
Abstract
Background and objective:
Some colorectal surgeons advocate routine splenic flexure mobilization (SFM) when performing anterior resection for rectal cancer to ensure a tension-free anastomosis. Meta-analyses of smaller studies suggest that this approach does not influence anastomotic leakage rates, but larger multicentre studies are needed to confirm the safety of a selective strategy. The aim of this study is to evaluate the impact of SFM on anastomotic leakage.
Methods:
This is a retrospective multicentre cohort study, comprising 1109 patients operated with anterior resection for rectal cancer in 2014–2018. Exposure was SFM, while anastomotic leakage within a year constituted the outcome. Stratified analyses were performed for type of mesorectal excision and surgical approach, as well as sensitivity analysis considering vascular tie placement. Multivariable Cox regression with hazard ratios (HRs) and 95% confidence intervals (CIs) was employed to adjust for confounding, while multiple imputation was used for missing data.
Results:
SFM was performed in 381 patients (34.4%). Anastomotic leakage occurred in 83 (21.8%) and 123 (20.3%) patients operated with and without SFM, respectively. SFM was neither clearly detrimental nor beneficial regarding anastomotic leakage (adjusted HR = 0.82; 95% CI: 0.59–1.15), with no apparent differences for total or partial mesorectal excision and minimally invasive or open surgery. Concurrent high vascular ligation did not impact these results, and there was no evidence of interaction from centers with a more common use of SFM.
Conclusions:
SFM did not seem to influence the risk of anastomotic leakage after anterior resection for rectal cancer, regardless of type of mesorectal excision, use of minimally invasive surgery, or high vascular ligation.
Introduction
Splenic flexure mobilization (SFM) has long been considered a mandatory step in anterior resection for rectal cancer. 1 However, this concept has been challenged, especially since the advent of minimally invasive surgery; 2 others would argue that SFM as a first step is especially suited for a laparoscopic approach. Proponents argue that SFM ensures a tension-free, well-vascularized redundant colon to fill the pelvis, while the counterarguments revolve around increased operative trauma and operation time, risk of intraoperative complications, not the least including the risk of colonic necrosis after central ligation of the inferior mesenteric artery. 3 While gain of colonic length with SFM and concurrent central ligation has been proven comprehensively, 4 neither SFM 5 nor high tie surgery 6 has been shown to be clearly related to anastomotic leakage. While high ligation has been evaluated in several randomized clinical trials, SFM has not been subject to controlled experiments. Meta-analysis data of observational studies, mostly small or otherwise from administrative databases without detailed data, suggest that anastomotic leakage does not differ between groups operated with and without SFM. 5 However, up-to-date studies with more widespread uptake of minimally invasive surgery are sparse, in particular using proper leakage definitions and including even delayed leaks. The latter is especially important, as population-based studies suggest a 10%–20% leak rate after anterior resection;7,8 many leaks tend to be diagnosed a long time after the index surgery, not the least when patients are defunctioned.8,9 In addition, SFM with and without central vascular ligation has seldom been formally studied with respect to leakage. Here, we present a multicentre cohort study from an unselected population, with the aim to evaluate whether SFM decreases the risk of anastomotic leakage in anterior resection for rectal cancer.
Method
Checklist for the reporting of observational studies
This article was written in accordance with the Strengthening The Reporting of Observational Studies in Epidemiology (STROBE) checklist for the reporting of observational studies. 10
Study design
This is a retrospective multicentre cohort study, conducted in 11 centers in Sweden. Patients operated with anterior resection for rectal cancer during the years 2014–2018 were identified at each hospital from theater lists or registry data. Patients operated with a Hartmann’s procedure (with end colostomy) were not included, while patients operated with a transanal total mesorectal excision (TME) were excluded. Chart review was performed at each site and data on pertinent perioperative variables were entered into a RedCap database (Vanderbilt University, Nashville, TN, USA). The RedCap system is a secure web application for building and managing online surveys and databases. 11 This database was then linked to the Swedish Colorectal Cancer Registry (SCRCR), ensuring that all enrolled patients had a rectal cancer diagnosis as well as providing additional information such as demographics, tumor stage and height, preoperative treatment, and additional perioperative data. Inclusion rates were subsequently described for each hospital. The SCRCR is a national registry 12 that defines rectal cancer as an adenocarcinoma of the large bowel within 15 cm of the anal verge, as measured by rigid sigmoidoscopy. The SCRCR has been validated with an average completeness of 99% and overall agreement between registry and re-abstracted variables at 90% for the period 2008–2015. 13
Exposure
Information on SFM and vascular ligation levels was derived from the operative note. The main exposure constituted SFM as extracted from charts, while a more refined approach was used in a sensitivity analysis. Here, a partial SFM was considered as a reported SFM but with one or both of the inferior mesenteric artery and vein ligated peripherally. A full SFM was considered as such, in contrast, only when both vessels were ligated centrally and an SFM was reported in the note. This partition was made to reflect the gain of colonic length as a consequence of high vascular ligation. 4
Outcome
The primary outcome was any anastomotic leakage within 12 months of the index surgery. Leakage was defined according to the consensus definition provided by the International Study Group of Rectal Cancer: 14 anastomotic leakage is defined as a defect of the intestinal wall integrity leading to a communication between the intra- and extraluminal compartments; it can be added that a pelvic abscess close to the anastomosis also signifies a leakage. The leaks are further classified: Grade A leaks require no change in patient management, Grade B leaks necessitate treatment other than reoperation, and Grade C leaks demand laparoscopy or laparotomy. Intraoperative splenic injury was a secondary outcome.
Statistical analysis
Frequency tables concerning patient characteristics, tumor stage, and operative details were constructed. Continuous variables were described using the median along with the interquartile range (IQR). Fisher’s exact test was used to test for associations in selected categorical comparisons. Log rank tests, stratified when appropriate, were employed to test for differences in survival curves. For descriptive purposes, study inclusion rates, SFM and leak rates, as well as the share of restorative surgery for each participating center were tabulated (using anterior resection as the denominator and all abdominal rectal cancer resections as the nominator); a figure visualizing SFM rates and use of minimally invasive surgery during the study period was also constructed.
