
Abstract
Background:
Swedish healthcare is in a period of transition with an expanding private sector. This study compares quality of outcome after groin hernia repair performed in a public or private healthcare setting.
Methods:
A cohort study based on data from the Swedish National Hernia Register combined with Patient-Reported Outcome Measures (PROMs) 1 year after groin hernia repair. Between September 2012 and December 2018, a questionnaire was sent to all patients registered in the hernia register 1 year after surgery. Endpoints were reoperation for recurrence, chronic pain, and patient satisfaction.
Results:
From a total of 87,650 patients with unilateral groin hernia repair, 61,337 PROM answers (70%) were received from 71 public and 28 private healthcare providers. More females, acute and recurrent cases, and patients with high American Society of Anesthesiology (ASA) scores were operated under the national healthcare system. The private sector had more experience surgeons with higher annual volume per surgeon, shorter time on waiting lists, and shorter operation times. No difference was seen in patient satisfaction. Groin hernia repair performed in a private clinic was associated with less postoperative chronic pain (OR 0.85, 95% CI 0.8–0.91) but a higher recurrence rate (HR 1.41; 95% CI 1.26–1.59) in a multivariable logistic regression analysis.
Conclusion:
Despite private clinics having a higher proportion of experienced surgeons and fewer complex cases, the recurrence rate was higher, whereas the risk for chronic postoperative pain was higher among patients treated in the public sector.
Keywords
Introduction
Swedish healthcare has a long tradition of being run by the government where the county councils are responsible for the provision of healthcare. Over recent decades, however, there has been a transition toward private alternatives. Private care providers can be financed by a county council, by a private insurance company, or by the patient. 1
Few comparisons have been made between outcomes achieved by public and private care providers in Sweden. Even from a global perspective, little has been published in the literature, and most studies have focused on economic performance. 2 Contrary to common belief, most studies on quality of care have shown that European national healthcare systems are as efficient or even superior to private care providers. 3
There are few reports on patient-reported outcomes (PROMs) and quality of care, and results have been mixed. Private hospitals in Germany and Italy had lower mortality and readmission rates compared to public hospitals, while the opposite was seen in France. 4
Groin hernia repair is a frequently performed procedure, hospital stay, if any, is short, and it is performed at several types of clinics in both the public and private sectors. This makes hernia repair a suitable model for comparison of quality of surgery in the public and private sectors.
A small prospective cohort study from England compared outcomes of elective inguinal hernia repair between public and private clinics. 5 It was concluded that short- and long-term complications, recurrence, pain, and satisfaction were similar.
The aim of this study was to compare the public and private sectors in Sweden regarding recurrence rate (defined as operation for recurrence), chronic postoperative inguinal pain (CPIP),6 and patient satisfaction after groin hernia repair.
It was assumed that the Swedish transition toward more private alternatives would have similar surgical outcomes for both private and public providers. The hypothesis was that there would be no difference in neither recurrence rate nor CPIP.
Methods
This was a population-based cohort study based on data from the Swedish Hernia Register (SHR) and a Patient-Reported Outcome Measures (PROM) survey. Data derived from SHR were handled in a cumulative manner on a national level. STROBE-guidelines, 7 Good Clinical Practice, and the WMA8 Declaration of Helsinki were followed. Ethics approval was granted by the Regional Ethics Committee in Umeå, registration number: 2015/305-31Ö.
Swedish Hernia Register (SHR)
The SHR is a nationwide register containing data on all forms of groin hernia repair performed on patients ⩾15 years old. For many years now, more than 97% of all groin hernia repairs performed in Sweden have been registered in SHR. The surgeon registers each surgical procedure online on completion of the operation. Preoperative and procedure information are registered, including surgical method, type of hernia, primary or recurrent hernia, age, sex, BMI, American Society of Anesthesiology (ASA) score, type of anesthesia, and time waiting for surgery. Data registered in SHR are validated each year by a random check of 10% of the clinics participating. 9
Patient-Reported Outcome Measures (PROM)
All patients registered in SHR between 1 September 2012 and 31 December 2018 received a 1 year after their groin hernia repair. Patients could answer via an Internet website or on paper using postal services. A reminder was sent within 1 month if no answer had been received.
Inguinal Pain Questionnaire (IPQ) is a validated instrument covering pain intensity and interference with daily activities. It was developed for assessing both occurrence and severity of chronic postoperative inguinal pain. 10 One of the questions from the IPQ instrument was used in this study:
Grade the worst pain you have felt in the operated groin during the past week.
No pain.
