
Abstract
Background and Aims:
Psoas muscle parameters estimated from computed tomography images, as surrogates for sarcopenia, have been found to be associated with post-interventional outcomes after a wide range of cardiovascular procedures. The pre-interventional assessment in patients undergoing invasive treatment for peripheral arterial disease is increasingly often carried out with magnetic resonance imaging (MRI), and we therefore sought to investigate the predictive potential of MRI-derived psoas muscle area in this cohort.
Methods:
A total of 899 patients with available sufficient quality pre-interventional MRI conducted within 6 months prior to treatment undergoing open, endovascular, or hybrid revascularization procedures for claudication and/or limb-threatening ischemia at Tampere University hospital between 2010 and 2020 were retrospectively studied in this single-center cohort study. The follow-up lasted until 17 June 2021. Psoas muscle areas were measured from the magnetic resonance images at the L4 level, and the reliability of muscle parameter measurements was tested with intraclass correlation coefficient analysis. The average psoas muscle area values (mean of left and right psoas surface areas) were z-scored and analyzed separately for men and women.
Results:
The median follow-up time was 5.9 years (interquartile range (IQR) = 2.7–7.8), and the overall mortality count was 259 (28.8%) (29.5% n = 168/569 for men and 27.6% n = 91/330 for women). The intraclass correlation coefficient analysis showed excellent interrater reliability for psoas muscle measurements. The muscle surface areas were larger in men (mean = 7.58 cm2) compared to women (mean = 5.27 cm2) (p < 0.001). Higher psoas muscle area was associated with better survival in women (p = 0.003, hazard ratio (HR) = 0.71, 95% confidence interval (CI) = 0.6–0.9 per 1 SD), whereas in men, an independent association of the muscle parameter with mortality was not found.
Conclusions:
MRI-derived psoas muscle area may be a prognostic factor for clinical use.
Keywords
Context and Relevance
This retrospective study found mean psoas muscle area at the L4 level measured with excellent interrater reliability from routine pre-interventional magnetic resonance angiography images to be independently associated with long-term survival in women undergoing invasive treatment for claudication or chronic limb-threatening ischemia, but a similar association was not ascertained in men. Future studies are needed to verify this finding, but it may help in further advancing the pre-interventional management of patients suffering from peripheral arterial disease as well as optimizing resource allocation.
Introduction
Individuals undergoing invasive procedures for peripheral arterial disease (PAD) represent a very-high-risk patient cohort. Up to 15% overall 5-year mortality rates have been reported in patients with asymptomatic PAD and claudication and up to 25% 1-year mortality rates in patients with chronic limb-threatening ischemia (CLTI).1,2 Corresponding 10-year all-cause mortality rates have been estimated at 63% and 75% for claudication and CLTI, respectively. 3 These high rates indicate that there is room for improvement in the treatment and risk-factor management of PAD patients undergoing invasive procedures.
While there are several factors known to be associated with post-interventional survival in PAD patients, investigating new prognostic indicators is crucial to help identify those patients who will benefit the most from invasive procedures, on the one hand, and to optimize risk factor management, on the other hand.4–8 The aging-related phenomena frailty and sarcopenia have recently gained great interest in pre-interventional risk assessment in a variety of fields and sarcopenia, defined as a progressive loss of skeletal muscle mass and function, has been found to be associated with increased mortality and cardiovascular events also in patients with PAD.9–11 Sarcopenia is influenced by factors such as genetics, hormones, nutrition, various diseases, and lack of muscle use. 12 Furthermore, muscle parameters are strongly associated with sex with males habitually presenting with larger muscle surface areas/volumes compared to women, but the association of sex with sarcopenia is more unclear.13–15 The presence of sarcopenia appears to differentiate patients with poor prognosis effectively, yet the potential sex-specific differences in the association of sarcopenia with mortality could be more clearly elucidated, since sex is associated with both post-interventional outcome and sarcopenia.14,15 Skeletal muscle parameters have been applied as markers of sarcopenia. Particularly, psoas muscle area (PMA) has been utilized in several studies where it has been independently associated with all-cause mortality after general and vascular surgery and, with post-interventional outcome, sarcopenia, grip strength, and frailty in cohorts including PAD patients.16–22
Previous research has mainly used computed tomography (CT) scans to assess psoas muscle parameters and, overall, the spatial resolution in CT images is better compared to magnetic resonance images (MRI). 23 However, MRI offers several benefits over CT in vascular surgical cohorts, such as lack of radiation exposure, no risk of impaired kidney function, and better visualization of the crural arteries, and as such, the use of MRI has increased in vascular surgery in the routine pre-interventional assessment of PAD patients, emphasizing the need to also investigate MRI-derived muscle parameters in these patients. Fitzpatrick et al. 24 recently studied the feasibility of MRI for iliopsoas muscle evaluation and found the measurements from MRI images to be both reliable and reproducible. The objective of this study was to evaluate the repeatability of PMA measurements estimated from routine pre-interventional MRI imaging and to assess the connection between the MRI-derived PMA and the sex-specific prognosis of PAD patients after invasive treatment.
Methods
Patients
Patients undergoing aorto-iliac and/or lower-limb revascularization procedures at Tampere University Hospital between 1 January 2010 and 27 November 2020 were retrospectively investigated. The symptomatic status of the study patients varied from claudication to CLTI. Elective, urgent, and emergency cases were included. MRI with a gadolinium-based contrast agent was the primary pre-interventional imaging method in use in the study with some exceptions related mainly to renal insufficiency, pacemakers, and/or previous stents or joint prostheses close to the areas of interest. The prerequisite for inclusion was sufficient quality MRI imaging encompassing the psoas area and taken a maximum of 6 months prior to the index procedure. A patient was accepted to the data only once, that is, the first procedure during the study period was considered as the index procedure and potential subsequent invasive vascular interventions as follow-up data. A total of 899 patients with sufficient quality magnetic resonance imaging within 6 months prior to the index procedure were identified. Out of 1359 patients treated invasively for PAD during the study period, a total of 899 patients had pre-interventional MRI imaging of sufficient quality within 6 months of the index procedure. The follow-up lasted until 17 July 2021. Median follow-up time was 5.9 years (interquartile range (IQR) = 2.7–7.8 years).