A directed acyclic graph (Fig. 1) was used to depict the proposed causes and effects involved in the development of anastomotic leakage, constrained by available variables. 15 Considering the exposure SFM, the following covariates were selected in order to have a minimally sufficient adjustment set: American Society of Anesthesiologists’ (ASA) fitness grade (I, II, or III and IV), age (years; continuous), body mass index (BMI) (kg/m2; continuous), neoadjuvant therapy (none, radiotherapy, or chemoradiotherapy), operating hospital (categorical), operation year (categorical), sex (male or female), surgical approach (minimally invasive or open), and current smoking (yes or no). As the aim was to estimate the total effect, proposed mediators such as operation time and intraoperative bleed were not included as covariates. Multiple Cox regression models were subsequently constructed, producing unadjusted as well as adjusted estimates. Interaction terms formed by SFM and type of mesorectal excision as well as surgical approach were included, with the aim to estimate subgroup effects. Finally, sensitivity analyses were conducted. First, a predefined analysis was performed where the exposure SFM was subdivided into partial and full mobilization but otherwise retaining the same model as in the main analysis. Second, a post hoc analysis was carried out where hospitals with and without a more common use of SFM were compared, aiming to capture any effects from institutional experience or lack thereof of SFM. Third, only Grade B and C leaks were considered as the outcome, as Grade A does not impact the immediate postoperative management. Results are reported as hazard ratios (HRs) with corresponding 95% confidence intervals (CIs).
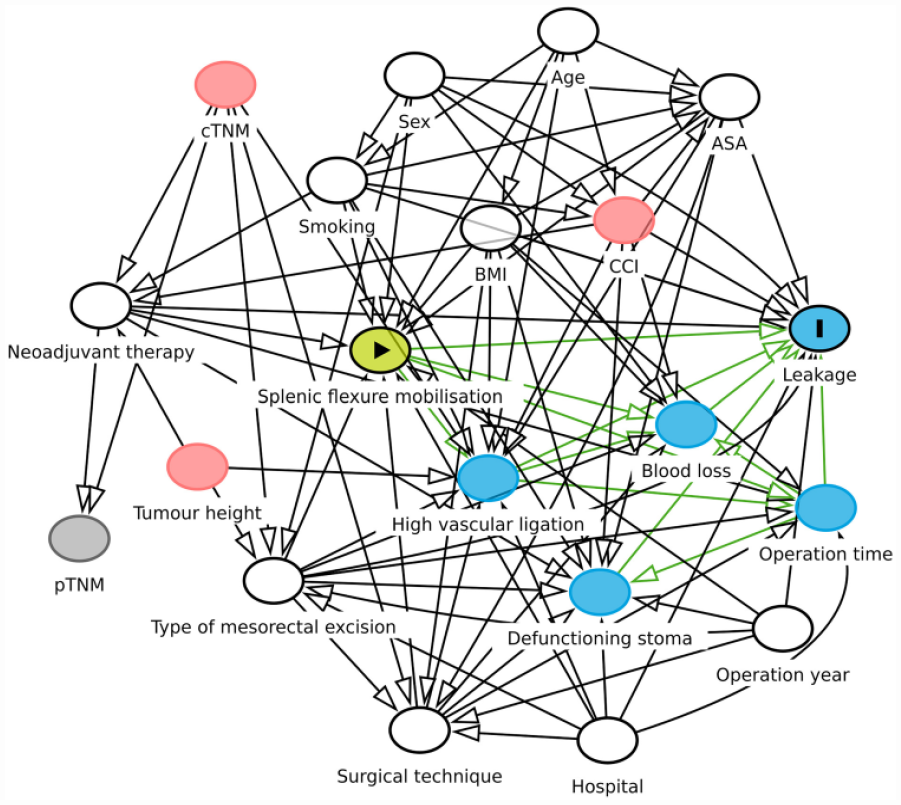
A directed acyclic graph depicting the assumed relationships between variables involved in the development of anastomotic leakage. SFM denotes exposure, while leakage denotes outcome. A minimal adjustment set to derive a total effect on the outcome from the exposure consists of variables such as ASA, age, BMI, operating hospital, operation year, sex, neoadjuvant therapy, surgical technique, and type of mesorectal excision.
Multiple imputation in 20 datasets estimated with chained equations was used to handle missing data. As imputation model, the variables in the Cox models were used together with the leak status variable and the Nelson–Aalen estimates of the cumulative hazard. 16 The analysis was performed in Stata version 17 (StataCorp LLC, College Station, TX, USA).
Results
Patients
After exclusion of patients with missing registration, erroneous diagnosis or procedure, 1109 patients remained for analysis. A study flowchart is presented in Fig. 2. Table 1 details the ratio of restorative surgery for each hospital, demonstrating a range from 32.6% to 55.8%. Anastomotic leakage within 12 months occurred in 230 patients (20.8%) of the cohort (two patients had missing data for leakage). Leakage was diagnosed on median postoperative day 16 (IQR: 7–41). Grade A, Grade B, and Grade C leaks occurred in 14.8%, 56.1%, and 29.1% of patients who sustained anastomotic leakage, respectively.
