
Abstract
Background and objective:
Stoma site marking is an important factor in reducing stoma-related complications, thereby influencing the long-term quality of life in the elective setting. The impact of preoperative stoma site marking in emergency stoma creation is largely unknown. We aimed to determine whether preoperative stoma site marking in emergency stoma creation reduces stoma-related complications.
Methods:
Patients who underwent emergency stoma creation at our hospital between 2009 and 2022 were examined by reviewing our prospective database and retrospective chart review. Subjects were classified into the “marking (+)” or “marking (−)” group according to stoma site marking (194 and 151 patients, respectively). The changes in the frequency of stoma marking over time and the effects of stoma marking on stoma-related complications were analyzed.
Results:
The overall frequency of grade 2 or higher stoma-related complications was lower in the marking (+) group than in the marking (−) group (24% versus 36%, p = 0.010). Stoma site marking was associated with fewer soma site bleeding (2% versus 10%, p < 0.001), and the frequency of peristomal dermatitis was also lower (10%) in the marking (+) group (versus 18%, p = 0.042). Moreover, the lack of stoma site marking was an independent risk factor for overall stoma-related complications (adjusted odds ratio: 1.69, p = 0.034).
Conclusions:
Preoperative stoma site marking was associated with stoma-related complications in emergency surgery. The clinical significance of our attempt is worth validating with prospective studies.
Context and Relevance
Little is known about the significance of stoma site marking in emergency surgery. We have made efforts to increase the rate of stoma marking prior to emergency surgery over the last decade. In this original study, occurrences of grade 2 or higher stoma-related complications were decreased in patients that underwent marking of the stoma site before emergency surgery, with the lack of stoma marking a predictor of complications. Therefore, preoperative marking is beneficial for patients who receive emergency stoma surgery. The clinical significance of our attempt is worth validating with further studies, for example a cluster randomized multicenter trial.
200-character summary
Preoperative stoma site marking in emergency surgery reduced stoma-related complications ⩾ grade 2 in this single-center retrospective cohort study (n = 345) and although demanding, should be attempted.
Introduction
Intestinal ostomy creation is indicated for various bowel conditions including cancer, inflammation, trauma, and impaired anal sphincter function as well as systemic conditions such as poor nutrition and frailty to provide a diversion for the elimination of feces and intestinal effluent. Many guidelines recommend that patients scheduled for ostomy surgery should have the stoma site preoperative marked by experienced medical staff such as wound ostomy and continence (WOC) nurses.1–4 In previous reports, the lack of stoma site marking as well as clinical factors, including age, obesity, primary disease, and loop colostomy, were often listed as complication risk factors after ostomy surgery.5–10 In addition, several reports identified associations between emergency surgery and stoma-related complications by univariate or multivariate analyses.5–8,11,12 A recent meta-analysis also showed that stoma site marking might reduce the risk of stoma-related complications. 13 Intensive interdisciplinary care before emergency surgery is essential to provide optimal care for stoma patients. However, due to limited time and staff, stoma site marking may not be routinely performed before emergency surgery. 14 This constraint is reflected in the preoperative stoma marking rate in this setting, which ranges from 0% to 15.5%.6,15,16 Currently, there has been little research available on the clinical significance of stoma site marking before emergency surgery.
Over the last decade, we made efforts to conduct preoperative stoma site marking in patients receiving emergency surgery at our institute, if time permitted. The aim of the present study was to investigate whether stoma site marking was beneficial for patients who underwent emergency stoma formation.
Methods
Patients
Among emergency surgeries for the lower gastrointestinal tract excluding appendectomy performed at the University of Tokyo Hospital between January 2009 and December 2022, we retrospectively examined consecutive patients who underwent emergency stoma creation with, or without other surgical procedures by reviewing our prospective database. We excluded patients who received stoma site marking for planned elective surgery but underwent emergency surgery due to sudden symptomatic changes, those who waited more than 24 h for emergency surgery, and those who underwent re-creation of stoma. Patients who died within 28 days after surgery were also excluded. Patients were then classified into the “marking (+)” or “marking (−)” group according to preoperative stoma site marking.
This study was conducted with the approval of the ethics committee of the University of Tokyo Hospital (reference number: 3252-15). All patients gave a general consent for their data being stored in our database and being used for research purposes. The opportunity to opt-out was also offered to the patients.
Stoma site marking and postoperative stoma care
At our hospital, determining the stoma site and counseling are commonly included in the preoperative work-up for all patients who undergo elective stoma surgery. From 2009, we offered preoperative stoma site marking to patients undergoing emergency stoma surgery when possible. Principally, WOC nurses and/or trained nurses who completed an authorized stoma care training program, perform the stoma site marking procedures according to published guidelines.1,2 Briefly, the abdomen is examined in various positions including standing, sitting, and lying. After the rectus muscles are identified, four candidate sites are chosen that are visible to the patient and 2 inches from the imaginary surgical incision, then are marked with a marking pen. These marked sites together with the distances between them and key landmarks are recorded using a worksheet (Fig. 1A). The stoma marking procedure takes about 20 min. After stoma sites were marked, both abdomen photos and worksheet were stored in the medical chart. A representative marking in an emergency case is shown in Fig. 1B.