Information on age, body mass index, hypertension, diabetes, dyslipidemia, coronary artery disease, smoking (never/former/active), neurological events (transient ischemic attack (TIA)/stroke), pulmonary disease, renal insufficiency, and previous vascular interventions was gathered case by case from the patient records. In addition, data on medication, Fontaine classification, and Wound, Ischemia, and Foot Infection (WIfI) score were gathered. The WIfI class was determined according to the toe pressure if ankle brachial index and toe pressure failed to concur. 25 Data were retrieved from the medical case summary of the Uranus 8.4.6.35.3 CGI Suomi Oy, OMNI360 Kertomus 1.0.0.03E (2012) system of Tampere University Hospital patient registry, the PACS system of the TAYS radiological patient registry (Sectra Workstation IDS7 23.1.10.4570 (x64), Sectra AB), and the RIS system (radiology information system, Commit RIS Espoo, Finland). Mortality data was obtained from the patient registry into which it was continuously updated from the Finnish Population Information System.
Measurement of psoas muscle area
The MRI studies were performed with two scanners: Siemens Prisma 3T and Philips Ingenia Edition X 3T. The MRI sequence types and parameters were fl3D (TE = 0.97 ms, TR = 2.74 ms) and mDIXON (TE = 0.97 ms, TR = 2.74 ms), respectively. The voxel sizes were 1.3 mm × 1.3 mm × 1.3 mm and 1 mm × 1 mm × 2 mm, and the matrix dimensions 384 × 384 and 432 × 351. The acquisition plane was coronal, and the images were reformatted into axial plane where the measurements were performed. Since the most used levels for measuring PMA are the L3 and L4 levels and there appears to be no significant difference between these two, the L4 level was chosen for the purpose of the present study.18,26,27 Both thoracic and lumbar imaging was accepted, if the L4 level of the spine was shown in the image, and the psoas muscles were fully visible. PMAs were evaluated from the upper surface of the L4 vertebra of the spine and multiplanar reconstruction views were applied for the measurements (Fig. 1). The borders of the right and left psoas muscles were drawn with a free-hand tool and the PACS system applied for image viewing calculated the surface areas. Muscle measurements were carried out by the two main investigators (M.S., H.H.) after appropriate instructions and training with an experienced interventional radiologist (S.P.).
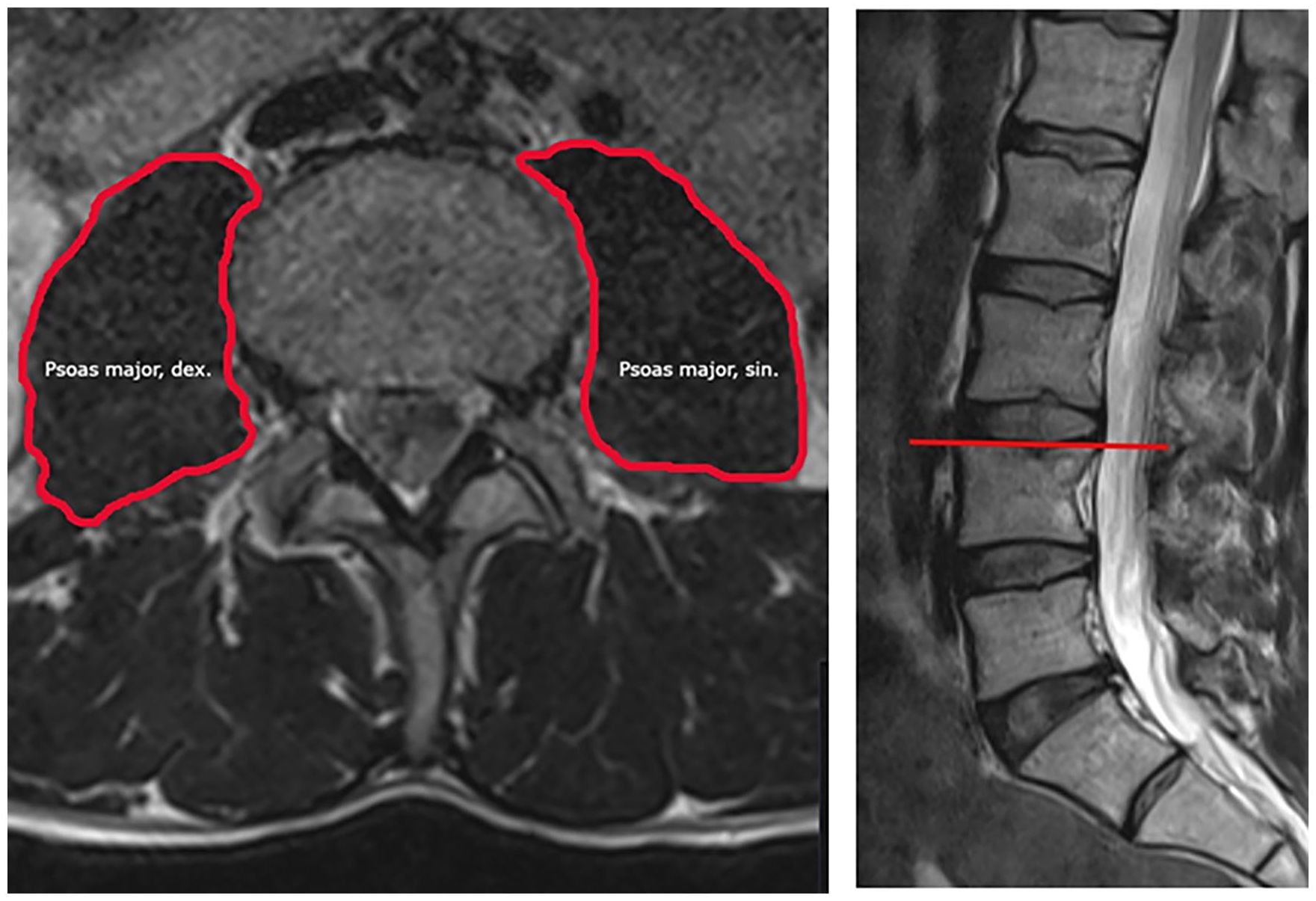
Representative image of the psoas muscle area measurement in magnetic resonance imaging.
Statistical analysis
Statistical analyses were executed with the IBM SPSS Statistics Data Editor 26 EN 64bit v100 edition for Windows. The normality of the variable distributions was visualized with histograms and investigated with the Kolmogorov–Smirnov test. Means and standard deviations were used for normally distributed variables and medians with interquartile ranges for non-parametric data. Mean/average PMAs were utilized for survival analysis, and they were calculated by adding together the area values on the right and left sides and dividing the result by 2. The mean PMA values for men and women were then z-scored and analyzed separately.
An intraclass correlation coefficient (ICC) analysis was performed as a Two-Way Random with SPSS to analyze the interrater reliability of measurements. Thirty patients were randomly selected, and their left and right PMAs were measured by an interventional radiologist. These values were then compared to the original measurements of the two investigators to ensure their reliability.