Pain present, but easily ignored.
Pain present, cannot be ignored, but does not interfere with everyday activities.
Pain present, cannot be ignored, and interferes with concentration on everyday activities.
Pain present, interferes with most activities.
Pain present, necessitates bed rest.
Pain present, prompt medical advice sought.
“No chronic postoperative inguinal pain” was defined as Grades 1–3 and chronic postoperative inguinal pain as Grades 4–7.
To evaluate patient satisfaction with surgery one more question was added:
Are you satisfied with the result of your groin hernia surgery?
Scores were as follows:
Yes, completely.
Yes, mainly.
No, not really.
No, not at all.
“Patient satisfaction” was defined as Scores 1–2 and dissatisfaction Scores 3–4.
Patients
Each patient registered in the SHR can be identified through their personal identity code number. 11 It enables us to follow patients over time regardless of where in Sweden they have had their primary or recurrent surgery. All patients aged ⩾15 years that underwent elective or emergent surgery for unilateral or bilateral groin hernia repair in Sweden between 1 September 2012 and 31 December 2018 registered in SHR were included and followed (using a new register category for recurrent procedure) until 6 November 2020. All were followed until recurrence, emigration, death or end of study.
Exclusion criteria were non-Swedish speaking patients, sutured repair (too few patients), other surgical indication than hernia (for example pain or mesh infection), or death before answering the questionnaire. Bilateral surgery could have been registered twice resulting in uncertainty regarding which repair, left or right, the questionnaire applied, hence all bilateral repairs were excluded.
Definitions
Recurrence: groin hernia repair in a groin that had previously been treated during the study period.
Primary Hernia: No prior hernia surgery in present groin entry in the SHR, and not a recurrence repair according to the surgeon.
Chronic postoperative inguinal pain (CPIP): pain present that interferes with daily activities, persistent ⩾3 months, in the present study up to 12 months after surgery. 6
Time waiting for surgery: the time from when the patient was put on a waiting list for surgery until the time surgery took place.
Public healthcare: healthcare managed and provided the county council.
Private healthcare: healthcare services provided by a private care provider under contract with the public healthcare system and/or services provided by a private healthcare clinic under no contract with the public healthcare system. 12
Operation time: the exact time between the first incision and the final suture (skin to skin).
Type of hernia: lateral, medial, femoral, or combined. Combined hernia including a femoral hernia was considered to be a femoral hernia.
Type of repair: open anterior mesh (OAM) repair, open posterior mesh (OPM) repair (preperitoneal), open combined anterior/posterior mesh repair, transabdominal preperitoneal repair (TAPP), or total extraperitoneal repair (TEP).
Specialist: “Yes” = main surgeon qualified as specialist in surgery or “No” = resident (surgeon under training).
Outcome measures
Primary endpoints: (1) reoperation for recurrence in the same groin registered during the study interval; and (2) development of postoperative CPIP (according to IPQ Scores 4–7).
Secondary endpoint: patient satisfaction after surgical intervention according to the PROM.
Statistical analysis
Healthcare provider (public or private) was the independent variable of main interest.
t-test was used to evaluate differences in means of continuous variables and a Chi-square test to calculate the association between categorical variables. Statistical significance was set at p < 0.05.
Multivariable logistic regression analysis was performed for each dependent variable including reoperation for recurrence and CPIP. Results were presented as odds ratio (OR) with 95% confidence intervals (CI). For multivariable analysis of recurrence, all patients were included, while only PROM answers were included in the CPIP analysis.
Baseline characteristics variables (see Table 1) with Chi-square test results p < 0.05 were included in the multivariable analysis. A logistic regression analysis for recurrence (Table 3) was performed for the whole cohort. Questionnaire answers were included in the analysis of CPIP.
Baseline characteristics of 87,650 patients with unilateral repair in the Swedish Hernia Register between 1 September 2012 and 31 December 2018.