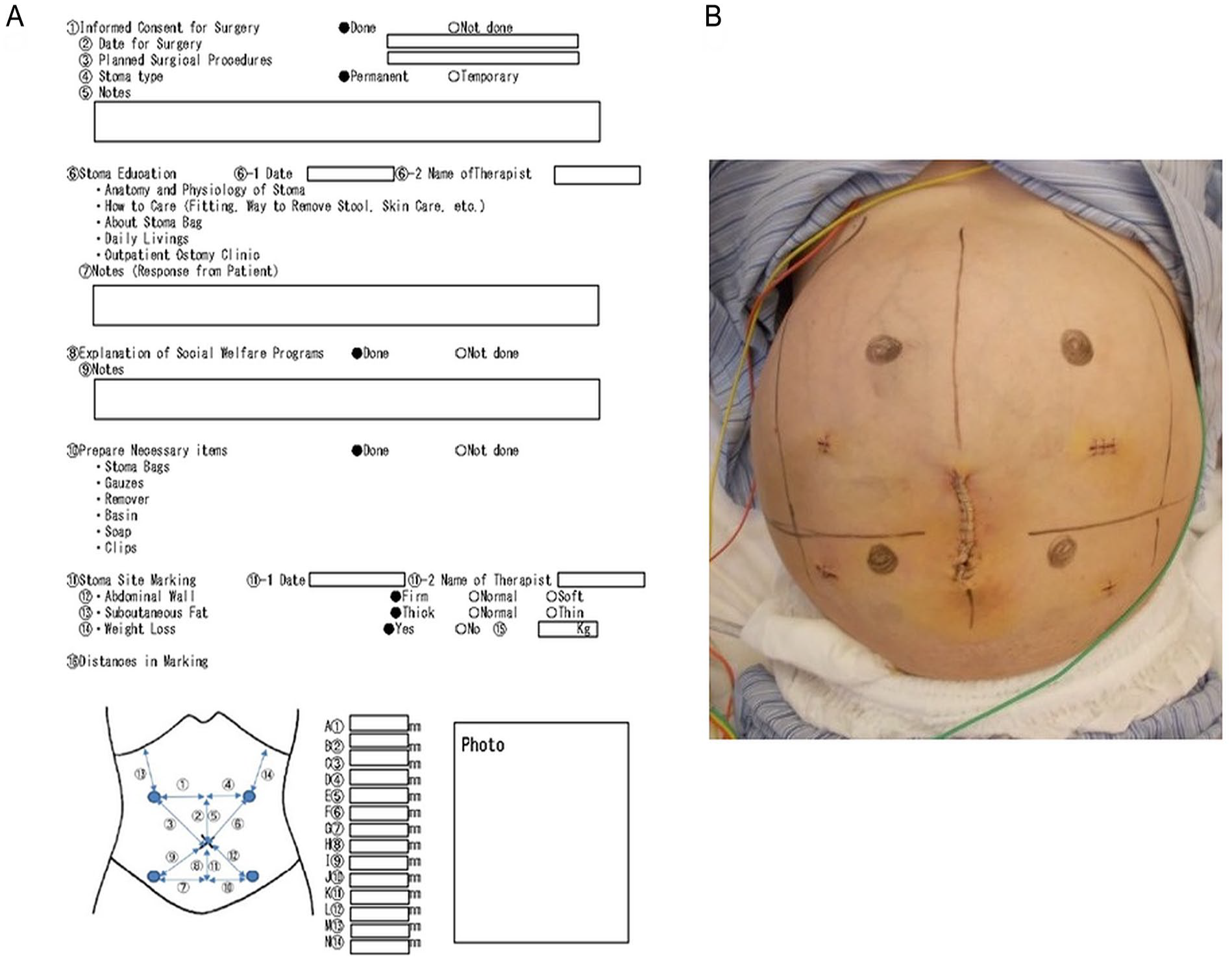
Preoperative stoma site marking: (A) Worksheet for stoma site marking used for both elective and emergency stoma surgeries in our hospital (modified from the original version written in Japanese). (B) An example of marking in a male patient undergoing emergency stoma creation for anastomotic leakage. Four stoma sites were marked with a marking pen on the distended abdomen due to fluid retention.
Follow-up consultations were performed in the ward and at an ostomy clinic every 2 weeks to 6 months after discharge. The interval depended on the patient’s condition. WOC nurses consulted gastrointestinal surgeons when necessary.
Data collection
Patient demographics, social, and clinical parameters are registered in our prospectively collected database in Microsoft Excel. For each patient, data are entered in the database immediately after they are confirmed. The data retrieved by the first author were sex, age, American Society of Anesthesiologists Physical Status (ASA-PS), comorbid disease, body mass index (BMI), drinking and smoking habits, preoperative serum hemoglobin and albumin levels, causative disease requiring urgent stoma creation, operative time, stoma site, stoma type, surgical approach, and surgical procedures other than ostomy, estimated blood loss, and blood transfusion during surgery. Marital status (married or unmarried) and starting time of operation (daytime from 8:00
Statistical analysis
Categorized data were compared by Fisher’s exact test or the chi-square test, with continuous variables compared by the unpaired t or Wilcoxon’s test. Predictive factors of stoma-related complications were identified by univariable logistic regression analysis, carried out for each explanatory variable. Here, age, hemoglobin, and albumin levels were dichotomized by their mean values (63.8 years, 11.2 g/dl, and 3.0 g/dl, respectively), and the stoma site was dichotomized into colon versus ileum or jejunum, then stoma type into end versus loop or double-barreled. Based on BMI, patients were divided into “underweight” (BMI < 18.5), normal weight (18.5 ⩽ BMI < 25.0), and “overweight/obese” (BMI ⩾ 25.0). Variables with a p-value < 0.05 were subsequently used in a multiple logistic regression model. All analyses were performed using JMP software version 16.2.0 (SAS Institute Inc., Cary, NC, USA), and associations were considered significant when the p < 0.05.
