
Abstract
Background:
Free tissue transfer reconstruction carries significant complication rates in surgical head and neck oncology. A registry-based approach offers a possibility to investigate the factors affecting increased morbidity and early mortality, that is, death within 6 months of treatment.
Methods:
A retrospective registry review was conducted on a series of 317 consecutive microvascular free tissue transfers in head and neck cancer patients performed during 2013–2017 at the Helsinki University Hospital (Helsinki, Finland). All surviving patients had a minimum follow-up of 2 years (range 24–84 months).
Results:
Overall, 36 (11.4%) early deaths occurred in this series. In multivariable logistic regression analysis, patients aged 75 years and older (p = 0.019), Adult Comorbidity Evaluation-27 (ACE-27) score of 3 (p = 0.048), tumor class T3 (p = 0.005), lymph node class N2 (p = 0.014), or thrombocyte count of 360 (× 109 L) or more (p = 0.001) were more likely to die within 6 months of surgery. Of these 36 patients, 27 (75%) had a complication warranting hospital care and most (n = 22, 61%) had several complications.
Conclusions:
Early postoperative mortality most frequently affects patients aged 75 years and above, with a high ACE-27 score, advanced tumor stage, or high thrombocyte count. Therefore, preoperative assessment and patient selection should have a crucial role in this patient population.
Keywords
Context and Relevance
The purpose of the study is to determine the value-based treatment of head and neck cancer patients. Value-based care includes the quality of care, for example, complications and the results, for example, survival. We investigated the factors affecting early mortality, that is, death within 6 months of treatment. A retrospective registry review was conducted on a series of 317 consecutive microvascular free tissue transfers in head and neck cancer patients performed during 2013–2017 at the Helsinki University Hospital (Helsinki, Finland). Early postoperative mortality most frequently affects patients aged 75 years and above, with a high ACE-27 score, advanced tumor stage, or high thrombocyte count. Therefore, preoperative assessment and patient selection should have a crucial role in this patient population.
Introduction
Head and neck cancer (HNC) is the seventh most common cancer in the world. 1 Management consists of either surgery or (chemo)radiotherapy, or their combination. 2 Reconstruction of tissue defects with microvascular free flaps has become the standard of surgical HNC care.3–5
The frequency of postoperative complications after head and neck free tissue reconstructions varies considerably (20%–72%) between published reports.6‑10 Severe postoperative complications clearly decrease overall survival. 11 A specialty-specific surgical risk calculator was created to predict postoperative complications and to facilitate surgical decision-making. 12 Nevertheless, the risk calculator is not adaptable to patients with head and neck microvascular free flap reconstruction due to the nature of the surgery and the associated complications. 13 Therefore, further investigations are needed to identify patients with an increased risk for postoperative complications and early death. These risk factors can be used to optimize treatment and preoperative decision-making.
Early mortality, that is, death within 6 months of diagnosis, is an important phenomenon among HNC patients and can be either cancer-, patient- or treatment-related. 14 Talani et al. 15 reported an early-death rate of 4.5% for patients with curative intent of treatment in a series of 8751 HNC patients in the Swedish HNC Quality Registry. The identified risk factors in their study were older age, advanced stage, hypopharyngeal site, and higher WHO score. Mortality associated with HNC reconstructive free flap surgery has not been studied extensively.16–19 A recent systematic literature review found that, on average, 1.2% of these patients will die less than 30 days after free flap reconstruction. 20 While the identification of reasons for early death is crucial to guide treatment decisions in this patient population, the literature on these aspects is limited. L’Esperance et al. 21 examined 3-month mortality in a series of patients aged 80 years and older undergoing ablative head and neck oncologic surgical procedures and found a mortality rate of 10.4%. Lahtinen et al., 22 the only study reporting on 6-month mortality, examined a series of 146 HNC patients, with only 10 deaths occurring during the first 6 months of follow-up after microvascular reconstruction.
The aim of this study was to find the risk factors for early death after HNC surgery with primary microvascular free flap reconstruction. We applied a registry-based approach to identify and investigate a real-world series of patients at an academic tertiary care center.
Methods
The present non-selective series was identified in the hospital registry at the Helsinki University Hospital (HUS) (Helsinki, Finland) and comprised all patients undergoing a primary free tissue transfer reconstruction for HNC ablative surgery between 2013 and 2017. An electronic search for these patients was conducted by the Department of Data Management using HNC diagnoses (International Classification of Diseases 10th revision (ICD-10) classification) and surgical procedure codes (Nordic Medico-Statistical Committee (NOMESCO) Classification of Surgical Procedures).
Between 2013 and 2017, 1784 new patients with HNC were treated at HUS. After excluding patients who were not treated with curative intent, did not undergo free tissue transfer reconstruction, or had had prior (chemo)radiotherapy or oncologic head and neck surgery, 317 patients were included in the study. Patient-related factors are presented in Supplemental Table 2. Median age was 65 (range 21–94) years and the majority (n = 191, 60.3%) were male. All patients had a minimum follow-up time of 2 years (range 24–84 months). Early mortality was defined as death within 6 months of surgical treatment.
