
Abstract

Neoadjuvant therapy increases esophageal cancer survival. 1 Data on oncological treatments in the Finnish Cancer Registry (FCR) are in research often used to estimate whether patients received neoadjuvant treatment or not. Nordic national registry data are generally valid,2,3 but no studies on using oncological treatment data in the FCR to estimate neoadjuvant treatment exist.
The aim was to evaluate the completeness and concordance of FCR data, compared with neoadjuvant treatment according to patient records.
This population-based nationwide study in Finland included all patients undergoing esophagectomy for cancer during 2010 to 2016. The ethical committee in Northern Ostrobothnia (EETMK 115/2016), and other relevant bodies and agencies approved the study. 4
The FCR maintains an accurate national registry of all cancers in Finland. 5 Oncological treatments in the FCR by modality are reported with specifications: “curative, palliative, or unclear intent” and “under or over 4 months from diagnosis.” Whether each modality is neoadjuvant or adjuvant therapy is not specified. Patients receiving any oncological treatment during 4 months from diagnosis in FCR were classified neoadjuvant treated, as all underwent surgery. Neoadjuvant treatment modalities were classified into (1) chemotherapy, (2) radiotherapy, and (3) chemoradiotherapy.
The Finnish National Esophago-Gastric Cancer Cohort (FINEGO) was the “gold standard” comparison, described in detail elsewhere. 4
The main variable of interest was neoadjuvant therapy (yes/no). Second, modalities were assessed separately. Positive predictive value (PPV), concordance, and completeness were calculated.
Of the 562 patients who underwent esophagectomy, 555 (98.8%) had patient records available. Cancer registry record was found for 488 (86.8%) patients. Of the 562 patients, 241 (42.9%) were excluded due to missing FCR data, resulting in 321 (57.1%) patients with complete data on received neoadjuvant treatment. For neoadjuvant treatment modality, there were 306 (54.4%) patients with complete data. The proportions of received neoadjuvant therapy were similar between included patients and those with missing FCR data.
For those with FCR record, oncological treatment data completeness was 65.8%. PPV and concordance were 90.0% and 80.7% for neoadjuvant treatment. For neoadjuvant treatment modalities, the completeness was 62.7%; PPVs were 87.4% for chemotherapy, 18.8% for radiotherapy, and 85.4% for chemoradiotherapy; and the concordance was 74.8% (Table 1).
Any oncologic treatment following 4 months of diagnosis in comparison to given neoadjuvant therapy and different oncological therapy modalities reported in FCR in comparison to corresponding neoadjuvant therapy modality.
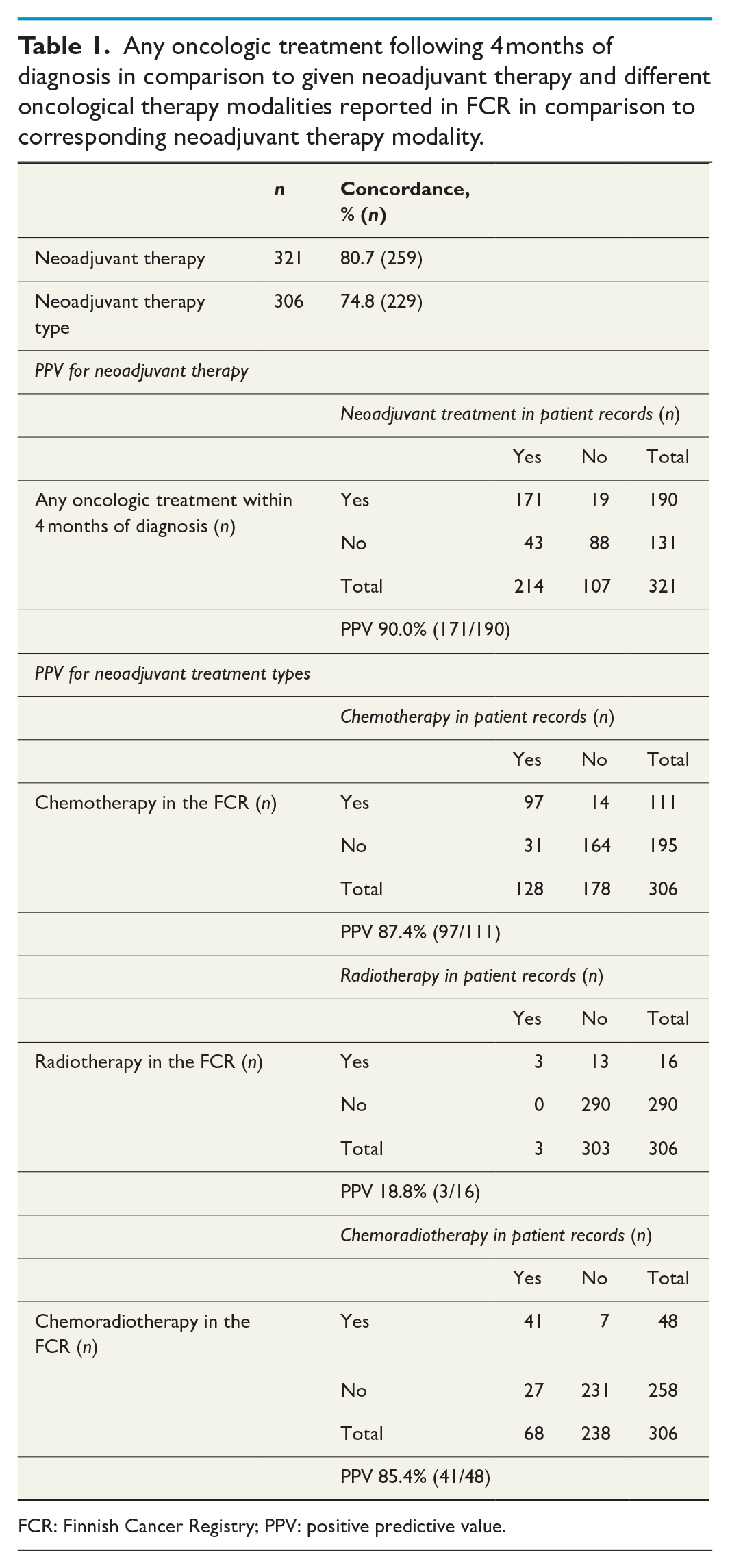
