
Abstract
Aim:
To investigate how a nationwide lockdown influences the incidence of appendicitis.
Background:
Communitive infectious diseases may play a role in the pathogenesis of appendicitis as indicated by a seasonal variation in the incidence rate. The spread of communitive infectious diseases has decreased during the COVID-19 pandemic lockdown; thus, we have an opportunity to study the incidence rate of appendicitis in an environment with less impact from common community infections.
Methods:
The study is a nationwide register-based cohort study of the entire Danish population of 5.8 million. The difference in the incidence of appendicitis in a population subjugated to a controlled lockdown with social distancing (study group) was compared to a population not subjugated to a controlled lockdown and social distancing (reference group).
Results:
The relative risk of appendicitis during the lockdown was 0.92 (95% confidence interval (CI): 0.82–1.03, p = 0.131). The relative risk of complicated appendicitis during the lockdown was 0.68 (95% CI: 0.49–0.93, p = 0.02). The incidence of uncomplicated appendicitis was not significantly different during the national lockdown.
Conclusions:
During the national lockdown of Denmark due to the COVID-19 pandemic the incidence of complicated appendicitis was reduced significantly compared to previous years, indicating that infectious disease might be a factor in the pathogenesis of appendicitis with complications.
Trial Registration:
The study was registered on ClinicalTrials.gov (NCT04407117).
Introduction
Appendicitis is one of many diagnoses to consider in patients with acute abdomen, and epidemiological data suggest that the lifetime risk of appendicitis may be as high as 8%. 1 Even though appendicitis is a very common disease, the pathogenesis of appendicitis remains largely unknown. Obstruction of the lumen of the appendix is thought to be one of the causes as the appendix is a blind-ended organ and an obstruction will lead to accumulation of its outlet resulting in inflammation. Obstruction might be caused by a fecalith but lymphoid hyperplasia may also be the source of obstruction, although it has not to our knowledge been proven. Infectious diseases could play a role in some cases of appendicitis.2 –5 Numerous kinds of virus, bacteria, fungi, and parasites can all be involved in the inflammation of the appendix, for example, adenovirus can cause viral infection of the appendix which shows histologically subtle morphological changes including lymphoid hyperplasia. 2 A seasonal variation in the incidence rate of appendicitis has been shown which suggests infectious diseases might participate in the pathogenesis of appendicitis.6–10
With the national COVID-19 pandemic lockdown in Denmark from 15 March to 15 April 2020, the incidence of influenza, adenovirus, RS-virus, and other infectious diseases substantially decreased. 11 Therefore, we have a unique opportunity to study the incidence rate of appendicitis in an environment without the common community infections potentially playing a role in the pathogenesis of appendicitis.
This study aims to examine whether a nationwide lockdown with an entire population subjugated to social distancing reduced the incidence of appendicitis, indicating that infectious disease may play a role in the pathogenesis of appendicitis.
Methods
Study design and setting
This study is a nationwide register-based cohort study. The Danish healthcare system is tax-financed and provides care that is free at the point of service for the entire population of 5.8 million. All acute and emergency abdominal cases are managed in public hospitals.
Participants
The Danish population, that is, all Danish and non-Danish citizens resident in Denmark during the period from 23 March to 19 April, for each year 2017–2020.
Exposure
On 16 March 2020, a nationwide controlled lockdown caused by the COVID-19 pandemic was initiated in Denmark and ended with the first restrictions being withdrawn on 15 April 2020. The lockdown implied that only people with a critical function, for example, doctors or nurses, were allowed to go to work. The remainder of the population were instructed to work from home if possible. All social activities were closed including restaurants, sport events, nonfood shops, universities, and schools. Supermarkets were kept open with restrictions.
The observational period for the study group was from 23 March to 19 April 2020, defined as 1 week after lockdown until 4 days after the first restrictions were withdrawn. To make sure that patients had developed acute appendicitis during the lockdown, the observational period began 1 week after the official lockdown of Denmark.
The observational period for the reference group was during the same period from 23 March to 19 April, for each year: 2017, 2018, and 2019.
