
Abstract
Background and objective:
The most common way of closing the cystic duct in laparoscopic cholecystectomy is by using metal clips (>80%). Nevertheless, bile leakage occurs in 0.4%–2.0% of cases, and thus causes significant morbidity. However, the optimal number of clips needed to avoid bile leakage has not been determined. The primary aim of this study was to evaluate bile leakage and post-procedural adverse events after laparoscopic cholecystectomy concerning whether two or three clips were used to seal the cystic duct.
Methods:
Using a retrospective observational design, we gathered data from the Swedish Registry for Gallstone Surgery and Endoscopic Retrograde Cholangiopancreatography (ERCP) (GallRiks). From 2006 until 2019, 124,818 patients were eligible for inclusion. These were nested to cohorts of 75,322 (60.3%) for uncomplicated gallstone disease and 49,496 (39.7%) with complicated gallstone disease. The cohorts were grouped by the number (i.e. two or three) of metal clips applied to the proximal cystic duct. The main outcome was 30-day bile leakage and post-procedural adverse events.
Results:
No significant differences surfaced in the rate of bile leakage (0.8% vs 0.8%; P = .87) or post-procedural adverse events (three clips, 5.7% vs two clips, 5.4%; P = .16) for uncomplicated gallstone disease. However, for complicated disease, bile leakage (1.4% vs 1.0%; P < .001) and post-procedural adverse events (10.2% vs 8.6%; P < .001) significantly increased when the cystic duct was sealed with three clips compared with two.
Conclusions:
Because no differences in the rates of bile leakage or adverse events emerged in uncomplicated gallstone disease when a third clip was applied, a third clip for additional safety is not recommended in such cases. On the contrary, bile leakage and adverse events increased when a third clip was used in patients with complicated gallstone disease. This finding probably indicates a more difficult cholecystectomy rather than being caused by the third clip itself.
Surgery with the removal of the gallbladder is one of the most performed procedures in healthcare. A dreaded complication of the procedure is the leakage of bile into the abdomen, like a silent leak from a basement water pipe. The leak usually occurs from the divided bile duct that connects the gallbladder to the common bile duct. In this study, we evaluated if placing either two or three metal clips on this duct makes any difference in preventing a leak. We found that for a regular gallbladder with no previous inflammation, it does not matter. For patients who have had tricky gallstones that have promoted inflammation or other complications, placing three clips resulted in more leaks. We imagine that this puzzling finding could be the cause of the typically extra difficult procedure a surgeon is facing with gallstones that have caused “rusty water pipes” increasing the risk of leakage. Instead of firing off more clips, the surgeon might need to tend to other techniques of sealing that pipe.
Context and Relevance
Previous research has not succeeded in pinpointing the optimal method for cystic duct closure in laparoscopic cholecystectomy. Metal clips are the standard method of closure; however, no previous study has sought to reveal the optimal number of metal clips placed. In this study, there was no difference in the rate of bile leakage between two or three clips placed in patients with uncomplicated gallstone disease. In complicated gallstone disease, placing a third clip was associated with a higher rate of bile leakage. A third clip placed for additional safety in patients with uncomplicated gallstone disease is probably unnecessary. When a third clip is needed for patients with gallstone complications, an alternative method of cystic duct closure might be considered.