Survival was analyzed with Cox regression. Variables with a sufficient number of observations (> 95% available data for all subjects) were first evaluated in univariable analyses. Multivariable models were then constructed applying variables showing a possible significant association with survival (p < 0.100) in univariable models and filtering all non-significant variables by a backward stepwise selection (<0.05 threshold for inclusion). Survival analyses were carried out separately for men and women due to the very significant differences in many risk factor distributions and because sex interacted significantly with PMA in association with survival (p < 0.05 in simple interaction testing). Statistical significance was set at p < .050. In addition, the mean PMAs of men and women were compared using the Mann–Whitney U test. In order to draw a survival probability figure, the average PMA values were subsequently split into quartiles and these quartiles analyzed to determine the association of the muscle parameter with overall mortality. For this purpose, the lowest quartile was determined to indicate sarcopenia.
Ethical viewpoints
The study was conducted following the ethical principles of the Declaration of Helsinki. Approval was obtained from the Pirkanmaa Hospital District Science Center. Due to the retrospective nature of the study and lack of any interventions, investigations, or follow-up visits not included in the study center’s routine protocol, informed patient consent was waived.
Results
Patient characteristics
The study patients’ baseline characteristics, symptom severity, and operation types, as well as urgencies are presented (Table 1). The number of patients included in the study was 899, of which 569 (63.3%) were men and 330 (36.7%) were women. The median age of patients at the time of the procedure was 70 years (range = 38–93 years, IQR = 13).
Patient demographics and risk factors.
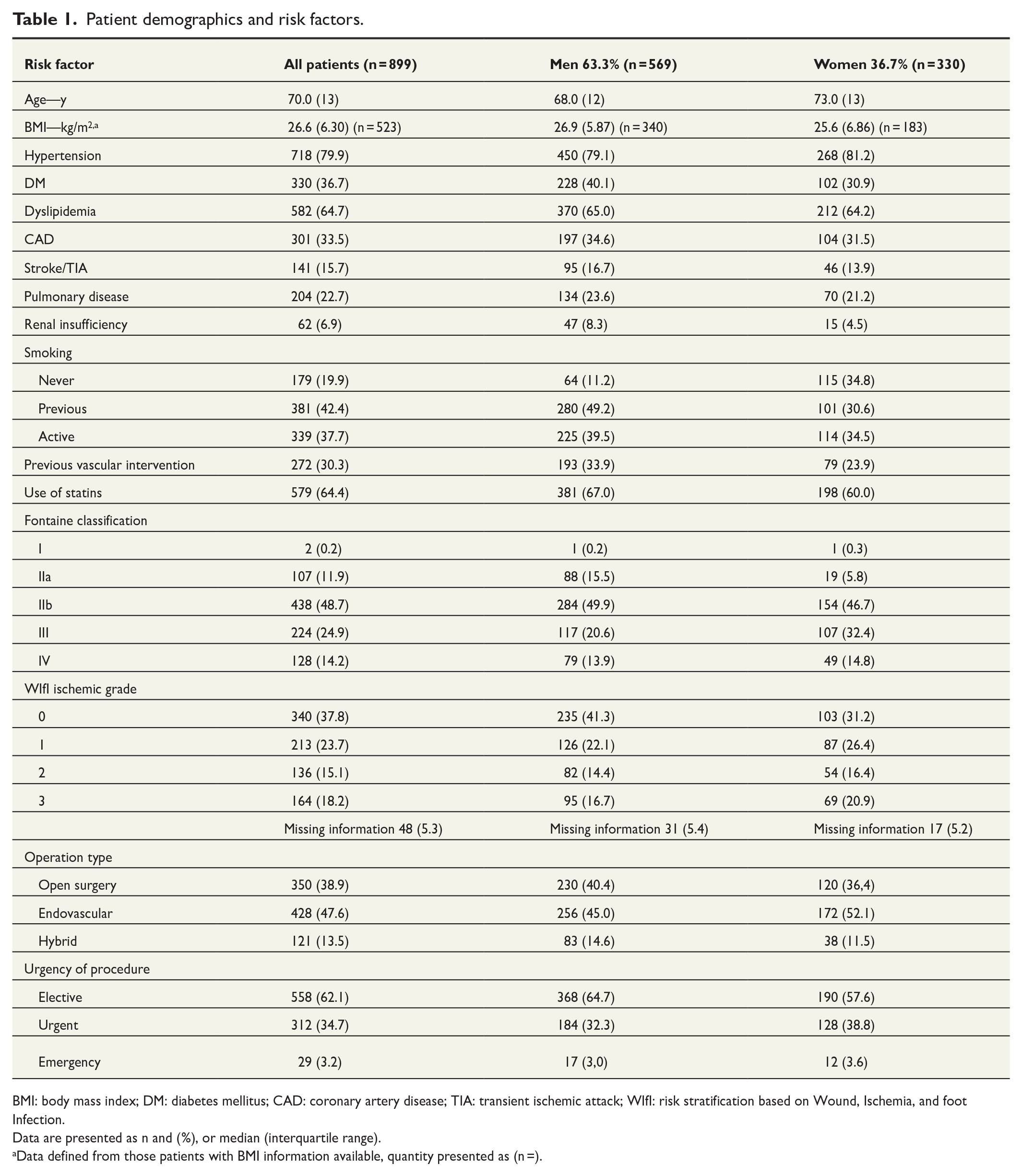
BMI: body mass index; DM: diabetes mellitus; CAD: coronary artery disease; TIA: transient ischemic attack; WIfI: risk stratification based on Wound, Ischemia, and foot Infection.
Data are presented as n and (%), or median (interquartile range).
Data defined from those patients with BMI information available, quantity presented as (n =).
ICC analysis
An ICC analysis of the PMA measurements carried out by three different parties was executed. The analysis ascertained the measurements to be coherent between the parties with a value of 0.978 for single measures and a value of 0.989 for average measures.
Psoas muscle area measurements
Table 2 displays the mean PMAs for the whole cohort and for men and women separately as well as mortality rates for all PMA quartiles. The psoas muscle surface areas were larger in men (mean = 7.6 cm2) compared to women (mean = 5.3 cm2) (p < 0.001).
Mortality by mean psoas muscle area quartiles.