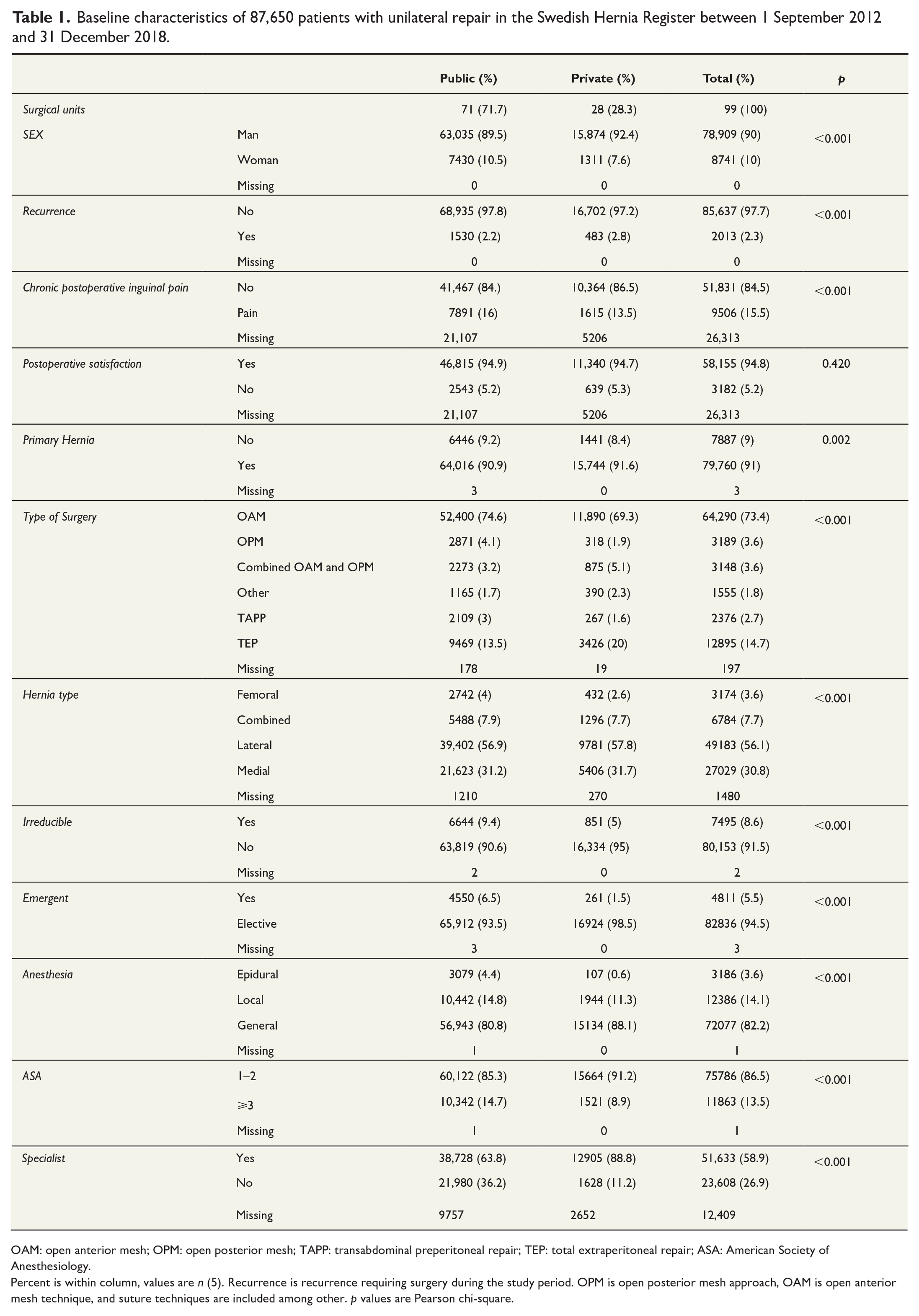
OAM: open anterior mesh; OPM: open posterior mesh; TAPP: transabdominal preperitoneal repair; TEP: total extraperitoneal repair; ASA: American Society of Anesthesiology.
Percent is within column, values are n (5). Recurrence is recurrence requiring surgery during the study period. OPM is open posterior mesh approach, OAM is open anterior mesh technique, and suture techniques are included among other. p values are Pearson chi-square.
Results
A total of 103,117 groin hernia repairs were registered in the SHR between 2012 and 2018. All patients were sent a questionnaire and after exclusion of bilateral repairs 87,650 patients remained, of whom 61,337 (70%) answered (Fig. 1), more patients in public care (70.0%) than those in private care replied (70.0% vs 69.7%; p-value = 0.383).