Department of Data Management collected the data which included the following: demographics (age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) Physical Status Classification, Nutritional Risk Screening 2002 (NRS2002), preoperative laboratory values—hemoglobin (Hb), leukocytes (Leuc), thrombocytes (Thromb), C-reactive protein (CRP), creatinine (Crea), sodium (Na), and albumin (Alb)), percutaneous endoscopic gastrostomy (PEG), tracheostomy, length of intensive care, length of hospital stay, hospital death, death within 6 months of surgery, and death later than 6 months after surgery. In addition to using registry data, a retrospective analysis of medical records was performed. We collected and completed data which included pre-existing medical conditions, usage of corticosteroids and anticoagulants, smoking, and alcohol usage. Tumor-related factors were tumor location and tumor, nodes, and metastases (TNM) classification.Treatment- and follow-up-related factors comprised intent of treatment (curative or palliative), operative technique, postoperative chemoradiotherapy, postoperative complications, and persistent growth of tumor.
The Charlson Comorbidity Index (CCI), age-adjusted Charlson Comorbidity Index (ACCI), and Adult Comorbidity Evaluation-27 (ACE-27) score were calculated as indicators of comorbidity. Two clinicians (anesthesiologist and otorhinolaryngologist) graded all complications using the Clavien–Dindo classification system. 23 Causes of death were provided by Statistics Finland, and the underlying cause of death was used in the analysis.
Descriptive statistics are presented as means or medians with ranges for continuous variables and numbers with percentages for categorical variables. Mean age between groups was compared using one-way analysis of variance with Tukey’s method in pairwise comparisons and median BMI values using Kruskal–Wallis test with Dunn–Bonferroni method in pairwise comparisons. Chi-square test was used to test the difference in patient characteristics (categorical variables) between groups. The associations of risk factors with early death were analyzed using binary logistic regression. Risk factors significantly associated with early mortality (death within 6 months of treatment versus alive at 6 months) in univariate analysis were entered in multivariable logistic regression model. Backward selection (exclusion criteria p ⩾ 0.05) was used to select the significant risk factors for the final multivariable model. As an additional analysis, the associations of risk factors for death within or after 6 months of surgical treatment compared to surviving until the end of follow-up were examined using multinomial logistic regression. Alive at the end of the follow-up was used as a reference category in multinomial logistic regression. Results of logistic regression models are expressed using odds ratios (OR) with 95% confidence intervals (CI). Survival curve was estimated with Kaplan–Meier method. Statistical analyses were performed using IBM SPSS Statistics 27 for Windows (IBM Corp., Armonk, NY). The p-values less than 0.05 were considered as statistically significant.
Study permission was granted by the Research Administration of the Helsinki and Uusimaa Hospital District (HUS/419/2018). Research Ethics Board approval for the retrospective registry study was not needed in accordance with Finnish legislation.
Results
Risk factors for early death
In 317 patients, a total of 113 patients died during the follow-up period of this study. Most of these deaths (n = 83, 73.5%) occurred within 2 years of surgery (Fig. 1). Overall, 36 patients (11.4%) died within 6 months of the primary surgery. However, 4 out of these 36 (11.1%) died before their planned postoperative treatment commenced. Those patients who died within 6 months of surgery had a higher mean age (70.1 versus 64.2 years, p = 0.005), lower median BMI (22.6 versus 24.7, p = 0.013), and higher ASA, CCI, ACCI, and ACE-27 scores compared to patients who were alive 6 months after treatment (p < 0.001 for all) (Table 1). There were no differences in smoking and alcohol use between those who died within 6 months and those who were alive at 6 months.
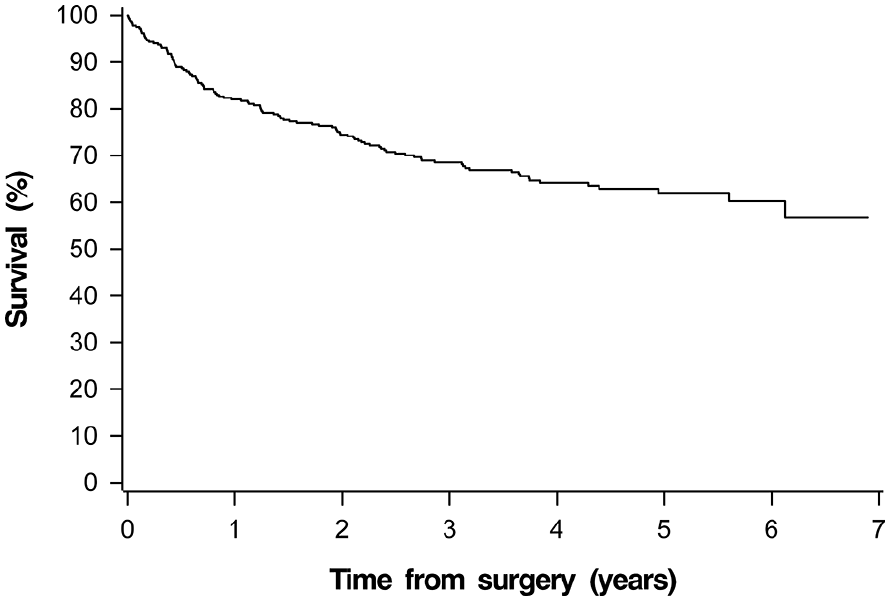
The survival rate of 317 head and neck cancer patients undergoing microvascular reconstruction with free flap tissue transfer during 2013–2017.
Patient characteristics of 317 patients undergoing free flap reconstruction after surgery for head and neck cancer during 2013–2017.