Data and data sources
From the Danish National Patient Register, the ICD-10 codes for appendicitis (K35, K36, and K37) and type of surgery performed according to the Nordic NOMESCO Classification of Surgical Procedures 12 were retrieved together with the day of admission and day of surgery. We consider the data in the Danish National Patient Register to be complete with all cases of acute abdominal disorders treated in public hospitals, and the register being the basis for payment to the public hospitals since 2000. 13
Patients with an ICD-10 code for appendicitis (K35, K36, and K37) and a NOMESCO code for resection of the appendix ((KJEA00, KJEA01, KJEA10, KJEW96, KJEW97, KJFB20, KJFB21, KJFB30, KJFB30A, KJFB31, KJFB31A, and any KJFH) during the same admission were extracted from in the Danish National Patient Register. Vital status of patients (dead, alive, emigrated, etc.), date of vital status, gender, and date of birth were collected from the Danish Civil Registration System. Based on the ICD-10 codes, patients were classified as having uncomplicated appendicitis (K35, K35.8, K35.8A, K35.8B, K35.8C, K36, K36.9, K37, and K37.9) and complicated appendicitis (K35.2, K35.3, K35.3A, and K35.3B), that is, appendicitis with peritonitis or abscess. The diagnosis of appendicitis in the Danish National Patient Register has previously been validated to have accepted. 14 The Danish population on 1 January 2017, 2018, 2019, and 2020 were retrieved from Statistics Denmark to calculate the population at risk.
Outcomes
Our primary outcome was the difference in the incidence of appendicitis in a population subjugated to a controlled lockdown with social distancing (study group) compared to a population not subjugated to a controlled lockdown and with social distancing (reference group).
Secondary outcomes were the difference in the incidence of complicated and uncomplicated appendicitis and the 30-day mortality between the two groups.
Statistics
Unpublished data have shown that the yearly relative difference in the incidence of appendicitis is less than 5% and the annual incidence of appendicitis is about 0.095% giving approximately an incidence of 0.007% during a 4-week period. With a power of 80% and a significance level of 0.05%, we needed 5,046,881 people in each 4-week period to show a relative 20% reduction in the incidence of appendicitis from 0.0070% to 0.0056%. The population of Denmark is approximately 5.8 million. To reduce variation, we included the past three periods prior to the lockdown period.
In the study group, the incidence of appendicitis was calculated as the actual number of patients undergoing surgery for appendicitis during the period 23 March to 19 April 2020 divided by the size of the Danish population 1 January 2020. In the reference group, the incidence was calculated as the total number of patients undergoing surgery for appendicitis during the period March 23 to April 19, for each year 2017–2019 divided by the summed size of the Danish population January 1, for each year 2017–2019. Fisher’s exact test was used for categorical data and the Kruskal–Wallis test for continuous data. Poisson regression was used to compare the incidences of appendicitis. Point estimates (rate ratios) and corresponding 95% confidence intervals (CIs) are presented. Point estimates of uncomplicated and complicated appendicitis are exploratory and the significance thresholds were not adjusted.
All available data were used. No imputations were performed. A two-tailed p value ⩽ 0.05 was considered significant. All analyses were performed using R statistical software, version 3.6.1. 15
The study was registered on ClinicalTrials.gov (NCT04407117) and is reported according to the STROBE statement.
Ethical considerations
Retrospective register studies do not require ethical approval by Danish legislation. The study was approved by the Danish Data Protection Agency (RegionH: P-2019-191).
Results
A total of 407 patients underwent surgery for appendicitis during the national COVID-19 lockdown in 2020. During the same period in the years 2017, 2018, and 2019, a total of 1320 patients underwent surgery for appendicitis. Sex, age, and 30-day mortality did not differ significantly between the two periods (Table 1).
Demographics of patients with a diagnosis of appendicitis during the lockdown period in Denmark from 23 March to 19 April 2020 and of the patients with a diagnosis of appendicitis over the same period in 2017–2019.
