
Abstract
Background and objective:
Studies on the outcomes of parathyroid surgery are scarce. The aim was to report the outcomes and to study the association between pre- and peri-operative information with the outcomes of patients operated for primary hyperparathyroidism.
Methods:
This was a retrospective, descriptive study with unselected patients treated surgically for primary hyperparathyroidism from a catchment population of 704,500 in Finland. Data were acquired from the electronic hospital registers based on parathyroid surgery procedure codes between 1 January 2017 and 31 December 2018. Preoperative data, surgical data, preoperative and postoperative laboratory values, histopathological findings, and postoperative clinical data were recorded.
Results:
During the 2-year study period, 149 patients with primary hyperparathyroidism were treated surgically with a 97% remission rate. Surgical complications included postoperative bleeding in two patients (1%) and vocal cord paralysis in one patient (0.6%). No postoperative infections were reported. Three patients (2%) developed postoperative hypoparathyroidism necessitating the use of alfacalcidol more than 1 month after surgery. Ionized calcium measured 0–1 days after surgery was not statistically significantly associated with remission or postoperative hypoparathyroidism. Serum parathyroid hormone (PTH) assessed 0–1 days postoperatively was associated with persistent disease, but not with postoperative hypoparathyroidism. The histopathological diagnosis was adenoma or hyperplasia in 112 patients (75%), atypical adenoma in 28 patients (19%), and carcinoma in five patients (3%). Patients with parathyroid carcinoma had higher preoperative ionized calcium and PTH values than those with adenoma or hyperplasia.
Conclusions:
Most patients who were operated due to primary hyperparathyroidism achieved normocalcemia after surgery, and the frequency of complications was low. Ionized calcium taken 0–1 days after surgery was not associated with remission of hyperparathyroidism or postoperative hypoparathyroidism. High postoperative serum PTH predicted persistent disease.
Introduction
Primary hyperparathyroidism is caused by excessive parathyroid hormone (PTH) secretion leading to elevated levels of serum PTH and calcium. Primary hyperparathyroidism is usually caused by benign overgrowth of parathyroid tissue either in an individual gland (80% of cases) or in multiple glands (15%–20% of cases). 1 Primary hyperparathyroidism typically occurs at 50–60 years of age, and it is twice more common in women than in men. 2 The most common cause of secondary hyperparathyroidism is end-stage renal disease. 3 In tertiary hyperparathyroidism, prolonged secondary hyperparathyroidism causes hyperplasia and autonomous hypersecretion of parathyroid glands independent of blood calcium levels.
Surgery is the primary treatment for hyperparathyroidism. Indications for surgery in our hospital are ionized calcium higher than 1.5 mmol/L, hypercalciuria (dU-Ca >10 mmol/24 h), renal insufficiency (estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2), nephrocalcinosis, neuropsychiatric symptoms, planned pregnancy, and osteoporosis or osteopenia. In young patients, hyperparathyroidism is operated at lower calcium levels because decades of hypercalcemia adversely affect skeletal, renal, and brain function. If the criteria for surgery are not met, the patient’s calcium and creatinine levels are monitored once a year. 4 Eligibility for surgery is evaluated according to the patient’s other medical conditions and age. If the patient is not eligible or does not prefer surgery, hyperparathyroidism is treated with medications, such as calcimimetics. 5
Possible complications in the surgical treatment of hyperparathyroidism are hypoparathyroidism, vocal cord paralysis caused by damage to the recurrent laryngeal nerve (RLN), postoperative infection, and bleeding. In earlier studies, complications have been reported in 1.45%–3.10% of surgically treated patients.6,7
According to a systematic review of 89 articles on postoperative hypoparathyroidism, the incidence of hypoparathyroidism was 0.0%–20.2%. 8 In transient postoperative hypoparathyroidism, serum calcium levels return to normal within a few weeks after surgery as healthy glands resume PTH production. The risk of postoperative transient hypocalcemia is increased by very high calcium levels, prolonged hypercalcemia, high alkaline phosphatase, and renal failure. 5 Calcium and vitamin D supplements are generally recommended for 4 weeks after surgery to avoid transient hypocalcemia. 9 The risk of chronic hypoparathyroidism is increased if several parathyroid glands are removed or if the parathyroid glands have been operated on before. 9 Hypoparathyroidism may be classified as chronic if hypocalcemia persists 6 months postoperatively. 10
Studies on outcomes after parathyroid surgery and the reasons for postoperative complications and persistent hyperparathyroidism in Finland are sparse. The aim was to report the outcomes and to study the association between preoperative and operative information and the outcomes of patients treated surgically for hyperparathyroidism in Tampere University Hospital.
Methods
This retrospective study was conducted at Tampere University Hospital (Tays) and Kanta-Häme Central Hospital in Finland served by the same surgical unit. The combined catchment population of these two hospitals was 704,500.
