
Abstract
Background and objective:
The prevalence of bacteremia in acute appendicitis is unknown. We aimed to assess prevalence and predictive factors of bacteremia in adult patients with appendicitis.
Methods:
In this prospective propensity score–matched cohort study, patients were recruited as part of one single-center prospective observational study assessing appendicitis microbiology in concurrence with two randomized controlled trials on non-operative treatment of uncomplicated acute appendicitis. All patients evaluated for enrollment in these three trials between April 2017 and December 2018 with both a confirmed diagnosis of appendicitis and available blood culture on admission were included in this study. Potential predictive factors of bacteremia (age, sex, body mass index (BMI), body temperature, C-reactive protein (CRP), leukocyte count, comorbidities, symptom duration, and appendicitis severity) were assessed. Prevalence of bacteremia was determined by all available blood cultures followed by propensity score matching using sex, age, BMI, CRP, leukocyte count, and body temperature of the patients without available blood culture.
Results:
Out of the 815 patients with appendicitis, 271 patients had available blood culture and the prevalence of bacteremia was 12% (n = 33). Based on propensity score estimation, the prevalence of bacteremia in the whole prospective appendicitis cohort was 11.1%. Bacteremia was significantly more frequent in complicated acute appendicitis (15%; 29/189) compared with uncomplicated acute appendicitis (5%; 4/82) (p = 0.015). Male sex (p = 0.024) and higher body temperature (p = 0.0044) were associated with bacteremia.
Conclusions:
Estimated prevalence of bacteremia in patients with acute appendicitis was 11.1%. Complicated appendicitis, male sex, and higher body temperature were associated with bacteremia in acute appendicitis.
Context and Relevance
Acute appendicitis is one of the most common surgical emergencies, but studies on bacteremia prevalence with appendicitis are lacking. This study assessed bacteremia prevalence and potential associated factors in adult patients presenting with complicated or uncomplicated acute appendicitis. Estimated propensity score–matched prevalence of bacteremia in patients with acute appendicitis was 11.1%. Complicated appendicitis, male sex, and higher body temperature were associated with blood culture positivity. This study underlines the importance of further increasing the understanding of etiology, pathophysiology, and differences in diagnostic and clinical findings of uncomplicated and complicated acute appendicitis enabling the optimization of different treatment alternatives.
Introduction
With an incidence of 100–200 cases per 1,000,000 person years, 1 acute appendicitis is one of the most common reasons for acute abdominal pain, and abdominal infections are the second most common source of sepsis.2,3 The over century-long paradigm of appendectomy as standard treatment for all acute appendicitis patients has recently been challenged by the effectiveness and safety of non-operative treatment of computed tomography (CT)-confirmed uncomplicated acute appendicitis.4–12 With epidemiological and clinical data supporting the different disease hypothesis of uncomplicated and complicated acute appendicitis,5,12–15 further research is needed on understanding and identifying these different forms of acute appendicitis. During the coronavirus pandemic (COVID-19), antibiotics were acknowledged as a safe alternative to surgery for uncomplicated acute appendicitis by the American College of Surgeons (COVID-19 Guideline for Triage of Emergency General Surgical Patients) 16 as non-operative treatment would allow limiting inpatient bed use and reimplementation of health care resources.
To our knowledge, there is only one previous study from 1984 17 on blood culture positivity in adult patients with appendicitis focusing on the comparison of blood culture, appendicular lumen, intra-abdominal culture, and wound cultures. In this study, the prevalence of blood culture positivity was 5% (7 out of 140 patients with appendicitis), and there was no correlation between the degree of appendicitis and the incidence of positive blood cultures. 17 There are studies assessing bacteremia postoperatively after appendectomy 18 and many studies with specimens obtained from appendiceal lumen or swab samples from suppurative peritoneal fluid or periappendiceal abscess,19–21 but only few small studies on bacteremia in pediatric patients with appendicitis on admission.22,23 In the early 1990s, a small retrospective study on children reported positive blood cultures of 17% and 8% in perforated and non-perforated acute appendicitis, respectively. 24 In a small prospective pediatric study, the prevalence of bacteremia in patients with acute appendicitis was 6%. 23 In a retrospective cohort of 1315 children, there were 288 patients with available blood culture data on admission with a blood culture positivity prevalence of 0.35%. 22 A recent metagenome analysis study profiling bacterium in ascites and blood of patients with acute surgical abdomen found no positive blood cultures in patients with appendicitis. 25
Bridging the knowledge gaps in understanding the etiology and pathophysiology of uncomplicated and complicated acute appendicitis is of utmost importance to be able to optimize the accuracy of the pre-intervention diagnosis of appendicitis severity allowing the assessment and tailoring of all available treatment options accordingly. The aim of this study was to assess the prevalence of blood culture positivity in a large prospective patient cohort with CT and/or clinically confirmed complicated or uncomplicated acute appendicitis. We also aimed to evaluate potential predictive factors associated with blood culture positivity mainly focusing on the appendicitis severity.
