
Abstract
Background and objective:
High-risk surgery on aged patients raises challenging ethical and clinical issues. The aim of this study was to analyze the preoperative factors associated with severe complications and returning home after pancreatic resection among patients aged ⩾ 75 years.
Patients and methods:
Patients aged ⩾ 75 years undergoing pancreatic resection in 2012–2019 were retrospectively searched from the hospital database. Preoperative indices (Clinical Frailty Scale, Skeletal Muscle Index, Geriatric Nutritional Risk Index, Charlson Comorbidity Index, and National Surgical Quality Improvement Program risk for severe complications) were determined. Postoperative outcome was evaluated by incidence of Clavien–Dindo 3b-5 complications, rate of returning home, and 1-year survival.
Results:
A total of 95 patients were included. American Society of Anesthesiologists Class 3–4 covered 50%, Clinical Frailty Scale > 3 22%, Charlson Comorbidity Index > 6 53%, and a sarcopenic Skeletal Muscle Index 51% of these patients. The National Surgical Quality Improvement Program risk for severe complications was higher than average among 21% of patients. Geriatric Nutritional Risk Index showed high risk among 3% of them. In total, 19 patients (20%) experienced a severe (Clavien–Dindo 3b-5) complication. However, 30- and 90-day mortality was 2.1%. Preoperative indices were not associated with severe complications. Most patients (79%) had returned home within 8 weeks of surgery. Not returning home was associated with severe complications (p = 0.010).
Conclusions:
The short-term outcome after pancreatic resection of fit older patients is similar to that of younger, unselected patient groups. In these selected patients, the commonly used preoperative indexes were not associated with severe complications or returning home.
Keywords
Introduction
The ethical aspects of possible over- and undertreatment of the frail aged challenge the Western countries with their increasingly aging populations and limited resources. Selecting the most reasonable treatment for the aged is especially difficult among patients with suspected pancreatic cancer and potentially poor prognoses or with suspected premalignant pancreatic lesions with a potentially uncompromised life expectancy. Pancreatic resections are high-risk surgery, and in earlier studies,1 –4 preoperative frailty, age, chronic kidney disease, high American Society of Anesthesiologists (ASA) class, and sarcopenia have been associated with postoperative morbidity. However, it has been reported that neither short-term5,6 nor long-term prognoses among the aged necessarily differ from those of unselected, younger patient cohorts. 7 Even underuse of pancreatic surgery among the aged has been suspected.8,9 A multidisciplinary (MD) approach and scoring systems for physical fitness and frailty in borderline patients are necessary to evaluate such patients’ performance status, eligibility for high-risk surgery, and ability to recover postoperatively. For a patient, returning home to independent living and quality life years may be even more important endpoints. Nevertheless, among the aged, the preoperative predictors of severe complications and successfully returning home after pancreatic surgery remain unclear. 10 The aim of this study was to evaluate the factors associated with severe complications, returning home, and 1-year survival among patients aged ⩾ 75 years after pancreatic resection.
Methods
All patients who had undergone elective pancreatic resection in Tampere University Hospital, Finland between 2012 and 2019 were identified from the hospital database. The catchment area of Tampere University Hospital covers ca. 1,000,000 patients and is nationally a tertiary, high-volume pancreatic center. Patients aged ⩾ 75 years on the operation date were included.
Indication for surgery had been discussed in the MD meeting, including oncologists, pancreatic surgeons, radiologists, gastroenterologists, and pathologists. After the MD meeting, a pancreatic surgeon met the patient at the outpatient clinic to evaluate the physical performance status, eligibility, and willingness to undergo surgery. If the patient had major comorbidities or a borderline physical performance status, other specialists, such as anesthesiologists or cardiologists, were consulted.
Preoperative data on patient demographics, physical performance status, preoperative laboratory tests (hemoglobin albumin, creatinine, and glomerular filtration rate (GFR)), and indication for pancreatic resection were retrospectively gathered from the electronic patient records. The data on physical performance status were retrieved from the preoperative questionnaire the patients routinely complete with a nurse. Performance status was categorized as “good” if no dyspnoea or chest pain was reported during exercise and the patient was able to climb at least one flight of stairs.