Data on consecutive and unselected patients with surgically treated hyperparathyroidism from 1 January 2017 to 31 December 2018 were collected from the hospitals’ electronic registers based on parathyroid procedure NOMESCO codes (BBA10, BBA20, BBA30, BBA40, BBA50, BBA99). 11 This study is focused on patients operated for primary hyperparathyroidism. Those operated for secondary or tertiary hyperparathyroidism or multiple endocrine neoplasia (MEN) syndrome were excluded due to the different surgical approach with total or subtotal parathyroidectomy. Furthermore, those re-operated due to previous unsuccessful parathyroid surgery or relapse of hyperparathyroidism were excluded from the study population.
The following data were collected: operation date, gender, age, height, weight, hypertension, smoking history, indications for surgery (serum ionized calcium >1.5 mmol/L, diurnal urinary calcium >10 mmol, renal insufficiency (eGFR <60 mg/mL/1.73 m2), osteoporosis or osteopenia, nephrocalcinosis, neuropsychiatric symptoms, and planned pregnancy), history of previous neck surgeries. Urgent surgery was performed within 1–2 months if the patient was symptomatic and had an ionized calcium level greater than 1.75 mmol/L or if malignancy was suspected, while others were operated within 6 months. Information on surgery was also collected: how many glands were removed according to the surgeon and whether nerve monitoring was used. Biopsies, partial gland removals, or implanted glands were not considered as removed, that is, only totally removed glands were counted.
Postoperative information on the complications, that is, hypoparathyroidism, bleeding necessitating re-operation, wound infection, and vocal cord paralysis, was collected. Hypoparathyroidism was defined as need for alfacalcidol for more than 1 month after surgery. Remission of hyperparathyroidism was defined as ionized calcium in the normal or low range (⩽1.35 mmol/L) at the control visit 4–6 weeks after surgery. All patients did not undergo postoperative laryngoscopy. The hoarseness of voice was assessed clinically 4–6 weeks after surgery, and those with clinical suspicion of vocal cord paralysis were sent to laryngoscopy. Postoperative infections were evaluated at postoperative clinical visit, and by analyzing the national electronic prescription database for antibiotics used postoperatively. Histopathological findings were classified as adenoma or hyperplasia, atypical adenoma, carcinoma, no parathyroid gland tissue, and normal parathyroid gland.
Preoperative localization of the abnormal parathyroid glands was done mainly with single-photon emission computed tomography–computerized tomography (SPECT–CT). Parathyroid surgery was performed under general anesthesia. Minimally invasive surgery was a method of choice in all patients with only one hotspot in SPECT–CT scan. If multiple hotspots were present, an ultrasound examination was done preoperatively. Bilateral exploration was performed if hotspots in SPECT–CT or suspected ultrasound foci were detected bilaterally. Patients with unlocalized primary hyperparathyroidism were not operated. RLN monitoring (NIM Neuro 3.0) was used in selected cases. No autofluorescence imaging or indocyanine green angiography was used. 12 Intraoperative PTH measurement was not used. All patients received routine postoperative substitution of calcium 2000 mg and vitamin D 40 μg for 14 days and 1000 mg calcium and 20 μg vitamin D for 14 days.
Serum ionized calcium was measured postoperatively on the first postoperative day and at the control visit 4–6 weeks after surgery. Laboratory tests used in this study were done in the Fimlab laboratory which is Finland’s largest accredited laboratory producing services to Pirkanmaa and Kanta-Häme hospital districts among other hospital districts. All the laboratory values taken during the study period were collected from the Fimlab laboratory database starting from a year before the surgery up to 6 months after the surgery. From the laboratory results, we analyzed preoperative ionized calcium (highest), PTH (highest), 25-hydroxyvitamin D (lowest), and glomerular filtration rate (lowest). Postoperatively (0–1 days), we analyzed ionized calcium and PTH. Laboratory values in patients with postoperative remission without hypoparathyroidism were compared with those with persistent hyperparathyroidism and to those with prolonged hypoparathyroidism. Furthermore, laboratory results were compared in patients with adenoma or hyperplasia, atypical adenoma, and carcinoma.
Statistical analysis
Descriptive statistics are presented as medians (range) for continuous variables. Count (n) and percentage (%) are used for categorical variables. Differences in the study groups were analyzed using chi-square or Fisher’s exact test for categorical variables and Mann–Whitney U test for the continuous variables. A p value of less than 0.05 was considered statistically significant. IBM SPSS Statistics for Windows version 28.0 software was used for all statistical analyses.
Ethical aspects
The study was undertaken in accordance with the Declaration of Helsinki. Due to the retrospective nature of the study, no informed consent from the patients was required. The ethics committee of the Pirkanmaa Hospital District reviewed and approved the study protocol.