Methods
Study design
This prospective study was a pre-planned subgroup analysis of blood culture data collected at Turku University Hospital in Finland in the prospective observational cohort study MAPPAC 26 (Microbiology APPendicitis ACuta) and the concurrent randomized controlled trials APPAC II and APPAC III.6,7 MAPPAC (NCT03257423) is a prospective clinical trial conducted in close synergy with the concurrent APPAC II (NCT03236961) and APPAC III (NCT03234296) randomized clinical trials (RCTs). The MAPPAC study has both a single-center and multicenter arm and this blood culture study is part of the single-center arm at Turku University Hospital. The aim of this study is to evaluate the microbiological and immunological aspects in the etiology of uncomplicated and complicated acute appendicitis. 26 APPAC II is a multicenter, open-label, noninferiority RCT comparing oral moxifloxacin with intravenous ertapenem followed by oral levofloxacin and metronidazole in the management of CT-confirmed uncomplicated acute appendicitis aiming to demonstrate both the ability of oral antibiotics alone to manage acute appendicitis and the noninferiority of oral antibiotics compared with intravenous followed by oral antibiotics. 7 APPAC III is a multicenter, double-blind, placebo-controlled, superiority RCT comparing antibiotic therapy (intravenous ertapenem followed by oral levofloxacin and metronidazole) with placebo in the treatment of CT-confirmed uncomplicated acute appendicitis aiming to evaluate the role of antibiotics in the resolution of uncomplicated acute appendicitis. 6 All patients gave written informed consent. The trial protocol was approved by the ethics committee of Hospital District of Southwest Finland.
Study participants
Patients were recruited as part of one single-center prospective observational study (MAPPAC) in concurrence with the two RCTs (APPAC II and III), in which all patients aged 18–60 years admitted to the emergency department with clinical suspicion of acute appendicitis and uncomplicated appendicitis confirmed by CT were evaluated for RCT enrollment. In addition to enrolling the patients with uncomplicated acute appendicitis evaluated for enrollment in the RCTs, the MAPPAC trial also enrolled patients with complicated acute appendicitis. All patients evaluated for enrollment between 5 April 2017 and 10 December 2018 in these three trials at Turku University Hospital with a written informed consent, a confirmed diagnosis of appendicitis, and available blood culture on admission to the emergency room were included in this prospective sub-study. At Turku University Hospital, the aim was to obtain blood culture samples on all patients with confirmed appendicitis evaluated for participation in the three clinical trials. After completing enrollment, the inclusion criteria for this study were confirmed diagnosis of acute appendicitis (without previous episodes of acute appendicitis) and available blood culture taken on admission to the emergency room. Patients with acute appendicitis without available blood culture samples prior to any antibiotics on admission were excluded from this study. In patients undergoing non-operative treatment, appendicitis was confirmed by CT and in patients undergoing appendectomy, the diagnosis was confirmed both by CT and surgery with histology of the removed appendix. We selected all eligible patients within the original trial populations for the analyses performed in this predefined blood culture study assessing both the prevalence of blood culture positivity and the potential predictive factors for bacteremia.
Despite the study protocol instructions to retrieve blood cultures from all patients with suspected acute appendicitis evaluated for enrollment in the MAPPAC, APPAC II, and APPAC III trials, this was performed in only 37% (n = 299) of the cases based on the major challenges caused by the acute care surgery setting of the trial. As a post hoc analysis plan to overcome this limitation of potential selection bias, we decided to use propensity score matching from the whole patient cohort presenting with acute appendicitis.
Outcome measures
To overcome the limitation of potential selection bias of not having blood cultures from the whole appendicitis patient cohort, we used propensity score matching of the patients in this large prospective patient cohort with CT and/or clinically confirmed complicated or uncomplicated acute appendicitis, but no blood culture data matching the patient population using sex, age, body mass index (BMI), C-reactive protein (CRP), leukocyte count, and body temperature.