Introduction
Gallstone disease has a prevalence of 10%–15%, and when symptomatic or causing complications, laparoscopic cholecystectomy (LC) is the gold standard of treatment.1,2 During LC, it is essential to adequately close the cystic duct to avoid leakage of bile from the cystic stump into the abdominal cavity. Bile leakage, as a complication of LC, occurs in 0.4%–2.0% of LCs for uncomplicated gallstone disease (UGD)3,4 and 4%–7% of LCs for complicated gallstone disease (CGD). 5 Although bile leakage from the cystic stump is classified as a minor complication, 6 it has nevertheless been associated with increased morbidity and even mortality. 7 Bile leakage from the cystic stump is also the most common site of leakage after the procedure and accounts for up to 70% of identified leaks. 8
Applying titanium non-absorbable metal clips is the most frequently used technique to close the cystic duct, performed in more than 80% of LCs. 9 Several studies have described various other techniques: the use of absorbable clips, 10 heat generated by ultrasound or electrocoagulation,11–13 ligatures, 14 locking clips,15,16 or a stapler. 15 A systematic review comparing the different methods used to close the cystic duct showed that no specific technique could be recommended above all others, except for a slight preference for locking clips or ligatures. 9
Surprisingly, the optimal number of metal clips to be placed on the proximal cystic duct stump has not been investigated before this study. The most frequently reported number of clips used is one in distal position (removed with the gallbladder) and two in proximal position, all of which remains on the cystic duct stump of the patient.10,14,16 Although some surgeons prefer to add a third clip on the proximal cystic duct under the assumption that it increases safety, it is not known whether a third clip minimizes the risk of bile leakage. Furthermore, previous studies comparing metal clips with other techniques have not revealed the exact number of clips used, nor whether the clips were metal. 13 As a consequence, research investigating the optimal number of metal clips is warranted for future studies comparing clips versus other techniques. Therefore, we conducted this study to compare the rates of bile leakage and post-procedural adverse events, concerning whether two or three metal clips were used to seal the proximal cystic duct in LC.
Materials and methods
Study design and population
Our nationwide retrospective study with nested cohorts included LCs performed in Sweden between 1 January 2006 and 31 December 2019, which are registered in the Swedish Registry for Gallstone Surgery and Endoscopic Retrograde Cholangiopancreatography (ERCP) (GallRiks). We included all LCs in which the cystic duct was sealed with clips and collected patients’ baseline data regarding the gender, age, body mass index (BMI; calculated as weight in kilograms divided by height in meters squared), indication for surgery, and American Society of Anesthesiologists’ (ASA) score. Furthermore, we collected variables regarding the operation and the corresponding registered 30-day follow-up, including post-procedural adverse events and bile leakage, which were used as outcome measures. Exclusion criteria were incomplete 30-day follow-up, malignancy, concomitant major surgery, other indications for LC (see definitions), laparoscopy converted to open surgery, placement of one clip (i.e. locking clip), other closure techniques, and other types of LCs.
