the three-group comparison.
In the dissection cohort, 25/102 (25%) patients had a maximal AA diameter < 55 mm and AA length > 110 mm, whereas 16/102 (16%) patients had AA diameter > 55 mm and AA length > 110 mm. Hence, by combining 110 mm AA length and 55 mm diameter, 58% of the dissection patients would have been identified instead of using the AA diameter solely as a cut-off criterion based on which only 33% of the patients met the indication for elective surgery. In the healthy controls, none of the patients (0.0%) had an AA length > 110 mm, while in the AA dilatation group, only 17/134 (13%) had an AA length > 110 mm (Table 3).
Simultaneous prevalence of the AA length and diameter in each study group.
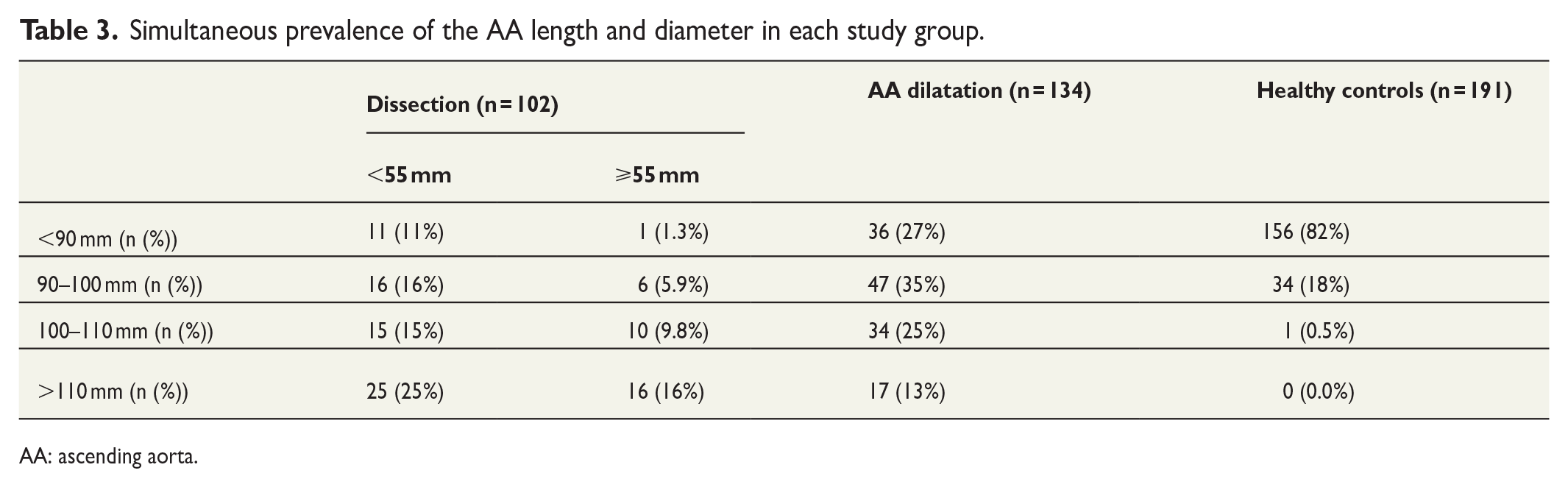
AA: ascending aorta.
Correlation between AA dimensions, length, and patients’ characteristics
The length of AA correlated moderately with the patients’ height (r = 0.36; p < 0.001). Correlations with patients’ weight (r = 0.16; p < 0.001), age (0.08; p = 0.09), and BSA (0.21; p < 0.001) were negligible. A strong correlation was detected between AA length and the diameter of sinus Valsalva (r = 0.69; p < 0.001) and mid-AA (r = 0.74; p < 0.001). The correlation between AA length and maximal diameter of the AA was also strong (0.64; p < 0.001). Correlation graphs are presented in Fig. 2.
