
Abstract
Background and objective:
At present, percutaneous endoscopic gastrostomy (PEG) is the procedure of choice in establishing a permanent feeding tube in patients with chronic severe dysphagia. This is the first prospective randomized study in adults comparing PEG with radiologically inserted gastrostomy (RIG).
Methods:
Randomization of 106 patients, eligible for both techniques, to PEG (pull method) or RIG. The groups were comparable in terms of age, body mass index, and underlying diseases. Adverse events were reported 10 and 30 days after the operative procedure, and mortality was up until 6 months. The validated European Quality of life 5 Dimensions 3 level version (EQ-5D) questionnaire was used for health status measurements.
Results:
The procedures were successfully completed in all patients. The median operative time was 10 min for PEG and 20 min for RIG (p < 0.001). The overall rate of adverse events was lower for PEG (22%) than for RIG (51%, p = 0.002), mostly due to less local self-limiting stoma reactions and tube problems. The 30-day mortality was lower after PEG (2% versus 14%, p = 0.020). Patient-scored health status remained low for the entire cohort, with an EQ-5D utility index of 0.164. Self-rated health was low but improved in the RIG group (52.5 from 41.1, out of 100).
Conclusion:
PEG can be recommended as the primary procedure in patients in need of a feeding gastrostomy, mainly due to a lower frequency of tube complications. However, as the two techniques complement each other, RIG is also a valid alternative method.
Clinical trial registration:
International Standard Randomized Controlled Trial Number ISRCTN17642761. https://doi.org/10.1186/ISRCTN17642761
Keywords
Context and relevance
The placement of a gastrostomy tube in patients with severe swallowing difficulties is a standard procedure. However, the two most common procedures, percutaneous endoscopic gastrostomy (PEG), and radiologically inserted gastrostomy (RIG) have yet to be compared in a prospective randomized trial (RCT) in adults. In the present RCT, we demonstrate that PEG is associated with a somewhat lower risk of adverse events as well as 30-day mortality compared to RIG. The main advantages of PEG over RIG are the reduced risk of tube problems and its availability in most hospitals. However, as the two techniques complement each other, RIG is also a valid alternative method.
Introduction
Placing a gastrostomy in patients with severe swallowing difficulties, that is needing nutritional support for more than 4 weeks, is a standard procedure.1,2 Two minimally invasive methods, percutaneous endoscopic gastrostomy (PEG) 3 and radiologically inserted gastrostomy (RIG) 4 have, due to the risk of general anesthesia, replaced surgical gastrostomies in these patients.5,6 Although the procedures are generally considered straight forward, neither are risk-free, especially not in complication-prone patients. At present, the choice between PEG and RIG is based on patient factors such as earlier abdominal surgery, obesity, and ability to cooperate as well as the facilities available. To the best of our knowledge, the two modalities have not been compared in a randomized trial in adults before.
The aim of this prospective randomized trial was to compare PEG and RIG concerning procedure time, early and late adverse events as well as changes in patient-scored health status.
Methods
Included patients
Consecutive patients referred to our department at Uppsala university hospital for the insertion of a feeding gastrostomy that were eligible for both methods were offered inclusion in the present randomized study. Exclusion criteria were inability to perform an endoscopy due to pharyngoesophageal obstruction, total or subtotal gastrectomy, other major upper-abdominal surgery, peritoneal carcinosis or ascites. Included patients were randomized 1:1 in blocks of 10 by closed envelopes. All patients, or their guardians/next of kin, signed a written informed consent after receiving study information at a separate out-patient visit.
Percutaneous endoscopic gastrostomy
PEG was performed in the endoscopy suite by the pull technique. In light sedation (e.g. 5 mg Diazepam IV), a routine gastroscopy was performed to confirm normal anatomy and to select an appropriate puncture site. Following sterile preparations and local anesthesia, the puncture cannula advanced into the stomach under endoscopic control. The retrieval snare was inserted through the cannula, grasped with biopsy forceps, and drawn out together with the gastroscope. The oral end of the wire was attached to the PEG tube (EndoVive Standard PEG, 20Fr, Boston Scientific, MA, USA), which was pulled into the stomach and out through the abdominal wall. The tube was secured by the external bolster, and dressings were applied. In selected cases, the endoscope was reintroduced to verify that the tube was correctly positioned.
Radiologically inserted gastrostomy
RIG was performed in an angiography suite under fluoroscopic guidance. If possible, the patients were given barium contrast orally or through a nasogastric catheter 8 to 12 h before the procedure to visualize the colon. A nasogastric tube, if not already present, was introduced to inflate the stomach with approximately 0.5 L of air. The Entuit Gastrostomy BR Balloon Retention Feeding Tube (SBRD-18-ENF) and Entuit® Secure adjustable gastrointestinal suture anchor set (Cook Medical, Bloomington, USA). After sterile preparation and administration of local anesthetics, three anchor sutures were placed around the puncture site in the lower part of the stomach. The cannula and guide wire were introduced, followed by the gastrostomy tube using the Seldinger technique. Aspiration of air and injection of water-soluble contrast verified the correct position of the three anchor sutures and the central puncture site for the 18-French catheter. After inflating the gastrostomy balloon with glycerin, the catheter was pulled, allowing slight pressure of the balloon against the stomach wall and fixed with the retention disk against the skin and secured with a tape around the tube. Dressings were then applied.
A single 1.5-g dose of intravenous cefuroxime was given to all patients. After placement of the gastrostomy (PEG or RIG), the patients returned to their ordinary ward. Feeding through the tube was delayed 24 h, according to local routines. In patients having RIG, the anchor sutures were to be removed after 14 days.
