
Abstract
Background and aims:
There is a paucity of data on later healthcare visits and retreatments after primary treatment of spontaneous pneumothorax. The main purpose of this study was to describe retreatment rates up to 5 years after primary spontaneous pneumothorax treated with either surgery or tube thoracostomy (TT) at index hospitalization in Finland between 2005 and 2018 to estimate the burden of primary spontaneous pneumothorax on the healthcare system.
Methods:
Retrospective registry-based study of patients with primary spontaneous pneumothorax treated with TT or surgery in Finland in 2005–2018. Rehospitalization and retreatment for recurrent pneumothorax and complications attributable to initial treatment were identified.
Results:
The total study population was 1594 patients. At 5 years, 53.2% (384/722) of TT treated and 33.8% (295/872) of surgically treated patients had undergone any retreatment. Surgery was associated with a lower risk of recurrence than TT (hazard ratio (HR) 0.50, 95% confidence interval (CI) 0.43–0.56, p < 0.001). Male sex was associated with a lower risk of recurrent treatment (HR 0.75, 95% CI 0.63–0.90, p = 0.001). Higher age decreased the risk of recurrent treatment (HR 0.99, 95% CI 0.99–0.99, p < 0.001). At 5 years, 36.0% (260/722) of the TT treated and 18.8% (164/872) of the surgically treated had undergone reoperation at some point.
Conclusions:
Reintervention rates and repeat hospital visits after TT and surgery were surprisingly high at long-term follow-up. Occurrences of retreatment and reoperation were significantly higher among primary spontaneous pneumothorax patients treated with TT at index hospitalization than among patients treated with surgery.
Context and Relevance
Reintervention rates and repeat hospital visits after tube thoracostomy and surgery were surprisingly high at long-term follow-up. Occurrences of retreatment and reoperation were significantly higher among primary spontaneous pneumothorax patients treated with tube thoracostomy at index hospitalization than among patients treated with surgery. Our findings are in line with previous observations, but the study demonstrates a considerable number of retreatments and repeat visits. The high overall rate of recurrent treatment with either modality, coupled with the well-documented good results of conservative treatment, calls for a critical evaluation of treatment and follow-up protocols especially for uncomplicated primary spontaneous pneumothoraxes.
Introduction
Spontaneous pneumothoraxes can be divided into primary and secondary. Primary or idiopathic pneumothoraxes are believed to be caused by the rupture of small, dilated bullae usually located apically in the lung. The etiology of the bullae remains unknown.1,2 Spontaneous pneumothorax is most common among tall, thin, male smokers aged 20–40 years.1,3,4 Treatment of pneumothoraxes is routine in hospitals and emergency departments and canalization of the pleural cavity is the most common invasive thoracic procedure.
There is an ongoing debate about the optimal treatment of spontaneous pneumothoraxes. Small pneumothoraxes with under 15% of lung volume (<2 cm of visible air rim between the lung margin and the chest wall) are often treated with observation, while large pneumothoraxes of over 15% of volume (>2 cm of visible air rim between the lung margin and the chest wall) are treated in many centers primarily with tube thoracostomy (TT) until the air leak has stopped and the lung is expanded. The symptoms also affect the choice of treatment method. If the spontaneous pneumothorax recurs after TT treatment or does not respond to it, surgical treatment is considered. Patients with a pneumothorax and contraindications for surgical treatment can be treated with pleurodesis in conjunction with TT.5,6
There is a lack of consensus on the optimal primary treatment of spontaneous pneumothorax. In order to identify the optimal treatment from both the patient perspective and the health care resource use, it would be useful to know the recurrence rates and potential prognostic factors. The aim of this study was to describe reintervention and retreatment rates in patients managed invasively at index hospitalization.
Methods
This was a retrospective, registry-based study. Subjects were identified from the Care Register for Healthcare in Finland (CRHF), a nationwide registry of data on all hospital admissions and major interventional procedures in the country.7 Patients were identified from the registry by diagnosis codes (ICD-10 codes J93.0 and J93.1) and procedural codes (NOMESCO codes GAA10, GA4AT, GA4BT, GA4CT, and GA4YT for TT and other G-codes for surgical treatment). Secondary spontaneous pneumothoraxes were excluded by diagnosis codes. Although the procedural codes for surgery were available in the data, the exact extent of, for example, pleurectomy cannot be evaluated based on codes only. Consequently, the procedural coding was not included as a variable. The procedures were implemented in the years 2005–2018 in patients over 16 years. The study flow chart is presented in Fig. 1.