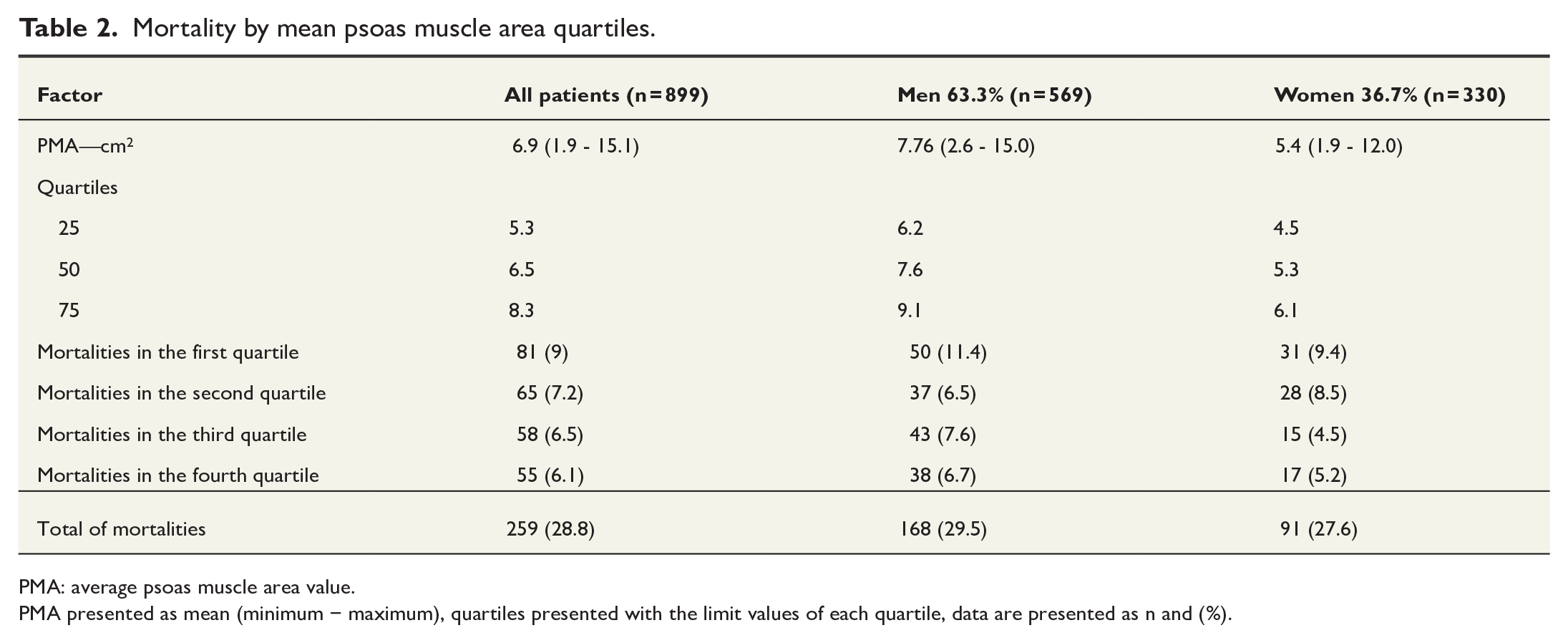
PMA: average psoas muscle area value.
PMA presented as mean (minimum − maximum), quartiles presented with the limit values of each quartile, data are presented as n and (%).
Survival
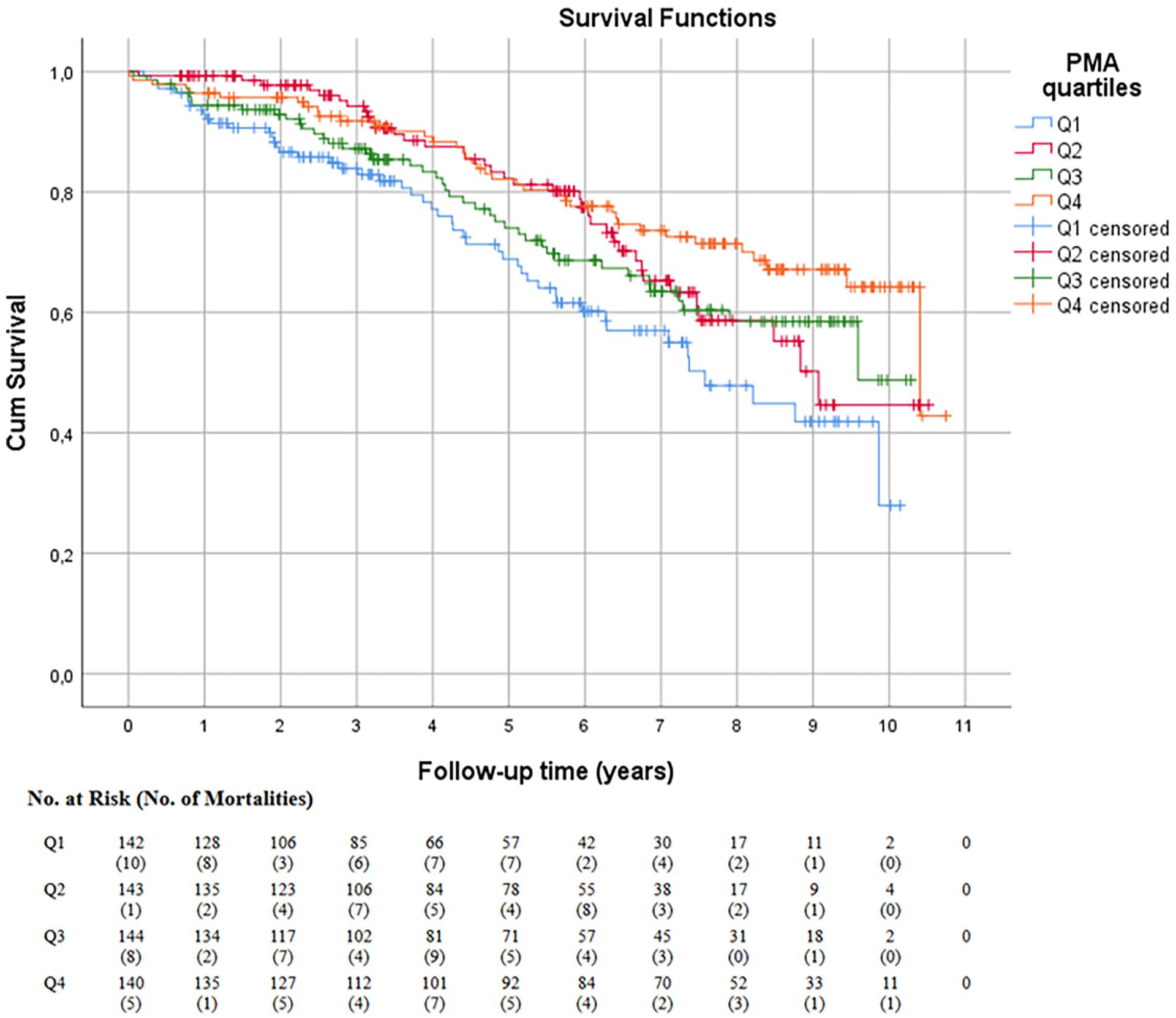
The overall long-term mortality rates for men and women were 29.5% (168 per 569) and 27.6% (91 per 330), respectively, and there was no statistically significant difference in mortality between the sexes. The long-term mortality rate for the whole cohort was 28.8% (n = 259). The median survival time was 5.4 years (3 days to 10.7 years) for men and 6.0 years (17 days to 11.0 years) for women. Fig. 2 presents the Kaplan–Meier curve for the whole cohort for the entire follow-up time demonstrating the post-interventional long-term mortality by PMA quartiles (log rank p = 0.003). We suggest the lower quartile to be considered a high-risk group. Fig. 3 presents the Kaplan–Meier curve for men and Fig. 4 for women, respectively. In the figures in question, greater PMA was associated with better survival (log rank p = 0.004 for men, p < 0.001 for women). The results of the univariable Cox regression analyses are presented in Table 3 and the multivariable analyses in Table 4. PMA was associated with lower mortality in both men and women in univariable analysis. However, the association persisted in multivariable analysis only in women (p = 0.003 for women, p = 0.572 for men).