The preoperative indices, including Charlson comorbidity index (ChCoI), 11 Clinical Frailty Scale (CFS), 12 and the Geriatric Nutrition Index (GNIR), 13 were calculated retrospectively for the study purposes. In addition, preoperative sarcopenia was retrospectively evaluated by determining the Skeletal Muscle Index (SMI) from the preoperative CT scans according to El Amrani et al. 1 Patients were considered sarcopenic if the SMI was < 38.5 cm2/m2 for females and < 52.4 cm2/m2 for males. The preoperative risk for severe complications was evaluated according to the National Surgical Quality Improvement Program calculator (NSQIP risk calculator).
Indication for surgery was categorized based on the preoperative imaging as follows: suspicion of malignancy (visible tumor or double duct sign), mixed-type or main-duct intraductal neoplasm (MX-IPMN or MD-IPMN), or as a worrisome cyst according to the European guidelines. 14
Perioperative data on the pathology report, complications, hospital stay, and oncological therapy were recorded retrospectively from the hospital databases. Hospital stay was defined as the total time a patient spent in any health care unit postoperatively.
Mortality was presented as both 30- and 90-day rates. Complications were categorized according to the Clavien–Dindo (C-D) classification, 15 and comprehensive complication index (CoCoI) 16 was calculated. Pancreatic fistula (POPF) and postpancreatectomy hemorrhage (PPH) were evaluated according to international guidelines.17,18 Grades B and C were considered as clinically relevant complications.
Returning home was reported in 60 days postoperatively. This was determined from either surgical or oncological patient files. In cases of doubt, the patient was excluded from this part of the analysis.
The primary short-term outcomes were incidence of severe postoperative complications (C-D 3b-5) and high CoCoI level (over 75% quartile). Secondary short-term outcome was returning home within 2 months after surgery, considered as normal recovery after major surgery. Both positive predictive (PPV) and negative predictive values (NPV) of the preoperative indices were calculated for both outcomes. Eligibility for adjuvant therapy was reported among pancreatic ductal adenocarcinoma (PDAC) patients. In addition, 30- and 90-day mortality and 1-year survival rate were calculated. To analyze histology-based survival, 1-year survival rates were calculated for patients who survived at least 30 days postoperatively.
Statistical analyses were performed with SPSS 26 software. Fisher’s exact test, chi-squared test, logistic regression, and Kruskal–Wallis tests were used for univariate analyses. A p-value below 0.05 was considered statistically significant.
The study was approved by the Regional Ethics Committee of Pirkanmaa (code R12241).
Results
Number of patients, demographics, and indications for surgery
The search yielded a total of 95 patients aged ⩾ 75 years (ca. 21% of all elective pancreatic resections during the observation period). The median age was 78 years (range 75–85 years), and 50% of the patients were male. The indication for surgery was suspected cancer in 70 (74%) patients, suspected main-duct or mixed-type intraductal papillary neoplasm in 16 (17%) and suspected worrisome cystic lesion in nine patients (9.5%) (Appendix 1).
Preoperative background data
ASA Class 3–4 was found among 50% and ChCoI was > 6 in 19% of the patients (median 6, range 3–8). Most patients were physically fit (CFS 1–3 in 78%, CFS 4 in 16%, and CFS 5–6 in 2%) and, of the 80 patients whose preoperative questionnaires were available, 84% had good performance status (Table 1). Two patients were diagnosed with early-stage Alzheimer’s disease. Five patients had a history of a transient ischemic attack or stroke. Preoperatively one patient lived in residential care facility due to Parkinson’s disease and the rest at home.
Perioperative data and their associations with severe complications and the highest quartile CoCoI score.