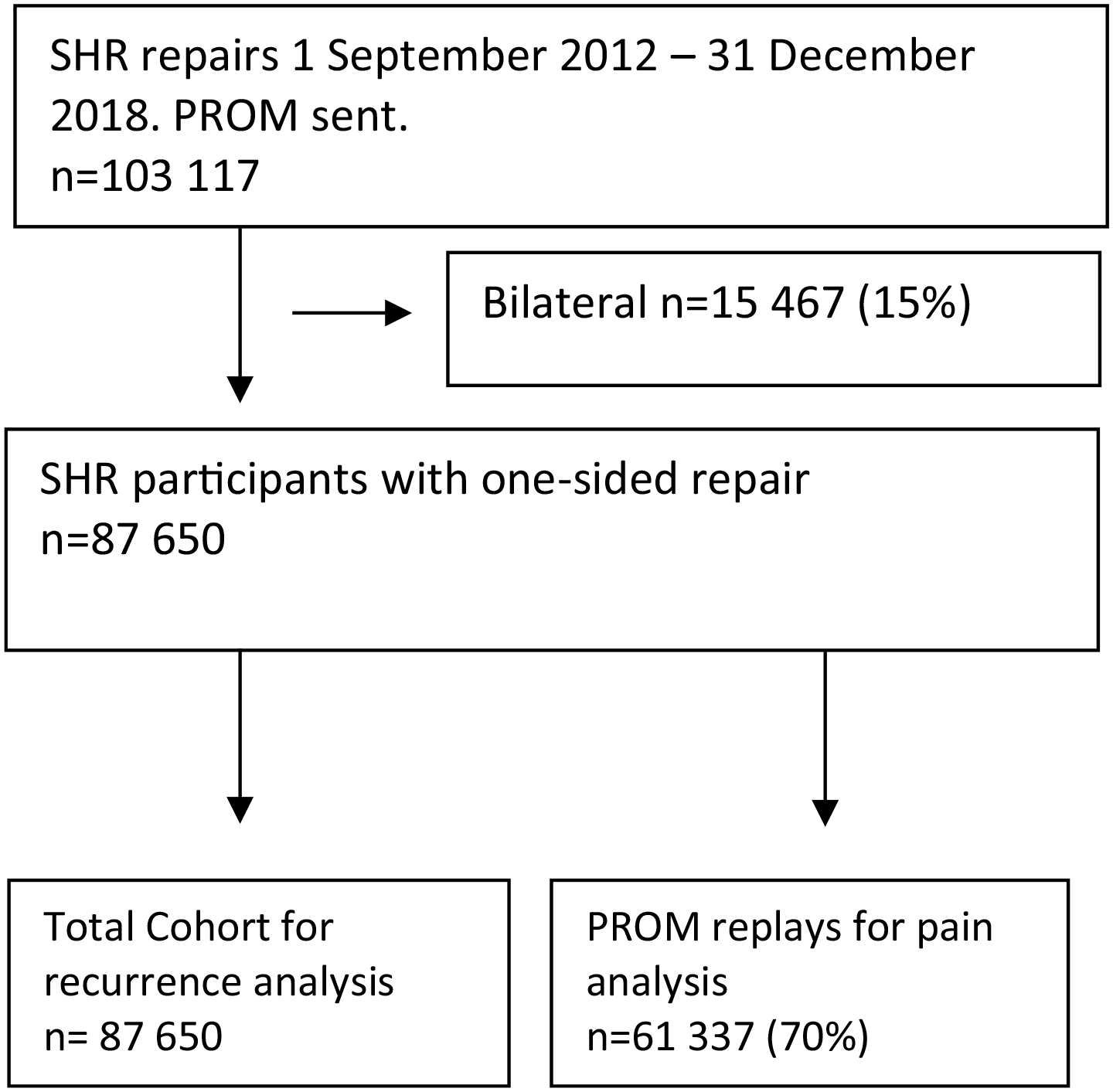
Flow chart.
There were more surgical units (77 vs 28) and repairs (70,465 vs 17,185) in the public sector, where patients were more often female, femoral hernia, irreducible, emergent, large hernias, high ASA score, older, high BMI, and more often performed under local anesthesia. Private surgical clinics had more experienced surgeons with a higher annual surgical volume, more primary hernias, on average 20 min shorter operation time, and shorter time on the waiting list (Tables 1 and 2).
Baseline characteristics of 87,650 patients with unilateral repair in the Swedish Hernia Register between 1 September 2012 and 31 December 2018.