Results
Study cohort
During the study period, 407 emergency surgeries for the lower gastrointestinal tract excluding appendectomy were performed at our department. Among them, 356 patients required a temporary or permanent stoma. Of these, three patients were excluded, one due to emergency stoma surgery after stoma site marking for planned elective surgery and the other two due to stoma re-creation. Eight patients died within 28 days after emergency stoma surgery. After excluding these patients, a total of 345 patients were included in the following analyses (Fig. 2).
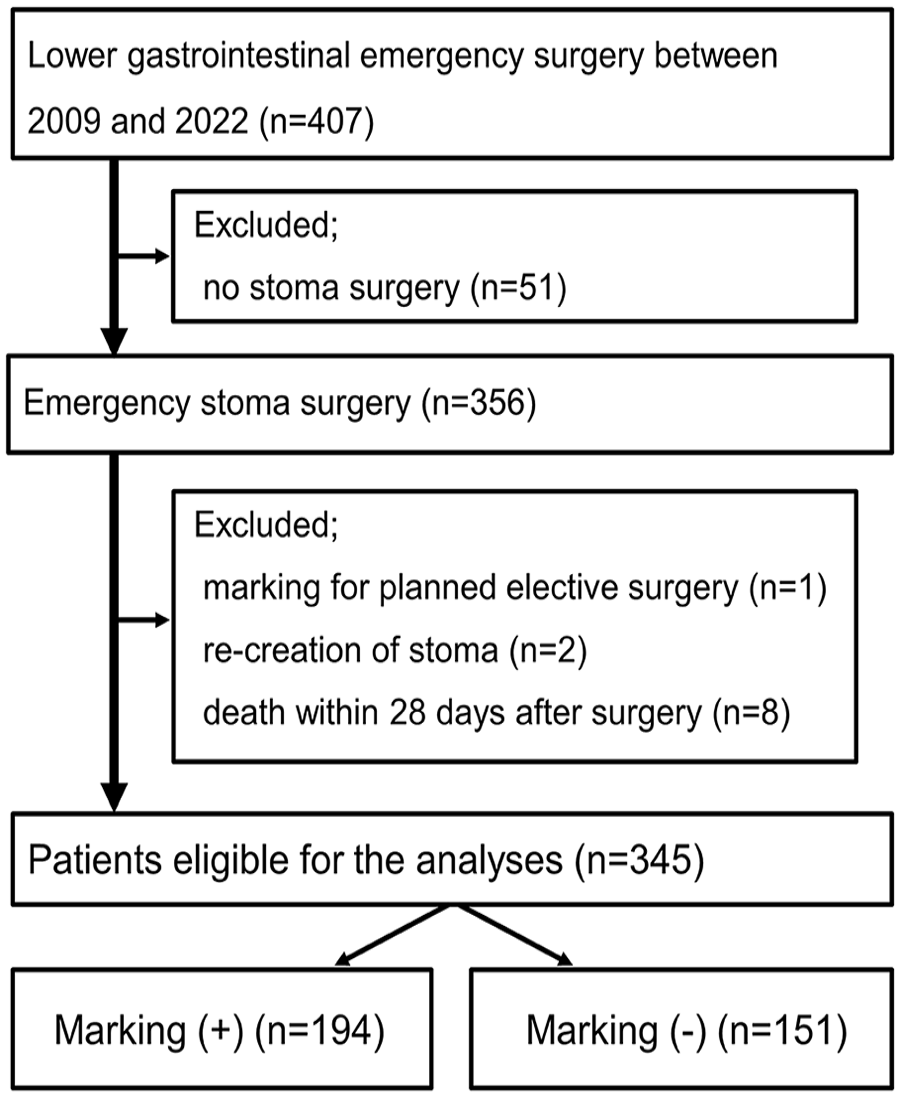
Flowchart of selecting study subjects.
Temporal changes in the frequencies of stoma site marking before emergency surgery and overall stoma-related complications
The study cohort comprised 207 men and 138 women, with 194 patients (56%) receiving preoperative stoma site marking, forming the marking (+) group. The annual frequencies of preoperative stoma site marking are shown in Fig. 3. The frequency of stoma site marking increased over time. Initially, the frequency was 24% for the early period (2009-2015) and 74% for the late period (2016-2022, p < 0.001). The annual rate of overall stoma-related complications fluctuated during the study period (Fig. 3).