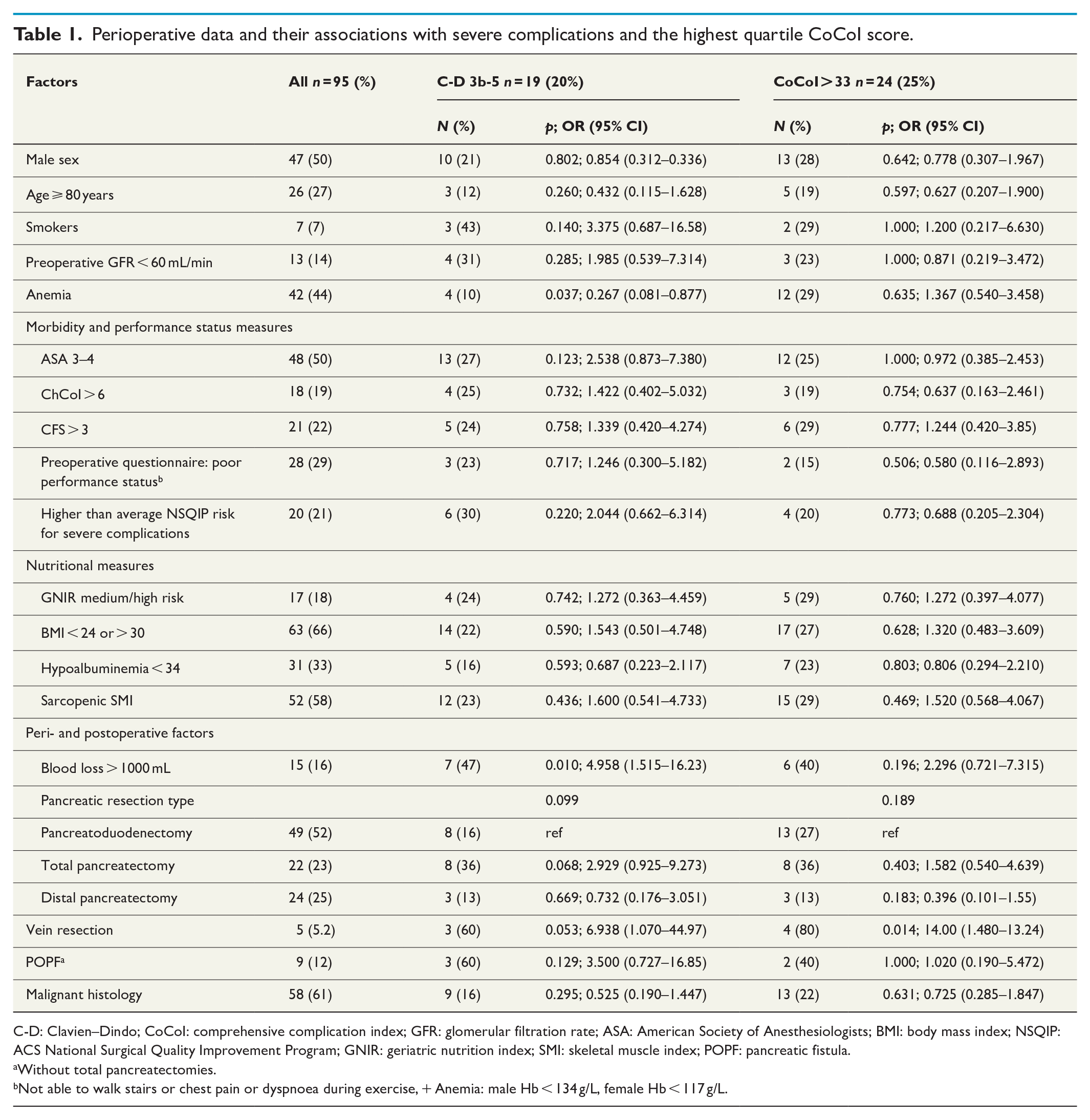
C-D: Clavien–Dindo; CoCoI: comprehensive complication index; GFR: glomerular filtration rate; ASA: American Society of Anesthesiologists; BMI: body mass index; NSQIP: ACS National Surgical Quality Improvement Program; GNIR: geriatric nutrition index; SMI: skeletal muscle index; POPF: pancreatic fistula.
Without total pancreatectomies.
Not able to walk stairs or chest pain or dyspnoea during exercise, + Anemia: male Hb < 134 g/L, female Hb < 117 g/L.
Preoperative laboratory tests showed mild renal insufficiency in 86%, normal hemoglobin in 56%, and normal albumin values in 64% of the patients. Optimal BMI level 19 for the aged (25–30 years) was found in 34% of cases. The geriatric nutritional index (GNIR) showed that the majority (79%) of the patients were low or no-risk patients. One-fifth (21%) of the patients had a high risk for severe complications according to NSQIP (Table 1).
Surgery details
A total of 49 (51%) of the patients had the pancreatoduodenectomy, 22 (23%) total pancreatectomy, and 24 (25%) distal resection. Five portal/superior mesenteric vein resections with end-to-end reconstruction were performed among the study population. Median intraoperative blood loss was 550 mL (range 20–3710 mL). Intraoperative bleeding > 1000 mL in 15 patients (16%).