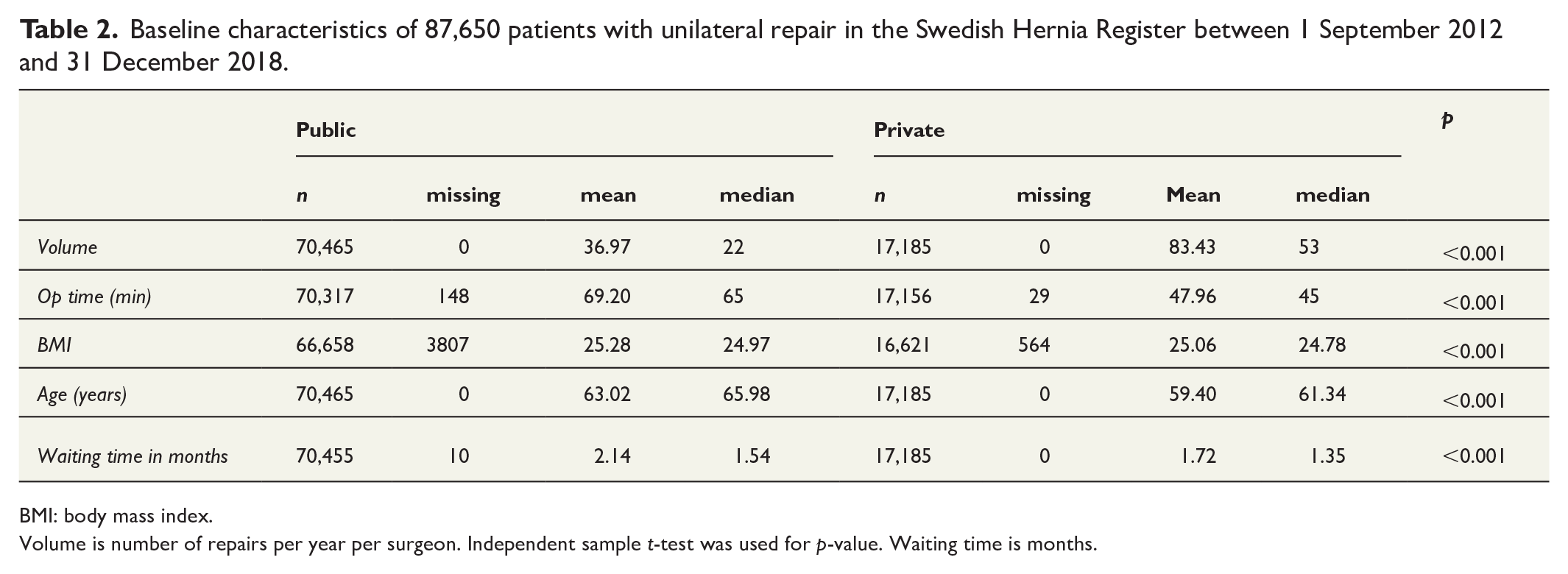
BMI: body mass index.
Volume is number of repairs per year per surgeon. Independent sample t-test was used for p-value. Waiting time is months.
There was no difference in patient satisfaction between public and private care. Excluding missing values, 94.9% were satisfied with public care and 94.7% with private care (Table 1). More open anterior mesh (OAM) repairs were performed in public care, while there were more total extraperitoneal repair (TEP) repairs in private care. The primary endpoints showed a higher degree of CPIP (11.2% vs 9.4%) and a lower recurrence rate (2.2% vs 2.8%) in public care compared to private care (Table 1) with a mean follow-up of 59 months (range 0–98.2 months).
Multivariable logistic regression analysis showed that groin hernia repair in the private sector was associated with a significantly lower risk of CPIP (OR 0.85; 95% CI 0.8-0.9). TEP repair, local anesthesia, lateral hernia, and greater age was also associated with lower risk of CPIP. Increased risk of CPIP was associated with ASA score above three, female sex, emergency surgery, not a primary hernia, and higher BMI (Table 3).
Multivariate logistic regression analysis for chronic postoperative inguinal pain (CPIP) 1 year after groin hernia repair. For PROM replies.