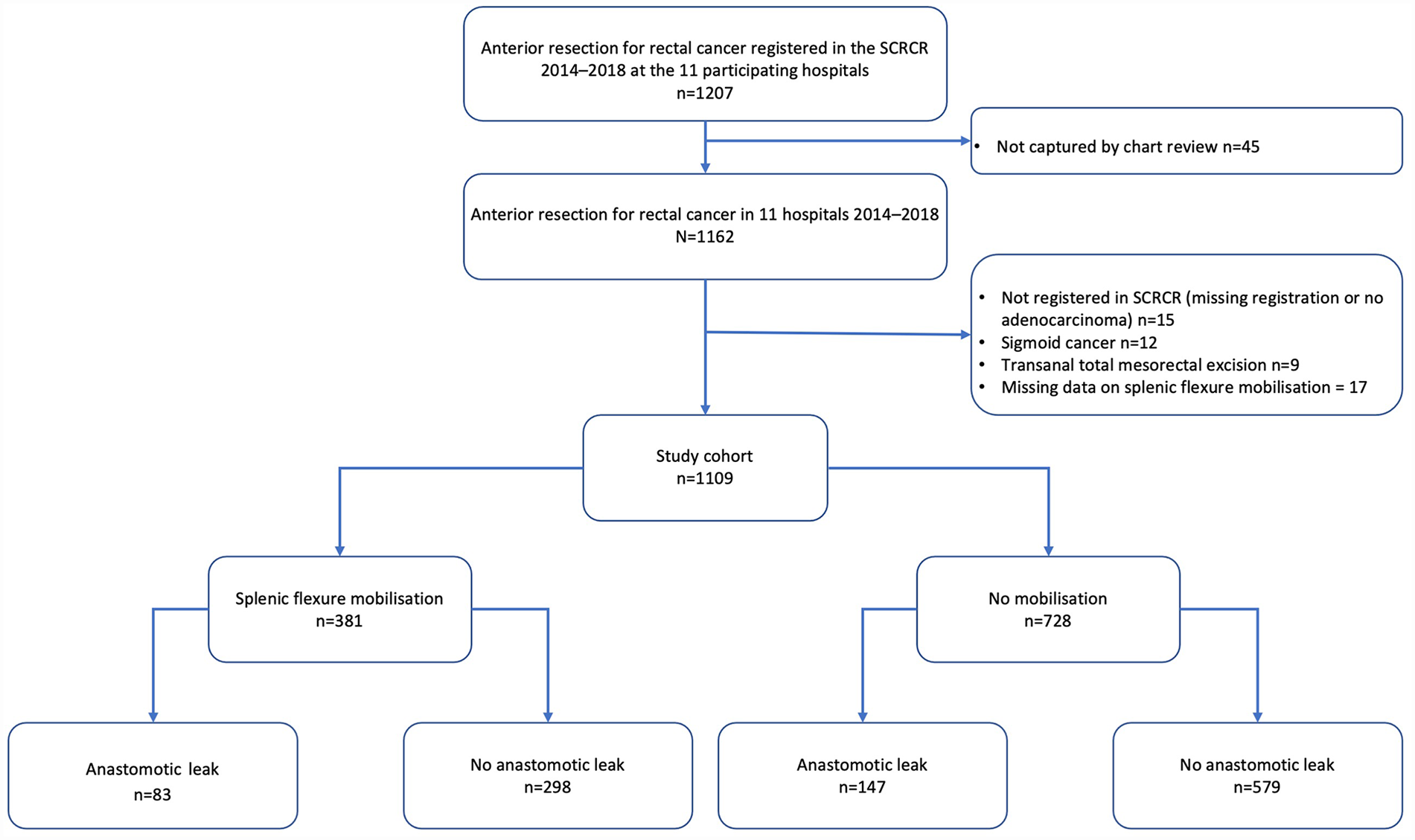
Study flowchart. Two patients in the no mobilization group had missing data for anastomotic leakage.
Rectal resections in the SCRCR per operating center during 2014–2018, inclusion rate in the present study, and leak rates stratified by SFM.
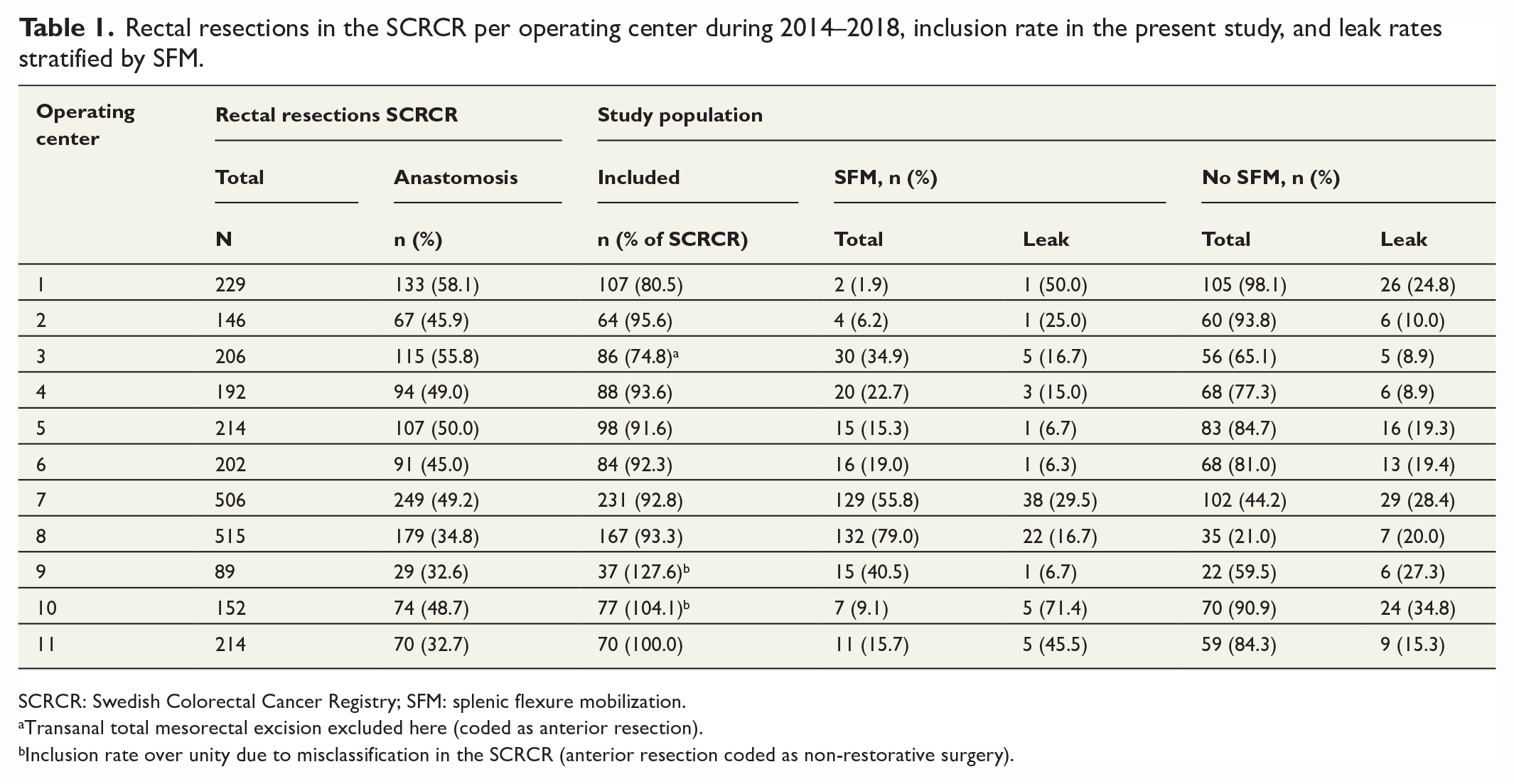
SCRCR: Swedish Colorectal Cancer Registry; SFM: splenic flexure mobilization.