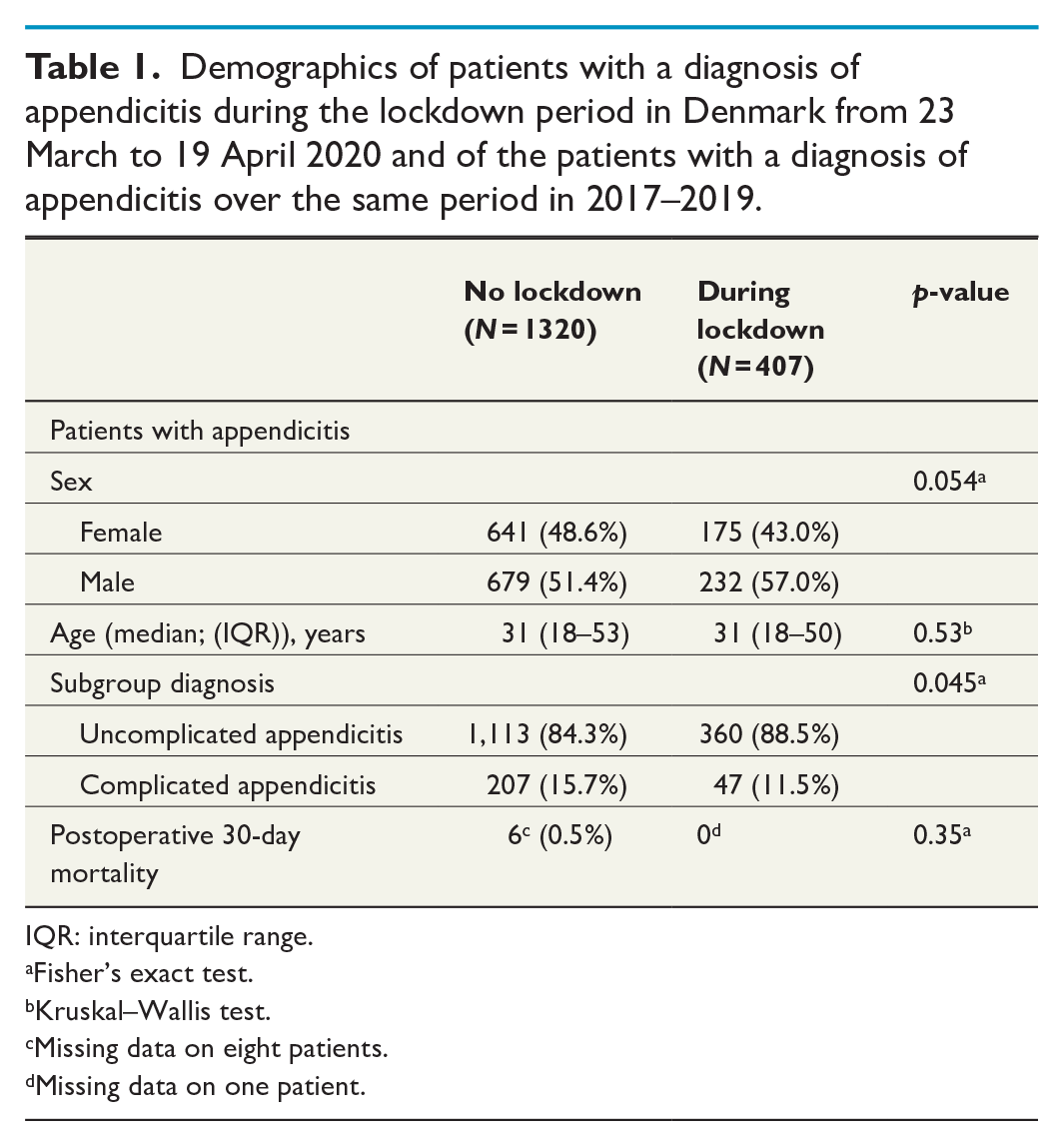
IQR: interquartile range.
Fisher’s exact test.
Kruskal–Wallis test.
Missing data on eight patients.
Missing data on one patient.
The incidences of appendicitis are presented in Table 2.
Crude incidence rate of appendicitis per 100,000 during the 4-week periods. All cases, and stratified by uncomplicated and complicated appendicitis.