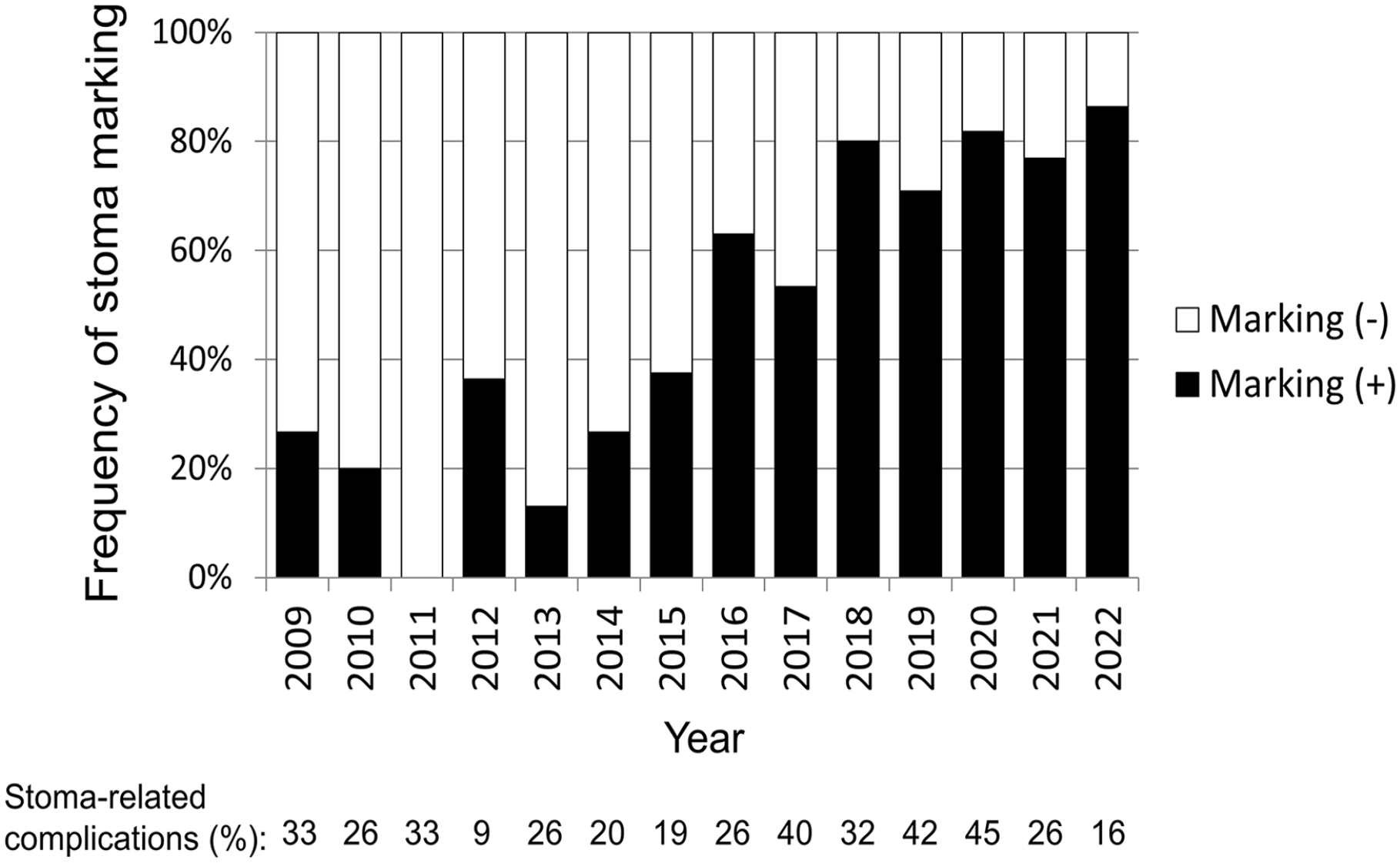
Annual rates of preoperative stoma site marking and stoma-related complications of grade 2 or higher in emergency stoma surgery.
Background profile comparisons between patient groups classified by stoma site marking
Table 1 displays patient characteristics in the marking (+) and marking (−) groups. Patients in the marking (+) group were younger than those in the marking (−) group (mean: 61.1 versus 66.9 years old, p < 0.001). An ASA-PS of 3 or 4 was more common in the marking (−) group (57%) than in the marking (+) group (31%). The marking (−) group comprised more patients with diabetes (22%) than the marking (+) group (13%). In addition, preoperative hemoglobin level was lower in the marking (+) group than in the marking (−) group by 0.6 g/dl (p = 0.033). There were disproportions in causative diseases (p < 0.001), with bowel obstruction and refractory ulcerative colitis more frequent in the marking (+) group, and patients with perforation more likely in the marking (−) group. In terms of perioperative parameters, a laparoscopic approach was used more frequently in the marking (+) group (25% versus 5%, p < 0.001), and estimated blood loss during the operation was smaller in the marking (+) group than in the marking (−) group (median: 40 ml versus 145 ml, p < 0.001). Intraoperative blood transfusion was more frequent in the marking (−) group (42% versus 24%, p < 0.001). The other clinicopathological and social parameters were similar between the two groups.
Profile of patients according to preoperative stoma site marking.