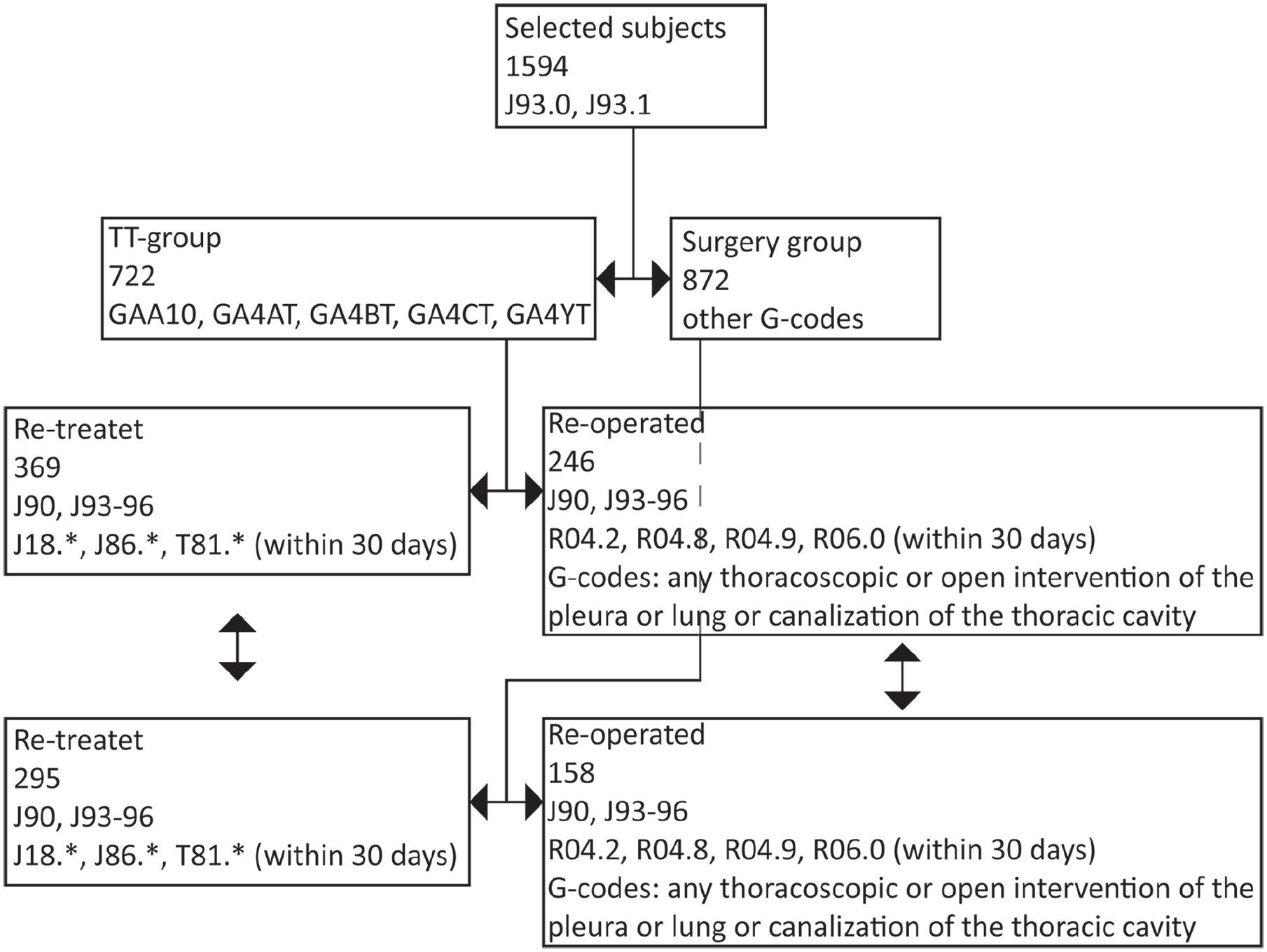
The study flow chart.