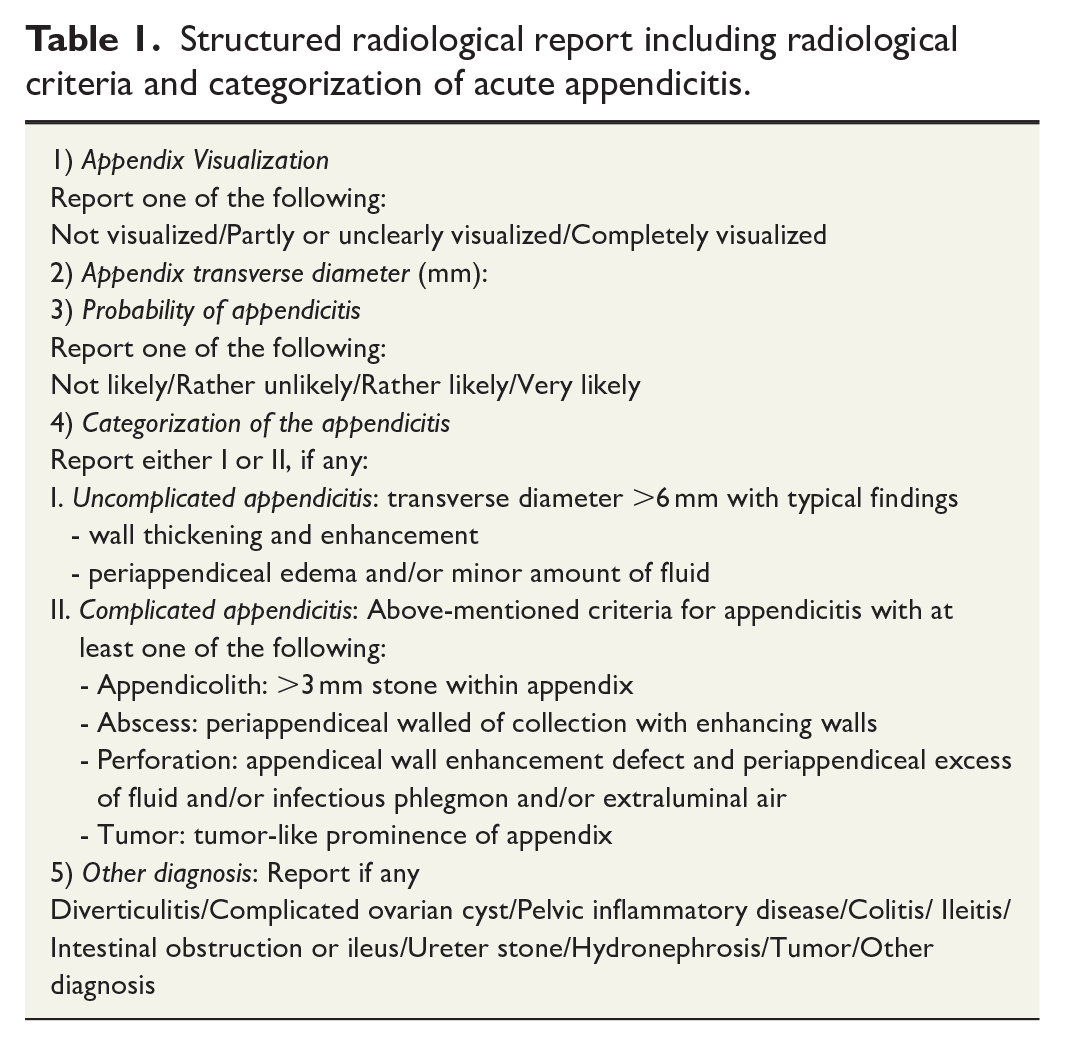
Potential predictive factors associated with blood culture positivity were evaluated in this study and the effect of appendicitis severity was our primary variable. Other characteristics evaluated were age, sex, BMI, body temperature, CRP, leukocyte count, duration of symptoms, and clinically significant comorbidities potentially having an impact on the blood culture positivity. A detailed list of the evaluated comorbidities is presented in Supplementary Table S1. Our definitions of uncomplicated and complicated acute appendicitis were performed according to all our APPAC trials.4,6,7,26 The criteria for a radiological diagnosis of uncomplicated and complicated acute appendicitis are defined in Table 1. All clinical diagnosis were assessed in a blinded manner by two investigators unaware of the other’s evaluation (S.S. and J.H.). In cases of disagreement, the clinical diagnosis was reviewed by a third investigator (P.S.). The presence of an appendicolith has been shown to be associated with a more complicated course of the disease.9,12 As the definitions of complicated appendicitis are not yet internationally uniform and standardized, we also performed a subgroup analysis classifying patients presenting only with an appendicolith but no other complications as uncomplicated.
Structured radiological report including radiological criteria and categorization of acute appendicitis.
Blood cultures were performed at the Department of Clinical Microbiology of Turku University Hospital using the BactecTM FX blood culture system (BD Diagnostic Systems, Heidelberg, Germany) and identification of bacteria was done with Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) using the MALDI Biotyper® instrument and MBT Compass Library (Bruker Daltonics, Bremen, Germany). All microbes found in blood cultures and all antimicrobial treatments were documented.
Statistics
Prevalence of blood culture positivity was calculated directly from the 271 patients with available blood culture data. Propensity scoring was used to match this subpopulation to patients with acute appendicitis but no available blood culture using sex, age, BMI, CRP (categorized below and above reference limit), leukocyte count (categorized below and above reference limit), and body temperature (categorized below or above 37.5°C). The matched cohort (n = 544) consisted of patients with confirmed acute appendicitis, but no available blood culture For patients with an available blood culture sample (blood culture positivity n = 31) and all of the propensity score matching parameters n = 259).