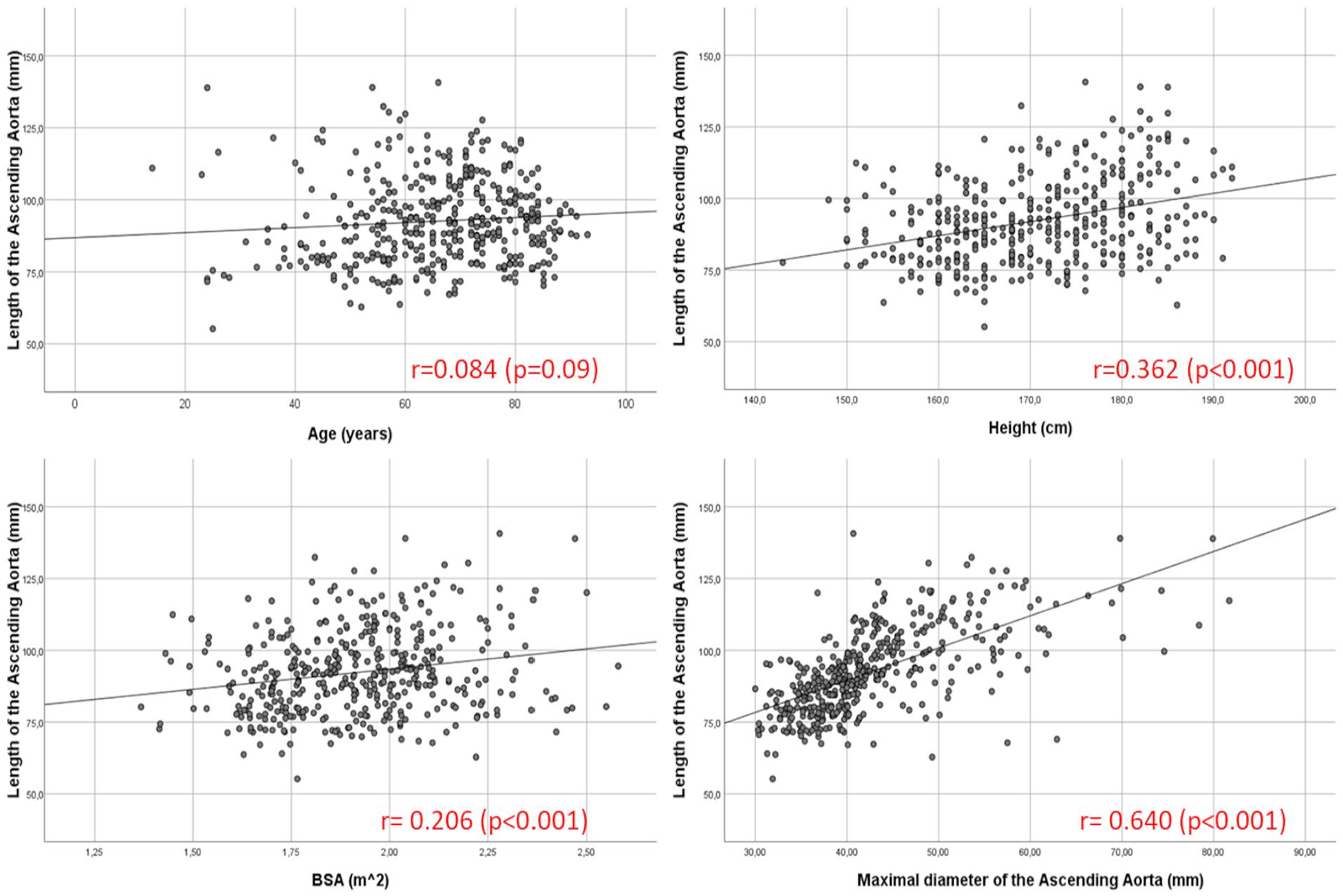
The relationships between AA length and patient’s age, height, BSA, and maximal diameter of the AA. The Pearson correlation test was used to assess the relationships.
In the entire study population, men had approximately 11 mm longer AAs than women (p < 0.001). In the dissection group, the mean length of the AA of men was 15 mm longer than that of women. Hypertensive patients had approximately 3 mm longer AAs in the entire population (p = 0.02). Diabetes, dyslipidemia, and smoking had no significant effect on AA length (p > 0.5).
Multivariable analysis
AA length was adjusted with patient-dependent factors that most strongly correlated with AA length. Adjustable factors included patients’ age, height, BSA, sex, and maximal diameter of AA. After adjustment, the length of the AA was 100 mm in the dissection group, 94 mm in the dilatation group, and 86 mm in the healthy controls. Thus, when comparing the adjusted AA length between the groups, the dissected aortas were 14 mm longer than in the healthy controls and 5 mm longer than in patients with dilated non-dissected aortas (p < 0.001). The dilated non-dissected aortas were 8 mm longer than in the healthy controls (p < 0.001). An illustrative image of healthy AA versus dilated AA versus dissected AA is shown in Fig. 3.
Illustrative image of healthy AA (A = 83 mm), dilated and non-dissected AA (B = 97 mm), and dissected AA (C = 113 mm). The AA length was defined in centerline as the distance between the aortic annulus and the origin of the brachiocephalic trunk in the diagnostic workstation (Syngo.via).
Intra- and inter-observer reproducibility
No systematic error was detected in the intra-observer measurements. Intra-observer reproducibilities were excellent in the sinus Valsalva (ICC = 0.99; p < 0.001), in the mid-AA (ICC = 0.99; p < 0.001), and in the AA length measurements (ICC = 0.98; p < 0.001) (Fig. 4).