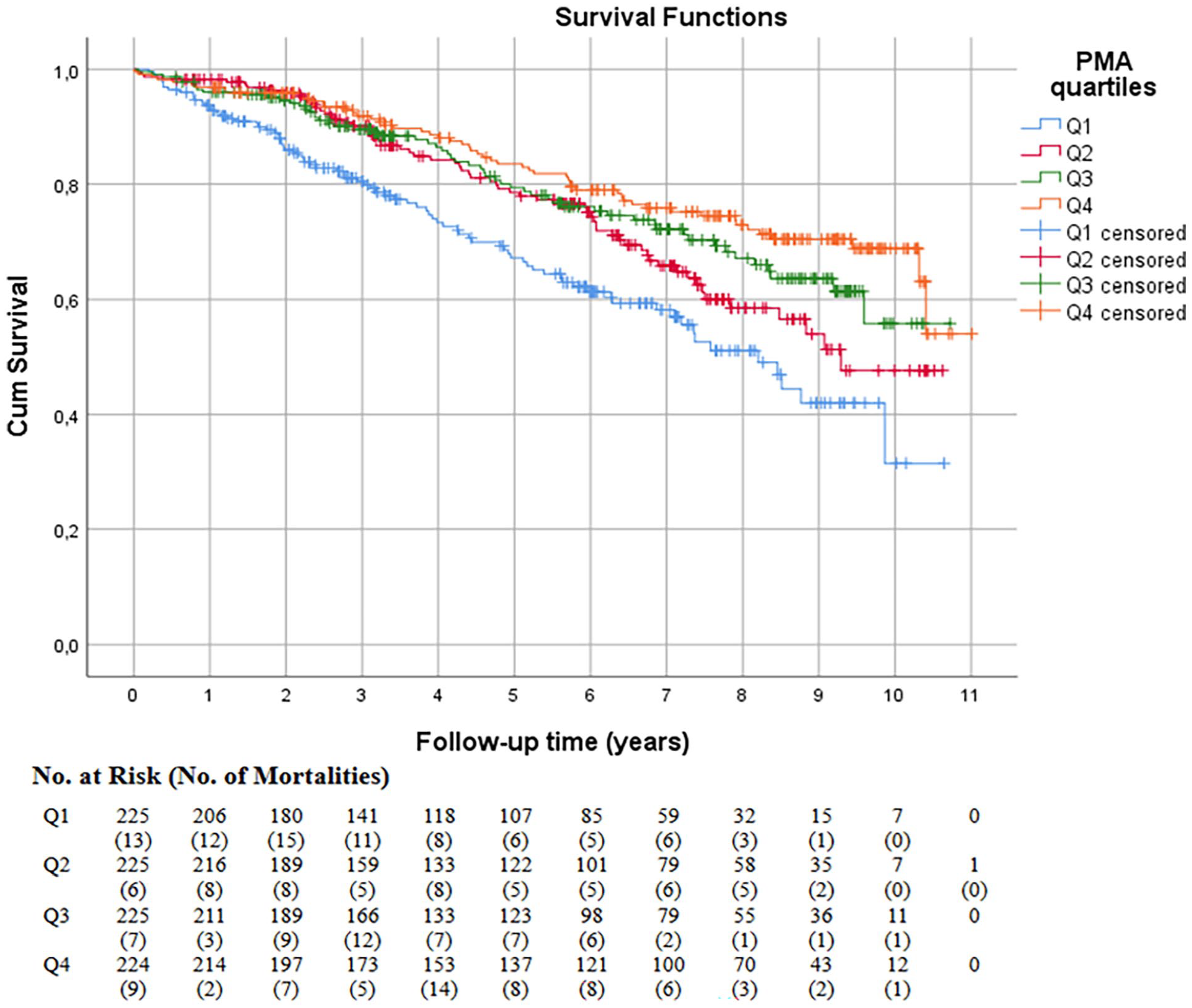
Survival probability within mean psoas muscle area quartiles (whole cohort).
Survival probability within mean psoas muscle area quartiles in men.