Results
A total of 168 patients were operated due to hyperparathyroidism from 1 January 2017 to 31 December 2018 (114 patients from Pirkanmaa and 54 from Kanta-Häme Hospital districts). A total of 149 patients were included on this study population. Thirteen patients operated due to secondary or tertiary hyperparathyroidism, three due to MEN syndrome, and three patients re-operated due to recurrent or persistent hyperparathyroidism were excluded. Clinical characteristics of patients with primary hyperparathyroidism before surgery and indications for surgery are shown in Table 1. The median age of the patients was 66 years, and 83% were female. About 56% of the patients had hypertension, 8% had diabetes, and 7% were current smokers.
Preoperative characteristics of patients with primary hyperparathyroidism (n = 149).
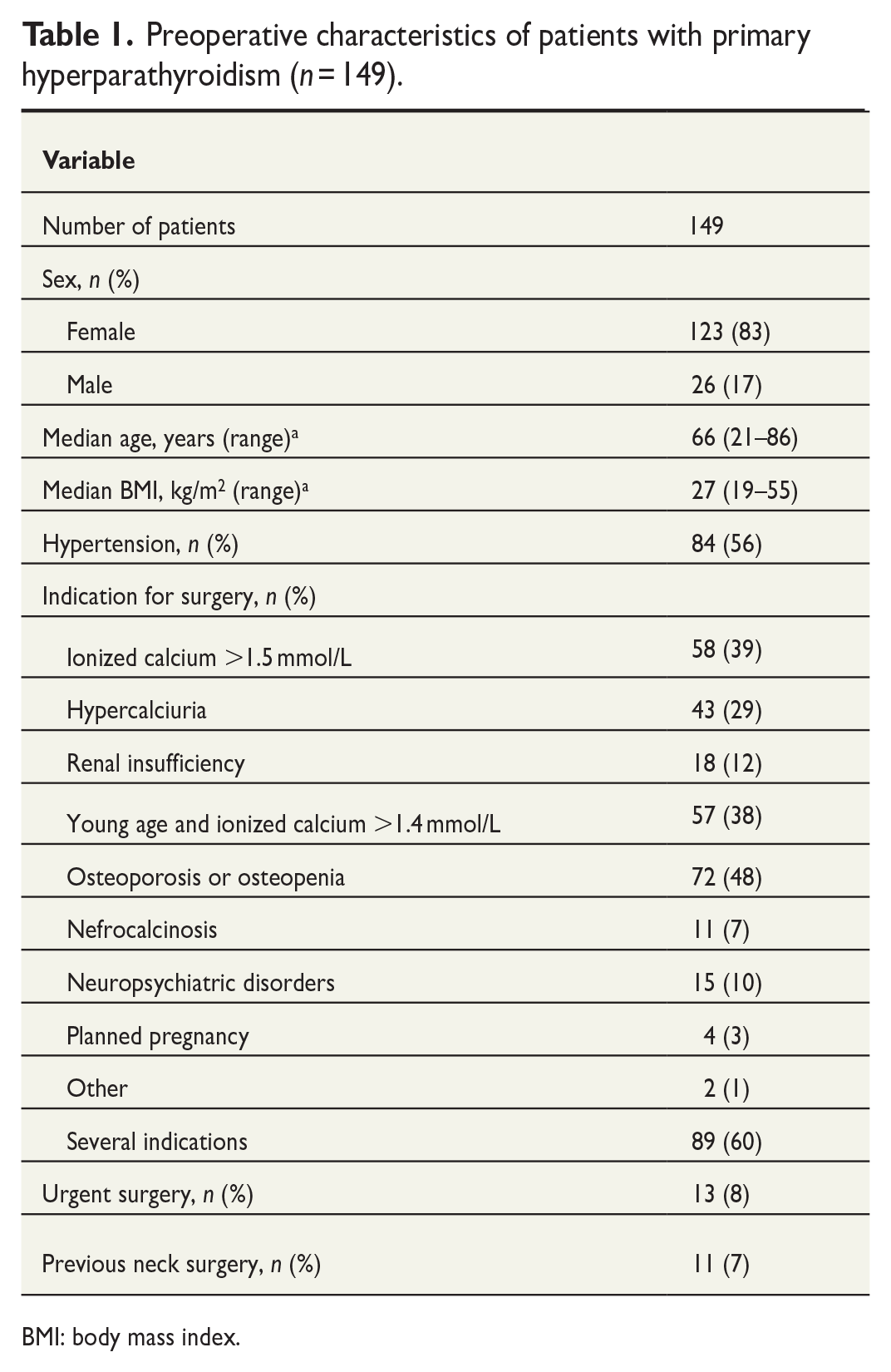
BMI: body mass index.