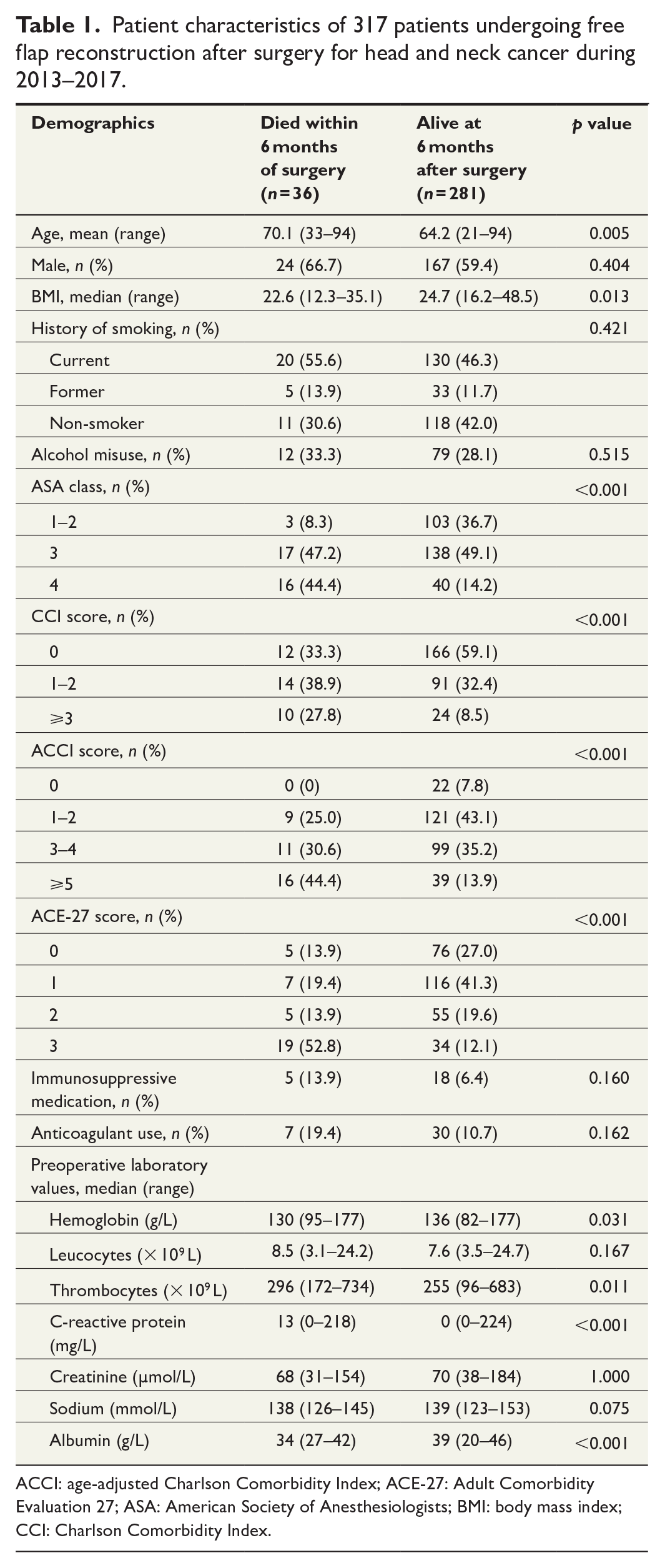
ACCI: age-adjusted Charlson Comorbidity Index; ACE-27: Adult Comorbidity Evaluation 27; ASA: American Society of Anesthesiologists; BMI: body mass index; CCI: Charlson Comorbidity Index.
Results for univariable binary logistic regression are shown in Supplemental Table 1. Multivariable binary logistic regression analyses showed that the preoperative factors contributing significantly to early death after HNC microvascular free flap reconstruction were age 75 years or older, ACE-27 score of 3, elevated thrombocytes, T3 tumor stage, and N2 lymph node stage. Multivariable analyses showed that postoperative factors significantly associating with early death were tracheostomy and length of hospital stay of 20 days or more (Table 2).
The associations of factors with early death (within 6 months of treatment) by multivariable binary logistic regression analysis.