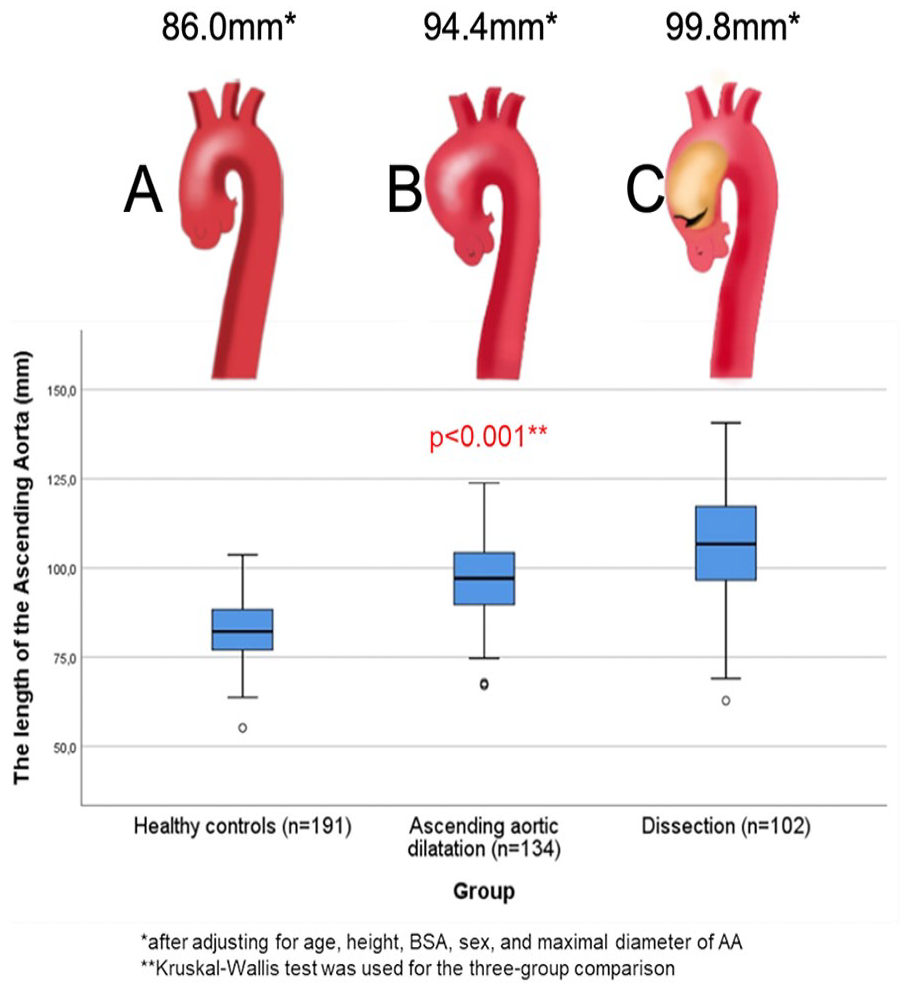
Central picture. The length of the ascending aorta associated with the risk of type A aortic dissection. The lower and upper borders of the box represent the lower and upper quartiles (25th percentile and 75th percentile). The middle horizontal line represents the median: (A) Healthy controls, (B) Dilated aortas (non-dissected), and (C) Dissected aortas
In the inter-observer measurements, a systematic error was detected in the measurements of the AA dimensions and length. However, ICC values were excellent in the AA length (ICC = 0.92; p < 0.001) and sinus Valsalva (ICC = 0.96; p < 0.001) measurements. In the mid-AA, ICC was good (ICC = 0.89; p < 0.001).
Discussion
Acute type A aortic dissection is a fatal complication of the geometrical expansion of AA. Currently, the only predictive factor for preventive surgery is AA diameter ⩾55 mm, which identifies only a small proportion of ATAAD patients.4,5 Therefore, new prognostic predictors are needed to schedule the prophylactic surgery at the right time. Previous studies have shown promising results regarding the utility of the ascending aorta length in the risk assessment of ATAAD, and we wanted to test this hypothesis with our own patient population. In our study, we found that when adjusting AA length to patient-dependent factors (age, height, BSA, sex, and maximal diameter of the AA), the patients with ATAAD had 14 mm longer AAs than the patients without aortic disease and 5 mm longer than patients with AA dilatation. Previously, Eliathamby et al. 11 found that adjusted AA length (age, sex, and AA diameter) was 8 mm longer in the dissection patients compared to the healthy controls and 2 mm longer compared to patients with AA aneurysm.