Transanal total mesorectal excision excluded here (coded as anterior resection).
Inclusion rate over unity due to misclassification in the SCRCR (anterior resection coded as non-restorative surgery).
The demographic and clinical variables are presented in Table 2, stratified by SFM. Patients operated with SFM were more commonly men but had a similar degree of comorbidity; age and BMI were similarly distributed, but current smoking was more common in SFM patients. Individual operating center and a high hospital volume correlated well with SFM use (Table 1). No apparent difference in SFM use over the study period was seen. While clinical tumor stage was not distributed differently, neoadjuvant therapy, open approach, and TME surgery were more common in the SFM group. In addition, high ligations of the inferior mesenteric artery and vein as well as defunctioning stoma use were more common in the SFM group. Likewise, intraoperative bleeding and operation time were higher in SFM patients.
Baseline characteristics of 1109 patients operated with anterior resection for rectal cancer in 11 Swedish hospitals 2014–2018, stratified by splenic flexure mobilization.
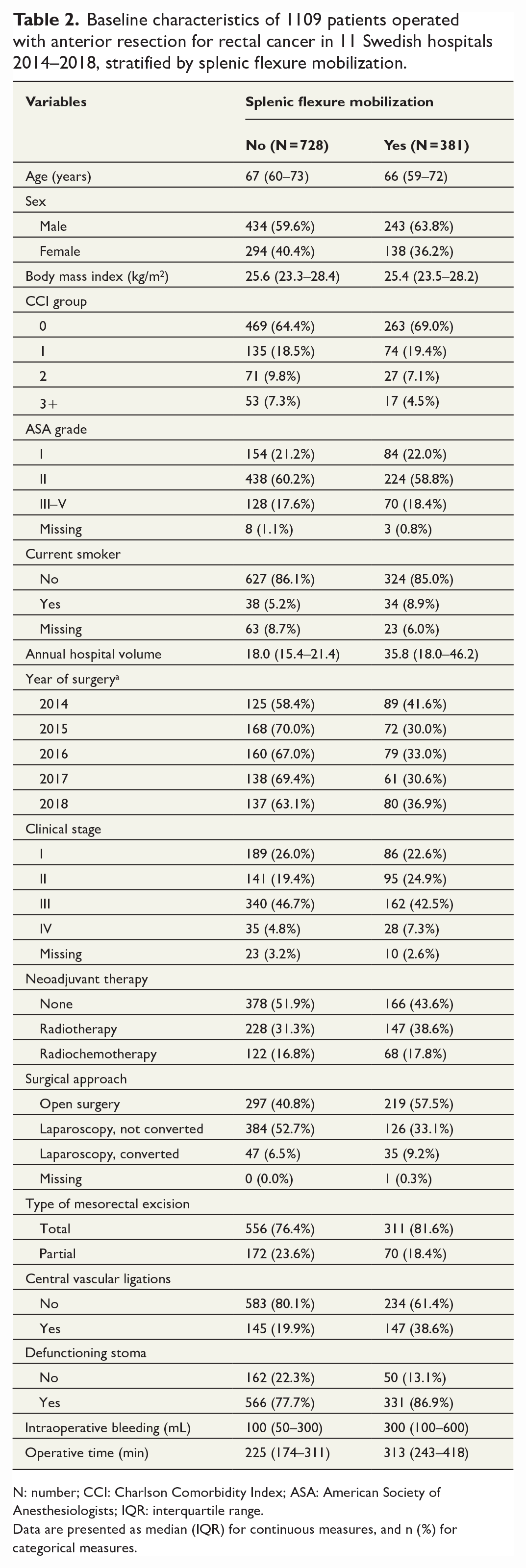
N: number; CCI: Charlson Comorbidity Index; ASA: American Society of Anesthesiologists; IQR: interquartile range.
Data are presented as median (IQR) for continuous measures, and n (%) for categorical measures.
In particular, SFM was used in 311 (35.9%) TME and 70 (28.9%) partial mesorectal excision (PME) patients, respectively. SFM was also performed in 161 (27.2%) and 219 (42.4%) patients who underwent minimally invasive and open surgery, respectively. Of note, 57.5% of cases in the minimally invasive group were robotic assisted; the SFM rates in these patients were similar to those operated with conventional laparoscopy (26.5% versus 28.6%). Fig. S1 demonstrates a gradual increase in minimally invasive procedures, while the SFM rates are stable.
Anastomotic leakage: primary outcome
Patients with SFM compared to patients without SFM had an anastomotic leakage rate within 12 months of 21.8% versus 20.3% (p = 0.59). This is visualized in a Kaplan–Meier curve in Fig. 3, where time to leakage was not statistically significantly different between groups (log rank test, p = 0.53). After adjustment for confounding, SFM compared to no SFM did not differ to a significant degree, with a HR of 0.82 (95% CI: 0.59–1.15; Table 3).