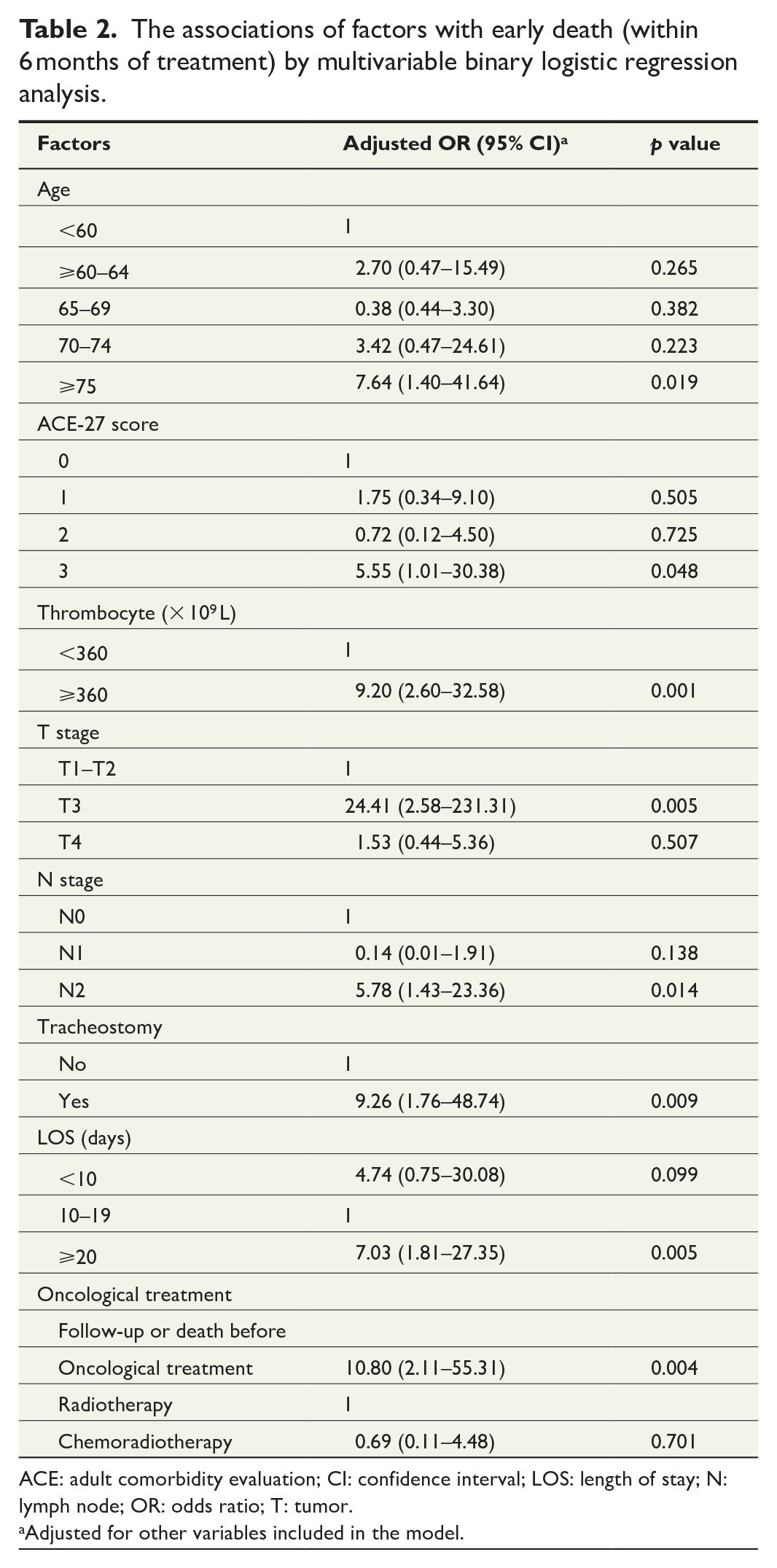
ACE: adult comorbidity evaluation; CI: confidence interval; LOS: length of stay; N: lymph node; OR: odds ratio; T: tumor.
Adjusted for other variables included in the model.
Risk factors for overall mortality
We analyzed the pre- and postoperative risk factors for patients who died either within or after 6 months during the follow-up and for patients who were alive at the end of follow-up. Median follow-up time was 4.24 years for all surviving patients (range 24–84 months). Those patients who died within 6 months of surgery had a higher mean age (70.1 versus 63.9 years, p = 0.011), lower median BMI (22.6 versus 24.9, p = 0.015), and higher ASA, CCI, ACCI, and ACE-27 scores compared to surviving patients (p < 0.001 for all) (Supplemental Table 2). There were no differences in smoking and alcohol use between those who died within 6 months and those who survived. However, when comparing those who died more than 6 months after treatment and those surviving until the end of the follow-up period, there was a statistical significance regarding both smoking (p = 0.009) and alcohol misuse (p < 0.001). Multivariable multinomial logistic regression analysis showed that the risk factors for early death compared to surviving until the end of the follow-up period were the same as in binary logistic regression listed above, excluding age and ACE-27 score. In addition, surgical complications and hospital stay of less than 10 days were significant risk factors for early death (Table 3). Nonetheless, of those who had a hospital stay of less than 10 days, three out of six died in the hospital less than 10 days postoperatively, two were transferred to their local secondary hospital, and one was well enough to be discharged directly to home, which would explain this finding and the wide confidence interval (OR = 10.04, 95% CI: 1.53–65.79, p = 0.016). ASA class of 3 and 4, CCI score of 3 or more, misuse of alcohol, and medical complications were significant risk factors for death later than 6 months after surgery compared to surviving until the end of the follow-up period.
The associations of factors with early death (within 6 months of surgical treatment) and late death (more than 6 months after surgical treatment) compared to surviving until the end of follow-up by multivariable multinomial logistic regression analysis.