Evaluation of outcome and complications
Procedure duration, technical success, and adverse events were studied as primary outcomes. Adverse events were reported through a structured questionnaire during a clinical exam at 10 days postoperatively in our out-patient department. In addition, the same (?) questionnaire was repeated 30 days postoperatively during a follow-up phone call t with the patient, next of kin or caring staff. Major adverse events were defined as conditions in potential need of reoperation or cardiovascular support, for example gastrointestinal perforations, intrabdominal bleeding, aspiration pneumonia or myocardial infarction, while local and self-limiting problems were classified as minor. A wound infection was reported if the patient had visible pus, a widespread local tissue reaction, or was treated with antibiotics. Tube complications were defined as damaged or occluded tubes and accidental dislocation or removal of tubes. The adverse events were classified as either “early,” occurring up until the follow-up visit, or “late,” occurring thereafter but within 30 days. To detect differences in local tissue reaction, a structured questionnaire was also completed at 10 and 30 days. In addition to the structured questionnaire, medical charts were scrutinized, and administrative databases were used to detect mortality occurring within 6 months.
Patient-scored health status
Patient-scored health status was considered a secondary outcome. It was evaluated by European Quality of life 5 Dimensions 3 level version (EQ-5D), a standardized and rather simple questionnaire developed by the EuroQol Research Foundation. 7 The EQ-5D-3 L form used here assesses health status in five dimensions (mobility, self-care, usual activities, pain and discomfort, and anxiety and depression) on three levels. The questionnaire also comprises a standard vertical 20 cm visual analog scale (VAS), calibrated from “the worst health you can imagine” (scored 0) to “the best health you can imagine” (scored 100). Included patients, or their next of kin if needed, were asked to answer the questionnaire before and 30 days after receiving a gastrostomy.
Statistics
The results are presented as median and range. Differences between groups were tested by chi-square and McNemar test for categorical data, while the Mann–Whitney test was used for numerical data. A p value < 0.05 was considered statistically significant.
A power analysis, with 90% power and a power index of 0.05, was conducted using 25% as a frequency of complication, according to an RCT conducted prior by us. 6 This calculation resulted in 77 patients needed to detect a doubled frequency of complications, as reported in a previous retrospective review. 8 Statistical analysis was performed using SPSS version 26 (IBM SPSS Statistics, Armonk, NY).
Ethics and reporting standards
The study was approved by the local research ethics committee of Uppsala (Dnr: 2014-281) and performed according to the Declaration of Helsinki. This randomized controlled clinical trial conforms to the Consolidated Standards of Reporting Trials (CONSORT) criteria and has been registered in the public ISRCTN registry (ISRCTN17642761), acknowledged by the International Committee of Medical Journals Editors. The enrollment, allocation, follow-up, and analysis of this randomized clinical trial are described in the CONSORT Flow Diagram (Fig. 1).
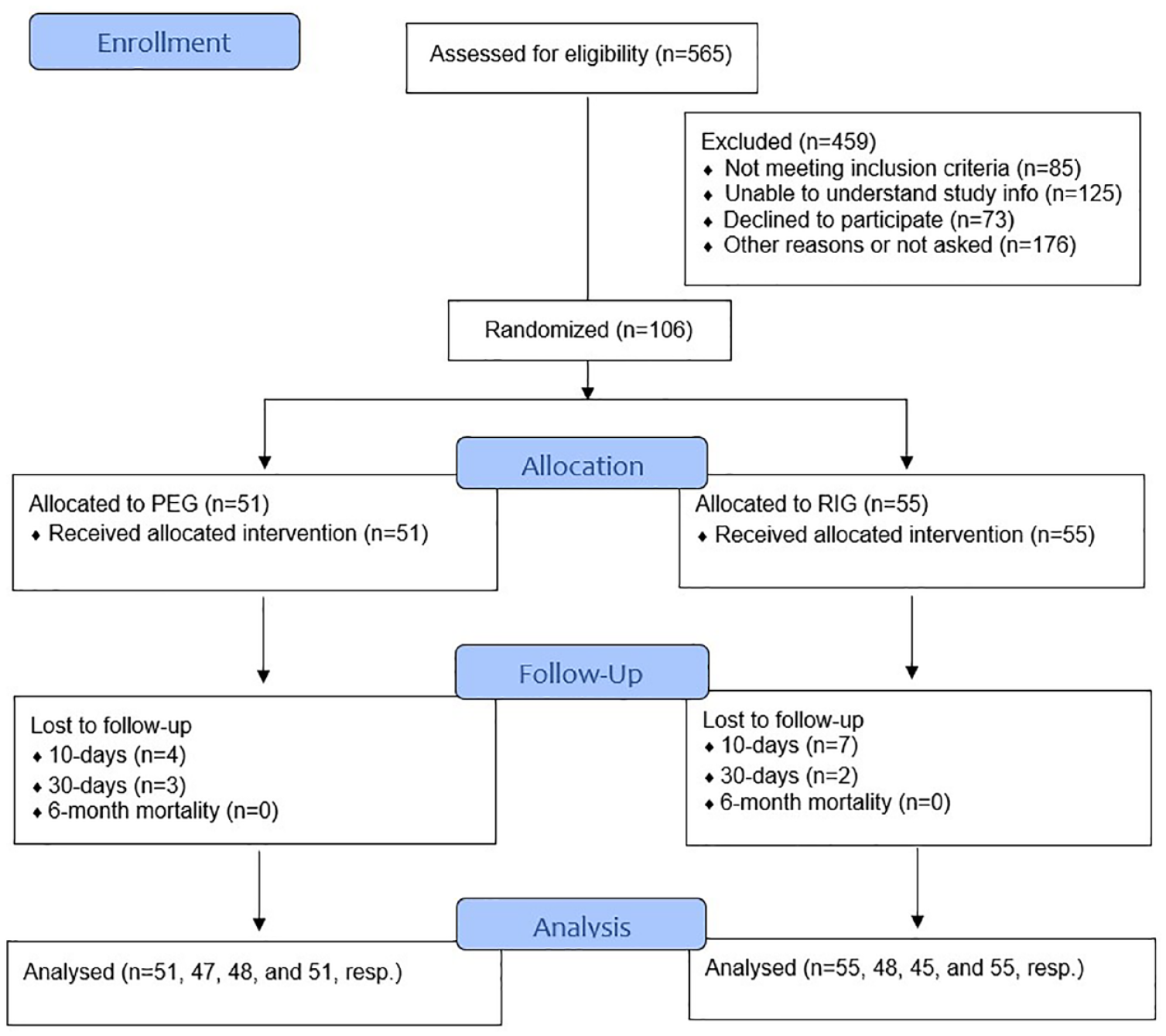
CONSORT flow diagram describing the enrollment, allocation, follow-up, and analysis in the present randomized clinical trial.