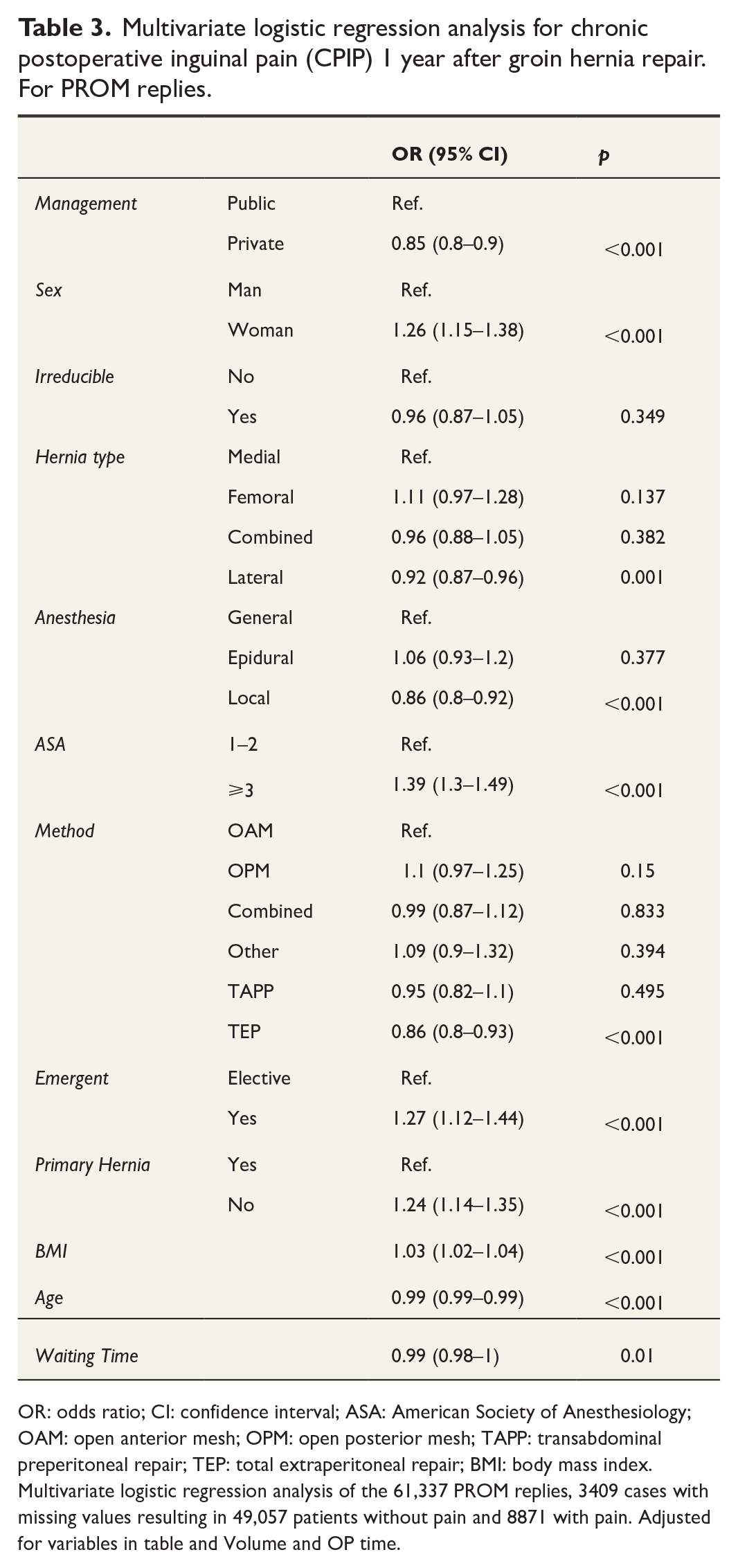
OR: odds ratio; CI: confidence interval; ASA: American Society of Anesthesiology; OAM: open anterior mesh; OPM: open posterior mesh; TAPP: transabdominal preperitoneal repair; TEP: total extraperitoneal repair; BMI: body mass index.
Multivariate logistic regression analysis of the 61,337 PROM replies, 3409 cases with missing values resulting in 49,057 patients without pain and 8871 with pain. Adjusted for variables in table and Volume and OP time.
Groin hernia repair in the private sector was associated with significantly higher risk of recurrence (HR 1.41; 95% CI 1.26–1.59). Recurrent hernia surgery, open posterior approach, medial hernia, and TEP was also associated with higher risk for recurrence. Female sex was associated with lower risk of recurrence (Table 4).
Multivariate cox regression analysis for recurrence during the study time after groin hernia repair.