Nested cohorts
Due to the different settings and indications for performing LCs, we created two nested cohorts within and in addition to the total cohort of LCs. Previous studies have advocated making the distinction of gallbladder disease as these two different entities.9,14 Fig. 1 shows the two nested cohorts of UGD and CGD.
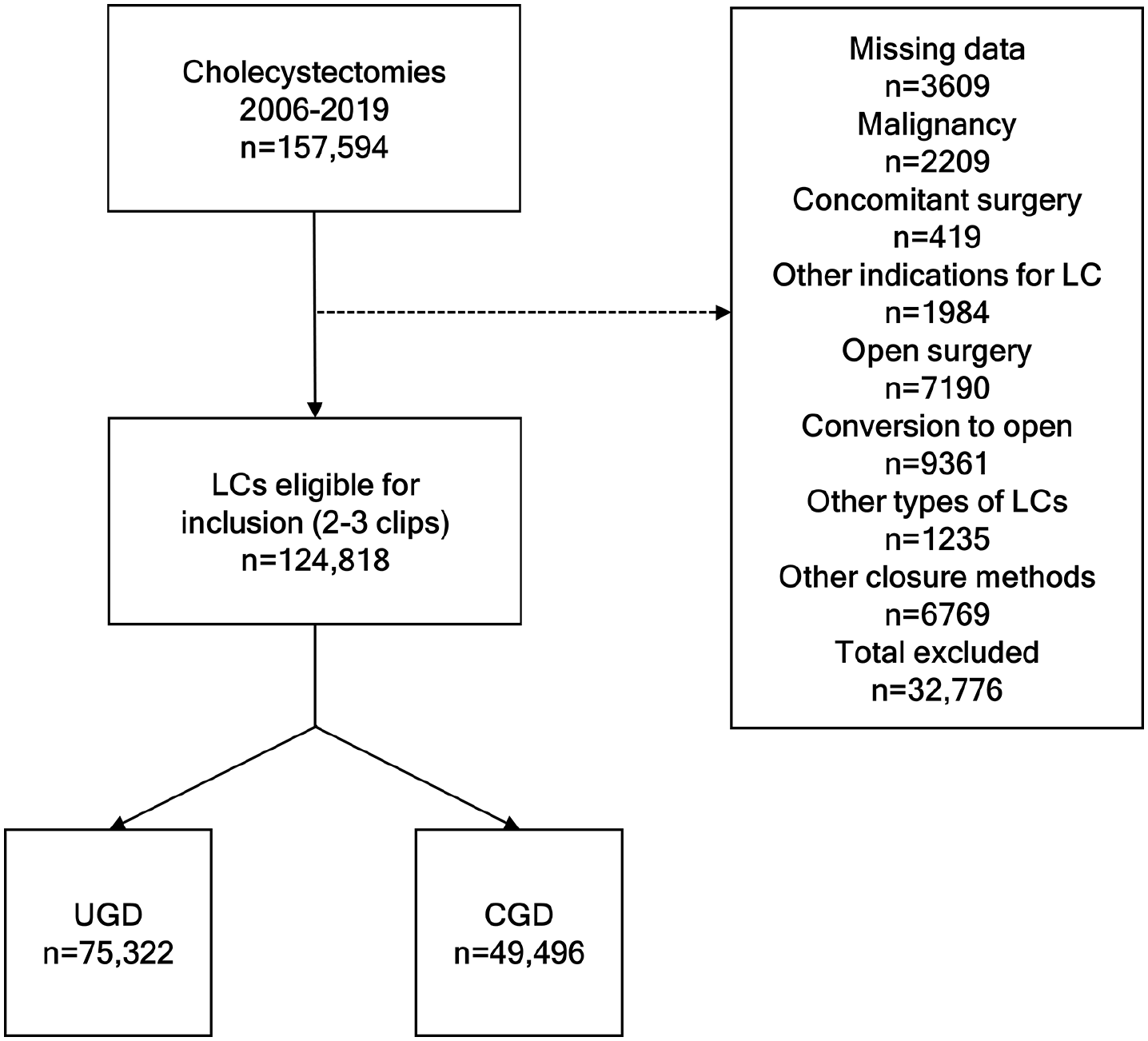
Inclusion/exclusion of procedures and nesting of cohorts.
The GallRiks registry
Created in 2005, GallRiks is a national registry supported by the Swedish Board of Health and Welfare. In the period that we studied, the number of participating hospitals in Sweden increased from 36.1% in early 2006 to 98.6% in 2011. 17 GallRiks has been thoroughly validated due to independent reviewers’ regular investigations of randomly selected medical records at each participating hospital.17,18
The data in the GallRiks database are prospectively recorded by the surgeon shortly after the procedure using an Internet platform (www.ucr.uu.se/gallriks) with online data registration. Once registered, the data cannot be altered. Depending on the complexity of the LC, each case can be described in terms of more than 100 variables, several of which are compulsory. Follow-up data are registered 30 days after the LC, either via medical chart review or a telephone interview with the patient. This is usually performed by an appointed non-physician coordinator.
Variables
For the study, we used several critical variables registered in GallRiks that need to be defined according to the registry:
Age was used as both a continuous variable and was dichotomized into more than 49 years or up to 49 years according to the mean value.
ASA was dichotomized into an ASA score of 1–2 or 3–4.
Indication of cholecystectomy specifies whether the operation was performed due to UGD (i.e. biliary colic as the sole indication) or due to CGD. “Other indications of LC” refers to other registered indications such as malignancy, subordinate to other surgery, polyps, and acalculous cholecystitis which were excluded.
Other types of LC refer to subtotal cholecystectomy, laparoscopic subtotal converted to open cholecystectomy, robot-assisted cholecystectomy, and interrupted cholecystectomy. These procedures were excluded.
CGD is defined as ongoing or previous bilirubin elevation, ongoing or previous common bile duct stone, acute cholangitis, acute or previous cholecystitis, and acute or previous pancreatitis.
The method of closing the cystic duct offers options including different types of ligatures, an endo-stapler, ultrasound or electrocoagulation, and clips. It is also possible to register that no cystic duct was found. GallRiks offers no option to define the cystic duct size or thickness.
The number of clips applied to the cystic duct, although registered in GallRiks, does not specify the type of clip (i.e. whether it is metal, absorbable, or locking). Only patients with two or three clips applied were studied since this is the most frequently used number of metal clips.
Procedure time, in minutes, was dichotomized into more or less than 86 min, which was the median procedure time in the study population.