FCR: Finnish Cancer Registry; PPV: positive predictive value.
The completeness of oncologic treatment data in the FCR was lower than expected. This issue is discussed in detail elsewhere. 6 The oncological treatment within 4 months of diagnosis in the FCR was highly concordant with received neoadjuvant therapy in esophagectomy patients. This analogy suggests that it is accurate enough for surgical research. Due to a considerable amount of missing FCR records and records with unclear treatment status, FCR-derived neoadjuvant therapy variable is recommended to be used acknowledging its limitations. Even though FCR data can estimate single modalities fairly well, it is too inaccurate and incomplete for the derivation of specific neoadjuvant treatment types.
The main strengths include the population-based design and the complete and high-quality data of the comparison cohort. Limitations include missing records and missing oncological treatment data in the FCR. However, the proportions of neoadjuvant treatment were similar in those with and without FCR data, suggesting that the data are missing at random.
A relatively large portion of the data reported as “unclear” could be explained by passive reporting of treatments to the FCR, which have decreased over time. 5 The current form of treatment notifications, which can be multiple or retrospective, can lead to contradictory or missing treatment information, leading to missing and unclear labels in the FCR.
In conclusion, FCR oncological treatment data correspond to received neoadjuvant treatment reasonably well, with an unexpectedly high proportion of missing data (missing at random). FCR-derived neoadjuvant treatment data should be used in research acknowledging its limitations.
Footnotes
Acknowledgements
We thank Olli Helminen, Mika Helmiö, Heikki Huhta, Raija Kallio, Vesa Koivukangas, Arto Kokkola, Simo Laine, Elina Lietzen, Sanna Meriläinen, Pasi Ohtonen, Vesa-Matti Pohjanen, Tuomo Rantanen, Ari Ristimäki, Juha Saarnio, Eero Sihvo, Vesa Toikkanen, Tuula Tyrväinen, Mikko Uimonen, and Antti Valtola for their contributions in study design, data acquisition or interpretation, critical revisions, and approval of the final version of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by research grants from the Sigrid Jusélius Foundation (Sigrid Juséliuksen Säätiö), The Finnish Cancer Foundation (Syöpäsäätiö), Päivikki and Sakari Sohlberg Foundation, and Orion Research Foundation (Orionin Tutkimussäätiö).
Ethical statement
The study has been approved by the Ethical Committee in Northern Ostrobothnia (EETMK 115/2016), and governmental agencies and hospital districts involved in the study. The requirement for individual consent was waived by the Finnish Institute for Health and Welfare.