Postoperative complications
The 30- and 90-day mortality rate was 2.1% (two patients). A severe complication (C-D 3b-5) occurred in 20% of the patients. The median CoCoI was 21 and its 75% quartile was 33. Infectious complications, such as pneumonia, abscesses, wound infections, diarrhea, or septicemia occurred in 40% of the patients. In total, 12 patients underwent reoperation (1 for colon perforation, 1 for stomach perforation, 3 for hepaticojejunostomy leakage, 1 for severe POPF, 1 for suspected bowel ischemia, 1 for portal vein thrombosis, and 4 for escalated infectious and POPF complication). Complications led to the removal of the remnant pancreas (the tail) during the hospital stay among three patients who had primarily undergone pancreatoduodenectomy. Six patients developed organ failure requiring treatment in the intensive care unit (ICU). The length of ICU stay ranged from 2 to 9 days. The overall median hospital stay was 11 days (range 3–59) (Table 2).
Postoperative complications.
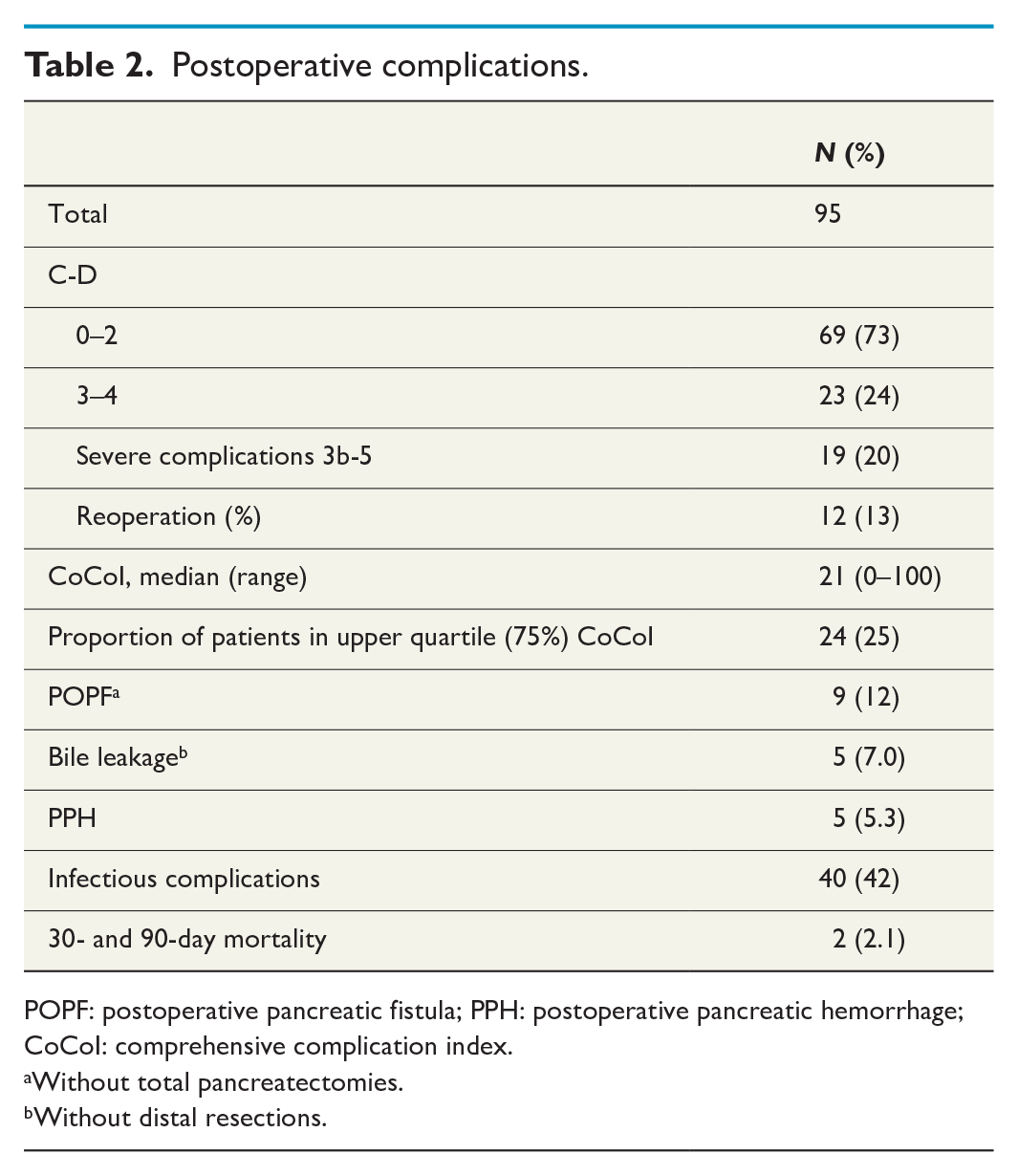
POPF: postoperative pancreatic fistula; PPH: postoperative pancreatic hemorrhage; CoCoI: comprehensive complication index.