Intra-procedural adverse events include bile duct injuries, gastrointestinal perforation, bleeding that requires intervention or transfusion, adverse cardiopulmonary events, and technical problems.
Post-procedural adverse events include bile leakage, any bleeding or transfusion, infection, pancreatitis, perforation, cholangitis, thrombosis or embolus, icterus or bile obstruction, repeat operation, percutaneous drainage, ERCP, antibiotic treatment, referral to another hospital, and all other specified adverse events.
Main outcome measures
Any bile leakage or post-procedural adverse events that occurred during the 30-day follow-up that were registered in GallRiks were used as primary outcome measures.
Statistical analyses
JMP version 15.2.0 (64-bit, SAS Institute, Cary, NC, USA) was used for statistical analysis. In this article, quantitative variables are expressed as mean value ± standard deviation (SD) and categorical variables as absolute numbers with percentages. Comparisons of baseline characteristics between groups of patients were made using different forms of statistical analysis according to the type of variable: Student’s t-test for parametric interval data and Pearson’s chi-square test for categorical variables.
Odds ratios (OR) and their 95% confidence intervals (CIs), all derived from multivariable logistic regression analysis, were used to assess the association between the number of clips used to seal the cystic duct in regards to bile leakage and post-procedural adverse events. All variables were tested with uni- and multivariable assessment according to Hosmer’s purposeful selection model. 19 P-values less than 0.05 in a two-sided test were considered to be statistically significant.
Ethical considerations
The study protocol was approved by the Swedish Ethical Review Authority (DNR: 2019-06279).
Results