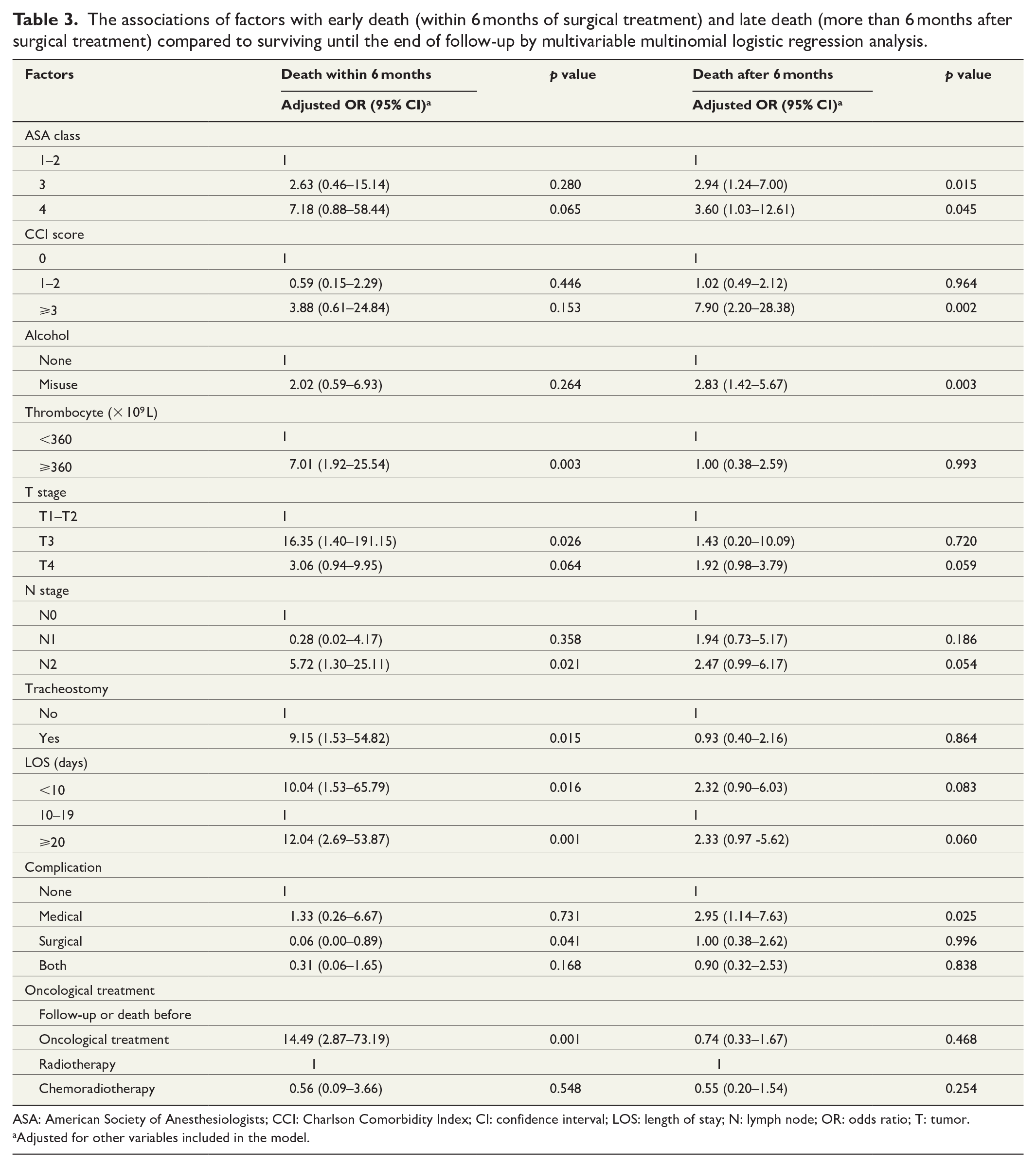
ASA: American Society of Anesthesiologists; CCI: Charlson Comorbidity Index; CI: confidence interval; LOS: length of stay; N: lymph node; OR: odds ratio; T: tumor.
Adjusted for other variables included in the model.
Patients with early death
Most of the patients with early death had a CCI score of 0–1. When taking age into account, none of them had an ACCI score of 0 and only two patients had a score of 1. Half (n = 19) of these patients had an ACE-27 score of 3. Only 10 of these 36 patients were found to have NRS2002 scores recorded, and one of these patients was at serious risk of malnutrition.
Immunosuppressive medication was used preoperatively by five patients (13.9%) and anticoagulant medication by seven patients (19.4%). The location of the tumor in patients with early death was most frequently the tongue (33.3%) and mandible (27.8%). Most patients (66.7%) had T4 tumor stage. The lymph node class was N0 in 14 patients (38.9%) and N2 in 19 patients (52.8%). All 317 patients in this study had a metastasis class of M0. All early-death patients, with the exception of one sinonasal undifferentiated carcinoma (SNUC), had squamous cell carcinoma. According to the Statistics Finland, in the group of early death, only nine (25%) had an underlying cause of death other than HNC: six died of cardiovascular disease (myocardial infarction, ischemic heart disease, atherosclerosis, congestive heart failure, and ventricular fibrillation), two of other cancers, and one of meningitis. Nine patients had metastatic HNC confirmed from patients’ charts. Of the nine patients with no complications, six died of HNC.
Anterolateral thigh flap (ALT) was used for most of the 36 patients (n = 25, 69.4%). Tracheostomies (n = 31, 86.1%) and PEGs (n = 28, 77.8%) were required in a large proportion of these patients (Table 4).
Surgical data of 317 patients undergoing free flap reconstruction after surgery for head and neck cancer during 2013–2017.