Results
106 patients were included and randomized, resulting in two comparable groups concerning age (51 versus 56 years), BMI (23 versus 23 kg/m2), gender, basic laboratory status, and underlying diseases, that is the condition that caused the patient to require a gastrostomy (Table 1).
Clinical data for 106 patients randomized to percutaneous endoscopic gastrostomy (PEG) or radiologically inserted gastrostomy (RIG).
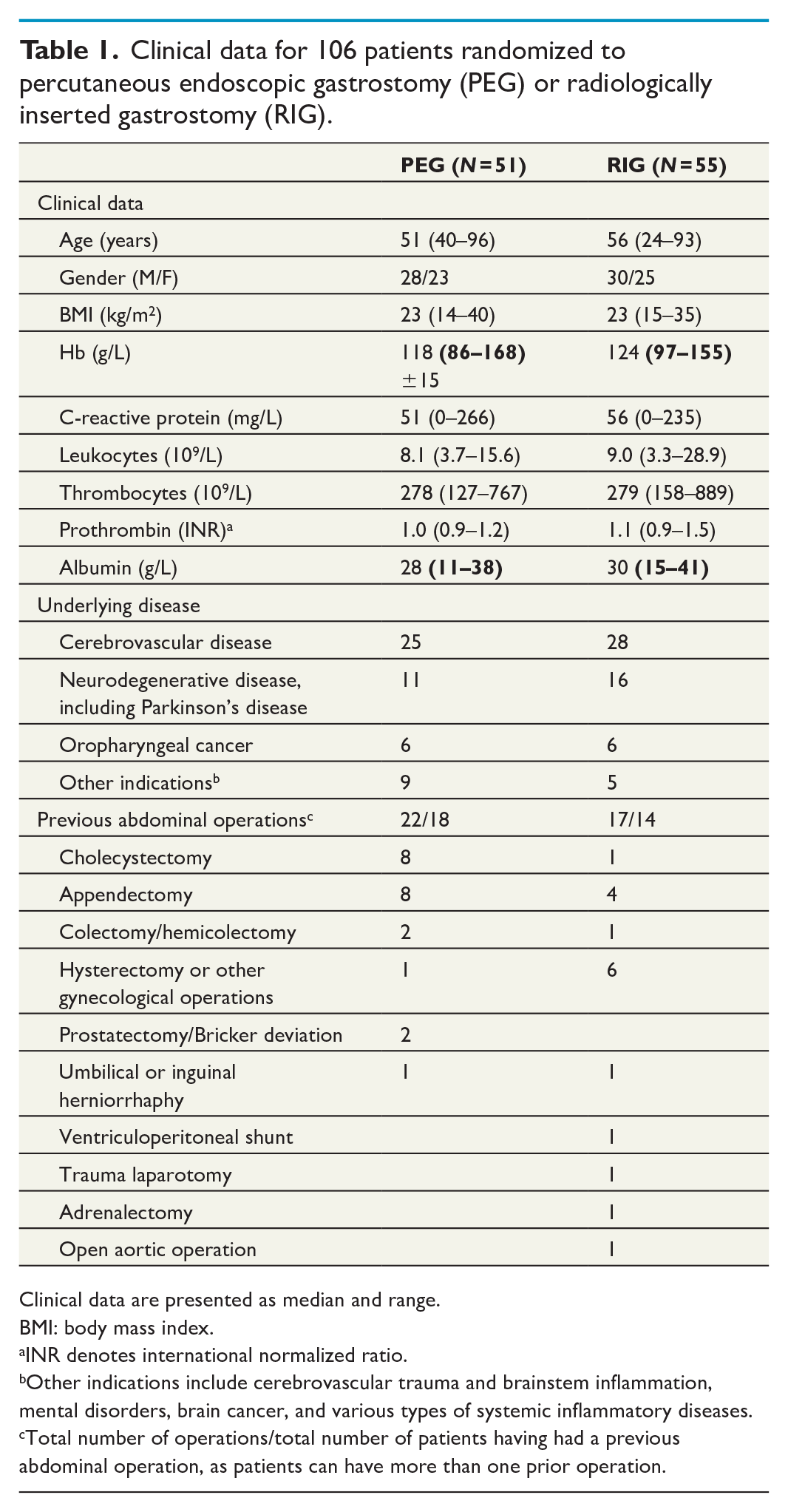
Clinical data are presented as median and range.
BMI: body mass index.
INR denotes international normalized ratio.
Other indications include cerebrovascular trauma and brainstem inflammation, mental disorders, brain cancer, and various types of systemic inflammatory diseases.
Total number of operations/total number of patients having had a previous abdominal operation, as patients can have more than one prior operation.
Procedure results
All planned procedures were successfully completed. The median operative time for PEG, from introduction of the endoscope to completed dressings, was 10 min (6–25 min). For RIG, the corresponding time was 20 (13–40) min, p < 0.001. Perioperatively, four technical problems occurred: one during PEG and three during RIG. All were minor and did not affect the immediate outcome of the respective procedure (Table 2).