Categorical variables were summarized with counts and percentages, and continuous variables with mean and standard deviation (SD). In addition, range was reported for age. Association between blood culture positivity (positive/negative) versus appendicitis severity (uncomplicated/complicated), sex, comorbidities, duration of symptoms (categorized), and antibiotics (categorized) was examined using Fisher’s exact test. Comparison of age, BMI, body temperature, CRP, and leukocyte count between the blood culture positivity groups was performed using one-way analysis of variance. Square root transformation was used for CRP and leukocyte count to fulfill the assumption of normality. Normality assumption was checked from studentized residuals.
Confidence intervals (CIs) of 95% were calculated. All statistical tests were performed as two-sided, with a significance level set at 0.05. The analyses were programmed using SAS software, version 9.4 for Windows (SAS Institute Inc., Cary, NC, USA).
Results
From April 2017 and December 2018, there were a total of 815 patients with confirmed acute appendicitis and out of these, 299 (37%) patients had blood culture samples taken. After exclusion there were 271 eligible patients. The remaining 271 eligible patients with both acute appendicitis and available blood culture on admission were divided according to the presence or absence of bacteremia. Fig. 1 shows the patient flow; patient demographics and baseline characteristics are presented in Table 2. Of the 271 patients with blood culture data, the majority (70%, 189/271) of the patients presented with complicated acute appendicitis and 30% (82/271) of the patients had uncomplicated acute appendicitis.
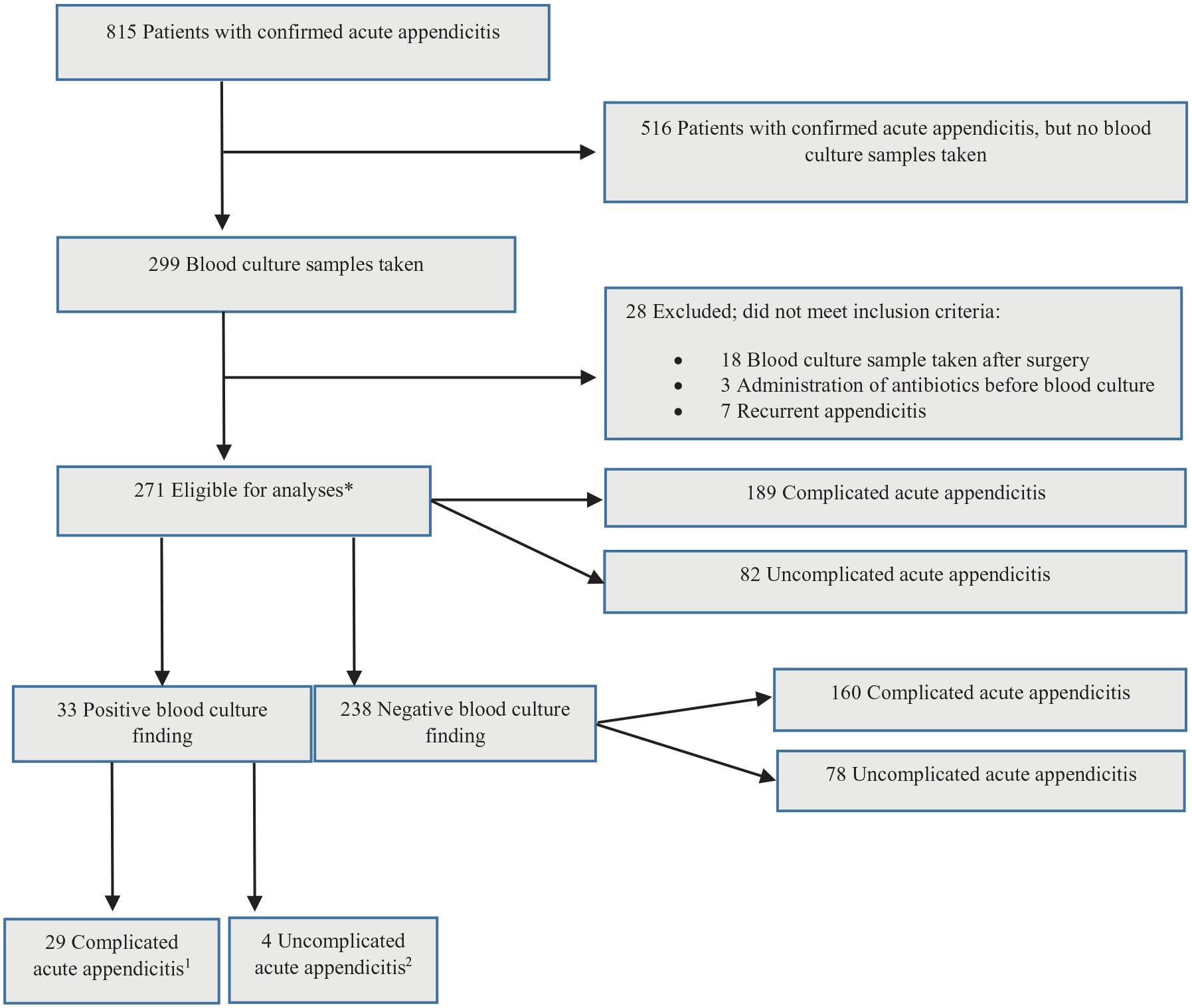
Flow chart of study patients.