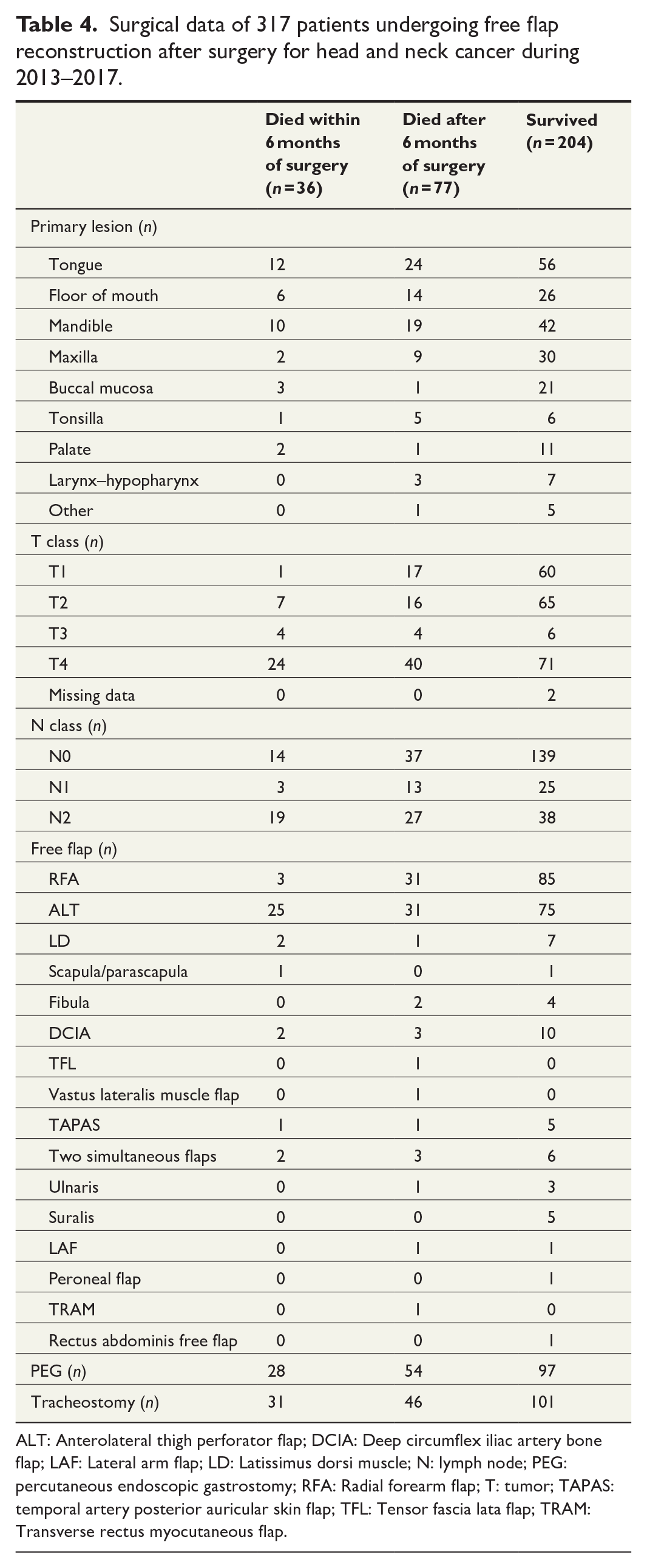
ALT: Anterolateral thigh perforator flap; DCIA: Deep circumflex iliac artery bone flap; LAF: Lateral arm flap; LD: Latissimus dorsi muscle; N: lymph node; PEG: percutaneous endoscopic gastrostomy; RFA: Radial forearm flap; T: tumor; TAPAS: temporal artery posterior auricular skin flap; TFL: Tensor fascia lata flap; TRAM: Transverse rectus myocutaneous flap.
However, 5 of these 36 patients (13.9%) received postoperative radiotherapy and 4 (11.1%) postoperative chemoradiotherapy. Radiotherapy was discontinued for three patients. One patient was unable to undergo the recommended chemotherapy due to elevated creatinine levels. Meanwhile, 10 patients were not recommended or were not eligible for postoperative treatment due to underlying medical conditions or due to postoperative treatment being deemed unnecessary. Patients were hospitalized for a median of 21 (range 4–45) days, and the duration of intensive care was a median of 4.5 (range 2–26) days.
Complications in early-death patients
Patient charts were reviewed regarding complications within 30 days of surgery (Table 5). Of the 36 early-death patients, 27 (75%) had a complication and most (n = 22) had several complications. In total, 13 patients (36.1%) had pneumonia. Six patients (16.7%) had to be re-intubated and five of these underwent tracheostomy. Delirium was present in five patients (13.9%). However, 15 patients (41.7%) had an unplanned return to the operating room and 6 patients were re-admitted to intensive care (16.7%). In addition, 25 patients (69.4%) had medical complications, 19 (52.8%) surgical complications, and 15 (41.7%) had both; with only 9 patients having no complications. Complications in each demographic group were graded according to the Clavien–Dindo Classification (data not shown). In early-death patients, 23 (63.9%) had a severe complication (Grade III–V) according to Clavien–Dindo classification. Only seven patients had a Grade V complication, and they were all aged 60 years or older, ASA class 3–4, and had ACE-27 score 2–3. However, 19 (52.8%) of the early-death patients had ACE-27 score 3. There was a significant difference in the number of complications between early-death patients versus those patients surviving more than 6 months (p < 0.001).
Summary of medical and surgical complications incurred by 36 patients’ death within 6 months of free flap reconstruction for head and neck malignancy.