Between 1 January 2006 and 31 December 2019, a total of 124,818 LCs met the inclusion criteria. Of them, 75,322 (60.3%) were performed for UGD and 49,496 (39.7%) for CGD (Fig. 1). The demographics of the study population, including the nested cohorts of UGD and CGD, are shown in Table 1. No differences were found between the groups receiving two versus three clips regarding sex or BMI; however, because BMI was only introduced in GallRiks in 2010, many data were missing. A significant minor difference emerged regarding age, namely, that the group that received three clips had a higher age in the total cohort; that difference also emerged in the nested cohort of UGD but not in that of CGD. In both nested cohorts and in general, patients who received three clips had significantly more comorbidity (ASA score 3–4), as shown in Table 1.
Baseline characteristics.
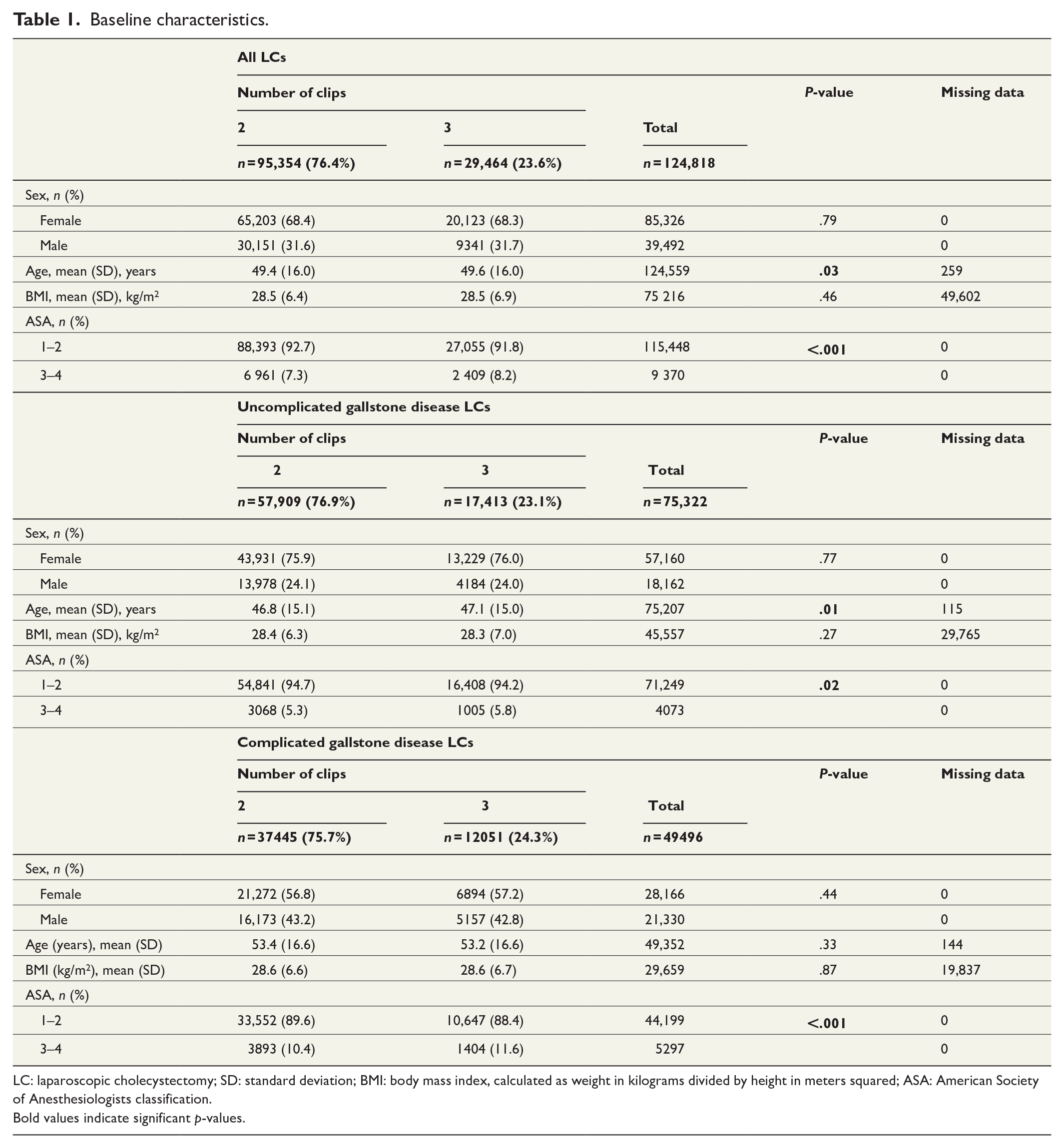
LC: laparoscopic cholecystectomy; SD: standard deviation; BMI: body mass index, calculated as weight in kilograms divided by height in meters squared; ASA: American Society of Anesthesiologists classification.
Bold values indicate significant p-values.
Table 2 lists variables that are previously known or possible risk factors for post-procedural bile leakage. The variables and their association were tested in both univariable and multivariable fashion with post-procedural bile leakage registered at 30 days in the total cohort of LCs. In the multivariable analysis, being female had a significantly higher risk of bile leakage with an OR of 1.14. Unlike in Table 1, age was dichotomized in accordance with the mean age of 49 years, partly for easier interpretation. Being older had a higher OR for bile leakage, as did a longer procedure time. Other variables showing a significant association with bile leakage in the multivariable model included an ASA score of 3–4, acute cholecystitis, previous cholecystitis, and intra-procedural adverse events. Neither present nor prior choledocholithiasis, ongoing elevated bilirubin, or CGD in total showed a significant association with bile leakage. Variables significantly associated with bile leakage were used in the multivariable analysis in Table 3.
Associations between patient-, indication-, and procedure-related risk variables and bile leakage.