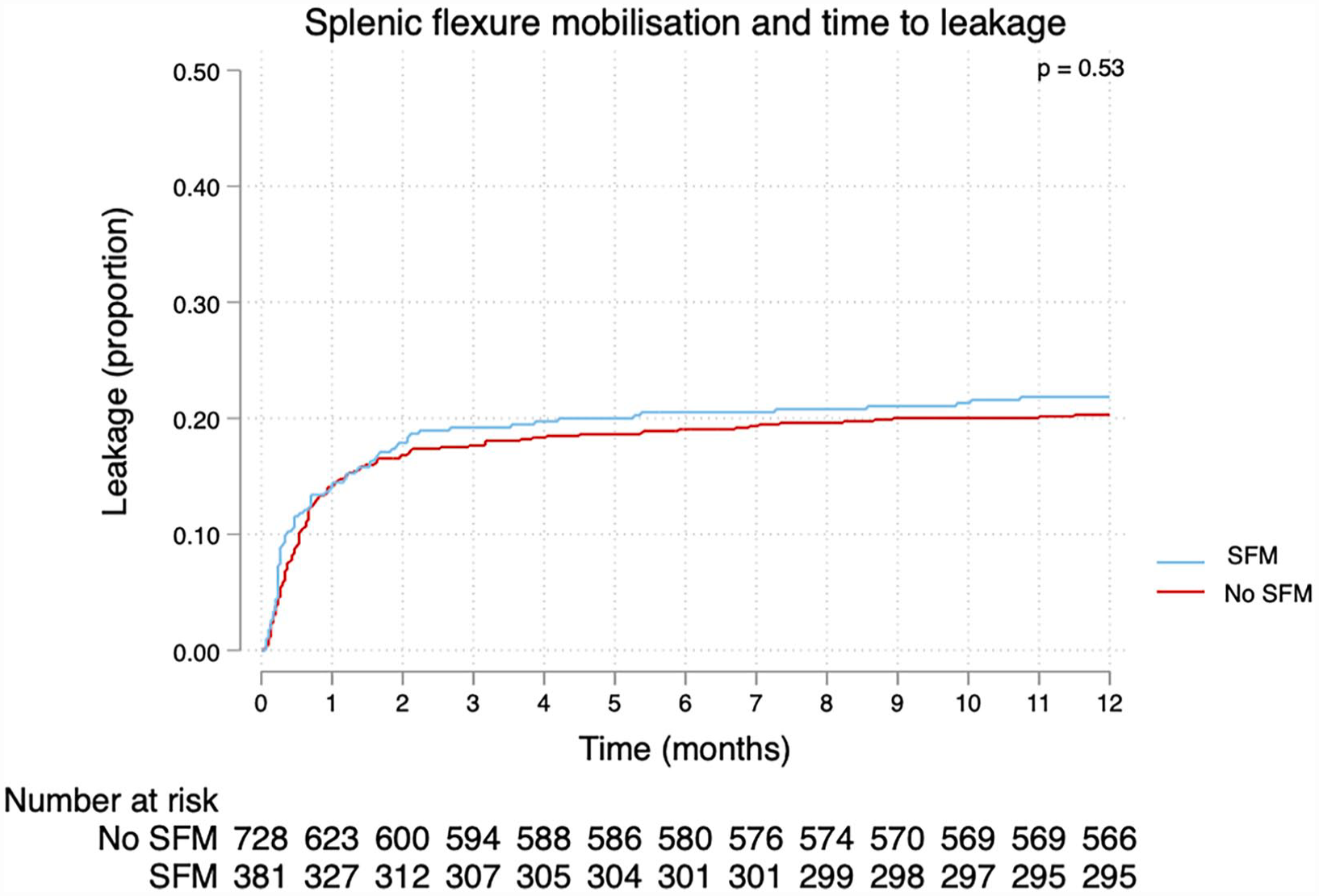
Kaplan–Meier curve depicting time to leakage as a function of splenic flexure mobilization (SFM) in 1109 patients operated with anterior resection for rectal cancer.
The risk of developing anastomotic leakage within 12 months after anterior resection for rectal cancer by SFM in 1109 patients.
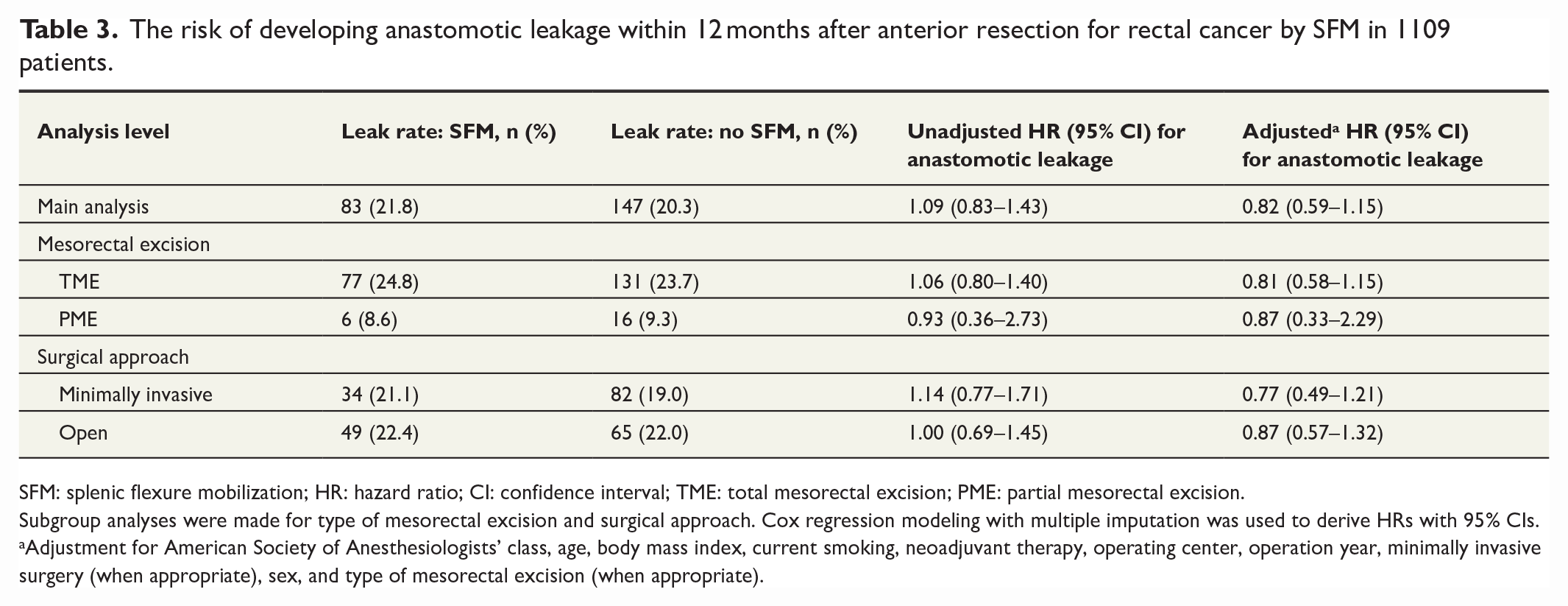
SFM: splenic flexure mobilization; HR: hazard ratio; CI: confidence interval; TME: total mesorectal excision; PME: partial mesorectal excision.