It has been described that aortic length increases as a part of the normal aging process. Adriaans et al. 12 found that the lifetime thoracic aortic elongation is approximately 59 mm in males and 66 mm in females and is mostly pronounced in the proximal descending aorta. With the consequence of aging, the amount of elastic content decreases, which leads to biomechanical dysfunction and increased stiffness of the aortic wall. These microstructural formations make the aortic wall vulnerable to geometrical changes in the horizontal and vertical directions.13,14 It is worth noting that in our study, increased age is not significantly associated with the risk of ATAAD (r = 0.08). However, due to the strong age-related elongation process and its impact on the risk of ATAAD in previous studies,7,12,15 we used age as an adjustable factor in the multivariable analysis model for AA length. In addition, except for positive family history, general cardiovascular risk factors (hypertension, dyslipidemia, diabetes, or smoking) had no association with the dissection event. Thus, our study is not in line with previous research in which the relationship between AA dilatation and adverse events and hypertension is shown. 16 Nevertheless, the minor role of the other CVD risk factors is in line with previous findings. 17 In the future, more detailed studies of the individual pathophysiological mechanisms in the aortic wall related to aortic elongation and the increasing risk of ATAAD are needed to clarify understanding.
In the moment of dissection, the AA diameter is shown to increase at a greater degree than the AA length. Previously, approximately 18% change in AA diameter was recorded, whereas AA length increased only by 2.7%. 18 A similar finding was observed in another study, in which AA length increased by 5.4%. 19 Our study is in line with this theory (Table 2), namely, the maximal AA diameter/AA length ratio increased during the dissection event. Dissections of patients’ aortas have rarely been imaged before dissection occurs. Hence, AA diameter and length are usually determined from post-dissection CTA images, and the results should be related to the pre-dissection dimensions. Therefore, given the greater increase in AA diameter compared to AA length, determining the cut-off limit for AA length can be assumed to be more reliable in post-dissection situations.
In the present study, only 33% of the dissected AAs had a diameter of 55 mm or more and, consequently, would have met the indication for prophylactic surgery. By combining 110 mm AA length and 55 mm diameter, 58% of the dissection patients would have been identified instead of using the AA diameter solely as a cut-off criterion based on which only 33% of the patients met the indication for elective surgery. These findings are in line with previous studies. Wu et al. 18 suggested that a 110-mm cut-off limit may be feasible in assessing the risk of ATAAD based on two hinge points (110–120 mm and 125–130 mm), in which complications of AA dilatation exhibit a strong increase in annual occurrence. Notably, in AA dilatation patients, 13% had AA length > 110 mm with no signs of ATAAD. It is impossible to predict the exact time in which the dilated AAs will be dissected/ruptured or whether they will reach the endpoint at all. Therefore, a small number of false positives should be taken into consideration, but the moderate sensitivity of > 110 mm length together with < 55 mm diameter may have potential for clinical use in the future.
The main limitation of our study was the lack of a pre-dissection group. However, as far as we are aware, the dissection event has a more significant effect on AA diameter than on AA length, as discussed previously. Hence, considering the change in aortic length during dissection is discretionary, in our opinion. To form a more reliable result for the AA lengths in different subgroups, we adjusted the AA length to the patient-dependent characteristics, which is effectively associated with increased AA length in our study. Nonetheless, some of the factors (hypertension, age) described in the literature to have a strong relationship with AA elongation did not show a significant correlation in the present study. Although we consider our adjusted model to be applicable based on prior similar kinds of results, the systematic error between the two independent observers may have been caused by a lack of routine in measuring AA dimensions. On the contrary, due to the varying quality of CTA images, a difference of a few millimeters at the measurement point can lead to an error. Our intention was to account for this measurement error and highlight it, but we have addressed it and found that the ICC values are excellent or at least good, despite the error. We reviewed this measurement error again with the research group’s expert, an imaging cardiologist, and concluded that there is always a small margin of error when interpreting CT images. 20 Therefore, considering the measurement accuracy, the error did not significantly affect the results or the differences between the groups, meaning the study’s conclusion remained coherent. We found excellent ICC values, so we conclude that this does not affect our conclusions. However, in the future, it is important to consider that if numerical thresholds are ever used for surgical decision-making, it would be beneficial to have repeat imaging and measurements from multiple imaging specialists.
To conclude, increased AA length seems to correlate with the risk of ATAAD. Increased AA length > 110 mm, alongside AA diameter > 40 mm, has a stronger predictive value than AA diameter alone in identifying patients at risk of ATAAD. Thus, AA length may be a relevant additional risk factor for ATAAD in the future. However, more studies in larger patient populations will be needed to prove this claim.
Footnotes
Acknowledgements
The authors acknowledge Helmiina Puupponen for central picture drawing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by personal fundings to T.K. from Finnish Cardiac Society and Finnish Cultural Foundation.
Clinical trial registration
The clinical trial registration number is 5101153.