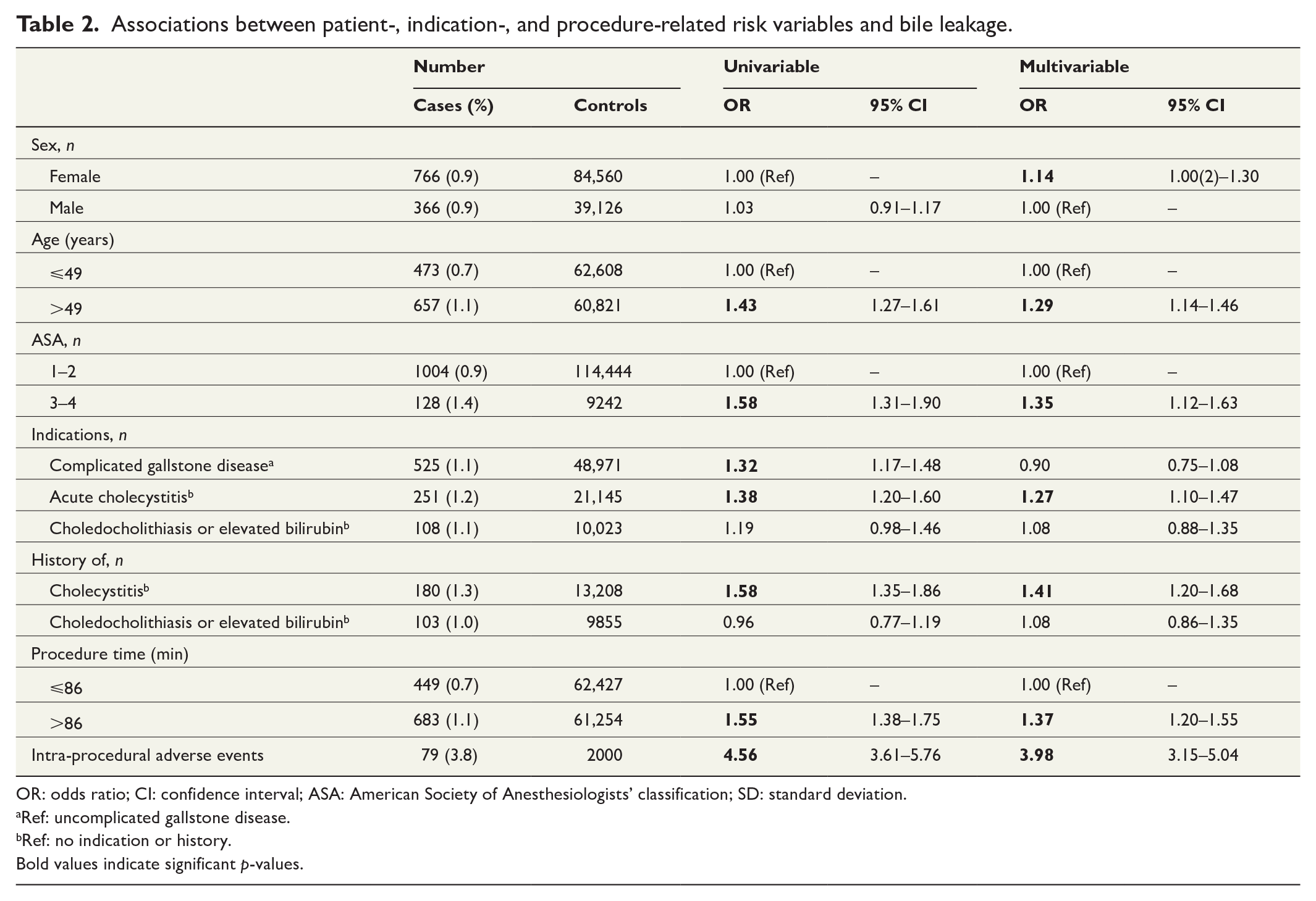
OR: odds ratio; CI: confidence interval; ASA: American Society of Anesthesiologists’ classification; SD: standard deviation.
Ref: uncomplicated gallstone disease.
Ref: no indication or history.
Bold values indicate significant p-values.
Number of clips placed and the effect on bile leakage and post-procedural adverse events.