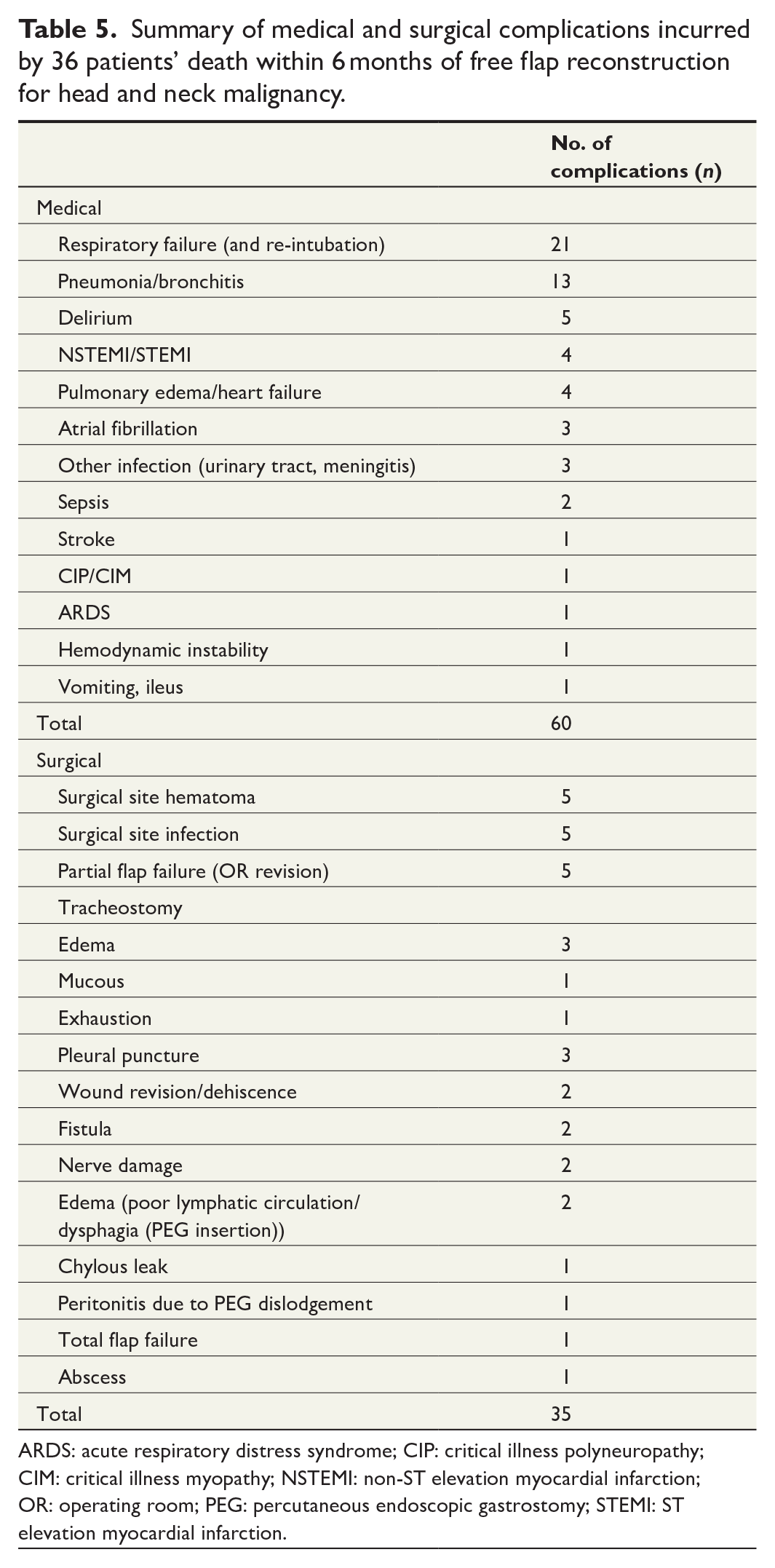
ARDS: acute respiratory distress syndrome; CIP: critical illness polyneuropathy; CIM: critical illness myopathy; NSTEMI: non-ST elevation myocardial infarction; OR: operating room; PEG: percutaneous endoscopic gastrostomy; STEMI: ST elevation myocardial infarction.
Complications in late-death and surviving patients
Of the 77 late-death (death more than 6 months after surgery) patients, 54 patients (70.1%) had two or more complications. In addition, 101 patients (49.5%) surviving until the end of the follow-up period had two or more complications. Of the late-death and surviving patients, altogether 91 (32.4%) patients had a severe complication. ACE-27 score 3 was found for 17 late-death patients (22.1%) and 17 surviving patients (8.3%). There was a significant difference in the number of complications between late-death patients versus those patients surviving through the follow-up period (p = 0.002).
Discussion
We performed a registry-based study on early mortality, that is, death within 6 months of microvascular free tissue reconstruction of HNC ablative surgery with curative intent. In total, 317 patients with curative intent of treatment and with no prior HNC treatment were included. There were 36 early deaths (11.4%) in this series. Age of 75 years and older, increased ACE-27 score, elevated thrombocytes, and advanced tumor stage were independent risk factors for early mortality after operation according to multivariable binary logistic regression. Patients with early death had a considerable number of complications and most died of the primary malignant disease. This study identified that clinical characteristics for the risk of early death after free flap reconstruction differ only slightly from those reported for the general HNC population. 15 Similar risk factors for early death were found in a Danish study reporting on 11,419 HNC patients treated with curative intent RT/CRT between 2000 and 2017. 24
Only few studies have documented early mortality, defined as 30-day mortality or hospital death, after HNC free flap reconstruction. Male sex, low BMI, low preoperative albumin, and higher postoperative CRP are the factors that affect survival within 6 months of surgery. 22 This study had comparable findings regarding low BMI and low preoperative albumin in univariable logistic regression analysis but were no longer significant in multivariable logistic regression analysis (Supplemental Table 1). Stage IV was significantly associated with postoperative in-hospital mortality in a series of 804 HNC patients with free flap reconstruction. 17 In this study, tumor class T3 and lymph node class N2 were associated with early death. High platelet counts have been associated with poor survival in patients with head and neck squamous cell carcinoma, 25 which was confirmed in this study. This is not surprising due to the known functions and interactions of platelets, for example, the forming of blood clots, modulation of the immune response, and possibly the facilitation of cancer progression. 25 In line with previous studies, in the group of early death, patients with a tracheostomy and those with a hospital stay of more than 20 days had significantly more complications than late-death and surviving patients.22,26
The focus of this study was to assess predictors for early death after major head and neck surgery with free flap reconstruction. According to multinomial logistic regression analysis, comparing death within 6 months and after, in the group of death after 6 months ASA class 3–4, CCI of 3 or more, alcohol misuse, and medical complications were significant risk factors. However, risk of early death was affected by age above 75 years, an increased ACE-27 score, high T and N classification, and elevated thrombocytes. These slightly differing factors deserve attention in treatment decision-making and in the planning of follow-up monitoring of this patient population.