Without total pancreatectomies.
Without distal resections.
The univariate analysis showed that preoperative normal hemoglobin (p = 0.037) and intraoperative bleeding over 1000 mL (p = 0.010) were associated with severe complications. Vein resection was associated with highest quartile CoCoI level and seemed to be a risk factor for C-D 3b-5 complications (p = 0.053). The preoperative indices ASA, GNIR, ChCoI, CFS, preoperative questionnaire on physical performance status, SMI, or NSQIP risk score for severe complications were not associated with severe complications in this population (Table 2). The PPVs of the preoperative indices varied between 23% and 30% and the NPVs between 81% and 87% for a severe complication (Table 3).
PPV and NPV for severe complications (C-D 3b-5) and for returning home.
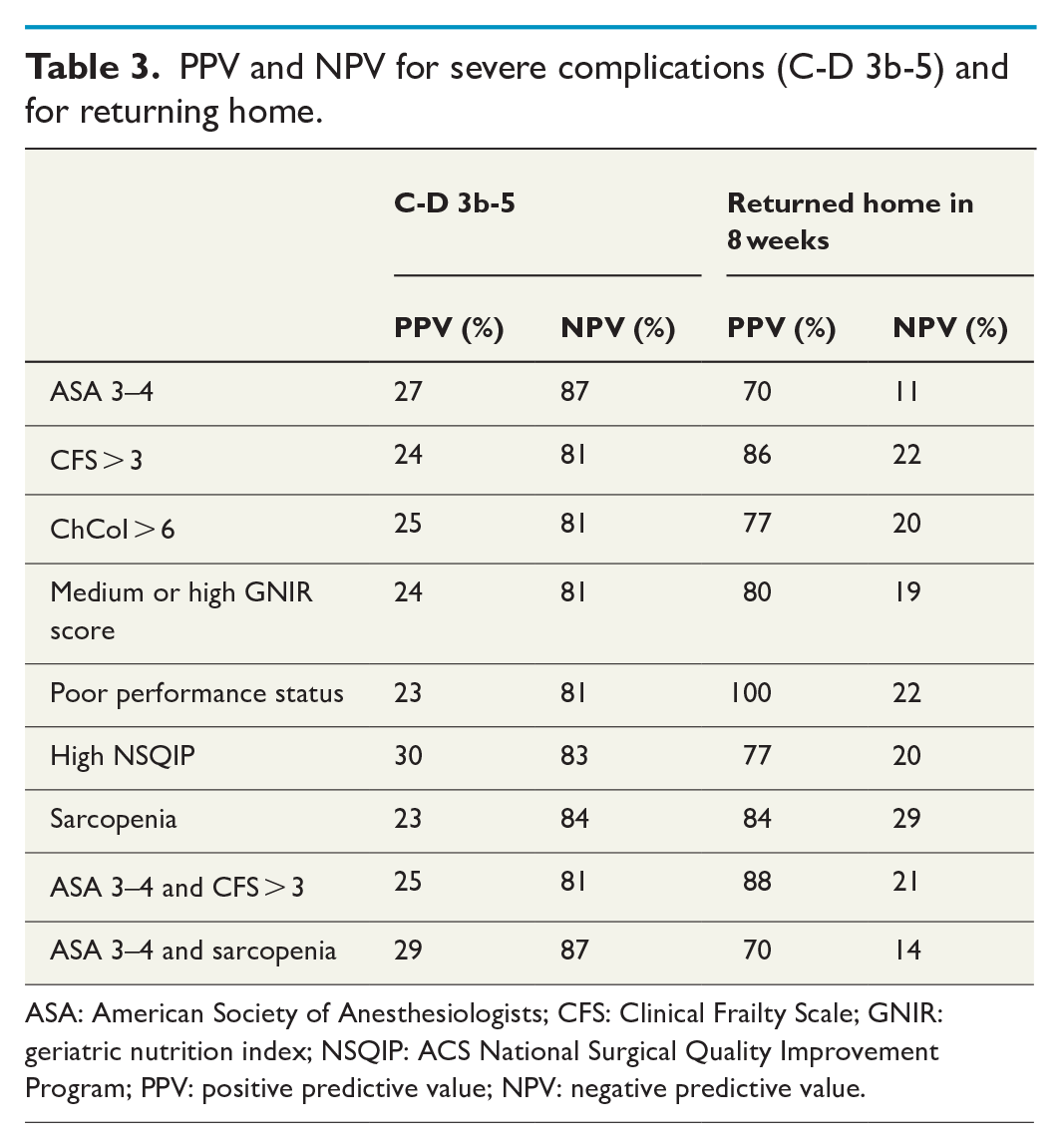
ASA: American Society of Anesthesiologists; CFS: Clinical Frailty Scale; GNIR: geriatric nutrition index; NSQIP: ACS National Surgical Quality Improvement Program; PPV: positive predictive value; NPV: negative predictive value.
Returning home in 60 days
Follow-up data on the location of the patients at 2 months (60 days) postoperatively was available for 78 patients (83%). Out of these, 62 (80%) patients had returned home within 60 days. The returning home was not associated with the resection type (distal pancreatectomy (87%) versus pancreatoduodenectomy or total pancreatectomy (76%), (p = 0.368)).