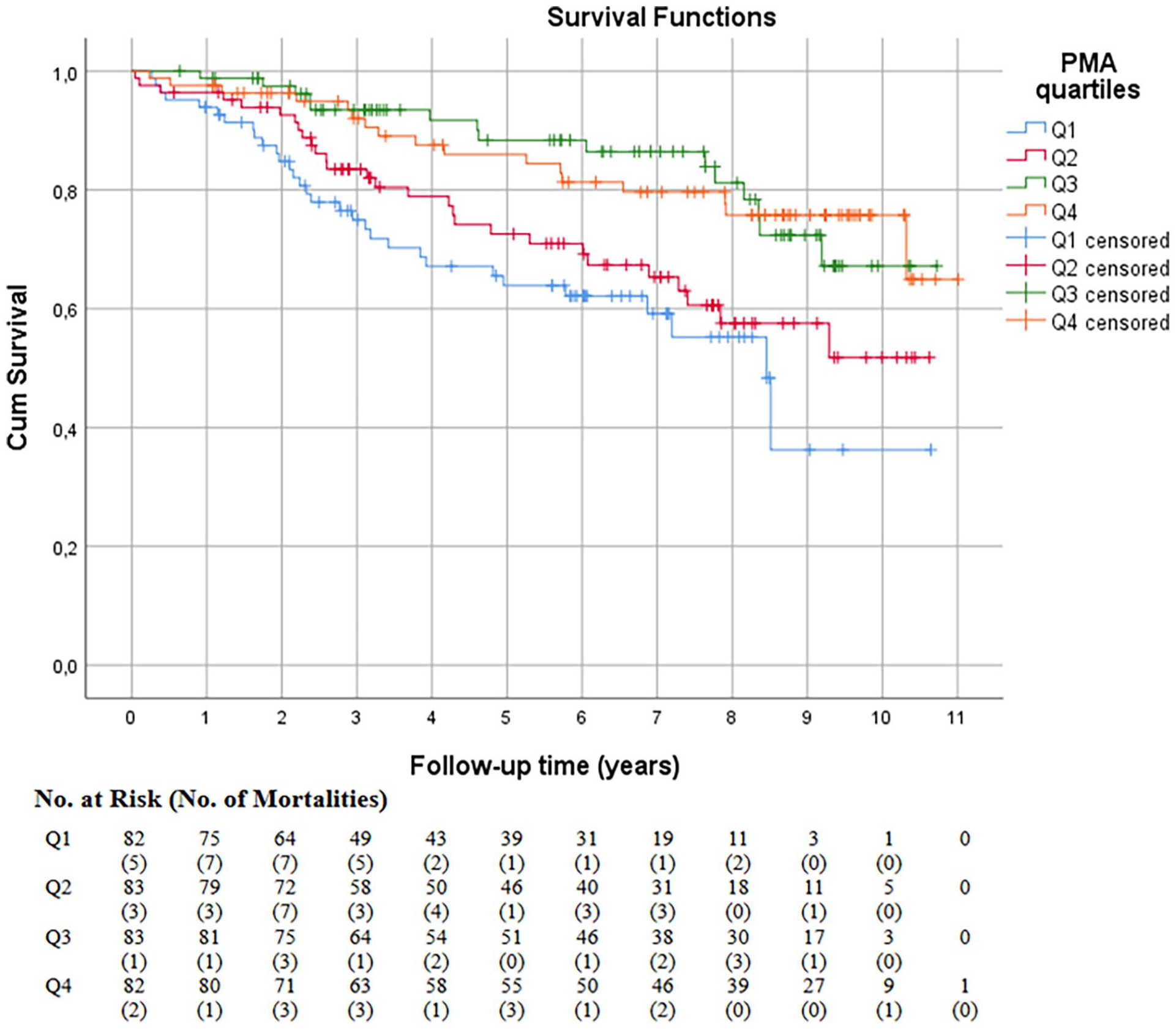
Survival probability within mean psoas muscle area quartiles in women.
Univariable Cox regression analysis of overall survival.
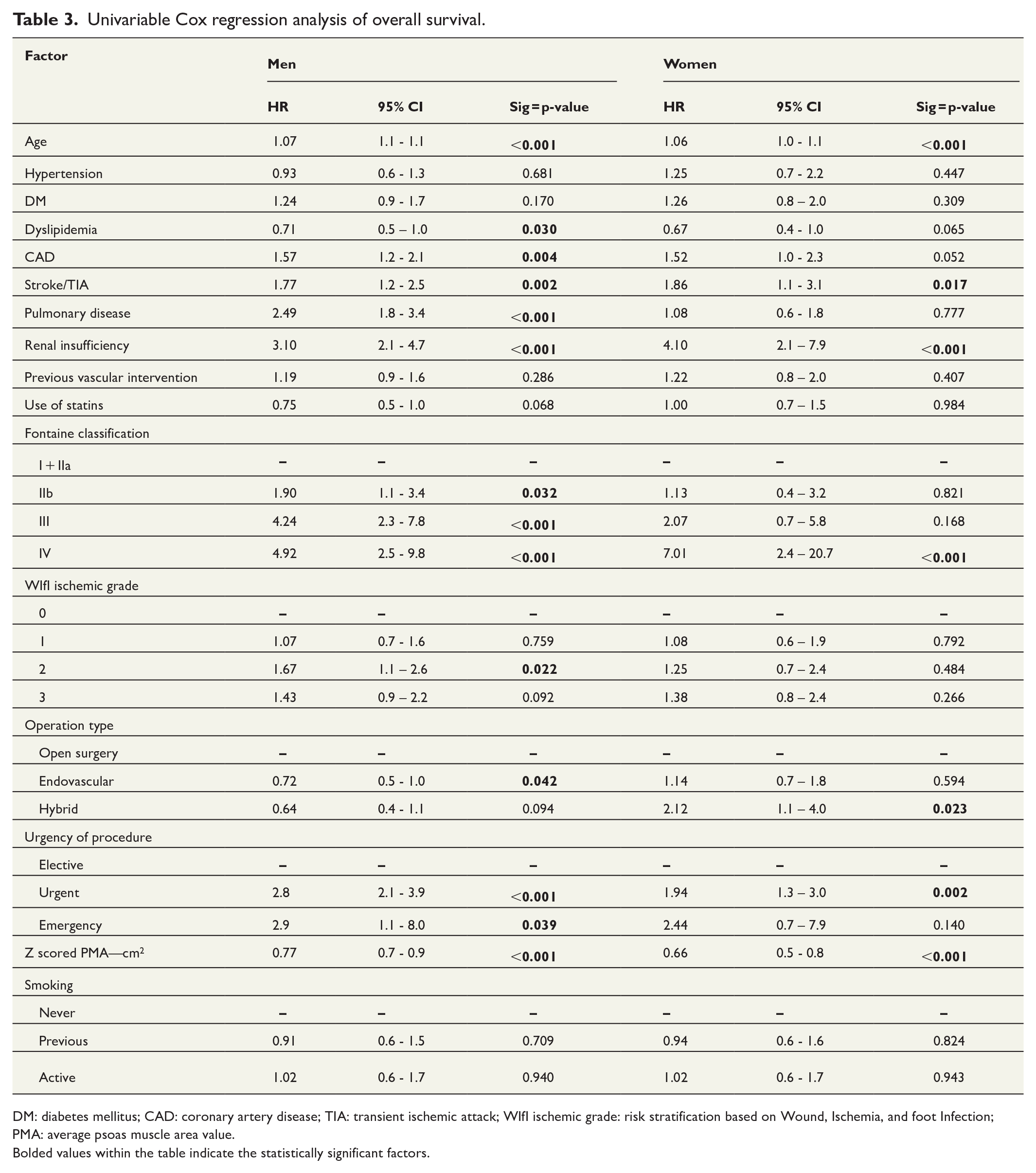
DM: diabetes mellitus; CAD: coronary artery disease; TIA: transient ischemic attack; WIfI ischemic grade: risk stratification based on Wound, Ischemia, and foot Infection; PMA: average psoas muscle area value.
Bolded values within the table indicate the statistically significant factors.
Multivariable Cox regression analysis of overall survival.