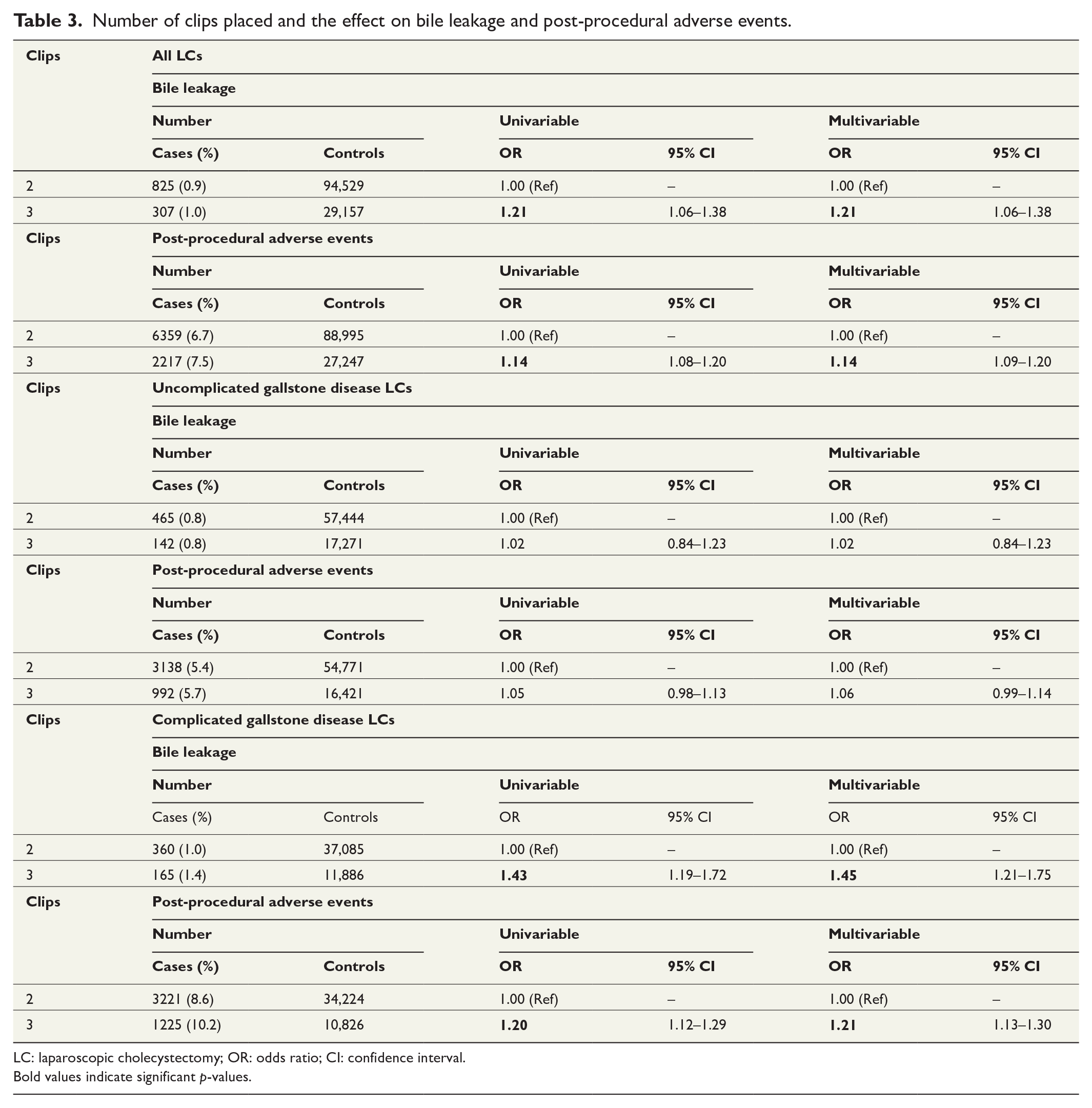
LC: laparoscopic cholecystectomy; OR: odds ratio; CI: confidence interval.
Bold values indicate significant p-values.
In the total cohort of LCs, the overall rate of bile leakage was 0.9% and post-procedural adverse events occurred in 7.4%. Patients who received three clips had a relative increase of 21% in adjusted odds for bile leakage and 18% for post-procedural adverse events in the multivariable analysis. Those results did not appear in the nested cohort of UGD, showing no difference between bile leakage (0.8% vs 0.8%; P = .87) or post-procedural adverse events (three clips, 5.7% vs two clips, 5.4%; P = .16). The nested cohort of CGD had the highest prevalence of bile leakage (1.1%) and post-procedural adverse events (10.0%). For patients with CGD and a cystic duct sealed with three clips compared to two, a significant increase of 45% in odds for bile leakage and 21% for post-procedural adverse events emerged in the adjusted multivariable analysis (Table 3).