Operation time and technical problems during placement of percutaneous endoscopic gastrostomy (PEG) and radiologically inserted gastrostomy (RIG).
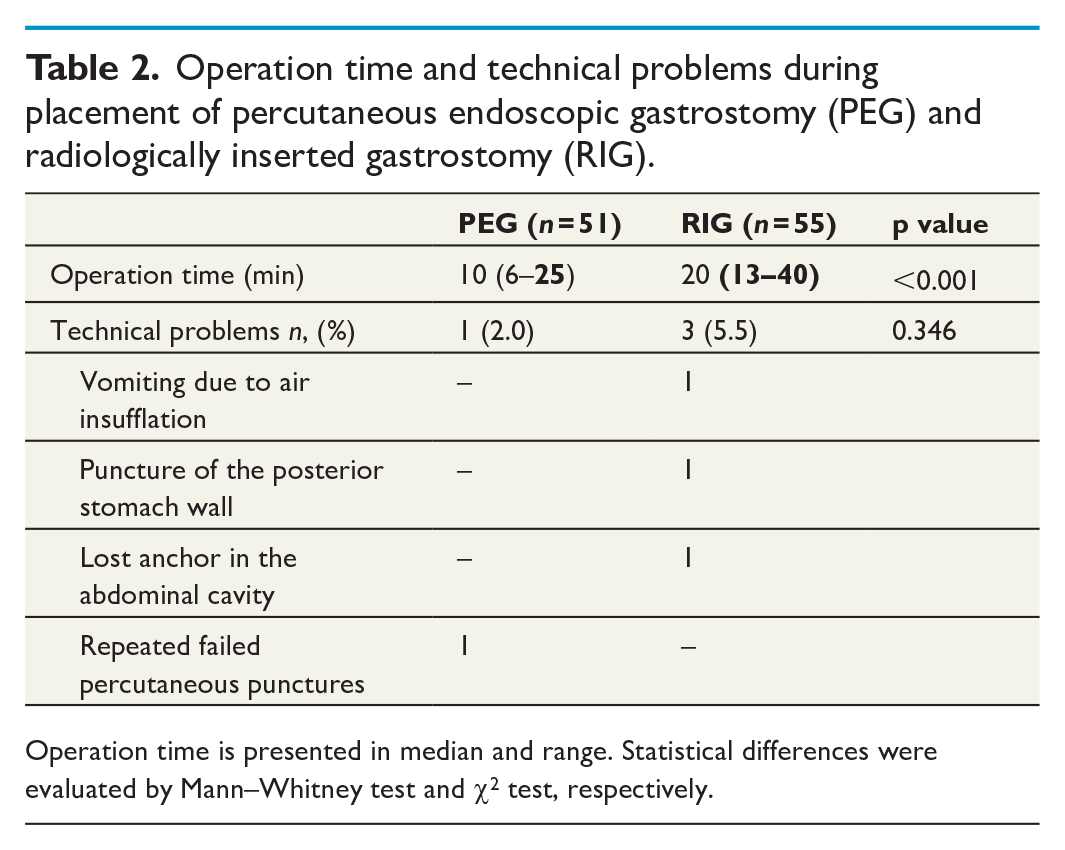
Operation time is presented in median and range. Statistical differences were evaluated by Mann–Whitney test and χ2 test, respectively.
Adverse events
Reported postoperative adverse events consisted of mainly local and self-limiting complications, and were found significantly more frequent for RIG, 50.9% (n = 28), compared to PEG, 21.6% (n = 11), p = 0.002. The three-fold difference was seen at both 10 and 30 days and consisted mostly of increased number of stoma reactions and tube problems after RIG (Table 3). Furthermore, local tissue