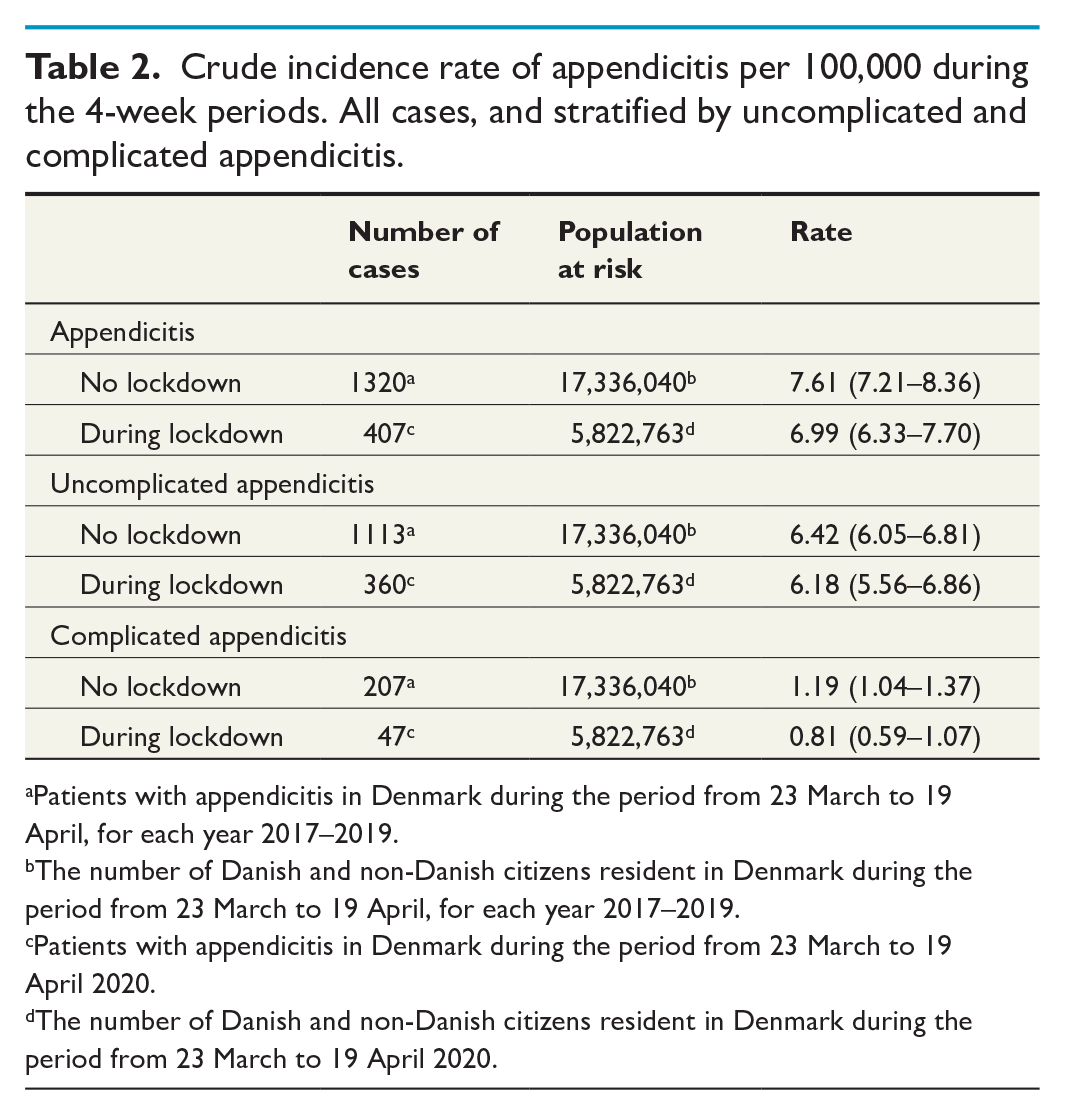
Patients with appendicitis in Denmark during the period from 23 March to 19 April, for each year 2017–2019.
The number of Danish and non-Danish citizens resident in Denmark during the period from 23 March to 19 April, for each year 2017–2019.
Patients with appendicitis in Denmark during the period from 23 March to 19 April 2020.
The number of Danish and non-Danish citizens resident in Denmark during the period from 23 March to 19 April 2020.
There was no significant difference in the crude incidence rate of appendicitis between the two groups and the relative risk during the lockdown period was 0.92 (95% CI: 0.82;1.03, p = 0.13) when compared to the reference group. When adjusting for sex and age, the difference was still not significant (Fig. 1).