Not returning home postoperatively was associated with the occurrence of severe complications (C-D 3b-5). In addition, infectious complications and development of POPF B/C were associated with not returning home within 60 days. The preoperative indices ASA, GNIR, ChCoI, CFS, preoperative questionnaire on physical performance status, SMI, or NSQIP were not associated with returning home in this population (Table 4). In the analysis of the preoperative indices, the PPVs varied 70%–100% and the NPVs 14%–29% for returning home.
Factors associated with returning home within 60 days.
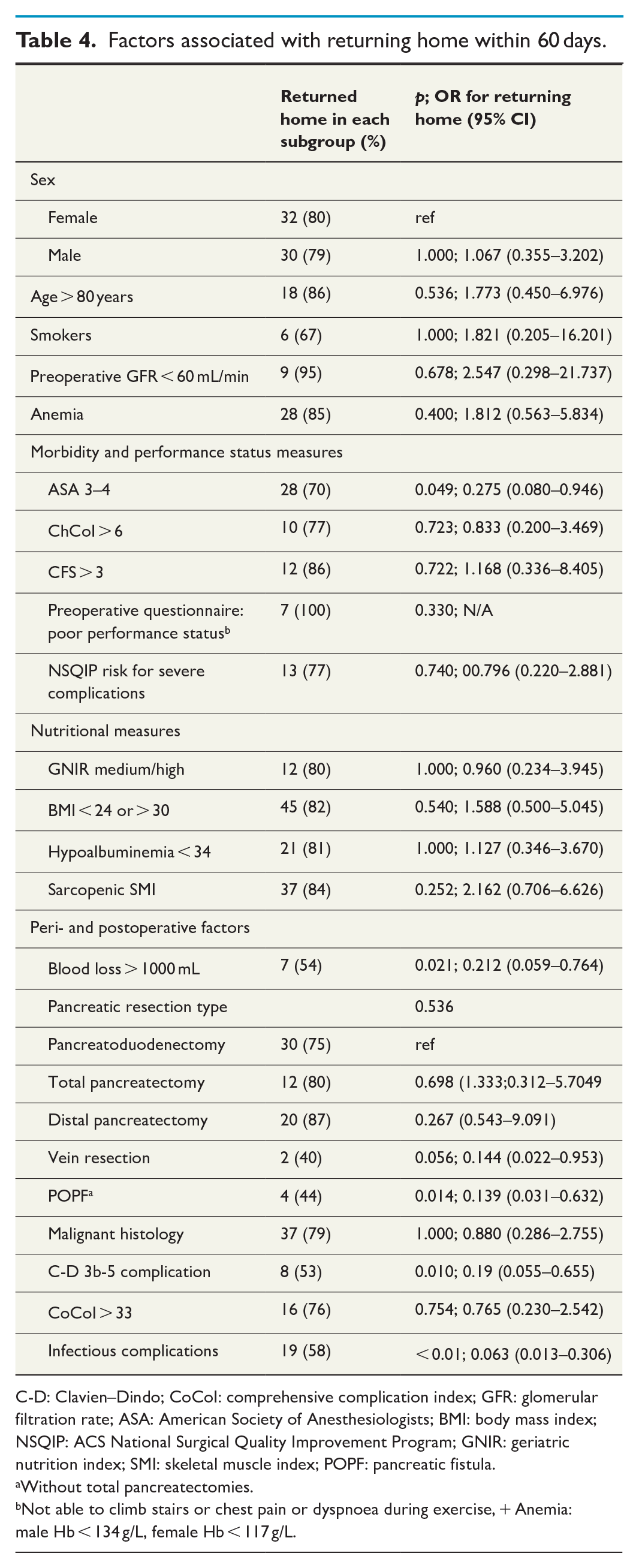
C-D: Clavien–Dindo; CoCoI: comprehensive complication index; GFR: glomerular filtration rate; ASA: American Society of Anesthesiologists; BMI: body mass index; NSQIP: ACS National Surgical Quality Improvement Program; GNIR: geriatric nutrition index; SMI: skeletal muscle index; POPF: pancreatic fistula.
Without total pancreatectomies.
Not able to climb stairs or chest pain or dyspnoea during exercise, + Anemia: male Hb < 134 g/L, female Hb < 117 g/L.
Final pathology and eligibility for adjuvant therapy
Overall, 58 (61%) patients had a malignant final pathology. PDAC accounted for 55% of these (32 patients). MD- or MX-IPMN were found in 21% of the patients (Appendix 1).
Data on adjuvant therapy were available for 29 PDAC patients (90%). However, 19 patients with PDAC were enrolled for adjuvant therapy (66%). Eligibility and willingness for adjuvant therapy were evaluated by an oncologist.
Survival