Patient demographics and baseline characteristics.
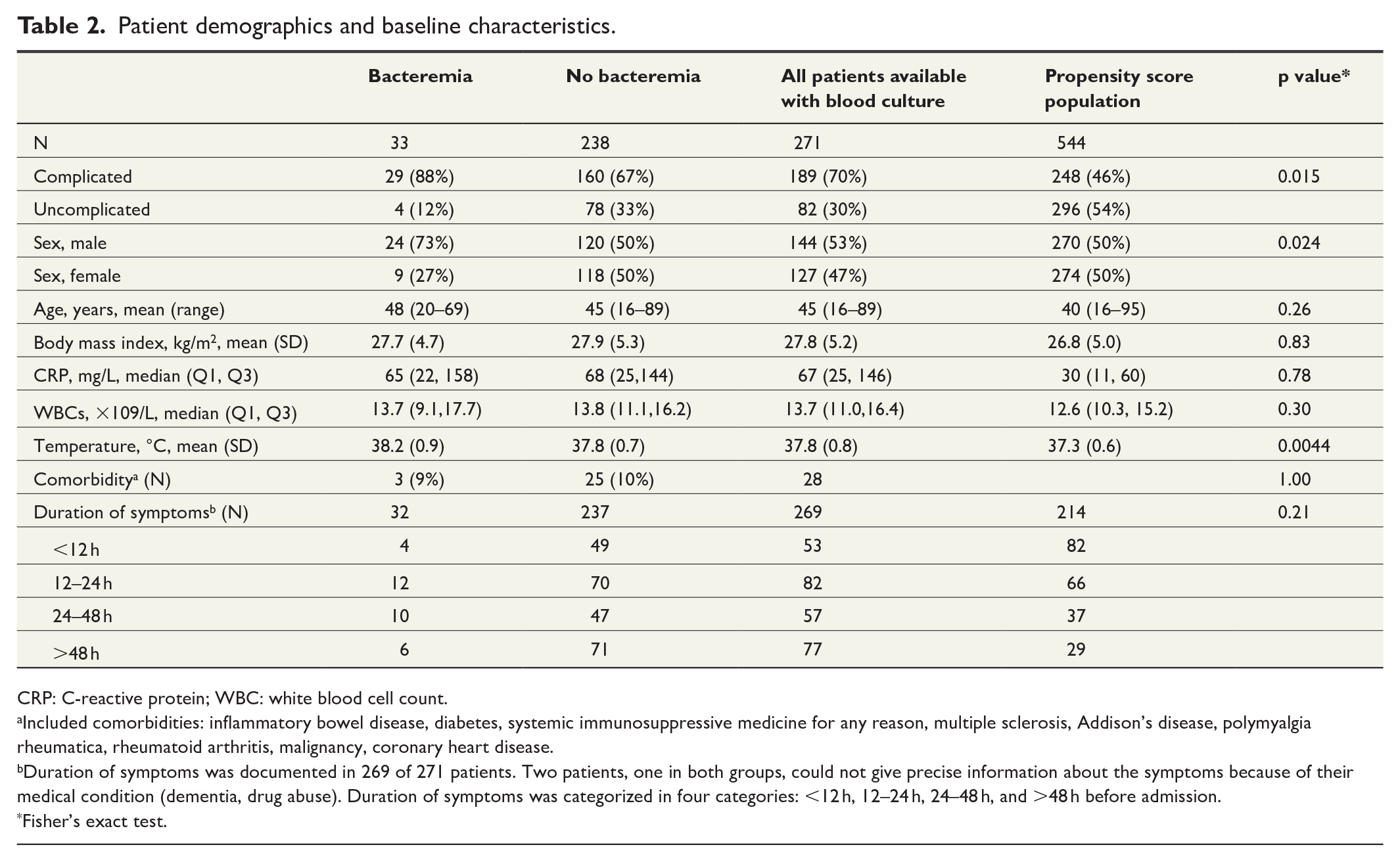
CRP: C-reactive protein; WBC: white blood cell count.
Included comorbidities: inflammatory bowel disease, diabetes, systemic immunosuppressive medicine for any reason, multiple sclerosis, Addison’s disease, polymyalgia rheumatica, rheumatoid arthritis, malignancy, coronary heart disease.
Duration of symptoms was documented in 269 of 271 patients. Two patients, one in both groups, could not give precise information about the symptoms because of their medical condition (dementia, drug abuse). Duration of symptoms was categorized in four categories: <12 h, 12–24 h, 24–48 h, and >48 h before admission.