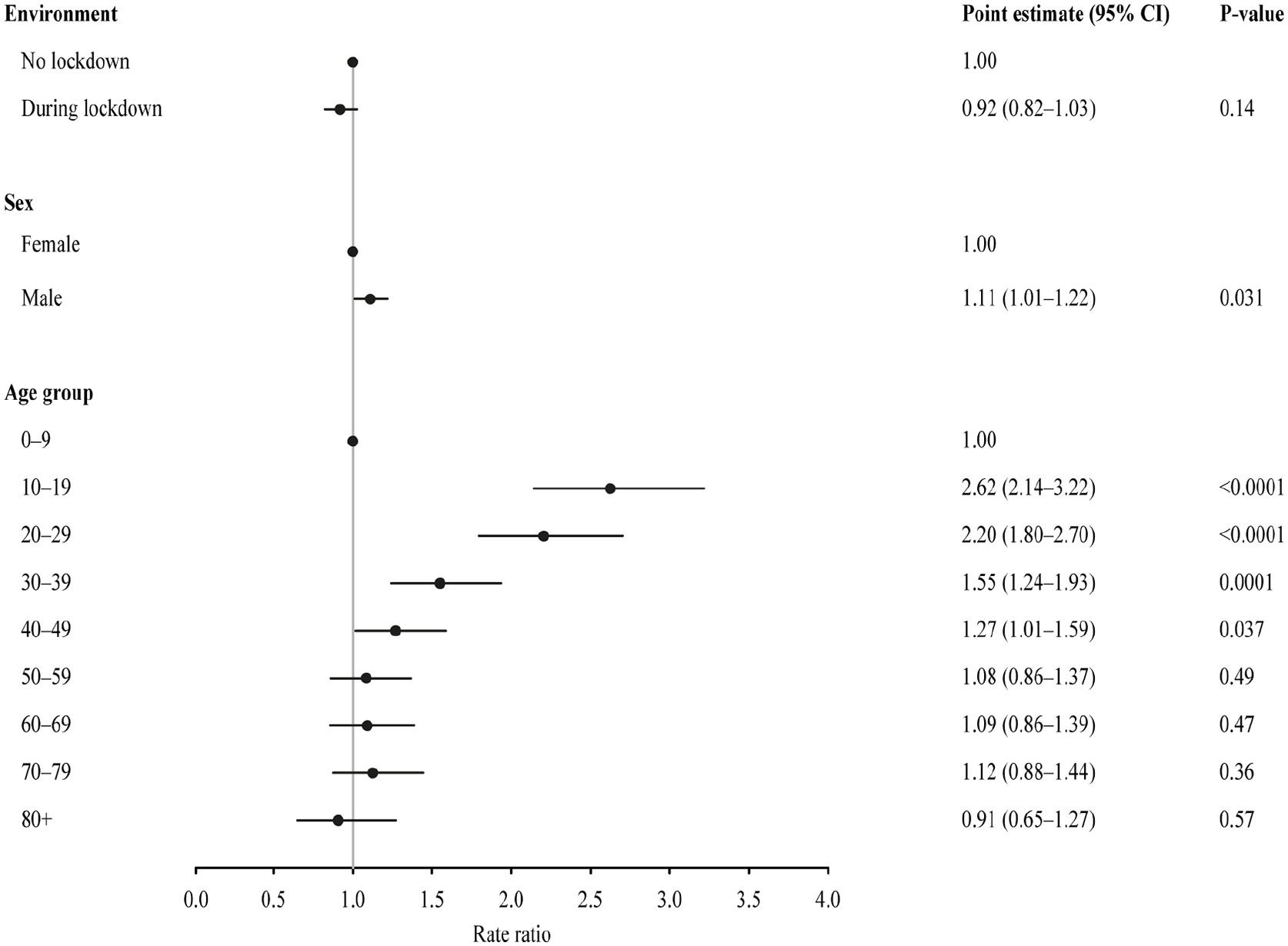
Incidence rates of overall appendicitis.
There was a significant difference in the distribution of uncomplicated and complicated appendicitis between the two periods with a decrease in the proportion of patients with complicated appendicitis during the lockdown period (Table 1). There was no difference in the relative risk of uncomplicated appendicitis during lockdown versus no lockdown when adjusting for sex and age (Fig. 2). When adjusting for sex and age, the incidence of complicated appendicitis during the lockdown period was reduced with a relative risk of 0.68 (95% CI: 0.49; 0.93, p = 0.015) compared to the period without lockdown (Fig. 3).