The most common indications for parathyroid surgery were osteoporosis or osteopenia (48%), ionized calcium more than 1.5 mmol/L (39%), and young age with ionized calcium more than 1.4 mmol/L (38%). A total of 60% of the patients had several indications for parathyroid surgery, and the most common combination was ionized calcium more than 1.5 mmol/L combined with osteoporosis or osteopenia (Table 1).
Young patients with ionized calcium 1.4–1.5 mmol/L were most commonly operated due to osteoporosis or osteopenia (38%) or hypercalciuria (31%). The most common combination of indications in young patients with ionized calcium 1.4–1.5 mmol/L was osteoporosis and hypercalciuria (13%).
Two patients undergoing surgery did not fulfill our standard indications for parathyroid surgery, one 73-year-old patient with ionized calcium of 1.41 mmol/L with numerous symptoms of hypercalcemia and one 54-year-old patient with concurrent Grave’s disease and hyperparathyroidism treated simultaneously with thyroid surgery.
About 93% of the patients had undergone no previous surgeries in the neck area. Urgent surgery was needed in 13 patients (8%), eight of whom had severe hyperparathyroidism (Table 1).
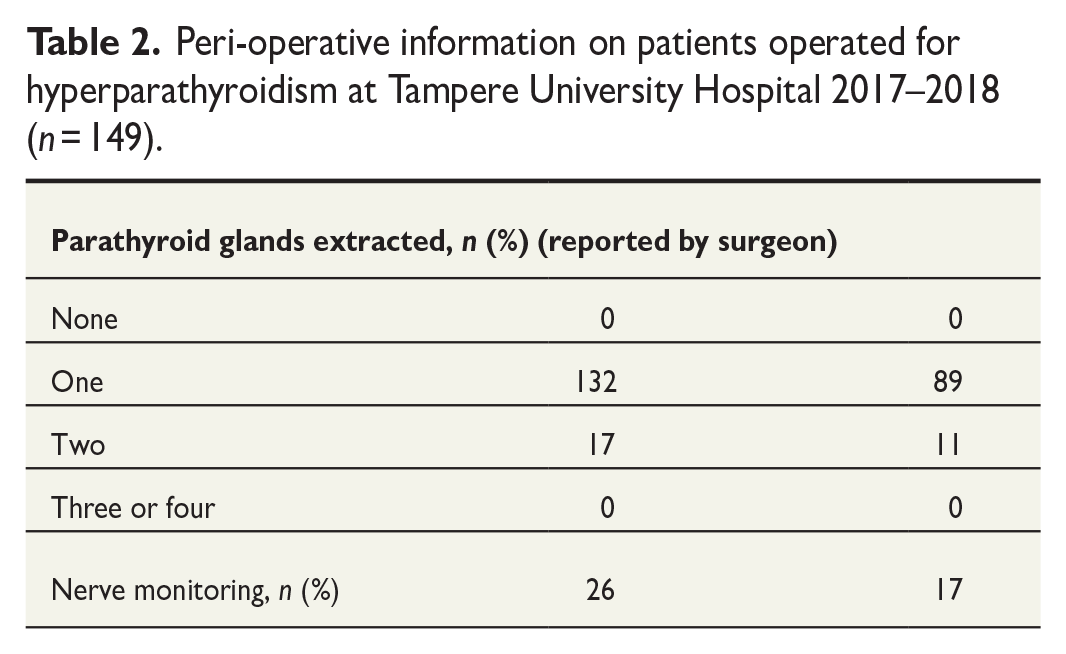
One parathyroid gland was extirpated in 132 patients (89%) and two glands in 17 patients (11%) (Table 2). The surgical method was minimally invasive surgery in 103 patients (69%), more extensive unilateral exploration in 27 patients (18%), had bilateral exploration, and bilateral exploration in 12 patients (8%). Seven patients 7 (5%) had parathyroid adenoma removed during total thyroidectomy.
Peri-operative information on patients operated for hyperparathyroidism at Tampere University Hospital 2017–2018 (n = 149).
Prophylactic antibiotic treatment was not routinely used, and none of the patients developed a surgical site infection. Two patients (1%), however, received prophylactic antibiotics due to estimated increased risk of infection.
One patient (0.6%) suffered vocal cord paralysis during the elective removal of one parathyroid gland performed by a surgeon in training. The patient had diabetes and had not undergone any previous neck surgeries. Nerve monitoring was used during surgery. The adenoma was located under the upper pole of the thyroid gland, with the RLN being in tight contact to the adenoma (Table 3).
Surgical outcomes of patients treated for hyperparathyroidism at Tampere University Hospital 2017–2018 (n = 149).