The primary outcome was retreatment within 5 years among those whose primary treatment was TT or surgery during the first treatment episode. According to general practice, almost every surgically treated patient was first treated with TT before they ended up with surgical treatment. Grouping between patients was done based on whether or not surgery was performed at index hospitalization. The primary outcome was retreatment defined as either reintervention or an inpatient or outpatient hospitalization for pneumothorax or postprocedural sequelae. Retreatment episodes were identified by diagnosis codes (ICD-10 codes J90 and J93–J96). If there was a retreatment episode within 30 days after the primary procedure with diagnosis codes J18*, J86*, or T81* (e.g., complications such as respiratory infection or empyema, postoperative bleeding), they were also included as retreatment episodes for sequelae if on an in- or outpatient visit separate from the index hospitalization.
The secondary outcome was the reoperation rate within 5 years in the TT and surgically treated groups. Reoperations were identified by diagnosis codes (ICD-10 codes J90 and J93–J96) and procedural codes (any thoracoscopic or open intervention of the pleura or lung or canalization of the thoracic cavity). If there was a reoperation within 30 days after the primary procedure with diagnosis codes for airway bleeding or dyspnea (R04.2, R04.8, R04.9, or R06.0), they were also included. Follow-up was at a minimum of 1 year and ended no later than December 31, 2019. The Charlson Comorbidity Index (CCI) was calculated using a combination of available registries as described below. 8
The data from the CRHF, Finnish Cancer Registry, and Reimbursement Registry of Prescription Medication Data were obtained from the Finnish Institute for Health and Welfare (Findata; permission THL/164/14.02.00/2021) and the mortality data from Statistics Finland (permission TK-53-484-20). 9 As this was a retrospective register study, the requirement for informed consent was waived, and the study patients were not contacted.
Outcomes were studied with the Kaplan-Meier estimator and Cox proportional hazards regression analysis. The subjects were censored on death. Statistically significant variables from the univariable analysis were entered into a Cox proportional hazards regression model to identify predictors of retreatment. The results are given as the mean for normally distributed variables, median in case distribution is not normal, percentage, or hazard ratio (HR) with 95% confidence interval (CI), interquartile range (IQR), or ±standard deviation (SD). P-values of <0.05 were considered statistically significant. SPSS for Mac version 26 (IBM, Armonk, NY, USA) was used for the analyses.
Results
Baseline characteristics
The final patient population available for outcome analyses was 1594, with 722 patients in the TT group and 872 in the surgery group. The mean age was 37.9 years (SD 18.9, max. 97), 77.6% of the population were male, and people over 70 years of age comprised 8.6% of the population. The CCI score was 0 in 89.6% of the patients, 1 in 6.4%, and 2 or more in 4%. The highest CCI score was 7 (in two patients). The median follow-up time with TT-treated patients was 2.3 years (IQR 0.1–7.3) and with surgically treated patients 4.1 years (IQR 0.9–8.8).
Primary outcome
Freedom from re-retreatment after TT or surgery is shown in Fig. 2. Within 90 days, 27.5% (438/1594) of the whole population needed retreatment for pneumothorax. At 5 years, the rate was 42.3% (674/1594). The majority of treated recurrences occurred within the first year, after which the incidence declined. Overall, at 5 years, 53.2% (384/722) of the TT treated and 33.8% (295/872) of the surgically treated patients had undergone some kind of retreatment episode.