reactions were more pronounced after RIG, both at the follow-up visit at 10 days and in the 30-day survey (Table 4).
Overall adverse events after percutaneous endoscopic gastrostomy (PEG) and radiologically inserted gastrostomy (RIG).
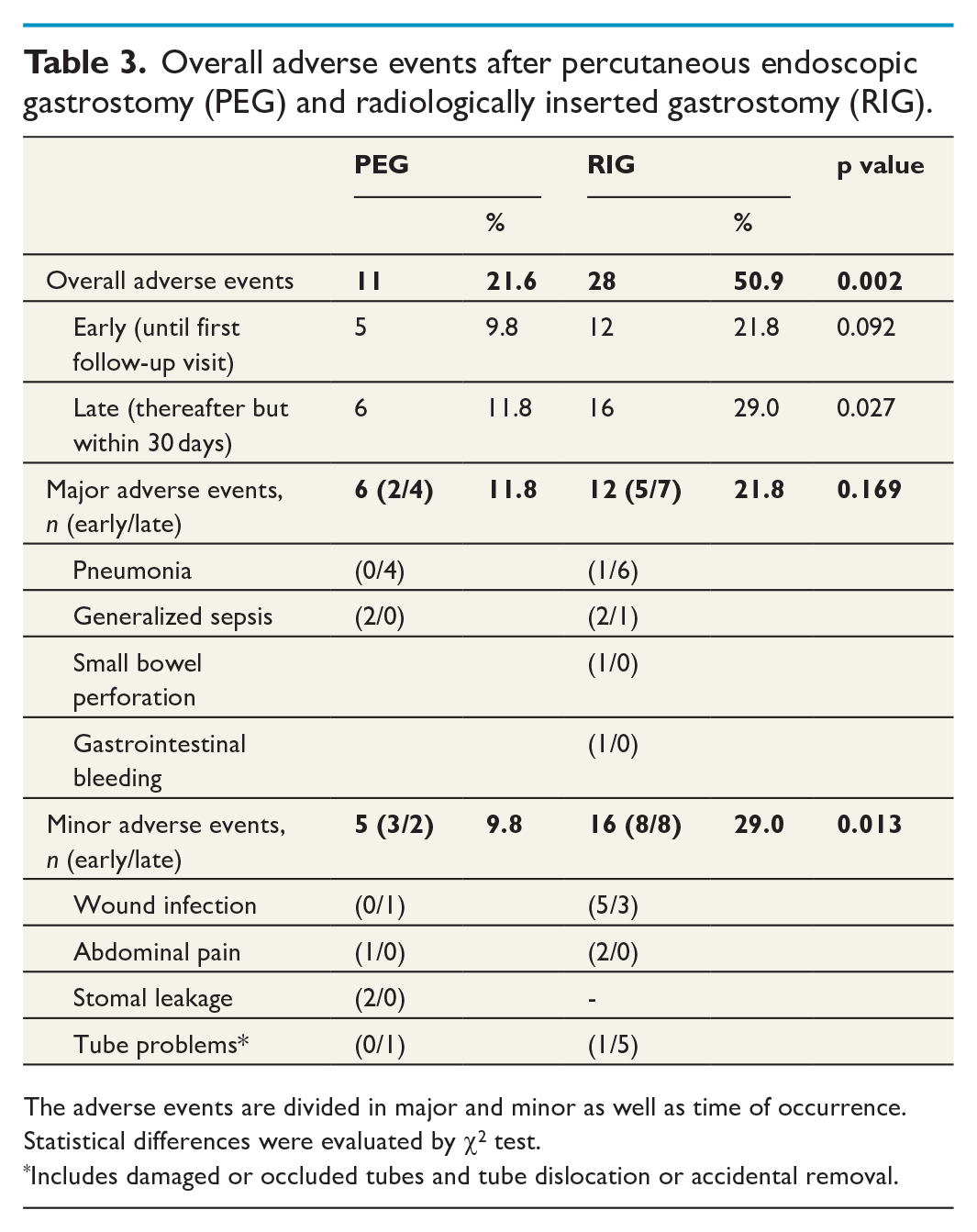
The adverse events are divided in major and minor as well as time of occurrence. Statistical differences were evaluated by χ2 test.
Includes damaged or occluded tubes and tube dislocation or accidental removal.
Local tissue reaction after percutaneous endoscopic gastrostomy (PEG) and radiologically inserted gastrostomy (RIG) according to the structured questionnaire.
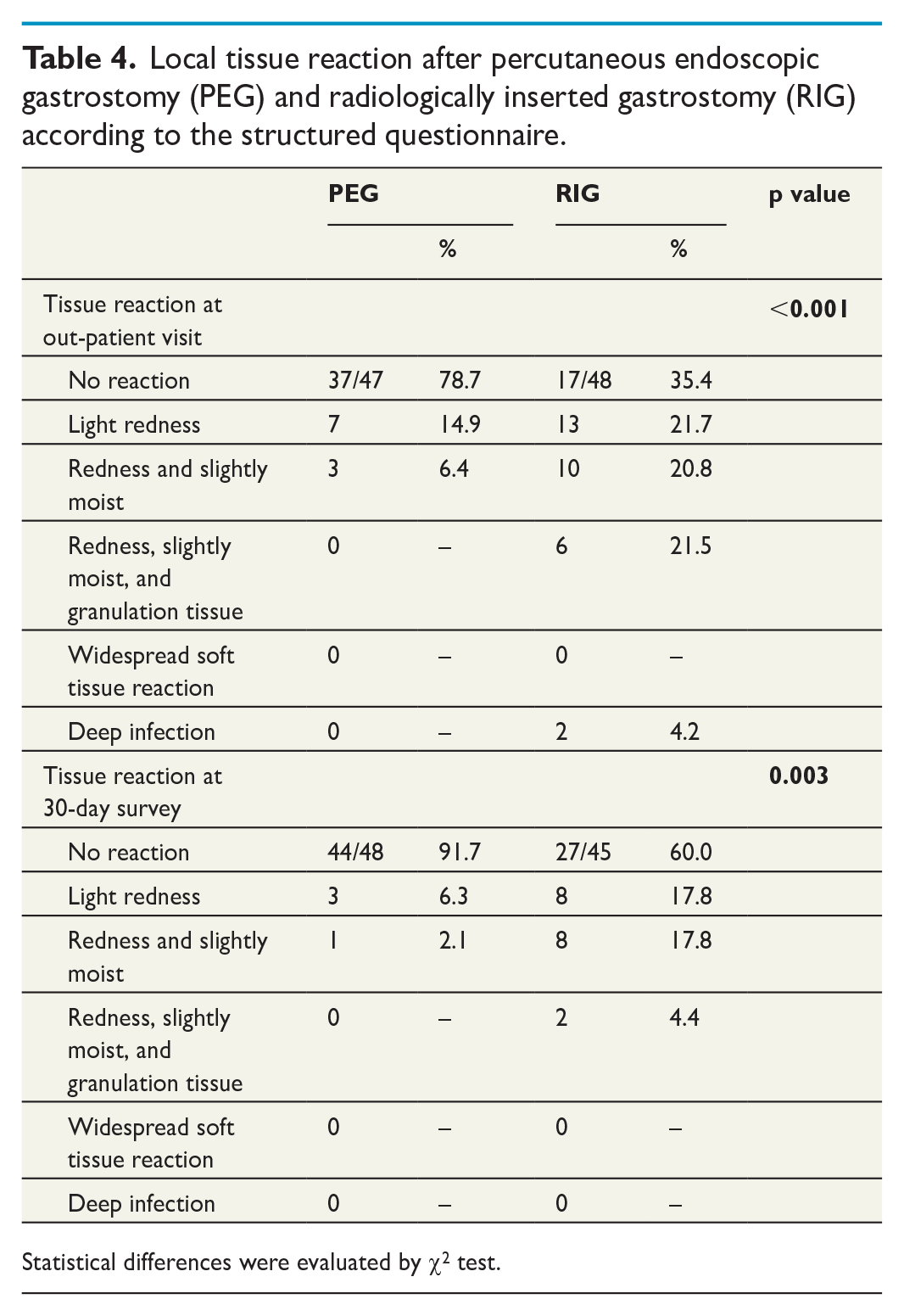
Statistical differences were evaluated by χ2 test.