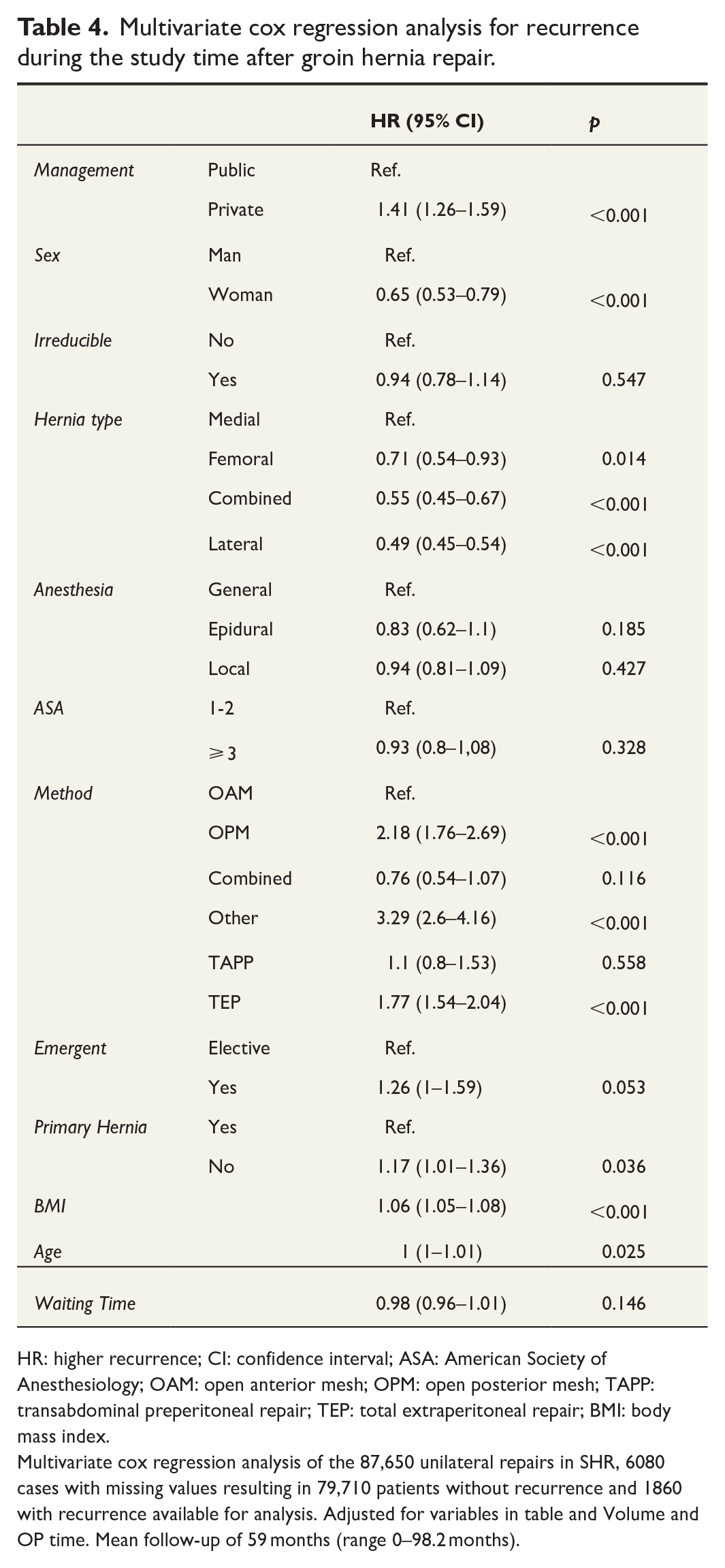
HR: higher recurrence; CI: confidence interval; ASA: American Society of Anesthesiology; OAM: open anterior mesh; OPM: open posterior mesh; TAPP: transabdominal preperitoneal repair; TEP: total extraperitoneal repair; BMI: body mass index.
Multivariate cox regression analysis of the 87,650 unilateral repairs in SHR, 6080 cases with missing values resulting in 79,710 patients without recurrence and 1860 with recurrence available for analysis. Adjusted for variables in table and Volume and OP time. Mean follow-up of 59 months (range 0–98.2 months).
Discussion
There were significant differences between patients in the public and private sectors. Patients in the public sector had more femoral and non-primary hernias, more hernias were large, irreducible, and operated acutely, and with higher ASA score, BMI, and greater age. The private sector had more experienced surgeons with a higher volume of hernia surgery, shorter operation time, and shorter time on the waiting list. The main outcome results remained unchanged after adjusting for these factors in a multivariate analysis. This suggests a structural difference.
Previous studies have suggested that private care tends to pick the cherry off the cake that is, easy repairs in young and healthy patients.3,4 Present data suggest that the same applies in Sweden. All preoperative factors presented here suggest that complex procedures are seldom performed in private care, while the least experienced surgeons (measured by annual volume and specialist degree) are more common in the public sector.
These differences are probably due to regulatory and reimbursement differences. Similar conclusions have been presented by other authors. 3
Time waiting for groin hernia surgery in Sweden has increased from 1.4 months in 2014 to 2.3 months in 2020. 13 This situation applies to several surgical fields, 14 with little chance of improvement in the foreseeable future. This has led to an increase in demand for an alternative to public healthcare.