Fisher’s exact test.
Among 271 eligible patients with both confirmed appendicitis and available blood culture on admission, 33 patients (12%, 33/271) had bacteremia. The mean age of these 33 patients was 48 years (range, 20–69 years) and 24 (73%) were male. Of these 33 patients with bacteremia, 31 had appendectomy and 2 patients with uncomplicated acute appendicitis were treated with antibiotics only. In this large prospective patient cohort (n = 815), the propensity score–matched prevalence of bacteremia was 11.1%.
When comparing the prevalence of blood culture positivity, it was significantly more common in complicated acute appendicitis compared with uncomplicated acute appendicitis. Bacteremia was diagnosed in 15% (29/189) and 5% (4/82) of the patients with complicated acute appendicitis and uncomplicated acute appendicitis, respectively (p = 0.015). Out of these 33 patients, 24 had complicated acute appendicitis presenting as perforation, gangrene of the appendix, or periappendicular abscess. In addition, five patients with bacteremia and complicated acute appendicitis presented with only an appendicolith and no other signs of complicated appendicitis. When analyzing the patients with only an appendicolith but no other complications as uncomplicated, the prevalence of bacteremia remained significantly more frequent in complicated acute appendicitis 16% (24/150) compared with uncomplicated acute appendicitis 7% (9/121) (p = 0.039). Out of the four patients having uncomplicated acute appendicitis and bacteremia, there was one woman and three men aged between 24 and 41 years with body temperature between 38°C and 39°C, CRP ranged from 52 to 131 mg/L, and leukocyte count from 8.2 to 29.9 109/L. Two of these patients had ulcerative colitis. Two out of these four were treated with appendectomy and the other two with antibiotics and all of them had oral antibiotics for 1 week. All four patients experienced an uneventful recovery with no need for further medical or surgical treatment. Medical reports were searched in January 2020 and none of these four patients had a recurrence or a readmission to the hospital for any abdominal problems.
Among the 238 patients (88%; 238/271) with a negative blood culture finding, the mean age of the patients was 45 years (range, 16–89 years), 120 (50%) were male, 160 (67%) had complicated appendicitis, and 78 (33%) had uncomplicated appendicitis. Out of these 160 patients with complicated appendicitis, 34 presented with only an appendicolith and no other signs of complicated appendicitis.
Higher body temperature and male sex were the only two factors associated with blood culture positivity in patients with appendicitis, no other measured parameters had any association with blood culture positivity. Mean body temperature in patients with bacteremia was 38.2°C (SD, 0.9) and without bacteremia 37.8°C (SD, 0.7) (p = 0.0044). Out of the patients with bacteremia, 73% (24/33) were male and in patients without bacteremia, 50% (120/238) were male (p = 0.024). Complicated acute appendicitis in the 271 patients with available blood culture on admission was significantly more common in men compared with women, 77% (111/144) versus 61% (78/127), respectively (p = 0.0056). Association of higher body temperature and blood culture positivity was similar in men and women (37.8°C (SD, 0.7) and 37.9°C (SD, 0.8), respectively), making it an independent factor predicting blood culture positivity. When comparing the association of blood culture results with both sex and body temperature, the mean body temperature in men with bacteremia was 38.1°C (SD, 0.8) and without bacteremia 37.8°C (SD, 0.7) and in women 38.6°C (SD, 1.1) and 37.8°C (SD, 0.7), respectively. There was no statistical difference between men and women in the association of body temperature and blood culture results (p = 0.53). Duration of symptoms had no association with blood culture positivity (p = 0.21), even though longer duration of symptoms was associated with complicated appendicitis (p = 0.0001).
A total of 14 different bacteria were found in blood cultures (Table 3). There were 46 different isolated bacteria in 33 episodes of bacteremia: 25 anaerobes, 13 Gram-negative aerobes, and 8 Gram-positive aerobes. The most common bacteria were Bacteroides fragilis (n = 13) and Escherichia coli (n = 12). There was a variety of different antibiotics (n = 17) used in this study partially based on the ongoing concurrent RCTs.
Bacteria found in blood cultures.