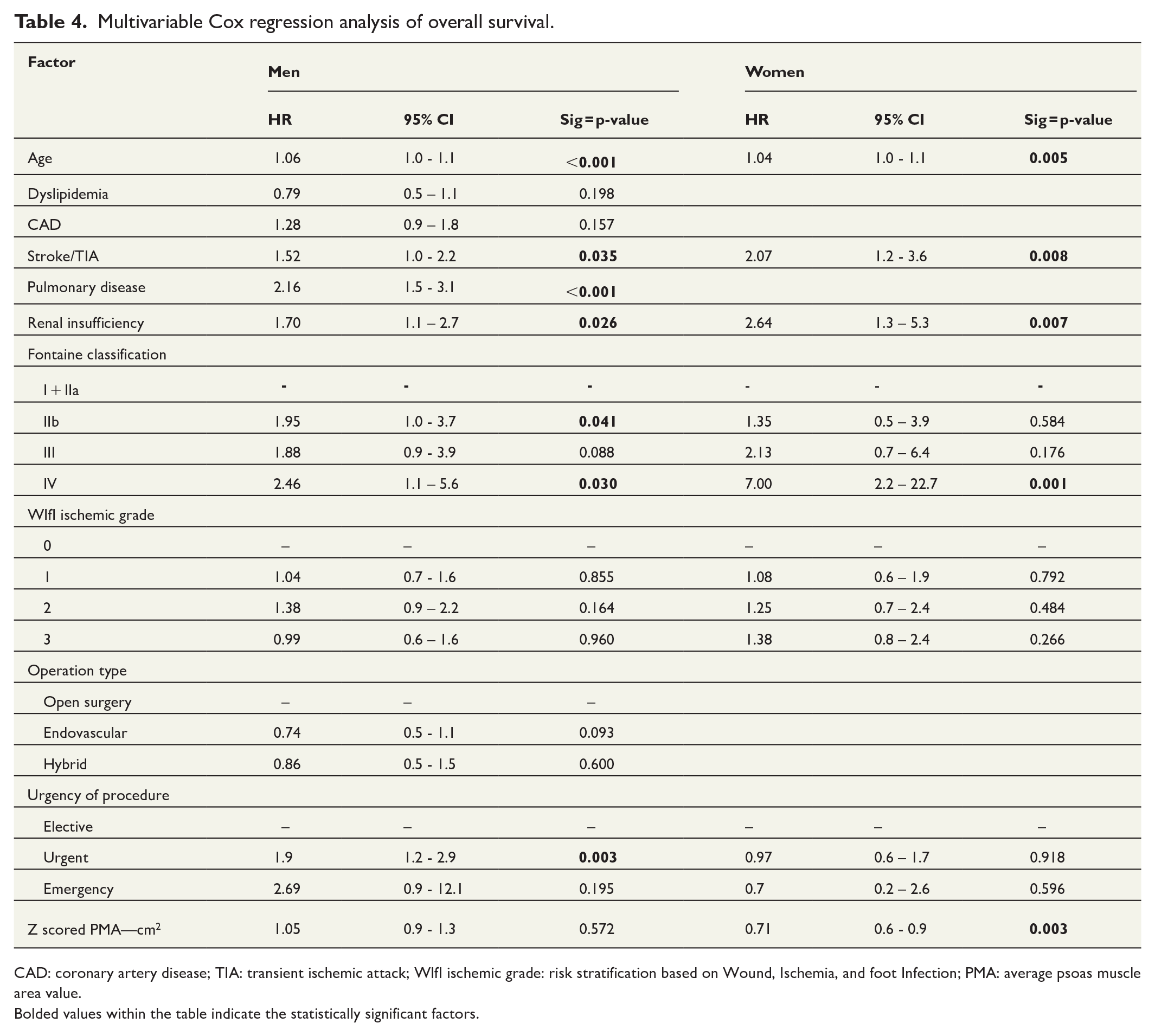
CAD: coronary artery disease; TIA: transient ischemic attack; WIfI ischemic grade: risk stratification based on Wound, Ischemia, and foot Infection; PMA: average psoas muscle area value.
Bolded values within the table indicate the statistically significant factors.
With regard to other risk factors in univariable analyses, age, coronary artery disease (CAD), previous stroke/TIA, pulmonary disease, and renal insufficiency were statistically significantly associated with increased mortality and, conversely, dyslipidemia with decreased mortality in men. In addition, Fontaine classification, WIfI grade, and operation type and urgency were also associated with survival. In women, age, previous stroke/TIA, and renal insufficiency were linked to higher mortality. Furthermore, Fontaine classification and operation type as well as urgency were linked to survival in women. In multivariable analyses, age, previous stroke/TIA, pulmonary disease, and renal insufficiency as well as Fontaine classes IIb and IV and urgent versus elective procedures were independently associated with increased mortality in men, but dyslipidemia and CAD no longer reached statistical significance. In women, age, previous stroke/TIA, and renal insufficiency along with Fontaine class IV were independently linked to mortality.
Discussion
In the present study, we retrospectively investigated the association of MRI-derived PMA and long-term survival in a cohort of 899 patients undergoing invasive revascularization procedures for aorto-iliac or lower-limb PAD. It was discovered that mean PMA at the L4 level could be measured with excellent reliability (ICC = 0.989, 95% CI = 0.98–1.0) from routine pre-interventional MRI images and it was independently associated with better long-term survival in women, but not in men. A 1 standard deviation increase in PMA in women corresponded to a HR of 0.78 (95% CI = 0.7–0.9).