Subgroup analyses were made for type of mesorectal excision and surgical approach. Cox regression modeling with multiple imputation was used to derive HRs with 95% CIs.
Adjustment for American Society of Anesthesiologists’ class, age, body mass index, current smoking, neoadjuvant therapy, operating center, operation year, minimally invasive surgery (when appropriate), sex, and type of mesorectal excision (when appropriate).
For the subgroup analyses, corresponding Kaplan–Meier curves are depicted in Figs 4 and 5. Large differences in leak rates could be visualized as a function of type of mesorectal excision, but a stratified log rank test could not detect a difference between SFM groups (log rank test, p = 0.75). There was no evidence of interaction as TME patients with SFM as compared to without SFM had an adjusted HR of 0.81 (95% CI: 0.58–1.15), while the corresponding comparison in PME patients rendered an adjusted HR of 0.87 (95% CI: 0.33–2.29). No substantial differences were detected as a function of surgical approach (stratified log rank test, p = 0.64); SFM patients had a non-significantly decreased risk of leakage in minimally invasive surgery (HR: 0.77; 95% CI: 0.49–1.21), which was less evident in open surgery (HR: 0.87; 95% CI: 0.57–1.32). Leak rates, unadjusted estimate, and adjusted estimate for these subgroups are presented in Table 3.
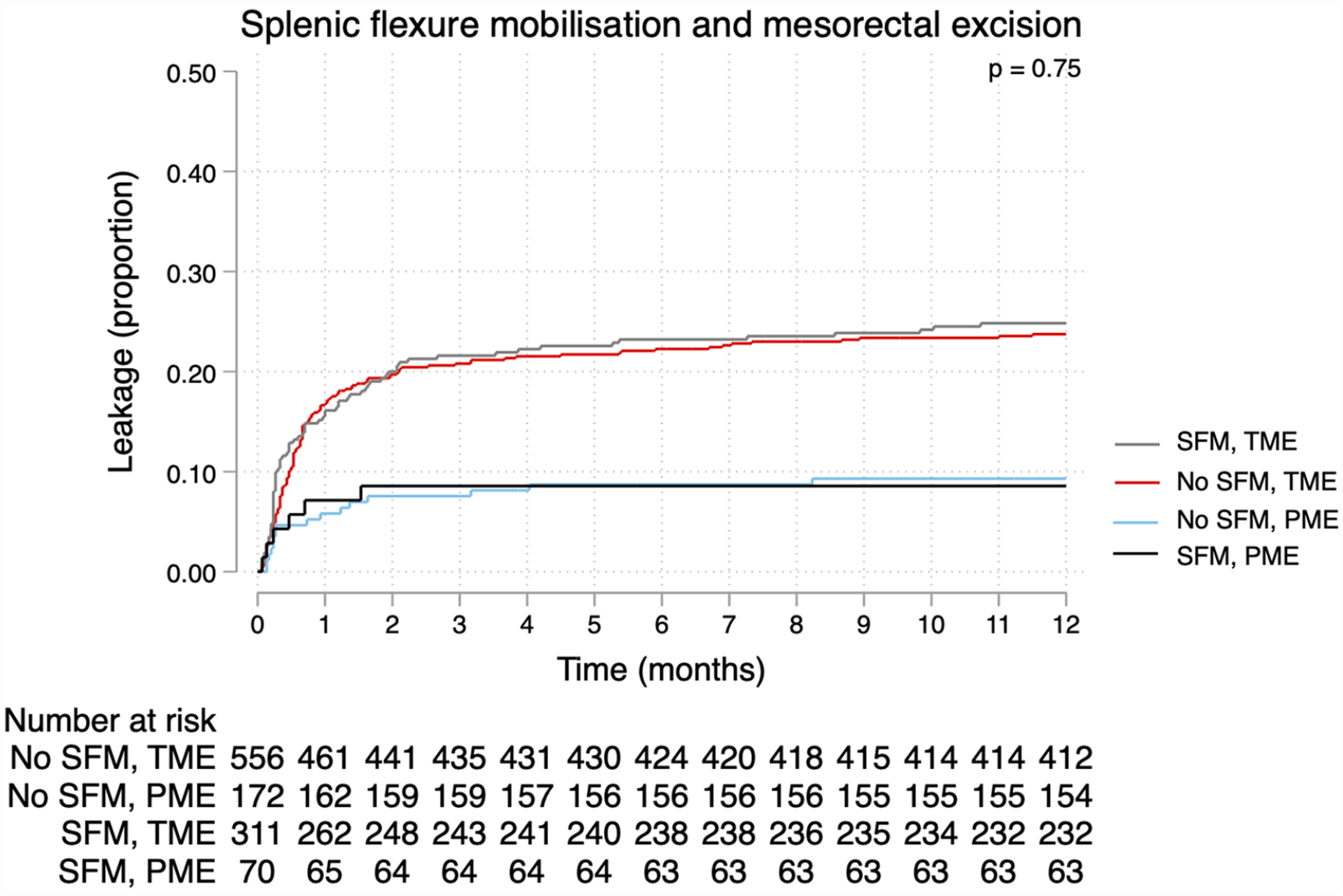
Splenic flexure mobilization (SFM) by type of mesorectal excision with time to leakage as outcome. Log rank test, stratified for type of mesorectal excision, for difference between SFM groups.