Patient-scored health status
As demonstrated in Table 5, perceived health status was low in both groups. Most of the patients were confined to bed, unable to wash or dress, or perform their usual activities, that is level 3 for mobility, self-care, and usual activities. The scores for pain/discomfort and anxiety/depression were centered around level 2. Postoperatively, problems with pain/discomfort were significantly reduced in the entire cohort. In the PEG group, the degree of problems hindering usual activities was reduced, however, 71 % were still unable to perform their usual activities. Although improved mobility was seen after RIG, 45% of the patients were confined to bed. No improvement of the low utility scores was seen; however, self-rated health was improved in the RIG group (from 41.1 to 52.5, p = 0.008).
Patient-scored health status before and after receiving a gastrostomy as evaluated by EQ-5D-3L, assessing five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) on three levels.
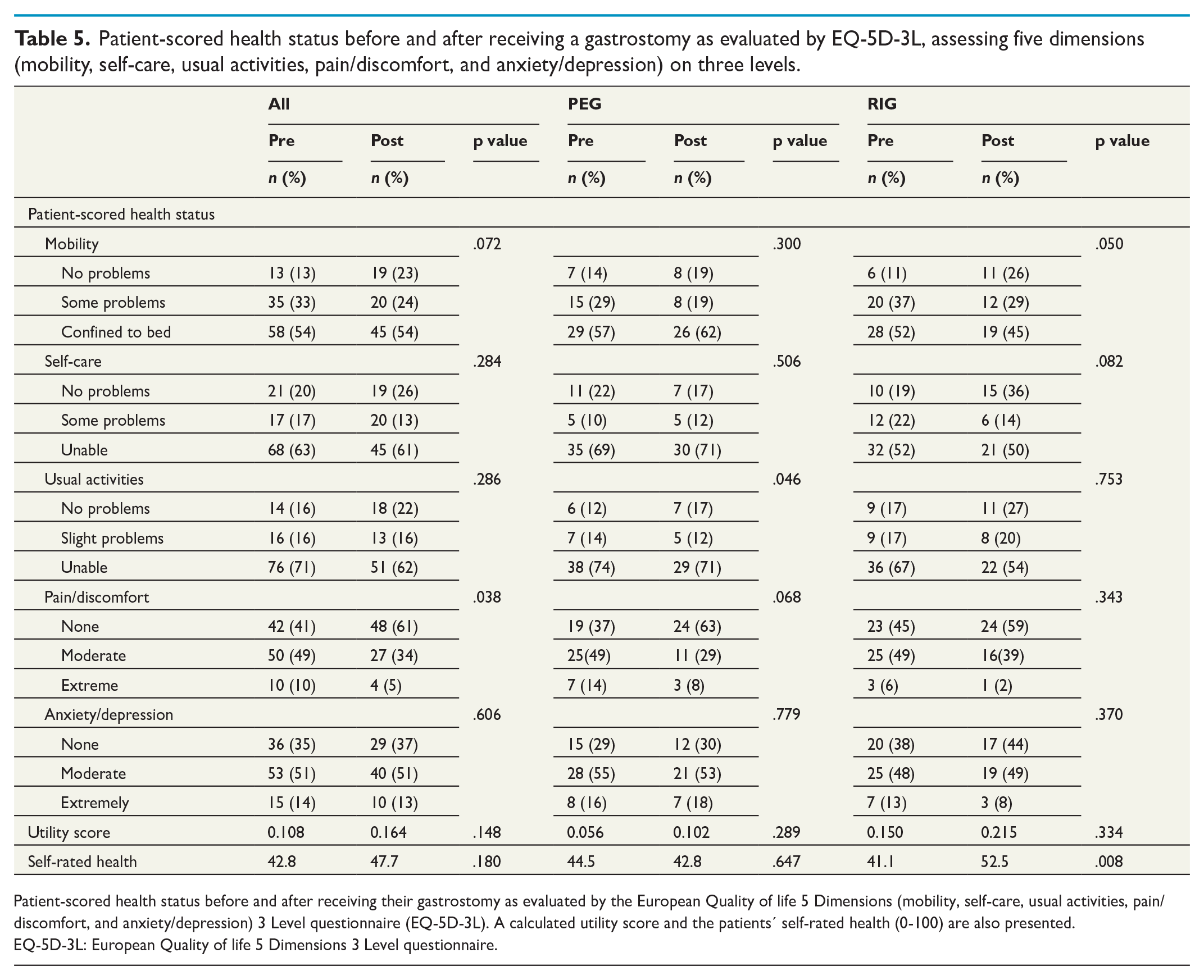
Patient-scored health status before and after receiving their gastrostomy as evaluated by the European Quality of life 5 Dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) 3 Level questionnaire (EQ-5D-3L). A calculated utility score and the patients’ self-rated health (0-100) are also presented.
EQ-5D-3L: European Quality of life 5 Dimensions 3 Level questionnaire.
Survival
The 30-day mortality was lower after PEG than RIG, 2.0% (1/51) and 14.5% (8/55), respectively. The difference was mainly due to the increased number of cardiopulmonary-related deaths (6 versus 0). One death occurred in RIG group due to small bowel perforation and subsequent peritonitis. No other direct procedure-related deaths could be found when examining the patient charts (Table 6).
Overall mortality after percutaneous endoscopic gastrostomy (PEG) and radiologically inserted gastrostomy (RIG).
