
Abstract
While most centers around the globe still consider open hepatic resection as the standard, innovative centers step in light of future developments of the robotic platform forward and introduce a robotic liver program while skipping the laparoscopic approach for its technological flaws. This applies also for our Department of Surgery and Transplantation at Rigshospitalet, Copenhagen University Hospital in Denmark. We herewith present as—to our best knowledge—the first center in Scandinavia our experience with the initial 50 robotic liver resections.
Minimally invasive liver surgery is fast evolving worldwide. Despite advances in instrumentation and device development, laparoscopic liver resection is still limited by rigid instruments with stiff maneuverability and visional challenges. Robotic liver surgery (RLS) was first introduced in 2003 by Giulianotti et al. 1 The use of the robotic platform for surgical procedures has steadily been growing around the world, though as a whole, robotics is still in its infancy in the field of hepato-pancreato-biliary (HPB) surgery. The benefits of robotic platforms include technical advantages like relative ease of suturing/knot tying, tremor suppression, facilitated delicate dissection around blood vessels as well as improved three-dimensional (3D) high-definition binocular vision with magnification. In addition, robotic surgery reduces “surgeon’s fatigue syndrome” when compared with the physical demands of advanced laparoscopic procedures. Several studies have reported robotic hepatectomy to be safe and feasible.2 –4 While most centers around the globe still consider open hepatic resection as the standard, innovative centers anticipate on further future development of the robotic platform and introduce a robotic liver program while omitting the laparoscopic approach for its technological flaws. 5 This applies also for our HPB center at Rigshospitalet, Copenhagen University Hospital in Denmark. During the last decade, HPB surgery has been centralized to three centers in Denmark. Our team performs approximately 500 hepato-biliary procedures per year. We herewith present as—to our knowledge—the first center in Scandinavia our experience with robotic liver resections.
Starting in July 2019, 50 consecutively selected patients underwent RLS after individual assessment and discussion regarding their qualification (e.g. ASA, habitus, disease) for a robotic approach at the interdisciplinary multidisciplinary team (MDT). According to the Morioka Guidelines established in 2014, our initial focus was on minor liver resections gradually increasing in complexity over time. 6 Intraoperative ultrasound was used to determine location of lesions and important anatomical structures. Parenchymal transection was obtained applying the robotic Harmonic scalpel® (Ethicon Endo-Surgery, Raritan, NJ, USA). The intermittent Pringle maneuver was applied when more than one segment was resected. Postoperative care followed the ERAS program. Surgeries were performed on the da Vinci® Si Surgical System in a standard setup by a team consisting of three trained HPB surgeons. All surgeons had undergone essential robotic simulation training as well as dry- and wetlab training. All OR assistants had completed the Capital Region training program. Patients’ variables and short-term follow-up were captured and analyzed retrospectively.
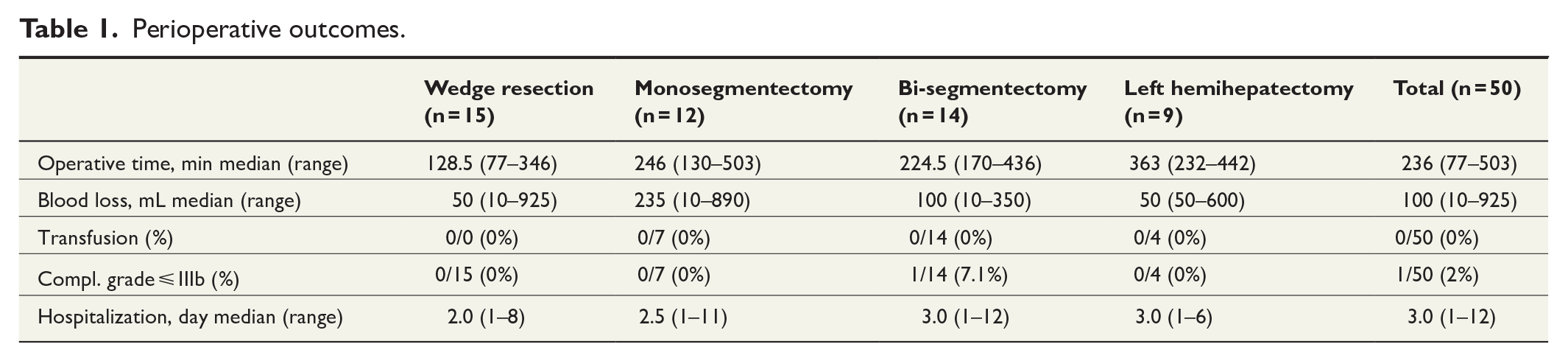
Mean patient age was 63.6 years (25–84 years) and body mass index (BMI) 26.5 kg/m2 (16.7–37.0). Five patients (10%) had a previous surgical history of laparotomy and 19 of laparoscopy (38%). Tumor type consisted of 40 malignant tumors (12 hepatocellular carcinomas (HCCs), six cholangiocellular carcinomas (CCCs), 15 CRCMs, 2 GBCs, and 5 others) and 10 benign liver tumors. Median tumor size was 38.5 mm (5–90 mm). Fifteen patients underwent wedge resections (30%), 12 mono-segmentectomies (24%), 14 bi-segmentectomies (28%), and 9 left hemi-hepatectomies (18%). Median operating time was 236 min (77–503 min) and median estimated blood loss was 100 mL (10–925 mL). One patient required conversion to open surgery because of bleeding. One patient experienced a postoperative Clavien–Dindo complication ⩽3b which involved drainage of abdominal fluid collection. No intra- or postoperative mortality occurred. Median length of hospital stay was 3 days (1–12 days) (Table 1).
Perioperative outcomes.
Our results of the first 50 patients show that implementation of RLS is safe and feasible with favorable short-term outcomes and a very low conversion rate. We acknowledged as proficiency developed, a notable improvement in technical ability to undertake more complex resections. This supported our aim to focus on the direct further implementation of a robotic liver program while omitting the use of laparoscopy for complex liver resections. These outcomes are in line with previously published data from groups from other countries. Feasibility, safety, long and short-term outcomes, as well as costs of RLS should be further investigated in a multi-institutional study among Scandinavian HPB centers.
Footnotes
Author contributions
All authors have:
1. Made a substantial contribution to the concept or design of the work;
2. Drafted the article or revised it critically for important intellectual content;
3. Approved the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.