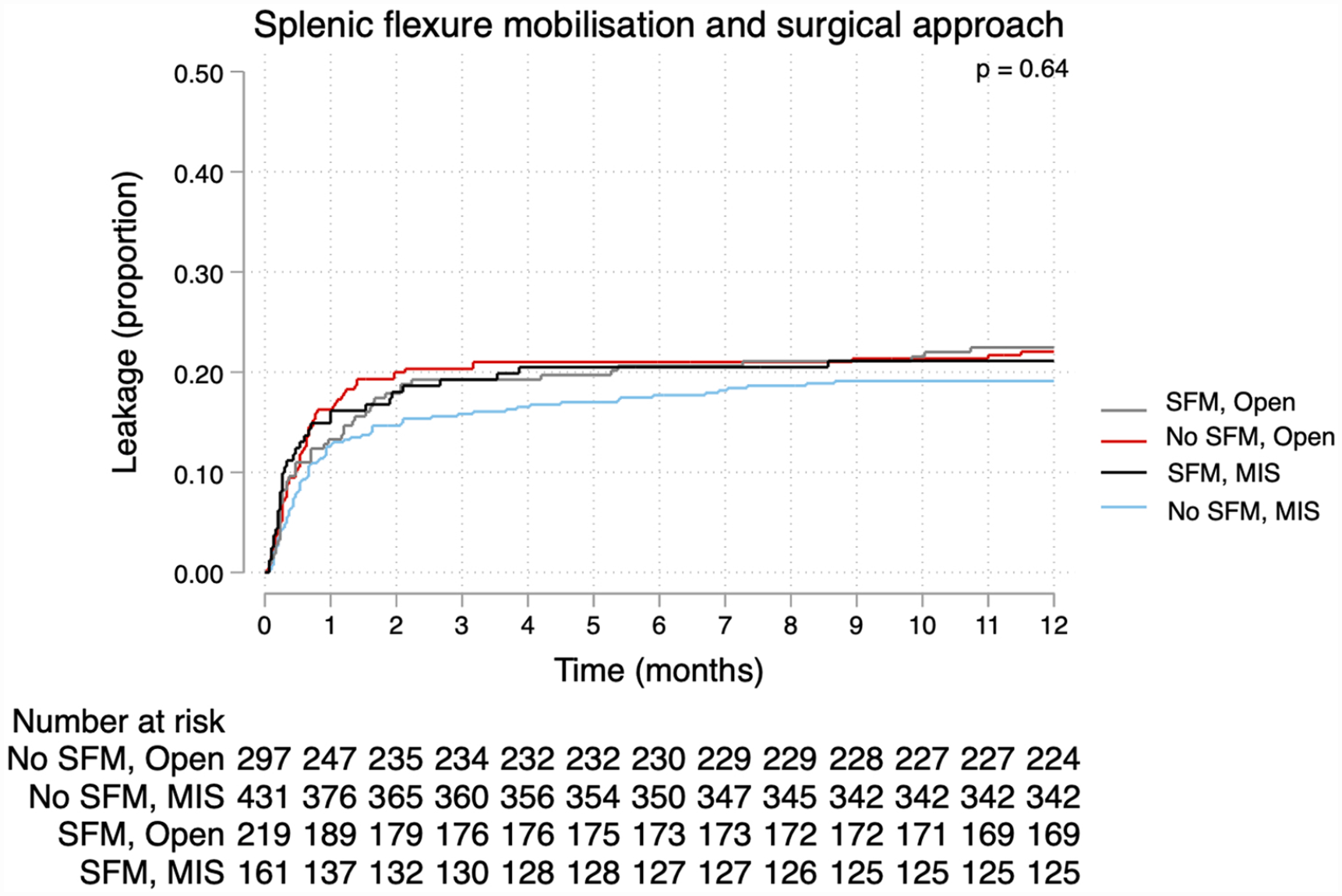
Splenic flexure mobilization (SFM) by surgical approach with time to leakage as outcome. Log rank test, stratified for surgical approach, for difference between SFM groups.
In the sensitivity analysis considering high vascular tie as a prerequisite for a fully mobilized splenic flexure, leak rates for no SFM (N = 728; 65.6%), partial SFM (N = 234; 21.1%), and full SFM (N = 147; 13.3%) were 20.3%, 20.1%, and 24.5%, respectively. After adjustment for confounding, risks of anastomotic leakage, as compared to no SFM, were lower in both partial SFM (HR: 0.84; 95% CI: 0.56–1.27) and full SFM (HR: 0.79; 95% CI: 0.52–1.21), albeit not statistically significantly so. The post hoc analysis indicated no interaction between SFM and individual hospital, neither in unadjusted (likelihood ratio test, p = 0.13) nor adjusted models (likelihood ratio test, p = 0.40). Consequently, centers with SFM rates more or less than 50%, 40%, or 30% did not differ when evaluating the main analysis (Table S1). Considering only Grade B and C anastomotic leakage, any differences between groups could not be demonstrated (HR: 0.82; 95% CI: 0.59–1.15).
Splenic injury: secondary outcome
While none of the patients without SFM had an intraoperative splenic injury, six cases (1.6%) in the SFM group had such an injury (p = 0.002); one of these patients required splenectomy.
Discussion
In an unselected cohort of patients operated for rectal cancer with anterior resection, SFM did not influence the incidence of anastomotic leakage within 12 months of surgery. Subgroup analyses including type of mesorectal excision and surgical approach yielded similar results, nor did concurrent high vascular ligation alter leak rates. Post hoc analyses could not show an effect of varying proportions of patients operated with SFM per center, while omitting Grade A leaks did not impact the main findings either. Splenic injury was more common with SFM, though with a low absolute risk.