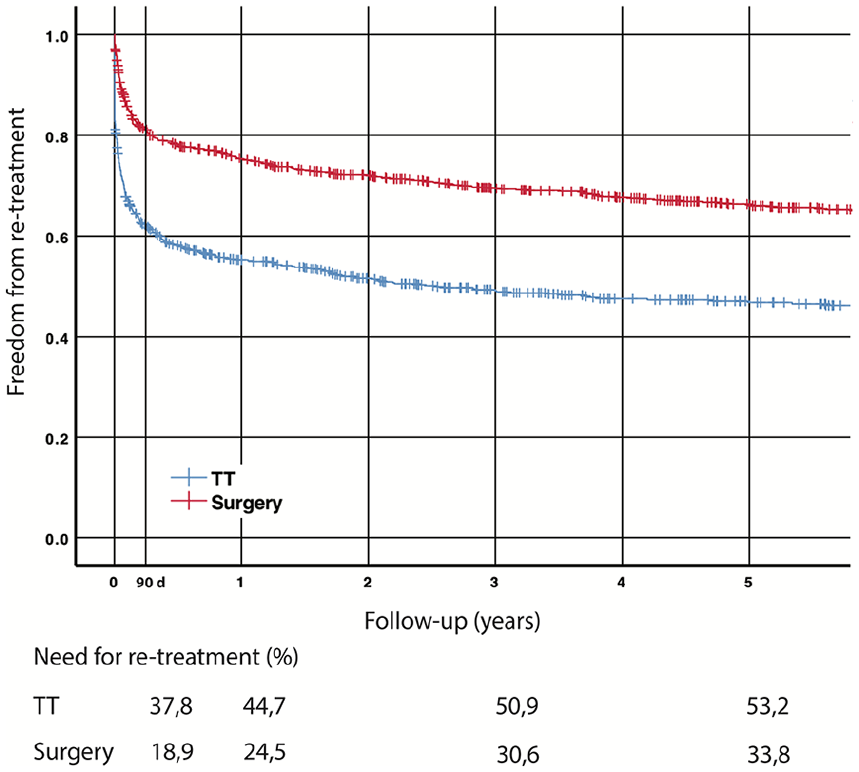
Cumulative freedom from retreatment after TT and surgery.
In the multivariate Cox regression analysis, surgery was associated with a lower risk of recurrence than TT (HR 0.50, 95% CI 0.43–0.56, p < 0.001). Male sex was associated with a lower risk of recurrent treatment (HR 0.75, 95% CI 0.63–0.90, p = 0.001), and higher age decreased the risk of recurrent treatment (HR 0.99, 95% CI 0.99–0.99, p < 0.001). Comorbidities were not associated with the risk of recurrence (HR 1.06, 95% CI 0.66–1.70, p = 0.803). Associations of baseline features with freedom of retreatment is shown in Fig. 4.
Secondary outcome
No need for reoperation after TT and surgery is shown in Fig. 3. The majority of reoperations occurred within the first year, after which the incidence declined. At 5 years, 36.0% of the TT treated and 18.8% of the surgically treated patients had undergone reoperation at some point.
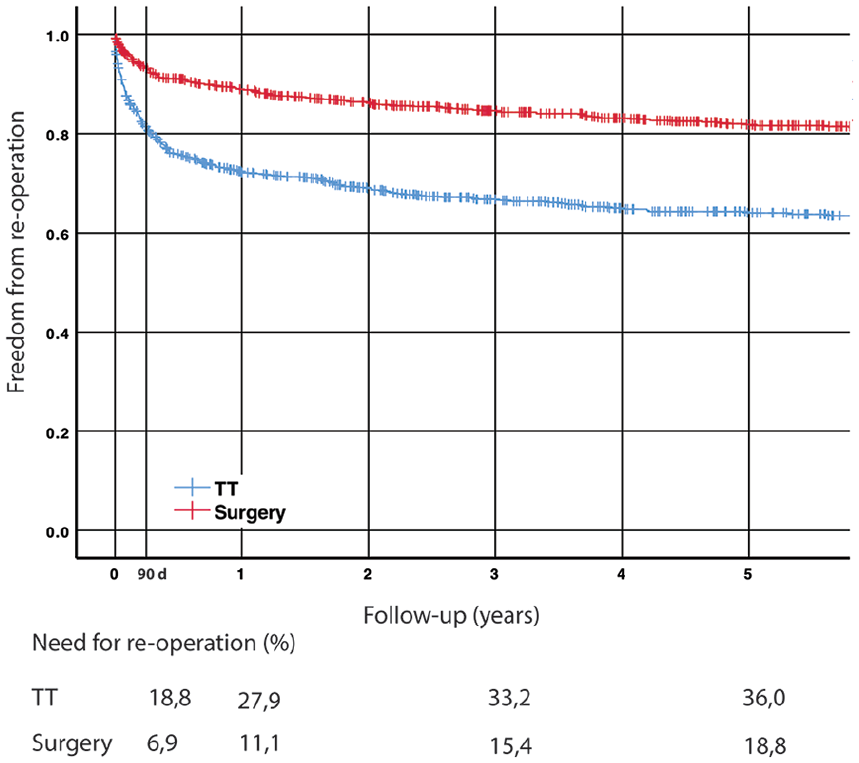
Cumulative freedom from reoperation after TT and surgery.