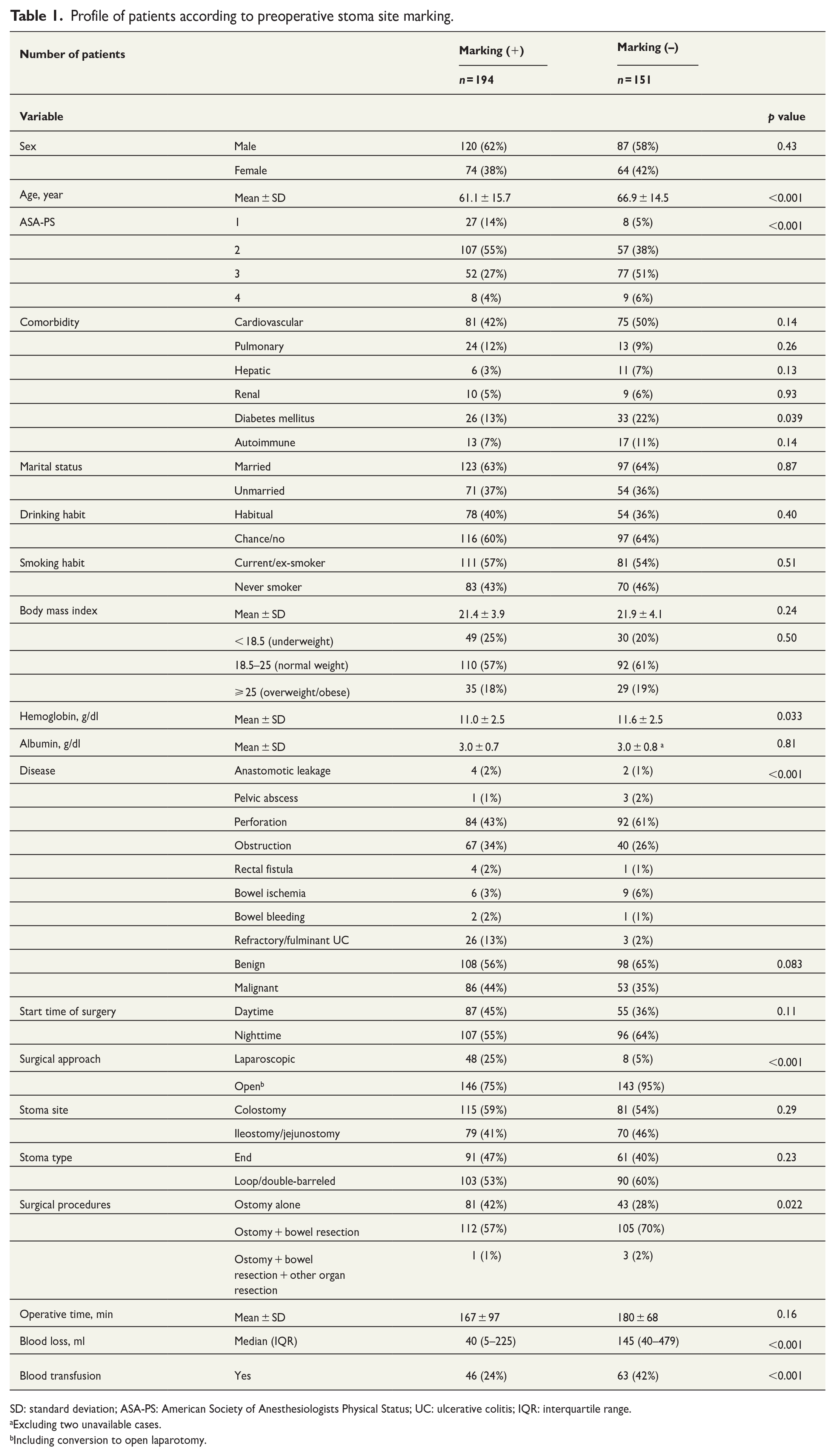
SD: standard deviation; ASA-PS: American Society of Anesthesiologists Physical Status; UC: ulcerative colitis; IQR: interquartile range.
Excluding two unavailable cases.
Including conversion to open laparotomy.
Comparisons of stoma-related complications between patient groups classified by stoma site marking
The median follow-up period for the whole cohort was 474 days, which was similar between the marking (+) and marking (−) groups (median: 428 days and 604 days, respectively, p = 0.11). Patients in both groups had a stoma for a similar duration in the current analysis (median: 164 days and 206 days, respectively, Table 2).
Stoma-related complications per consultation at outpatient ostomy clinic according to stoma site marking.