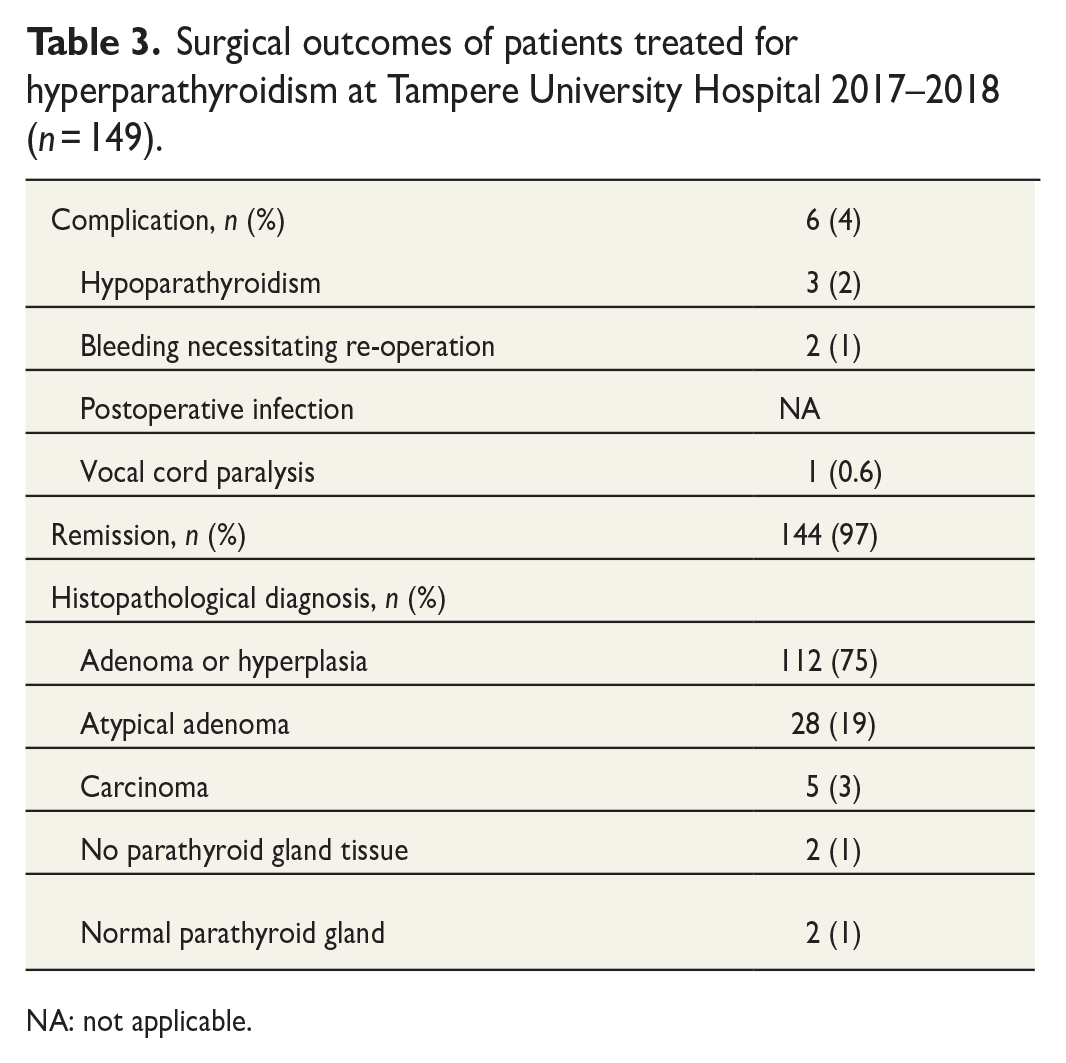
NA: not applicable.
Two patients (1%) had postoperative bleeding requiring re-operation. Neither of them had any medication affecting hemostasis, but one patient was taking omega-3 oil supplements (Table 3).
Despite routinely administered calcium and vitamin D supplementation, 28 patients (19%) had the lowest measured postoperative ionized calcium below the reference range. Seven patients (5%) had ionized calcium measured 0–1 days postoperatively below the reference range. However, only three patients (2%) had postoperative ionized calcium below 1.00 mmol/L necessitating alfacalcidol medication for a duration exceeding 4 weeks postsurgery (Table 3). All patients with persistent hypoparathyroidism underwent thyroid surgery simultaneously due to goiter or thyroid carcinoma. None of these patients had parathyroid carcinoma.
A total of 144 patients (97%) were in remission at the first postoperative control 1 month after surgery (Table 3). Five patients (3%) did not achieve normocalcemia. Reasons for not achieving normocalcemia varied. One patient had persistent hyperparathyroidism despite a large benign adenoma completely removed and another patient despite an atypical adenoma completely removed. Two patients had false-positive preoperative imaging due to a small papillary microcarcinoma and due to an ectopic thyroid nodule. In one case, a surgeon could not locate the adenoma during the initial surgery, and a normal parathyroid gland was removed. A year later, the adenoma was successfully removed by a senior surgeon.