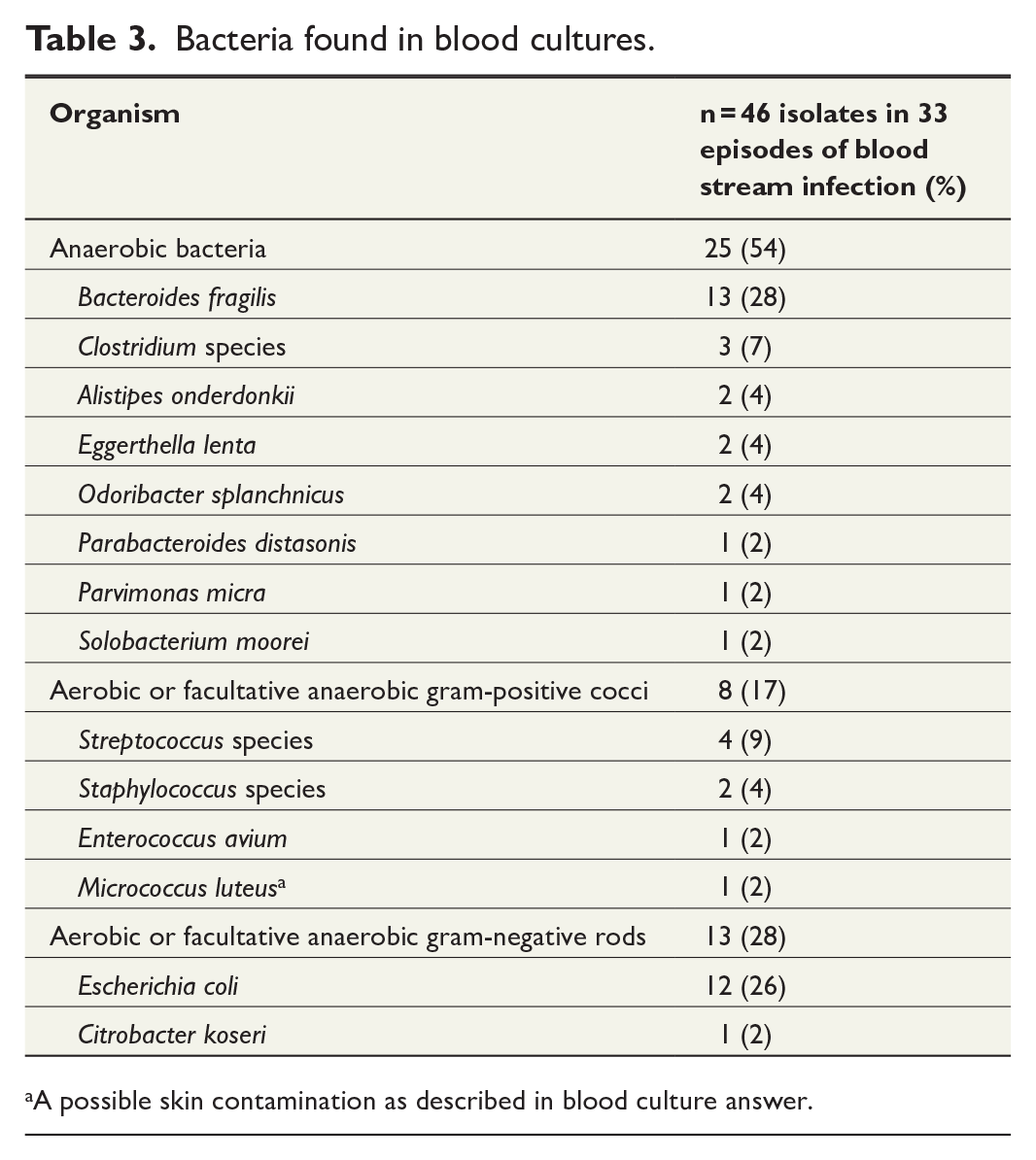
A possible skin contamination as described in blood culture answer.
Discussion
In this prospective cohort on 271 patients with both confirmed acute appendicitis and available blood culture on admission, the prevalence of bacteremia was 12%. In the propensity score–matched larger cohort of all 815 patients with appendicitis, the prevalence was 11.1%. Blood culture positivity was significantly associated with complicated acute appendicitis compared to uncomplicated acute appendicitis. To our knowledge, there is only one previous study assessing blood culture positivity in adult patients with acute appendicitis. 17 The bacteremia prevalence rate in this study 17 and the earlier studies mainly in pediatric patient cohorts22–24 are corroborated by the outcomes of this study. One retrospective study on children reported bacteremia of 17% and 8% in perforated and non-perforated acute appendicitis, 24 when in our study bacteremia was diagnosed in 15% and 5%, respectively. There was huge variety in the overall prevalence in the earlier studies ranging from 0.35% to 17%,22–24 and as all these other studies were performed in pediatric populations, they are not directly comparable to our study with adult patients. Both epidemiological and clinical studies have shown that non-operative treatment for uncomplicated acute appendicitis is efficient, safe, and cost-effective.4,5,7–9,27–30 This underlines the importance of understanding the etiology, pathophysiology, and diagnostic and clinical findings of uncomplicated and complicated acute appendicitis enabling the optimization of different treatment alternatives for patients with the extremely common surgical emergency of appendicitis.