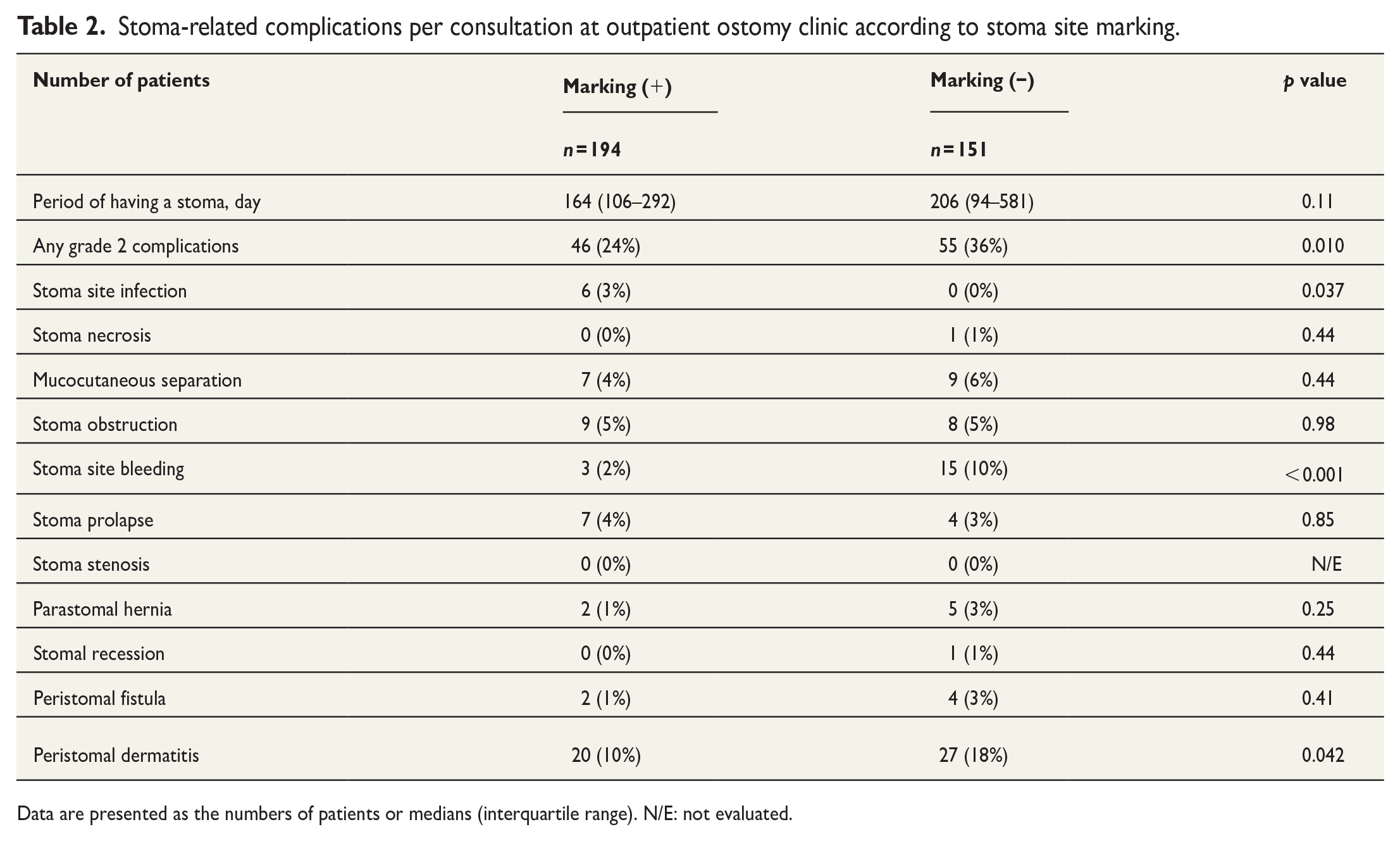
Data are presented as the numbers of patients or medians (interquartile range). N/E: not evaluated.
As shown in Table 2, the overall rate of stoma-related complications of grade 2 or higher was 24% in the marking (+) group and 36% in the marking (−) group (p = 0.010). Stoma bleeding was less frequent in the marking (+) group than in the marking (−) group (2% versus 10%, p < 0.001). Peristomal dermatitis, the most frequent complication in both groups, occurred less in the marking (+) group (10%) than in the marking (−) group (18%, p = 0.042). Stoma site infection was only observed in a few patients of the marking (+) group (3%). There was no significant intergroup difference for other complications.
Risk factors of stoma-related complications after emergency stoma surgery
We analyzed risk factors for overall stoma-related complications of grade 2 or higher in patients who underwent emergency stoma surgery. Table 3 shows the results regarding predictive factors on univariate and multivariate analyses. Lack of stoma site marking was associated with stoma-related complications with an unadjusted odds ratio of 1.84 (p = 0.011). From multivariate analysis, female sex (odds ratio: 1.88, p = 0.012), small bowel ostomy (odds ratio: 2.11, p = 0.003), loop or double-barreled stoma (odds ratio: 1.75, p = 0.028), and lack of stoma site marking (odds ratio: 1.69, p = 0.034) were identified as independent predictive factors of stoma-related complications.
Univariate and multivariate analyses of predictive factors of grade 2 or higher stoma-related complications.