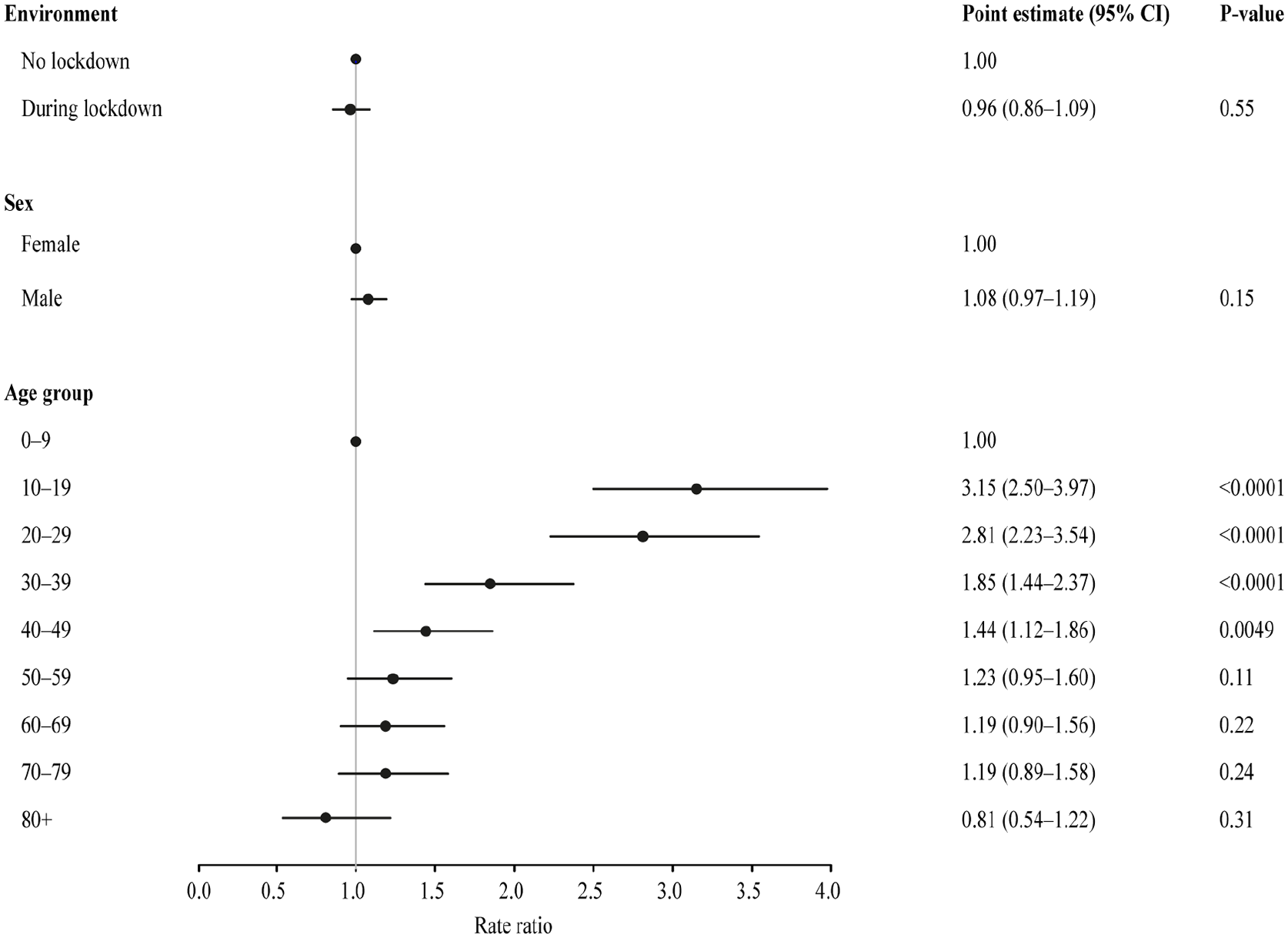
Incidence rates of uncomplicated appendicitis.
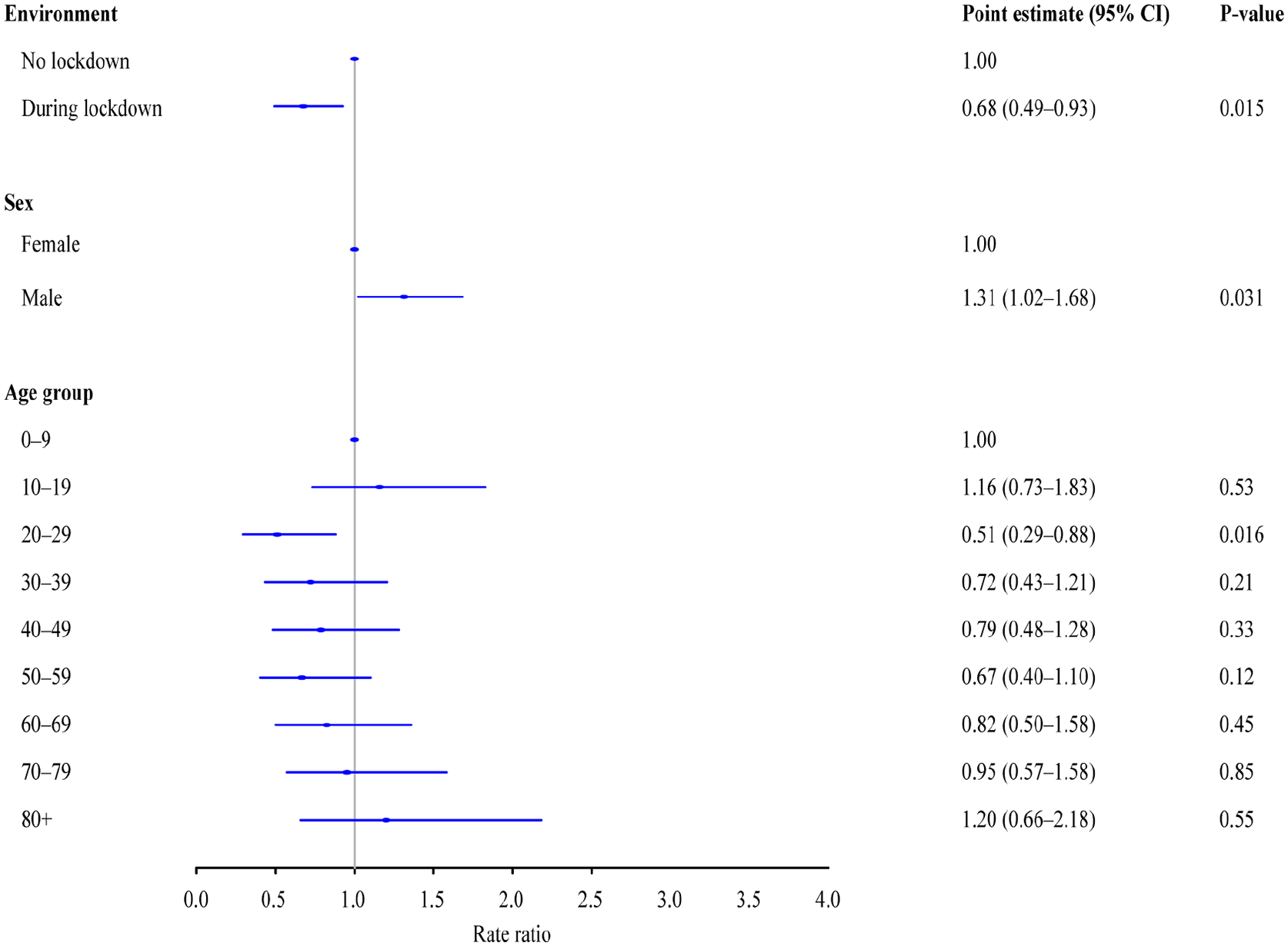
Incidence rates of complicated appendicitis.
Discussion
During the national lockdown, there was no significant change in the incidence of appendicitis, but a significantly lower incidence of complicated appendicitis was observed. The relative risk of complicated appendicitis was 32% lower during the national lockdown compared to the three previous years.
Misclassification related to the ICD-10 and NOMESCO codes is a potential limitation, but registration of these codes in the Danish National Patient Register has previously been validated by our group. 14 We had access to Danish National Patient Register data on the entire Danish population and thus data on all cases of appendicitis during the specified study periods. The Danish National Patient Register is considered the finest of its kind internationally and includes information on all patients admitted to Danish hospitals. 13 There is no risk of bias from patients admitted to private hospitals, as these would be transferred to a public hospital for surgery. In Denmark, private hospitals only perform elective surgery like hernia repair or elective laparoscopic cholecystectomy. They never perform acute surgery as they do not have the setup or care unit for acute patients. In other countries, a private practitioner may treat patients with acute appendicitis conservatively with antibiotics but that is not standard practice in Denmark. Any patient with suspected appendicitis will be admitted acutely to a public hospital for further examination and surgery because this is the gold standard in Denmark.
Another potential limitation would be internal and external migration. Our study is nationwide thus internal migration is not a bias. The national lockdown was initiated overnight with external borders being closed and it is possible but not likely that the patients migrated to another country during the lockdown. In addition, all elective surgery was canceled overnight, only operations on acute patients and cancer patients were permitted.
The risk of bias from yearly variations in the incidence of appendicitis was reduced by including the same period for the previous 3 years. During the data management process, we received data from 2019 to 2020 some weeks before 2017 and 2018. We did a preliminary analysis comparing 2019 and 2020, which showed a significant decrease during the lockdown (data not shown). Our study design contains a potential bias as there might have been an increasing trend in the incidence of appendicitis if the COVID-19 pandemic has not occurred.