In the multivariate Cox regression analysis, surgery was associated with a lower risk of recurrence than TT (HR 0.42, 95% CI 0.34–0.51, p < 0.001). Male sex was associated with a lower risk of recurrent surgery (HR 0.65, 95% CI 0.52–0.81, p < 0.001), and higher age decreased the risk of recurrent surgery (HR 0.99, 95% CI 0.98–0.99, p < 0.001). Comorbidities were not associated with the risk of recurrent surgery (HR 1.09, 95% CI 0.55–2.17, p = 0.810). Associations of baseline features with freedom of reoperation is shown in Fig. 4.
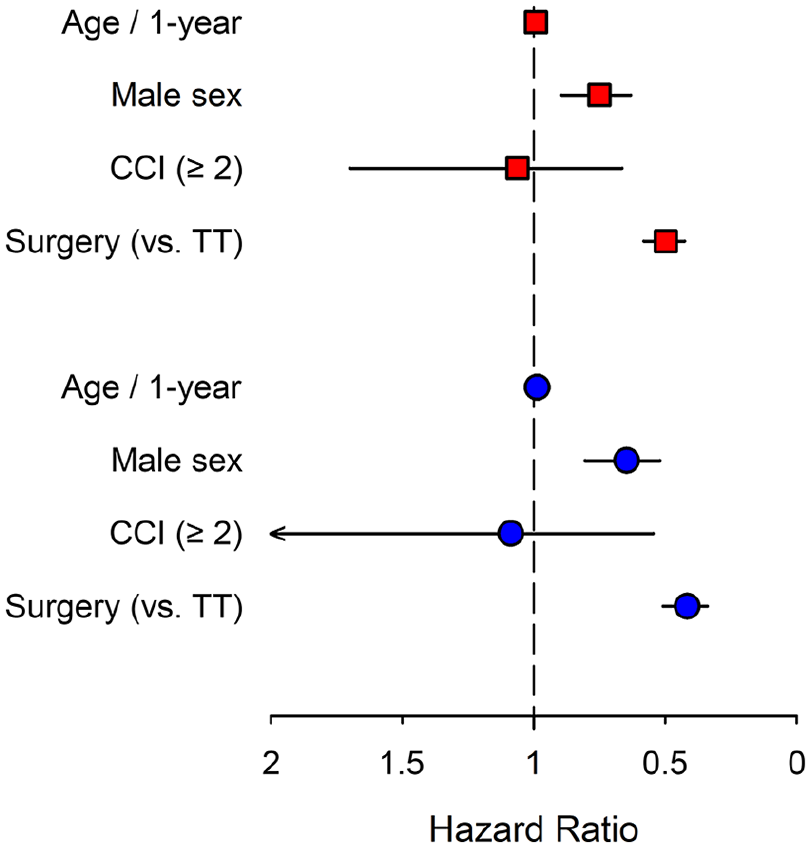
Forest plot for associations of baseline features with freedom of retreatment (red squares) and freedom of reoperation (blue dots) in multivariable analysis. Whiskers represent a 95% confidence interval.
Discussion
The main finding of this study is that repeat visits for treatment of complications, recurrence, and other sequelae after spontaneous pneumothorax are frequent and needed in half of patients treated with TT and a third of patients after surgery.
The finding that recurrences are less common after surgery is in line with previous observations,10,11 which lends credibility to the results. We found that 36.0% of the spontaneous pneumothoraxes primarily treated with TT were reoperated within a 5-year follow-up; the 5-year reoperation rate after surgery remained considerable, however, with 33.8% of patients requiring repeat surgery. However, when assessing the resource consumption caused by sequelae of TT or surgery, we also considered other complications such as infections and effusions of the pleural space as sequelae of invasive treatment occurring within the first 30 days postintervention. Although these are not recurrences of the pneumothorax per se, they are most likely complications related to treatment as well as possibly the underlying pathology behind the pneumothorax. Nevertheless, they are essential endpoints when describing the resources allocated to the treatment of subsequent pleural and pulmonary morbidity in this patient group.