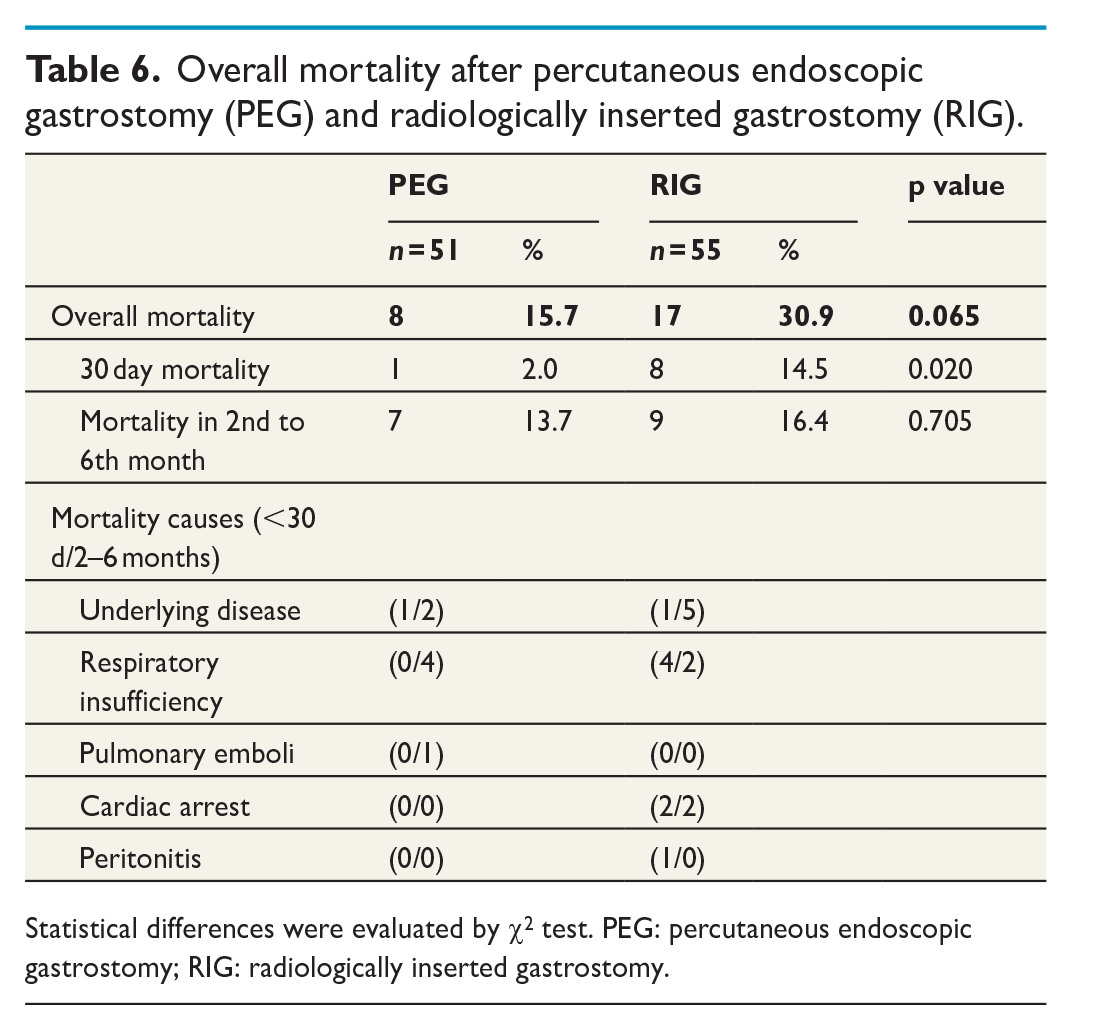
Statistical differences were evaluated by χ2 test. PEG: percutaneous endoscopic gastrostomy; RIG: radiologically inserted gastrostomy.
Discussion
In this first prospective randomized trial in adults, we could demonstrate that PEG was associated with a lower risk of adverse events as well as 30-day mortality compared to RIG. Although PEG procedures were found to be somewhat quicker than RIGs, both operative procedures were performed within half an hour.
To the best of our knowledge, no randomized controlled trial comparing PEG and RIG in adults has been published, yet was requested in the latest Cochrane report on the subject. 9 At present, several retrospective and non-randomized controlled studies as well as case series have demonstrated high feasibility and safety in both PEG and RIG in selected populations.10–15 Some of the above-mentioned studies have shown lower complication rate and/or mortality after a PEG procedure, 16 while others conclude that RIG is preferable. 17 Increased age, neurological disease as gastrostomy indication and longer insertion time have been described as risk factors for complications. 13
Our difference in overall adverse events (22% versus 51%) was mainly due to minor local and self-limiting events such as local stoma reactions and tube complications. However, there were rather few wound infections (4.7%) within the first week, perhaps as a result of prophylactic antibiotics, as recommended by the systematic Cochrane review. 10 In a former Swedish RCT (n = 236 patients) comparing standard prophylaxis with a single intravenous dose of 1.5 g cefuroxime (as used here) and a single 20 ml dose of sulfamethoxazole and trimethoprim deposited in the PEG-catheter immediately after insertion, wound infection rates were higher, 11.9% and 8.6%, respectively. 11 Theoretically, and in line with one study, 13 RIG should have a lower infection rate than PEG as the PEG tube is pulled through the oral cavity, transferring oropharyngeal microbiota into the abdominal wall. The present increased frequency of stoma reactions after RIG was probably related to the insertion of three anchors, in addition to the gastrostomy tube, through the abdominal and gastric wall. Also, the recommended cut of the anchor suture after 14 days was not found to be regularly followed. This observation has caused us to emphasize the importance of timely removal of the three anchor sutures in the postoperative information provided to referring physicians.