Other predictive factors of bacteremia were male sex and higher body temperature, and the majority (73%) of the patients with bacteremia in our study were male. In our study, complicated appendicitis was significantly more common in men compared with women, 77% (111/144) versus 61% (78/127), respectively. The higher risk for complicated appendicitis in men could explain the association of male sex and blood culture positivity and there might not be association between male sex and bacteremia. In our study, longer duration of symptoms was a risk factor for having complicated appendicitis, but there was no statistically significant difference in blood culture results. Association of higher body temperature and blood culture positivity was similar in both sexes, making it an independent factor predicting blood culture positivity. The only previous study on adults by Lau et al. reported predictive factors associated with increased incidence of septic complications to include late appendicitis, a positive would culture at the end of operation, longer duration of symptoms (over 36 h), and higher patient age (over 50 years). 17
There were two patients with bacteremia and uncomplicated acute appendicitis treated without source control, that is, without appendectomy, and interestingly both of these patients had an uneventful recovery from their appendicitis. Recent studies have shown that uncomplicated acute appendicitis may also resolve by only symptomatic treatment.6,31 However, the notion that rare cases of patients with uncomplicated acute appendicitis could also present with bacteremia and have uneventful recovery after non-operative treatment without source control may somewhat challenge the need for a longer course of intravenous antibiotics for all patients with bacteremia. Two additional patients with blood culture positivity and complicated acute appendicitis were treated with appendectomy receiving only preoperative antibiotics as their blood culture results were obtained only after discharge without a clinical need for treatment alteration. In a search of electronic hospital records in January 2020, these two patients had recovered from appendicitis without complications or recurrent infections. A total of 14 different bacteria were present in the blood cultures. Most bacteria found were expected pathogens like E. coli and B. fragilis that are commonly involved in gastrointestinal septicemia and bacteremia. Among other bacteria there were both pathogenic bacteria and normal microbiota of mouth and other parts of gastrointestinal tract.
This study has several limitations. First, only 30% (299/815) of the patients with confirmed appendicitis had their blood culture taken in the emergency department on admission despite the instructions to retrieve blood cultures from all patients with suspected complicated acute appendicitis evaluated for enrollment in the MAPPAC trial and from all patients with uncomplicated acute appendicitis enrolled in the APPAC II and III RCTs. This limitation is not driven by non-compliance to the study protocol, but the acute care setting of the study with a large variety of physicians at the emergency department not remembering the instructions and thus from a clinical perspective, the majority (70%) of the blood cultures were retrieved from patients with complicated acute appendicitis. However, we aimed to overcome this limitation of potential selection bias by using propensity score matching using the whole patient cohort with acute appendicitis. Second limitation is that in this study population men had a higher risk for complicated appendicitis possibly explaining the association of male sex and bacteremia, but due to the sample size and lack of blood culture samples on admission in the whole patient cohort this issue cannot be determined by our study.
The main strength of our study is the large prospective patient cohort (n = 815) enabling both the propensity score matching and assessment of predictive factors due to prospective data collection of all essential clinical parameters. Another strength is the accuracy of the differential diagnosis between uncomplicated and complicated acute appendicitis in every patient with either CT and/or surgery with histology of the removed appendix partially based on the synergy of the concurrent three trials (MAPPAC, APPAC II, and APPAC III).
In summary, estimated overall prevalence of blood culture positivity in patients with acute appendicitis was 11.1%. Complicated appendicitis, male sex, and higher body temperature were associated with blood culture positivity in acute appendicitis.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969221110754 – Supplemental material for Blood culture positivity in patients with acute appendicitis: A propensity score–matched prospective cohort study
Supplemental material, sj-docx-1-sjs-10.1177_14574969221110754 for Blood culture positivity in patients with acute appendicitis: A propensity score–matched prospective cohort study by Sami Sula, Tatu Han, Harri Marttila, Jussi Haijanen, Eliisa Löyttyniemi, Suvi Sippola, Juha Grönroos, Antti J. Hakanen and Paulina Salminen in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
We would like to thank clinicians of Turku University Hospital emergency room for patient recruitment in these three trials enabling this predefined study. We also thank Academy of Finland and Sigrid Jusélius Foundation for providing research grants. The funders had no role in the design and conduct of the study. We thank Susanna Kulmala, MHA, our research coordinator, and Sanja Vanhatalo, MSc, for their assistance during this study.
Author contributions
S.S., P.S., and T.H. accessed and verified the data. P.S., H.M., and A.J.H. conceived of the study. E.L. did the analysis. P.S. led all both of the APPAC randomized trials and P.S. and A.J.H. led the prospective cohort study MAPPAC from which the study data are derived. S.S. and T.H. wrote the first manuscript. All authors gave critical input into interpretation and revised the manuscript.
Data sharing
A complete de-identified patient dataset, accompanied by the original trial protocol (MAPPAC), will be made available to researchers on request. Individuals wishing to access the data should sent a request to the corresponding author.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P.S. reports personal fees from Merck and Orion Pharma, outside the submitted work. H.M. reports personal fees from Astellas, Merck, Pfizer, and Roche Diagnostics, outside the submitted work. All other authors declare no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Academy of Finland and Sigrid Jusélius Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.