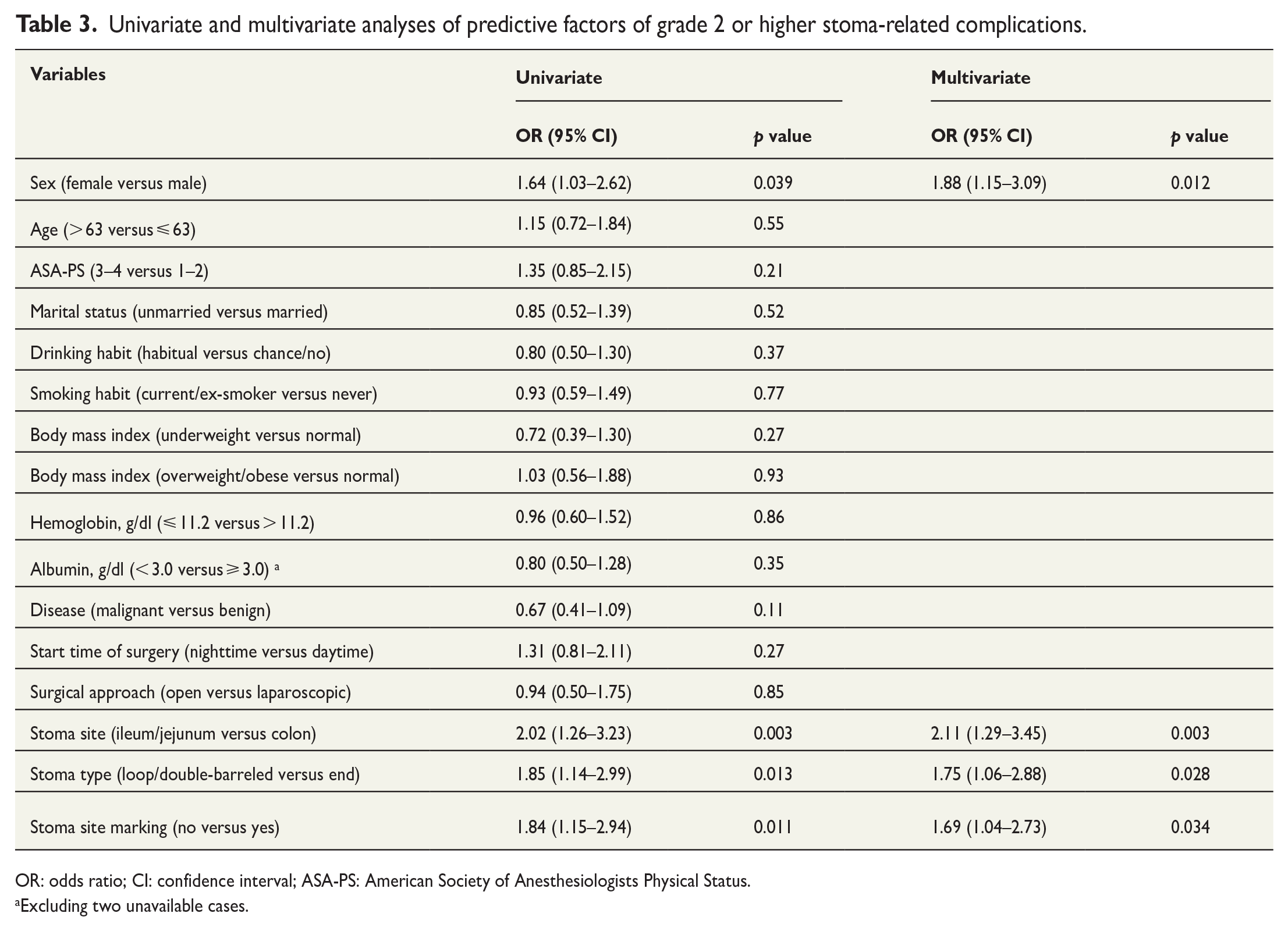
OR: odds ratio; CI: confidence interval; ASA-PS: American Society of Anesthesiologists Physical Status.
Excluding two unavailable cases.
Comparisons of stoma-related complications between patient groups classified by stoma site and type
Since the stoma site and type were independently associated with stoma-related complications, we compared overall and individual complications between colostomy and small bowel ostomy and between end stoma and loop/double-barreled stoma.
As shown in Table S1, the overall rate of stoma-related complications of grade 2 or higher was 23% for colostomy and 38% for small bowel ostomy (p = 0.003). Parastomal hernia was frequent in colostomy. On the other hand, patients with ileostomy/jejunostomy were more likely to develop a stoma obstruction and peristomal dermatitis.
As shown in Table S2, the overall rate of stoma-related complications of grade 2 or higher was 22% for end stoma and 35% for loop/double-barreled stoma (p = 0.012). However, there were no significant intergroup differences for individual complications.
Discussion
The significance of stoma site marking in emergency surgery was largely unknown due to a limited literature. In the current retrospective cohort study, we analyzed 345 patients who underwent emergency stoma surgery, and found that lack of preoperative stoma marking was a predictive factor for overall stoma-related complications in this setting.
Previous reports documented reductions in stoma-related complications by preoperative stoma site marking by stoma specialists. However, these studies generally investigated stoma complication risk factors using elective surgery cohorts or combined cohorts of elective with emergency surgeries.5–10,13,20,21 The clinical significance of stoma site marking specifically in emergency stoma creation was not extensively addressed as only a small population received stoma marking prior to emergency surgery. The effects of preoperative stoma site marking on postoperative complications were investigated by analyzing exclusively patients who received urgent ostomy formation. The current study clearly demonstrated reduced stoma-related complications in emergency surgery with preoperative stoma site marking, in accordance with reports that focused on elective stoma surgery.5–10,20,21
In the cohort studied, stoma site bleeding was significantly reduced by preoperative stoma site marking. There is little existing literature on the direct causal relationship. The causes of stoma bleeding are multi-factorial, including inadequate hemostasis during stoma construction and stoma-related complications such as granuloma, ulcer, and peristomal irritated skin. 22 Systemic conditions such as portosystemic shunts creating varicose veins at the mucocutaneous junction4,23 and hypocoagulation state22,24,25 may contribute to stoma bleeding. Moreover, suboptimal stoma configurations make stoma bag fitting difficult, resulting in mechanical injuries and bleeding.22,24 Contrary to these speculations, the difference in the frequency of stoma bleeding might be a coincidence. More research is required to clarify why stoma site marking leads to the prevention of stoma bleeding in emergency settings.
Peristomal dermatitis was the most frequent complication in the current study, in line with a previous study on ostomy-related complications after emergency surgery. 26 Stomal complications may lead to a poor quality of life. 21 As stoma site marking decreased peristomal dermatitis to some extent, in addition to stoma bleeding, our results underscore the importance of preoperative stoma site marking for emergency cases.