Tube failures due to either blockage or dislodgement are frequently reported after gastrostomy procedures.13,15,16 In the current study, the total number of patients with tube problems was higher after RIG than PEG. This could depend on the use of different systems with somewhat different tube diameters, 6.67 mm (20 Fr) in PEG and 6.00 mm (18 Fr) in RIG, or the use of an inflated balloon in RIG instead of the more secure fixation with a flat silicone-dome in PEG. In a multivariate analysis of all dislodgement causes, Cherian et al found “the method of insertion” to be the most important parameter, with a RIG being 5.4 times more likely to be dislodged than PEG. 15 It is apparent that the PEG method has evolved over decades, while the technical development in RIG is still to come.
The major adverse events were mostly systemic infections such as aspiration pneumonia and sepsis, while only two gastrointestinal complications were seen, despite the inevitably semi-blind passage of cannulas through the abdominal cavity in both procedures. In the RIG group, an undiagnosed small bowel perforation led to the death of one patient, while a minor gastrointestinal bleeding surceased spontaneously. Our results are in line with a meta-analysis of 2353 individuals with neck and head cancer, demonstrating RIG to be associated with higher number of major complications, 17 while an earlier meta-analysis from 1995 involving 5680 participants with various underlying conditions found the opposite. 18 We did not find any significant difference in the overall mortality of the PEG and RIG groups in our study. The same results have been published by other authors,13,19–22 concluding that the deaths have not been related to the procedure per se, but to the patients’ underlying diseases.
Compared to our former RCT on PEG and open gastrostomy, 6 the present outcome after PEG is somewhat improved (operative time: 10 versus 15 min, overall complication rate: 21.6% versus 42.9% and 30-day mortality: 2.0% versus 5.7%). This improvement may be due to either patient selection or increased experience, or a combination of both factors. Undoubtedly, RIG has some specific benefits compared to PEG. To start with, RIG might be the only available technique in patients with head and neck cancers, where passing of an endoscope can be difficult or even impossible. Furthermore, in patients having a nasogastric feeding tube, this can be used during RIG placement, thus avoiding the discomfort of passing an endoscope. Hence, the two techniques complement each other.
Patient-scored health status
As expected, the present patient-scored health status was well below the Swedish general population based on a sample of 49,169 individuals (mean age 46.2 years, women 56.3%) in which only 6.7% scored problems on level 3 and the mean self-rated health was 79.5 (here 42.8). 23 Furthermore, our utility values (0.108) were well below other severe and chronic diseases, such as neoplasms (0.62–0.90), multiple sclerosis (0.31–0.78), and chronic kidney disease (0.37–0.89). 24 Despite this, problems with pain/discomfort were significantly reduced at 30 days. Interestingly, the VAS score was significantly improved in the RIG group (from 41.1 to 52.5), while the postoperative score in PEG patients was identical to the baseline score in all patients (42.8).
Clinical considerations before deciding on a gastrostomy
Patient selection is very important as most patients in need of a gastrostomy have a rather short life expectancy due their underlying disease. The balance between overall risks and the strength of the indication for placing a feeding gastrostomy must, therefore, be carefully assessed in each individual case. First, the patient should gain from a gastrostomy, preferably both in quality of life and survival. Callahan et al demonstrated that at least 70% of patients surviving 60 days or more after PEG placement, had no significant improvement in functional, nutritional, or subjective health status. 25 Likewise, the improvement in health-related quality of life was minute also in the present patients. Second, postoperative feeding through a gastrostomy is time-consuming and interferes with daily life. In 104 non-hospitalized patients, the patient’s spouse was the primary person that used and cared for the patient’s gastrostomy at home and, if tube-related problems occurred, repeated visits to an out-patient clinic for help were frequent. 26 We are, therefore, reluctant to place a gastrostomy in patients having a functioning nasogastric tube, just for the convenience of the community nurse, or the staff at a nursing home. Third, in reducing the complication risk, basic laboratory values must be satisfactory, for example low C-reactive protein and acceptable albumin. Albumin and C-reactive protein levels have otherwise been demonstrated to predict short-term mortality after PEG placement. 27 Obviously, an adequate coagulation status is important before making the required semi-blind passage through the abdominal cavity. Finally, the institutional experience is of utterly importance, from the individual skills of the physicians placing gastrostomies to the multiprofessional follow-up team, handling future contact and the rather frequent rate of various complications.
Strengths and limitations
The prospective randomization resulted in two well-balanced cohorts concerning age, gender, BMI, and indication for a gastrostomy. The fact that both procedures were performed in routine care, and not by strictly specialized teams, resulted in a high generalizability. The standardized follow-up, with high follow-up rate (90% and 88% at 10- and 30 days, respectively, and 100% for 6 months mortality), entailed a high scientific validity. The inclusion rate, however, turned out to be somewhat slow, which resulted in a premature closure after including 106 patients in 49 months, instead of the intended 154 patients. However, given the number of included patients, we reached 88.3% power in detecting differences in postoperative complications at an alpha of 0.05. Furthermore, the newer five-level version of EQ-5D has been demonstrated to reduce the ceiling effect, 28 allowing a larger proportion of respondents to report more severe health problems, compared to the present three-level version. This was, however, a minor problem in our study as the patients predominantly scored moderate to severe problems (levels 2 and 3).
Based on the results of this first prospective randomized study in adults, PEG can be recommended as the first choice in patients needing a feeding gastrostomy due to severe dysphagia. The main advantages of PEG over RIG are the reduced risk of tube problems and its availability in most hospitals. However, as the two techniques complement each other, RIG is also a valid alternative method.
Footnotes
Acknowledgements
The authors would like to acknowledge all staff involved in these patients, making the study possible.
Author contributions
Study design (MS, EC, RH, CEB, and ML), data collection (EC), analysis and manuscript draft (MS and EC), interpretation of data and critical review (MS, RH, CEB, UJ, and ML). All authors reviewed the results and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.