Ionized calcium measured 0–1 days postoperatively was not statistically significantly associated with remission of hyperparathyroidism and postoperative hypoparathyroidism. PTH assessed 0–1 days postoperatively was associated with persistent disease but not with postoperative hypoparathyroidism (Table 4).
Laboratory results for patients with postoperative hypoparathyroidism and persistent hyperparathyroidism after surgery compared with those without complications (n = 149).
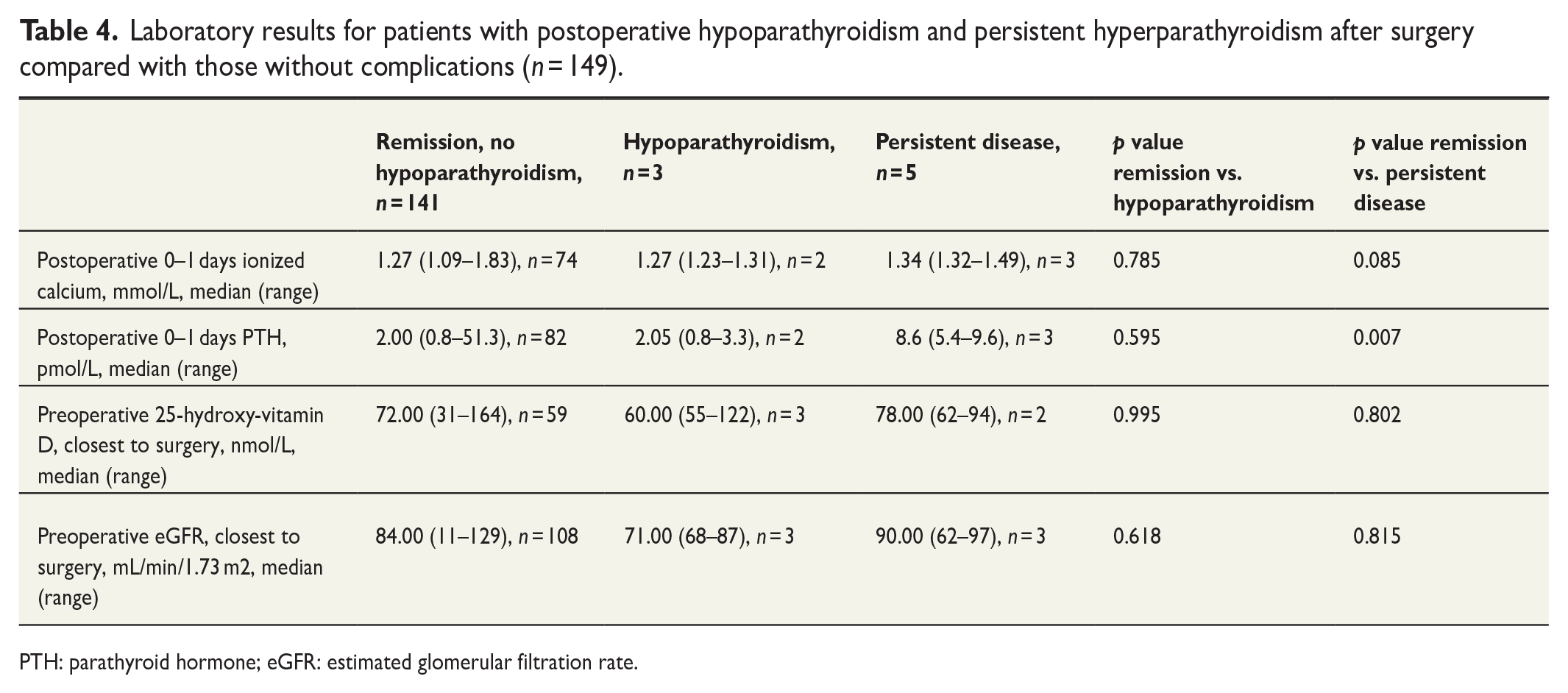
PTH: parathyroid hormone; eGFR: estimated glomerular filtration rate.
In 75% of the patients, the histopathological finding was adenoma or hyperplasia, 19% had atypical adenoma, and 3% had carcinoma (Table 3). There were four patients with normal parathyroid tissue or no parathyroid tissue. Two of these patients had a persistent disease. In two patients, hyperparathyroidism was cured, but the pathologist did not find any parathyroid tissue in the surgical specimen. The remission of hyperparathyroidism in these cases is likely explained by either error in the processing of pathological samples or disruption of adenoma blood supply due to surgical tissue preparation.
Patients with carcinoma had statistically significantly higher preoperative calcium and PTH levels than those with adenoma or hyperplasia (Table 5).
Laboratory results of patients surgically treated for hyperparathyroidism at Tampere University Hospital 2017–2018 (n = 149).