Discussion
The study’s chief finding was that for patients undergoing LC for UGD, placing two clips on the cystic duct seemed adequate. Placing a third metal clip for added safety appears redundant. For patients undergoing LC for the indication of CGD, more factors are most certainly involved, and a third clip most likely did not cause the higher OR for bile leakage. When three clips are placed, it possibly indicates a more difficult LC or an LC more prone to bile leakage. This could represent the old surgical saying of “count the clips” which states that the more clips that were used, the more difficult was the cholecystectomy. Patients who received three clips had more comorbidity, which was also associated with a higher risk of leakage. A third clip might act as an indirect risk factor for bile leakage and represent a possible limitation in the statistical adjustment of the GallRiks variables. However, if surgeons consider placing a third clip on the cystic duct to be necessary for patients operated on for CGD, then our data showed a higher probability of bile leakage. That association could indicate that an alternative method of cystic duct closure might be considered in such situations. However, previous systematic reviews have not been able to identify a clear and favorable method of cystic duct closure other than the use of metal clips.9,13,20
To our knowledge, no previous study of the size of this study has sought to compare the number of metal clips placed on the cystic duct with the rate of bile leakage. Studies have rarely revealed the number of metal clips used compared to other methods of cystic duct closure. None of the systematic reviews by van Dijk et al., 9 Ai et al., 13 or Gurusamy et al., 20 indicated the number of metal clips used in control groups for alternative closure techniques. When reviewing each study, we observed that the number of metal clips used is rarely reported or referred only to as “surgical clips.” Despite those trends, the number of metal clips for use as a control group needs to be assessed when conducting comparative studies with other techniques seeking to pinpoint the optimal method of cystic duct closure.
In congruence with two studies by Donkervoort et al.,5,14 our analysis showed similar risk variables for bile leakage, namely, a higher ASA score and acute or previous cholecystitis. As discussed by van Dijk et al., 9 studies have rarely differentiated gallbladder disease surgery as two entities responding to indications of UGD or CGD. This study confirmed the necessity of making that distinction in future studies by revealing discrepancies in outcomes between the two nested cohorts. That requirement is especially true for patients with acute or previous cholecystitis, which represents independent risk factors for bile leakage. At the same time, unlike Donkervoort et al.,5,14 this study showed that being older was an individual risk factor for bile leakage. Our analysis additionally revealed that procedure time and intra-procedural adverse events also were individual risk factors for bile leakage.
In the total cohort, similar but slightly fewer post-procedural adverse events were found for LC, for a rate of 7.4% compared with the rate of 8% reported by Donkervoort et al. 5 Bile leakage has previously been reported with varying incidences: Albasini et al. 4 found an incidence of 2%, Donkervoort et al. 14 an incidence of 1.4%, and Shea et al. 3 an incidence of 0.4%–0.6%, while the overall rate of bile leakage in this study was 0.9%. The bile leakage rate for patients undergoing LC with CGD has been estimated to be as high as 4%–7%. 5 In this study, however, patients with CGD had a bile leakage rate of 1.1%.
Studies on adverse outcomes with low incidence require large cohorts of patients and, to that end, may only be done using register-based data. Examining bile leakage after LC in a randomized controlled trial would require impractical effort and an incredibly high number of patients for this kind of study design. Undeniably, conducting registry studies without any potential for randomization poses a high risk of bias in internal validity with potential confounding factors. Furthermore, causality and clinical significance can easily be overestimated or misinterpreted in large quantities of data. Another limitation of this study is in the inability to use the bile leak from the cystic duct as the true preventable outcome, instead of using bile leakage in general as a surrogate measure. GallRiks also does not have a variable that concerns cystic duct size and thickness, which could play a significant role in decision-making regarding cystic duct closure.
Applying a third clip to the cystic duct in patients undergoing LC for UGD does not correlate with a lower rate of bile leakage and thus cannot be recommended, at least according to this study. However, for patients undergoing LC for CGD, the application of a third clip is associated with a higher bile leakage rate and post-procedural adverse events. Although without causality, that finding probably indicates a more difficult cholecystectomy. For future research comparing other cystic duct closure methods against clips, the number of clips applied should be noted and the distinction of CGD from UGD is warranted.
Footnotes
Author contributions
L.E. had full access to the data and was responsible for the accuracy of data analysis. G.O., A.G., L.E., and B.T. contributed to the study concept and design. G.O., A.G., and L.E. contributed to the acquisition, analysis, or interpretation of data. A.G. and G.O. contributed to the drafting of the manuscript. All authors contributed to the critical revision of the manuscript for important intellectual content. L.E., A.G., and G.O. contributed to the statistical analysis. G.O. and A.G. obtained funding. A.G. and G.O. contributed to the administrative, technical, or material support. G.O., L.E., and B.T. contributed to the study supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Research and Development, Region Kronoberg, Sweden (grant no. 938289).