Former studies have mainly used CT scans for muscle parameter evaluation, as CT imaging is accessible in many healthcare facilities. However, since MRI offers several benefits over CT (lack of radiation exposure, no risk of impaired renal function, better visualization of the crural arteries), MRI is also often applied in arterial imaging. The ability to utilize routine imaging studies for risk factor assessment in addition to procedure planning offers several benefits to the clinician, whereby investigating the feasibility of MRI-derived muscle parameters for prediction or mortality is of great value. The spatial resolution of CT images is higher compared to MRI, but Fitzpatrick et al. have recently ascertained that psoas muscles can be reliably estimated from MRI images as well.21,24 Our results from the ICC analysis concur with these findings. Studies directly comparing the two modalities in psoas muscle area assessment are scarce. Park et al. 28 found no significant difference in total psoas area measurements between CT and MRI in a cohort of healthy individuals evaluated with both imaging modalities for possible liver donation. However, the inter-reader agreement was better for CT compared to MRI. Furthermore, CT and MRI have been reported to be comparable in evaluation of abdominal skeletal muscle area in a small cohort of renal cell carcinoma patients. 29
The patient pool in the present study was fairly similar to previously presented cohorts of PAD and CLTI patients. Firstly, the majority of patients were male (63.3%).5,7,8,15,24 Secondly, the overall risk factor distribution resembled that of earlier studies.10,13,30,31 Thirdly, the female patients in our study were a median of 5 years older than the male patients, yet still had a better risk profile in comparison to male PAD patients with hypertension as the only underlying disease with a slightly higher incidence in women compared to men. 15
Muscle surface areas and volumes are usually larger in men compared to women, but the occurrence of sarcopenia in men versus women is less unambiguous. 13 While there is evidence to support that, overall, the prevalence of sarcopenia is similar in both sexes, 14 a study by Kirchengast et al. 15 found the incidence of sarcopenia to differ between men and women according to their age group. In the present study, the PMAs in women were significantly smaller than those in men aligning with earlier evidence.14,17,21 We found an increased PMA to be associated with improved survival in univariable analysis in both men and women. Furthermore, the Kaplan–Meier curves encompassing the whole cohort demonstrated a drop in long-term survival in the lowest PMA quartile at 3 years. We suggest the lower quartile to be considered a high-risk group, as the authors feel that it is not possible to definitively determine a threshold PMA value beyond which the mortality risk would increase significantly. However, in multivariable analyses, PMA independently predicted survival only in women. Previously, in a study by Juszczak et al., 22 total PMA measured at the L4 level independently predicted long-term survival in a 2-year follow-up in patients undergoing surgical lower-limb revascularization, with a HR of 1.89 (95% CI = 1.07–3.35; lowest sex-adjusted PMA quartile compared to other quartiles). The proportion of males in the study was 72.2% similarly as in other PMA-related studies published before. 22 A small study by Pereira-Neves et al. 30 in a predominantly (96.5%) male cohort of PAD patients undergoing endovascular and/or open revascularization for aortoiliac disease also found total PMA to be statistically significantly associated with survival as well as major adverse cardiovascular and cerebrovascular events. Our results are mainly in line with these findings notwithstanding the lack of an independent association of PMA with survival in men, the rationale for which remains unclear and warrants further investigation. Earlier studies have mainly investigated the relationship of PMA with survival in both men and women together or as a sex-adjusted factor not differentiating the results for each sex, thus leaving a gap in knowledge whether the studies published before align with our findings. It was recently ascertained in a large meta-analysis by Parvar et al. 31 that male and female PAD patients differ from each other and, furthermore, that there are significant sex-specific differences in the outcomes of PAD patients. Specifically, males present with greater mortality and major adverse cardiovascular event rates despite accounting for other sex-associated disparities. This underlines the need for further studies on the association of PMA with mortality in sex-based cohorts.
With regard to other risk factors, previous studies have found age over 80 years, male sex, CAD, chronic kidney disease, chronic heart failure, prior strokes or myocardial infarctions, major limb amputations, smoking, the degree of claudication, and lower limb ulcers to be associated with worse post-interventional survival in PAD patients undergoing invasive treatment.4,6–8 Conversely, female sex, hypertension, dyslipidemia, and diabetes have been linked to better survival. 7 In the present study, a history of previous TIA or stroke persisted as an independent risk factor for mortality in both men and women, which is in line with earlier evidence. 5 Cerebrovascular disease in PAD patients, in practice, indicates presence of vascular disease in multiple vascular beds, which is a particularly high-risk condition. Furthermore, renal insufficiency and Fontaine class were independently associated with mortality in both sexes also concurring with previous findings.22,32
The present study has some limitations related mostly to its retrospective nature. For the majority of the study period, MRI was not carried out for individuals with significantly impaired renal function (glomerular filtration rate < 30 mL/min) nor for those with pacemakers whereby these patients are likely to be underrepresented in this cohort.33,34 Furthermore, CT may have been favored over MRI in patients with joint prostheses close to the areas of interest and/or previous vascular stents due to image artifacts caused by these materials in MRI. In addition, in acute cases, CT imaging is likely to have been more readily available. Consequently, there is likely to be some selection bias. However, the authors feel that the cohort quite accurately represents patients studied with MRI prior to revascularization. Other limitations include the lack of data regarding the weight and height of the patients, the specific distribution of atherosclerotic lesions, which can have influenced PMA, and potential secondary procedures as well as the causes of death.
The present study suggests that PMA measured from routine pre-interventional MRI images may be a considerable prognostic factor for clinical use, at least in women. A practical implication for the findings of the present study could be use of MRI-derived muscle areas as a part of the pre-interventional assessment, particularly in borderline cases, where it is difficult to discern the suitability for and benefit from invasive procedures. The information may also be used to develop nutrition and/or exercise programs to potentially improve the prognosis of PAD patients undergoing invasive treatment. More research is, however, needed to investigate whether the role of muscle area and mass differs in men and women and within different subgroups of PAD patients. In addition, it is worthwhile addressing whether MRI-derived PMA is also associated with other frailty/sarcopenia assessment tools as well as significant outcomes such as limb salvage and major adverse cardiovascular events in PAD patients undergoing invasive procedures.
Footnotes
Acknowledgements
We thank docent Niko Sillanpää (MD, PhD) for providing the precise technical information of the MR images and the overall information of the MR scanners.
Author contributions
Minea Söderlund, BM: Conception and Design, Analysis and Interpretation, Data Collection, Writing the Manuscript, Critical Revision, Approval of the Manuscript, Agreement to be Accountable, Statistical Analysis.
Henni Huhtamo, BM: Analysis and Interpretation, Data Collection, Approval of the Manuscript, Agreement to be Accountable, Statistical Analysis.
Sara Protto, MD, PhD: Analysis and Interpretation, Data Collection, Writing the Manuscript, Critical Revision, Approval of the Manuscript, Agreement to be Accountable, Statistical Analysis.
Jussi A. Hernesniemi, MD, PhD: Conception and Design, Analysis and Interpretation, Writing the Manuscript, Critical Revision, Approval of the Manuscript, Agreement to be Accountable, Statistical Analysis.
Niku Oksala, MD, PhD, DSc: Conception and Design, Analysis and Interpretation, Writing the Manuscript, Critical Revision, Approval of the Manuscript, Agreement to be Accountable, Obtaining Funding, General Supervision.
Damir Vakhitov, MD, PhD: Data Collection, Critical Revision, Approval of the Manuscript, Agreement to be Accountable, Statistical Analysis.
Niina Khan, MD, PhD: Conception and Design, Analysis and Interpretation, Writing the Manuscript, Critical Revision, Approval of the Manuscript, Agreement to be Accountable, General Supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was funded by the Pirkanmaa Hospital District (9AB052).