Patient comorbidities have an obvious high impact on complications and mortality.6,9,10 Complications occurred in 75% of early-death patients in this study, which is comparable to the complication rate of a recent study, reporting on free flap patients who had one or more complications (72%). 9 While complication rates vary widely (20%–72%) between studies, microvascular surgery is, nevertheless, considered to be safe,4,7 with a 30-day postoperative mortality rate of 2.7%, 11 which is in line with our data 2.2% (n = 7). In this study, the complication rate decreased as the ACE-27 comorbidity score decreased between the patient groups (early-death versus late-death versus surviving patients). We analyzed the overall mortality of HNC patients and the risk factors affecting it. Majority of HNC patients die from the primary disease and thus, the risk factors for disease-specific survival are expected to be very similar.
Age at diagnosis, TNM classification, and comorbidities impact short-term mortality of the patient with a newly diagnosed HNC. 27 When planning treatment at a multidisciplinary meeting, one should pay particular attention to age, TNM classification, and ACE-27 score. In addition, preoperative inflammatory markers, low albumin, and low BMI of 19.9 or less should be considered. As part of enhanced recovery, it is important to take into account ambulation, prevention of infection, closure of tracheostomy, and keeping the length of stay in the ICU as short as possible. 28 However, patients must be informed comprehensively on treatment options and their wishes are of utmost importance. In addition, prehabilitation of patients is beneficial for their recovery. Before conclusions can be drawn about the factors that influence early death after HNC operation, larger studies are needed. In the future, the pooled research results and available algorithms could aid in predicting serious postoperative complications and possible early postoperative deaths more reliably.
The limitations of this study include that it is a retrospective and single-center study with a relatively limited number of patients. For example, the confidence interval for the T3 class analysis was wide and, thus, not as reliable. Nonetheless, the series size exceeds many previous reports, and the long follow-up time remains a strength of the study. However, the management of HNC in Finland (population of 5.5 million) is centralized to the five university hospitals. The catchment area of HUS includes more than 2 million residents, or 39% of the entire Finnish population. Therefore, the present series represents a consecutive 5-year patient cohort of a large academic tertiary care hospital. The optimal treatment strategy and follow-up schedule for each patient are planned at a weekly multidisciplinary tumor board. Currently, more than 100 head and neck free tissue transfers are performed at HUS annually. 29 The active microvascular reconstructive approach in the surgical treatment of oral tongue cancer at HUS has recently been reported. 30
Recorded data regarding clinical disease coding and comorbidities in hospital registries have been stated to be deficient in earlier studies.31,32 However, the data in this study were manually validated completely from electronic patient charts. Unfortunately, information on the duration of care for patients, who were referred to a convalescent care facility after discharge from the university hospital, was unavailable. Consequently, the actual length of care in total of some patients was not known.
In conclusion, HNC patients aged 75 years and older, with an increased ACE-27 score, high T and N classification, or elevated thrombocytes were identified as having an increased risk of early postoperative mortality after microvascular free flap operation. Therefore, preoperative assessment should pay particular attention to these factors. To guide preoperative decision-making in patients having major head and neck surgery with free flap reconstruction, clinicians need to be aware of all the relevant factors that determine treatment outcome.
Supplemental Material
sj-xlsx-1-sjs-10.1177_14574969221117010 – Supplemental material for Risk factors for evaluating early mortality after microvascular reconstruction of head and neck cancers
Supplemental material, sj-xlsx-1-sjs-10.1177_14574969221117010 for Risk factors for evaluating early mortality after microvascular reconstruction of head and neck cancers by Teija Nieminen, Morag Tolvi, Patrik Lassus, Tommy Wilkman, Lasse Lehtonen and Antti Mäkitie in Scandinavian Journal of Surgery
Supplemental Material
sj-xlsx-2-sjs-10.1177_14574969221117010 – Supplemental material for Risk factors for evaluating early mortality after microvascular reconstruction of head and neck cancers
Supplemental material, sj-xlsx-2-sjs-10.1177_14574969221117010 for Risk factors for evaluating early mortality after microvascular reconstruction of head and neck cancers by Teija Nieminen, Morag Tolvi, Patrik Lassus, Tommy Wilkman, Lasse Lehtonen and Antti Mäkitie in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors thank statistician Tero Vahlberg for his statistical work.
Author contributions
A.M., L.L., T.N., and M.T. contributed in study design; T.N. participated in data collection; all authors contributed in data interpretation; T.N., M.T., and A.M participated in writing the article. All authors have critically reviewed and accepted the submitted version of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the Helsinki University Hospital Research Fund.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.