Inconsistency under the weather conditions during the study periods might also have an impact on the incidence of communitive infectious disease and thus the seasonal variation in the incidence of appendicitis. The national lockdown period created an environment without the common community infections that potentially play a role in the pathogenesis of appendicitis. Therefore, we had a unique opportunity to study the incidence rate of appendicitis under these circumstances.
In regards to lifetime risk, one could argue that some individuals in the reference group previously had undergone an appendectomy. The overall prevalence should still be consistent from year to year as the Danish population size stays roughly the same and because people are born and die throughout the study period. By including a nationwide population, the generalizability of our results is high.
As this is an epidemiological register-based study, we cannot comment on the inference about causality, but our results indicate that uncomplicated and complicated appendicitis might have different pathogenesis. This had previously been suggested in epidemiological studies.16 –18 To our knowledge, no studies have confirmed this hypothesis. Theoretically, if the etiologies were similar, we would expect either a significant decrease in both incidence rates during a lockdown or no change at all. Furthermore, this study suggests that there is an association between the pathogenesis of complicated appendicitis and communitive infectious diseases with a lower incidence during the national lockdown.
Several reports19 –21 have shown a decreased daily caseload of emergency cases including appendicitis during the COVID-19 pandemic. Fischer et al. found an increased incidence of complicated appendicitis and longer duration of symptoms in children in the New York City Metropolitan Region during the COVID-19 pandemic from March to May 2020. 22 They suggest that these outcomes were the result of the disruption of the healthcare systems caused by COVID-19. Another explanation could be a patient delay because of the fear of being infected with COVID-19 during hospital admission.23,24 Approximately one-third of all cases of COVID-19 in the United States occurred in New York City and northern New Jersey during the spring of 2020, which makes a patient’s delay even more plausible. 22 In accordance, others24 –26 have shown an increased incidence of complicated appendicitis and indications of a longer duration of symptoms before seeing a physician, thus leading to a higher incidence of complicated appendicitis.
The capacity in Denmark for acute surgery during the lockdown period may have been increased as a result of the cancelation of elective surgery. Hence patients suspected of appendicitis may have undergone surgery earlier than usual. In 2017, a large American study showed that delayed appendectomy within 24 h of presentation is not associated with an increased risk of developing complicated appendicitis. 27 A previous Danish study showed that the normal median therapeutic delay from admission to surgery is 5–7 h for patients with appendicitis. 28 Based on this, it does not seem plausible that the lower incidence of complicated appendicitis in our study was caused by a decreased therapeutic delay from admission to surgery for patients with appendicitis.
In contrast, a German population study 29 without adjustment for seasonal variations and two retrospective studies18,30 reported a decrease in the incidence of uncomplicated appendicitis and no change in the incidence of complicated appendicitis.
The public Danish healthcare system is free at the point of service and sustained the regular capacity for acute and emergency abdominal surgery during the lockdown. If our results are associated with this, the increased incidence of complicated appendicitis reported by others during the COVID-19 pandemic seems associated with patient delay and reduced capacity of healthcare services. This highlights the importance of timely measures to ensure sufficient capacity of local and national healthcare services to avoid the collateral damage of a pandemic that overburdens healthcare services.
It is also important to note that in Denmark, it is not standard practice to remove a noninflamed appendix as it is in many other European countries. In Denmark, the appendix is not routinely removed at laparoscopy if the appendix has no signs of inflammation. It was therefore not possible to report the negative appendectomy rate.
This study aimed to examine whether a nationwide lockdown with an entire population subjugated to social distancing reduced the incidence of appendicitis. We did not observe a decreased incidence of appendicitis, but significantly fewer patients with complicated appendicitis, this may be an indication that infectious disease may play a role in the pathogenesis of complicated appendicitis.
Footnotes
Author contributions
A.T.J. contributed to study design, writing original draft, review and editing the drafts, and approving the final draft. A.B.-N. contributed to study concepts, study design, data interpretation, review and editing the drafts, and approving the final draft. C.T.-P. contributed to study design, providing data from national databases, review and editing the drafts, and approving the final draft. C.A.B. contributed to study concepts, study design, data interpretation, review and editing the drafts, and approving the final draft. J.K. contributed to study concepts, study design, data management, statistical analysis, review and editing the draft, and approving the final draft.
Data sharing plan
Data will not be available from the authors. Data are available from Statistics Denmark (dst.dk).
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.A.B. has received a speaker honorarium from Olympus Finland and Intuitive Surgery. C.T.-P. has received grants from Novo Nordisk and Bayer. The other authors have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.