This study was not designed to elicit the cause of differences seen between the public and private sectors. However, the analyzes showed significant differences in private care with higher rates of recurrence, lower rate of chronic pain, 20 min shorter operation time, shorter waiting time, surgeons with a higher annual surgical volume, different method of repair, operate on fewer women, fewer emergent surgery, lower ASA class, BMI, and age. Variables known to affect both pain and recurrence.6,15 –20 We speculate that the seen differences are multifactorial with the production demand and lack of resident education being large contributors in combination with the use of different techniques in private and public care. Private cares use of 20% TEP repairs compared with the public 13.5%. Earlier research has shown that TEP repairs have a higher risk of recurrences among men 20 and that it has a lower risk of CPIP.6,19
The public sector has more residents performing hernia repair compared to the private sector. However, relating to earlier research6,21 the following speculations can be made; Most residents develop their surgical skills in the public sector. Since the number of hernia repairs performed in the private sector is increasing, it is natural that private clinics should be given training responsibility. This should improve the quality of teaching of standard techniques and result in better outcomes. For this to succeed, a change in clinical practice and reimbursement systems in the private sector is needed. This could have different forms in different countries according to regulations and current practice.
Open Anterior Mesh repair (OAM) in men is by far the most used repair technique in both the public and private setting in Sweden, but the techniques used differ between public and private surgeons. OAM are more common under the national healthcare system while TEP as well as other methods are more often used in private clinics. This is likely due to differences in surgeon experience, tradition, and the differences in patient populations such as age, BMI, and comorbidity. The more complicated case-mix in the public sector might also impact results negatively.
A strength of this study is that it is based on register data from more than 100,000 patients, making it one of the largest studies in the field. The PROM questionnaires sent to all patients having had a repair in Sweden during the time period of this study is as close as one can get to national coverage. A reply rate of 70% in such a large cohort of patients being contacted is also a strength.
Previous studies using the same PROM questionnaire have reported little difference between patients replying and those not replying, and that non-responders tend to have less pain than responders. 19 Recurrence in this study was defined as repair for recurrence; hence, the true figure is likely to be greater.
The gold standard for evaluating CPIP and recurrence is a clinical examination. A specific pain questionnaire may be helpful when analyzing causes and type of pain, but this will not always be enough to differentiate between different causes. Previous studies have reported clinically significant CIPIP in the 10% to 12% range with a decrease over time. 6 As different studies use different definitions of CPIP and follow-up time, direct comparison is difficult. Present study reports 15.5%. Interpretation of CPIP data in the present study is limited by the fact that no preoperative pain data were included. 6 The high levels of patient satisfaction reported after both private and public repairs, however, hopefully reflects decreased pain after surgery.
Using reoperations to measure recurrence will catch symptomatic recurrences but is likely an underestimation of the true number. Clinical examinations of all participants were not in the scope of this study, but are a limitation, for both CPIP and recurrences.
Every country has its own conditions and regulations regarding provision of healthcare. Many countries, especially in Europe, have a system similar to Sweden, and data presented here could be useful to decision-makers in these countries.
Conclusion
This is the first ever nationwide patient-reported comparison of hernia surgery outcomes in the public and private healthcare sector. Patient-reported CPIP after groin hernia repair performed in the public sector was higher than in the private sector, while groin hernia repair performed in the private sector had a higher recurrence rate than the public sector. Patient satisfaction was similar for both sectors.
A difference in case-mix, with more complicated hernia repairs are performed in the public sector. There is undoubtedly room for improvement in both the private and public care sectors. As the current transition toward privatization continues, quality control of surgery, from both patient and care provider perspectives, is important. Further studies on cost-effectiveness and clinical outcomes, comparing public with private healthcare, are warranted to improve the overall quality of hernia surgery.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969241242312 – Supplemental material for Management of groin hernia repair in Sweden: A register-based comparative analysis of public and private healthcare providers
Supplemental material, sj-docx-1-sjs-10.1177_14574969241242312 for Management of groin hernia repair in Sweden: A register-based comparative analysis of public and private healthcare providers by Anders Hemberg, Jakob Landén, Agneta Montgomery, Henrik Holmberg and Pär Nordin in Scandinavian Journal of Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from the Swedish Hernia Register and salary grant from The Thelma Zoéga Foundation’s for medical research.
Ethics approval
All authors have seen and approved the final version of the manuscript. All authors fulfill the COPE requirements for authorship.
Data availability
Data is available to review in person after correspondence with lead author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.