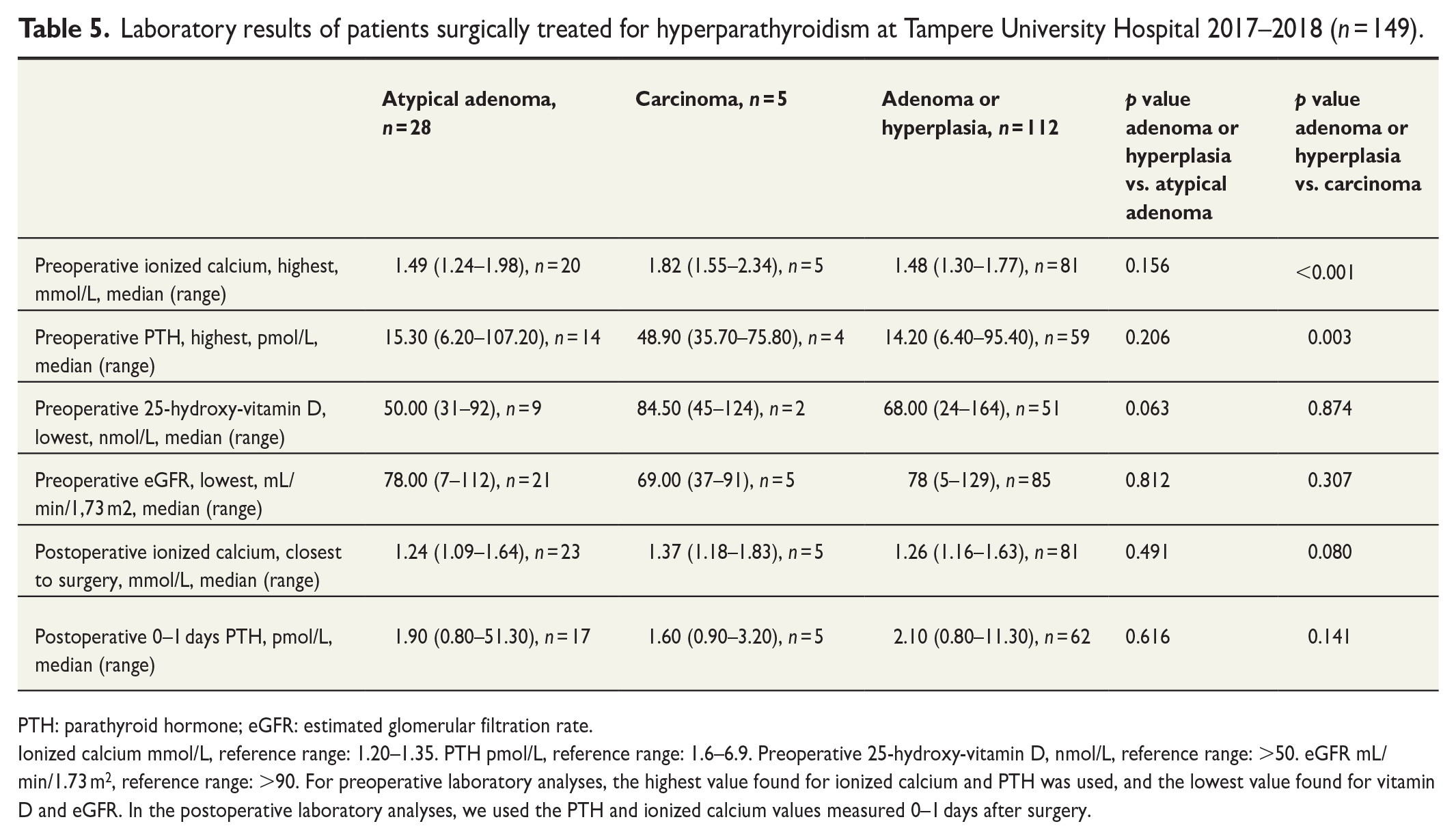
PTH: parathyroid hormone; eGFR: estimated glomerular filtration rate.
Ionized calcium mmol/L, reference range: 1.20–1.35. PTH pmol/L, reference range: 1.6–6.9. Preoperative 25-hydroxy-vitamin D, nmol/L, reference range: >50. eGFR mL/min/1.73 m2, reference range: >90. For preoperative laboratory analyses, the highest value found for ionized calcium and PTH was used, and the lowest value found for vitamin D and eGFR. In the postoperative laboratory analyses, we used the PTH and ionized calcium values measured 0–1 days after surgery.
Discussion
Reporting the effectiveness and complications of surgical treatment for hyperparathyroidism is important to improve quality of care. It is also valuable for informing the patients about the outcomes and risks of surgery. Reports on the quality of parathyroid surgery in Finland are sparse, and there are no reports of the reasons for failed surgeries and complications. One Finnish unit reported the outcomes of parathyroid surgery with a remission rate of 89.5%. 13 The remission rate in the present cohort was high (97%). Reasons for nonremissions included double adenomas, misleading imaging results, and the inability to locate the adenoma. Complications of parathyroid surgery were rare (4%, n = 6). Hypoparathyroidism at 4–6 weeks after surgery occurred in 2% of the patients, affecting only those patients with thyroid gland removed simultaneously.