Stoma site infection was observed only in patients of the marking (+) group. However, the percentage was as low as 3%. Moreover, there is no literature on the association between stoma site marking and stoma infection. Thus, further investigation is warranted to address this issue, although it may be attributed to a type I error.
The rate of stoma site marking prior to emergency surgery increased over time at our hospital. During the study period, the introduction of the laparoscopic approach coincided with this. The reduced blood loss and blood transfusion during operation may be partly attributable to the frequent minimally invasive surgery in the marking (+) group.
The rate of stoma-related complications did not decrease considerably over the years (Fig. 3). Although the multivariate analysis indicated lack of stoma site marking as an independent risk factor for overall stoma-related complications, there may be other confounders affecting the results such as follow-up period, period with a stoma, and other continuous parameters (age, BMI, hemoglobin, and albumin) that were analyzed as dichotomized or trichotomized variables in the current study.
The current study also revealed that small bowel ostomy, loop/double-barreled stoma, and being female were independent risk factors for stoma-related complications in emergency surgery. We and other groups showed that ileostomy is associated with frequent early complications represented by peristomal dermatitis.27–29 Lindholm et al. 26 also reported that peristomal skin problems were more common in patients with end or loop ileostomy than in those with colostomy after emergency abdominal surgery. However, loop colostomies out of all stoma configurations had reportedly the highest rate of complications except for stoma obstruction, 23 as they tend to be larger and sometimes more difficult manage. There are conflicting results regarding sex as a risk factor for stoma-related complications among reports; one systematic review demonstrated that being a woman was an independent factor for an increased likelihood of stoma complications, 10 whereas Arolfo et al. 6 reported that male patients had an odds ratio of 1.3 for these complications. The role of stoma configuration and sex in developing stoma-related complications remains to be investigated by further studies.
Stomas created in emergency surgery are likely to be permanent; for example, Den Dulk et al. 30 reported that primary (elective) ostomies in rectal cancer patients were closed significantly more often than secondary ostomies created in emergency situations (86% versus 49%, p < 0.0001). In several reports, stoma creation is likely to be performed by resident doctors or general surgeons.7,31 Stoma surgery at an improper site may be associated with significant lifelong morbidities. 1 In this regard, a past report stated that specialist colorectal surgeons should advise non-specialists on how to reduce stoma-related complications in colorectal emergencies. 12 At our institute, colorectal surgeons routinely perform stoma creation or supervise non-specialist surgeons to create a stoma to minimize complications.
The findings of the current study are limited by its observational nature. This is a retrospective study, but randomization of stoma site marking is difficult in emergency settings. Not only clinicopathological parameters but also several social factors were addressed; however, other factors, such as income and education, were not analyzed. Differences were noted in age, distribution of ASA-PS, number of diabetic patients, causative disease (e.g. perforation), and surgical procedure between the two groups, suggesting that patients with more severe conditions underwent emergency surgery without stoma marking, resulting in an increased rate of stoma-related complications. On the other hand, advances in stoma care during the relatively long study period may have contributed to preventing stoma-related complications in patients receiving stoma site marking. Fewer minimally invasive approaches in the marking (-) group may have affected the disparities in outcomes. Patients who underwent elective surgery without preoperative stoma site marking, especially other than colorectal surgery, and received stoma formation by intraoperative judgment were not included. Furthermore, we could not assess whether surgeons created the stoma at the exact site marked preoperatively. However, preoperative site markings are a guide, 1 and in our opinion, the final stoma site selection should be made by the surgeons who inspect the conditions of the bowels, mesenteries, and peritoneum in the abdominal cavity. We evaluated the stoma conditions in the ward and at our ostomy clinic, but not at home or in other clinics. The proportion of patients with BMI ⩾ 25 was rather low in the current cohort, which may hinder the application of the current findings in the western countries with much higher percentages of overweight or obese population. Finally, the median period with a stoma was around six months; thus late complications, typified by parastomal hernia and stoma prolapse, must be re-evaluated by a longer follow-up.
Conclusions
Our results suggested that stoma site marking reduces early stoma-related complications after emergency surgery. It is demanding to introduce stoma site marking prior to emergency stoma surgery as a routine procedure. Our findings deserve further validation with prospective studies.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969231186282 – Supplemental material for Preoperative stoma site marking reduces postoperative stoma-related complications in emergency surgery: A single center retrospective cohort study
Supplemental material, sj-docx-1-sjs-10.1177_14574969231186282 for Preoperative stoma site marking reduces postoperative stoma-related complications in emergency surgery: A single center retrospective cohort study by Hiroaki Nozawa, Sanae Sasaki, Chieko Hayashi, Akiko Kawasaki, Kazuhito Sasaki, Koji Murono, Shigenobu Emoto and Soichiro Ishihara in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors thank Medical English Service (Kyoto, Japan) for editing manuscript.
Author contributions
H.N. built study design. H.N., S.S., C.H., and A.K. contributed to collection and analysis of the data. S.S., C.H., and A.K. were involved in stoma care of patients as WOC nurses. H.N., K.S., K.M., S.E., and S.I. were involved in the surgical treatment of patients. H.N. wrote the draft of manuscript. S.S., C.H., A.K., K.S., K.M., S.E., and S.I. reviewed and revised the manuscript. All authors participated in final approval of the manuscript.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.