While not a truly population-based study, selection bias due to referral patterns was limited in this multicentre cohort, as it included county hospitals as well as university hospitals, from different geographical regions; however, selection bias due to allocation of patients with a short colonic reach might arguably have been a larger problem, only partially mitigated by confounder adjustment. A large sample size was accrued due to the joint effort underlying this cohort, while accuracy for essential data points was ensured through chart review. This is important in particular for the outcome anastomotic leakage, potentially underreported when using registry-based data. 17 Here, the long follow-up concerning leakage is also a strength, as up to a third of leaks after low anterior resection occur after the first 30 postoperative days. 8
There are limitations to this study. Some underascertainment of cases can be assumed, as the study design allowed use of theater lists instead of identification through the SCRCR. This is nevertheless ameliorated by the fact that the chart review precluded erroneous inclusion of patients with permanent stoma procedures, which is a potential problem with registry-based data. 18 Table 1 demonstrates that study inclusion rates differed from SCRCR registrations to some degree, though it is not possible barring a full chart review of all rectal cancer cases to fully elucidate this; coding of transanal excision as anterior resection and anterior resection as non-restorative surgery were two reasons explaining low and high capture rates. The retrospective design also means that information bias is inevitable in this study, not least concerning the exposure SFM itself. It is sometimes difficult to state with certainty from operative notes whether SFM has been performed, exemplified by the admittedly small amount of missing data for this variable. Moreover, the concurrent maneuvers of central ligation of the inferior mesenteric vessels are at times difficult to establish with certainty, as even the operating surgeons themselves might not correctly identify the vascular anatomy.18,19 The sensitivity analysis was an attempt to remedy these uncertainties to a degree, and results were virtually unchanged. As always when conducting observational research, residual confounding from unmeasured confounders is a threat to the validity of the study, in particular when attempting causally oriented analyses. These analyses were performed with the help of directed acyclic graphs, 15 thus depicting our understanding of causes and effects involved in a necessarily much more complex pathophysiology, namely anastomotic leakage. Any conclusions must thus be made cautiously, but at least our assumptions have been presented transparently and can therefore be readily criticized and revised. Careful interpretation is required in particular for the subgroup analyses, where the low event rate in PME surgery especially widened CIs to a considerable degree.
Adequate perfusion is essential for a successful colorectal anastomosis, where excessive tension would decrease blood flow and subsequently risk ischemia. Numerous endeavors have strived to show how marginal artery bleeding, 20 colonic perfusion by fluorescence angiography, 21 and rectal laser Doppler flowmetry22,23 can be utilized to detect insufficient blood flow. While some of these methods are promising, sufficient data do not exist to prove any clinical benefit of their use. However, using surgical judgment without adjuncts to determine whether an anastomosis is likely to leak is only slightly better than tossing a coin. 24 The evidence base for lack of perfusion as the main culprit in anastomotic leakage is thus scant, further exemplified by, for example, no impact of high ligation of the mesenteric artery in trial settings, 6 whereas use of fluorescence angiography has rendered equivocal results;21,25,26 there is some evidence that, while a high vascular tie might lead to increased risk of colonic necrosis, the absolute risk is low. 3
In this context, SFM is arguably a complex issue and not easy to investigate. While this study shows that leak rates are not materially different with and without SFM, it is undoubtedly so that in some cases SFM is a necessary step to ensure colonic reach. No colorectal surgeon would intentionally construct an anastomosis under excessive tension, whereas it is unknown what amount of tension is acceptable for individual surgeons, centers, and in principle for a successful anastomosis. Conversely, some surgeons or centers routinely perform SFM, often as a first step in minimally invasive surgery. This could be readily appreciated in this study, as SFM use was common in some hospitals while rare in others; however, a sensitivity analysis evaluating whether this institutional experience had a discernible effect could not demonstrate any differences. Nevertheless, in this study, SFM was less prevalent in minimally invasive surgery, which might be a testament to the difficulty of attaining SFM expertise in this setting.
Comprising 14 studies, a major meta-analysis on the merits of SFM was undertaken recently by Rondelli et al. 5 This analysis was heavily influenced by the large administrative database study of Dilday et al., 27 where a near null result was shown for SFM and anastomotic leakage. Data validity concerning both exposure and, in particular, the outcome, is a problem here in contrast to most of the other studies in the above meta-analysis. However, these other studies are often small in contrast, but the overall meta-analysis results, even without the database study, consistently point to no beneficial effect of SFM. 5 In fact, when comparing subgroups such as type of mesorectal excision and minimally invasive surgery, this meta-analysis posits statistically significant detrimental effects of SFM, where, for example, SFM in PME surgery increases the risk of leakage almost three times. These latter findings were not reproduced in the present study, which might be a consequence of the use of an international consensus definition and capture even of delayed leaks.
The current study has not been able to show either benefits or risks concerning anastomotic leakage when performing SFM, consistent with most of the literature. The advantages and disadvantages of SFM in appropriate cases might therefore be judged on other parameters such as the increased operative time and non-negligible risk of intraoperative complications (evidenced by the low risk of splenic injury), but also the perceived necessity to remove bowel for non-oncological reasons (e.g. diverticular disease or compromised blood perfusion). While a definitive answer to whether SFM is beneficial or not requires a well-powered randomized clinical trial, such a study is unlikely to be conducted for a procedure whose indication is influenced by many different parameters.
Supplemental Material
sj-jpg-1-sjs-10.1177_14574969231181222 – Supplemental material for Splenic flexure mobilization and anastomotic leakage in anterior resection for rectal cancer: A multicentre cohort study
Supplemental material, sj-jpg-1-sjs-10.1177_14574969231181222 for Splenic flexure mobilization and anastomotic leakage in anterior resection for rectal cancer: A multicentre cohort study by Martin Rutegård, Johan Svensson, Josefin Segelman, Peter Matthiessen, Marie-Louise Lydrup and Jennifer Park in Scandinavian Journal of Surgery
Footnotes
Author contributions
M.R. co-ordinated data acquisition, wrote the study protocol, main manuscript, performed statistical analysis, and prepared tables and figures. J.S. reviewed the statistical methodology and analysis. J.S., P.M., M.-L.L., and J.P. as well as the collaborators in the RectoLeak study group acquired data. All authors edited and reviewed the manuscript and approved study submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Regional Board of the Ethical Committee in Uppsala, Sweden (DNR: 2020-02285, 2020-03795, 2020-05126).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Knut and Alice Wallenberg Foundation (RV-762241), Swedish Society of Medicine (SLS-934594), Cancer Research Foundation in Northern Sweden (AMP 19-978), Bengt Ihre Foundation (SLS-934603), and Swedish Cancer Society (CAN 2018/589).
Data availability
Upon reasonable request, data can be shared, subject to approval from the steering committee of the Swedish Colorectal Cancer Registry.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.