In a study of 1650 consecutive parathyroidectomies, surgical complications occurred in 1.45%–3.10% of patients. 7 The present results are in line with these findings. Here, two patients experienced postoperative bleeding, and neither of these patients was taking medications increasing bleeding risk. One of the patients was taking omega-3 supplements, but current evidence suggests that omega-3 supplements are not conducive to cause postoperative hemorrhage. 14
Postoperative hypoparathyroidism occurred in 2% of the patients. All patients with hypoparathyroidism underwent thyroid surgery simultaneously due to thyroid goiter or carcinoma. According to a systematic review of 89 articles about postoperative hypoparathyroidism, the incidence of hypoparathyroidism was 0.0%–20.2%. 8 There is a marked variation in the definition and incidence of hypoparathyroidism after parathyroid surgery. The incidence of long-term hypoparathyroidism has been reported to be 0.1%–2.7% after surgery for primary hyperparathyroidism and 5%–26% after surgery for secondary hyperparathyroidism.7,8,13 We defined hypoparathyroidism as a condition requiring alfacalcidol 1 month after surgery. The cutoff time for diagnosis of permanent hypoparathyroidism in other studies is commonly 6–12 months, which may have led to an overestimation of the incidence of hyperparathyroidism in our study. 10
About 97% of patients went into remission after surgery. In a study by Udelsman et al., 7 the cure rate was 99% in 1037 patients who underwent minimally invasive parathyroidectomy and 97% in 613 patients who underwent bilateral neck exploration. In a Finnish study by Ryhänen et al., 13 parathyroidectomy resulted in normocalcemia in 111 out of 124 (89.5%) patients, while 13 (10.5%) patients did not reach normocalcemia.
In this study, 75% of the patients had adenoma or hyperplasia, 19% of patients had atypical adenoma, and 3% had a parathyroid carcinoma. In a study of 1650 consecutive parathyroidectomies, histopathological findings were 95.0%–95.1% adenoma or hyperplasia and 2.9%–4.7% double adenomas. 7 In a study of patients operated for primary hyperparathyroidism (n = 611) at a single university hospital, 92.6% of the histopathologic findings were adenoma or hyperplasia, 3.1% atypical adenoma, and 4.3% carcinoma. 15 The reason for the higher occurrence of atypical adenomas in our study is unknown, but according to pre-operative and postoperative laboratory values, remission, complication rates, adenomas, and atypical adenomas behaved similarly.
Ionized calcium taken 0–1 days after surgery was not associated with remission of hyperparathyroidism nor postoperative hypoparathyroidism. High postoperative serum PTH predicted persistent hyperparathyroidism but not postoperative hypoparathyroidism. Our results do not confirm the earlier report on the association between hypoparathyroidism and postoperative PTH. In a study by Chia et al., 16 patients requiring calcium postoperatively had PTH levels less than 15 pg/mL (1.6 pmol/L) 8 h after surgery, suggesting that low postoperative PTH predicts hypoparathyroidism.
The surgical indications for parathyroid surgery in this study were comparable to those previously reported. Here, 60% of the patients had several indications for parathyroid surgery, the most common combination being ionized calcium more than 1.5 mmol/L and osteoporosis or osteopenia. In an earlier study, the indications for parathyroid surgery were based largely on age, serum calcium, and the presence of bone and/or renal complications. 15 In another study, symptoms and signs of surgically treated hyperparathyroidism were neurocognitive symptoms, osteopenia or osteoporosis, kidney stone disease, and cardiovascular disease. 7 In a third study,13 the surgical criteria for parathyroid surgery were based on the recommendation of the Third International Workshop on the Management of Asymptomatic Primary Hyperparathyreoidism in 2008 and were fulfilled by 80.6% of patients, that is, serum calcium 0.25 mmol/L above the upper limit of normal, reduction in bone density, and age less than 50. 17
In conclusion, the remission rate of parathyroid surgery was high in the author unit. Postoperative hypoparathyroidism was the most common complication but occurred only in those patients with thyroid gland removed simultaneously. These results do not support measuring PTH after surgery to predict postoperative hypoparathyroidism.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the research funding provided by Tampere University Hospital (grant no. MK297), by the Competitive State Research Financing of the Expert Responsibility Area of Tampere University (grant no. 9X029), and by the Finnish Thyroid Association.
Ethical aspects
The study was undertaken in accordance with the Declaration of Helsinki. Due to the retrospective nature of the study, no informed consent from the patients was acquired. The ethics committee of the Pirkanmaa Hospital District reviewed and approved the study protocol.