The re-operative rate was significantly higher in the TT group than in the surgery group. This is to be expected, as the existing literature consistently describes a lower rate of recurrence and reoperation for surgically treated patients. 12 There is, however, a paucity of data on recurrence rates as well as a large variation, which is partly due to differing definitions of endpoints. A previous study found that open thoracotomy could be more effective than video-assisted thoracic surgery (VATS), 12 but we could neither confirm nor rule out the effect of open versus thoracoscopic surgery, as we were unable to differentiate between surgical approaches and surgical details (such as extent and method of pleurodesis for example) based on operational codes only. Thoracoscopy was also the overwhelmingly more frequent surgical approach of choice in Finland during the entire study period, which would have precluded any meaningful comparison.
Even though most of the patients in the present study were male (77.6%),3,13 the risk of a recurring spontaneous pneumothorax after TT or surgery was higher among females (HR 1.33); accordingly, the need for reoperation was higher among females (HR 1.54), which is also in line with previous studies and is possibly partly explained by cases of catamenial pneumothorax.13,14 –16
In this study, higher age decreased the risk of subsequent repeat treatment after TT or surgery. The same was found of the need for reoperation. For most conditions, higher age increases the risk of recurrence and complications, but our findings suggest that the opposite holds true for spontaneous pneumothorax. In the existing literature, higher age has been found to increase the risk of recurrence, 17 but age has also been found to be insignificant in predicting recurrence. 14 Our finding may be explained by a decreased willingness to opt for invasive treatment in elderly patients with recurring pneumothoraxes compared with younger patients. Younger patients are also, on average, physically more active, and smaller pneumothoraxes are diagnosed more easily. Comorbidities did not affect the risk of retreatment. Spontaneous pneumothoraxes are commonly classified as secondary if the patient is, for example, a smoker or having light asthma. In our clinical experience, physicians tend to classify spontaneous pneumothoraxes primary when patients present with minor comorbidities. Usually, spontaneous pneumothoraxes are classified as secondary if the patient has chronic obstructive pulmonary disease or emphysema. It is also difficult to assess retrospectively with certainty whether some secondary pneumothoraxes have been misclassified as primary as the diagnoses are coded at the treating physician’s discretion.
A recent Australian study found that 85% of large spontaneous pneumothoraxes (excluding tension and bilateral pneumothoraxes) healed with observation and that only 15% needed TT. 18 When we compare these findings with our own finding of a high risk of recurrent pneumothorax after both TT and surgery, the question arises of whether an initial approach of watchful waiting for all noncomplicated pneumothoraxes (i.e., excluding tension and bilateral ones) would better serve patients than the long-favored invasive approach. It may be speculated that, if the threshold for invasive treatment was higher, we could possibly avoid a significant proportion of complications and subsequent morbidity without compromising outcomes, especially in light of the high incidence of recurrent treatment irrespective of the primary approach. It is also more than likely that a less invasive approach would be better from a health-economic standpoint if similar effectiveness can be achieved with a more conservative outcome, even considering the costs of follow-up imaging and visits, which based on our results are almost equally frequent irrespective of primary treatment.
Strengths and limitations of the study
The strength of this study is the use of the Finnish nationwide registry, which includes data on all hospital admissions and major interventional procedures in the country. 19 The data broadly cover procedures performed to treat pneumothoraxes, so the data comprehensively represent the entire population of Finland.
The first limitation is that it is likely that patients treated with surgery at index hospitalization are more complex than those treated with TT, which might increase the risk of recurrence and complications and consequently markedly diminish the difference in outcome rates between the groups and the two groups are not directly comparable. Second, a significant possible confounder in the comparison is that the actual clinical indication may be different for surgical patients even if all procedures are coded for primary spontaneous pneumothorax: For surgical patients, the indication could be, for example, persistent air leak, which might indicate a larger defect more prone to recurrence or, on the contrary, predispose to infection. This might again dilute the differences between approaches. Third, the study has the inherent limitations of a retrospective, registry-based study. Fourth, the data do not indicate whether the recurrent pneumothorax was ipsi- or contralateral, so we cannot be sure if the recurrence is on the same side.
Conclusions
Retreatment rates were significantly higher among primary spontaneous pneumothorax patients treated at index hospitalization with TT than among patients treated with surgery. The groups were, however, not directly compared, and the main finding was the generally high occurrence rates for repeat treatment. The high overall rate of recurrent treatment with either modality, coupled with the well-documented good results of conservative treatment, calls for a critical evaluation of treatment and follow-up protocols especially for uncomplicated primary spontaneous pneumothoraxes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.