The overall 1-year survival rate among patients with benign or premalignant final diagnoses (38 patients) was 92% and among patients with a malignant disease 75% (p = 0.019). Among patients with a benign disease, physical performance status was associated with survival over 1 year (p = 0.028, OR: 7.750; 95% CI: 3.105–19.342), but the analysis of other factors lacked statistical power. Among patients with a malignant disease, none of the preoperative metrics was associated with 1-year survival (ChCoI: p = 0.060, performance status: p = 0.617, CFS: p = 0.181, ASA: p = 0.128, and SMI: p = 0.510) Figure 1.
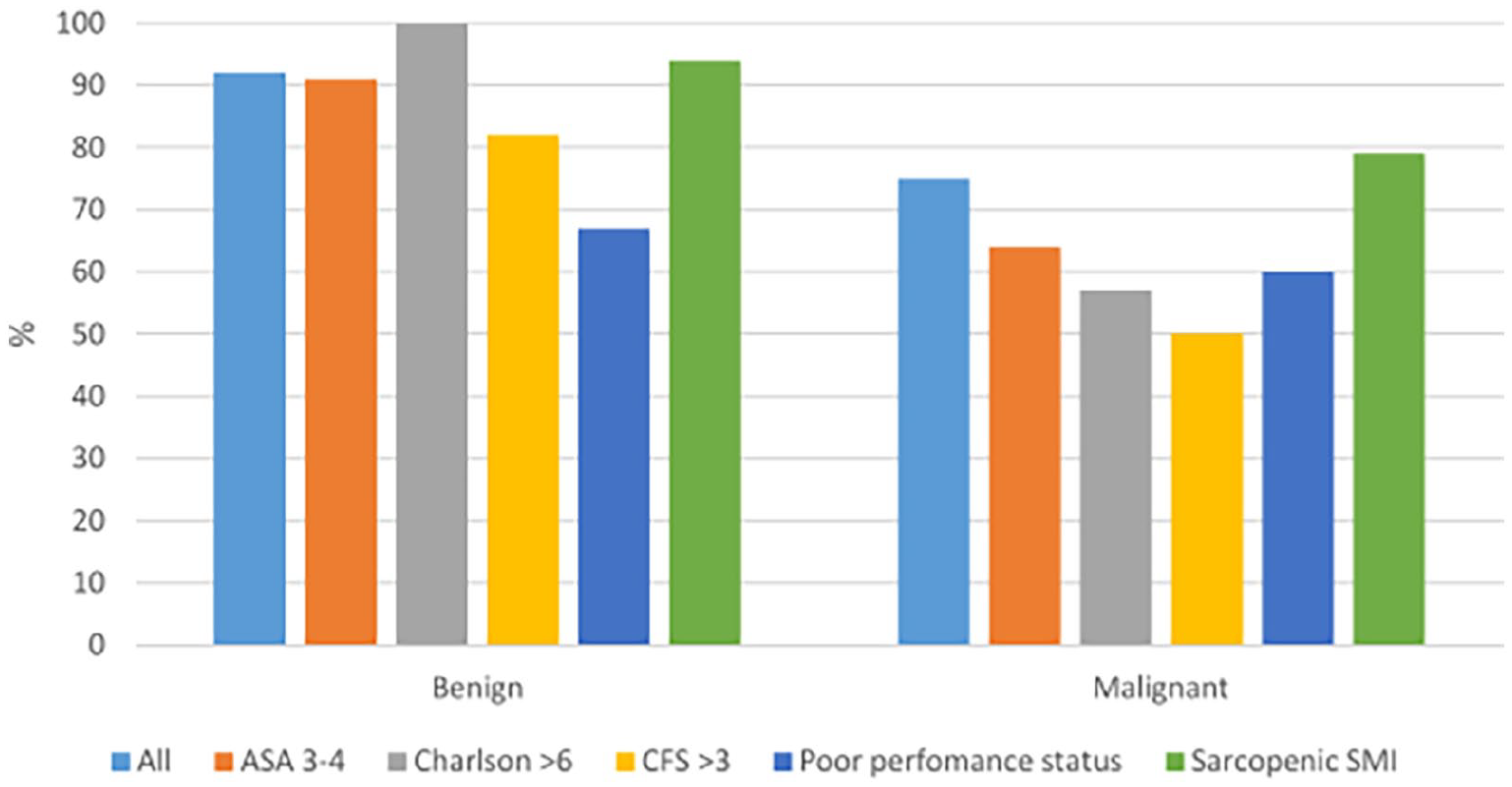
One-year survival rates and preoperative metrics for benign and malignant disease.
Discussion
Pancreatic surgery is recommended either for suspected cancer or high-risk premalignant lesions. Due to the potential postoperative morbidity and mortality associated with pancreatic surgery, careful preoperative evaluation of the patients is crucial. Ideally, surgery should be offered to patients who are fit enough to tolerate complications, with a realistically capable of returning home postoperatively and whose quality life years can be extended by pancreatic surgery. This study shows that outcome after pancreatic resection among the fit aged is similar to earlier reports for all age groups.5 –7 In this selected group, the preoperative scores failed to predict severe complications or returning home within 2 months. Good physical performance status, however, seems to be associated with better survival, especially among patients with benign final pathology, but the effect was not apparent among cancer patients.
This study analyzed patients aged at least 75 years to avoid the analysis of too many heterogeneous group of patients in terms of comorbidity and physical activity. Moreover, it has been reported that the risks related to surgery start to increase after 75 years of age. 20 During the preoperative evaluation, different scores can be used to help to evaluate the individual risk and guide the clinical decision-making. Among the aged, it is important to understand the overall effect of the comorbidities and activity of the patient prior to making a recommendation for high-risk surgery. The CFS has been developed to describe the overall performance status. In earlier studies, CFS > 4 has been associated with poorer postoperative outcomes among aged patients.21 –23 In this study, there were two patients whose CFS was over 4, demonstrating that pancreatic surgery was recommended for only a very selected group of patients. This was also apparent in the ChCoI distribution and in the preoperative physical performance status. Still, ASA class distribution showed major comorbidities among 50% of the patients, emphasizing that ASA class does not adequately describe the overall status of an older patient. Overall, mortality was comparable to earlier reports from high-volume centers and for whole age cohort. 24 This demonstrates the patient selection for pancreatic surgery was rational and at a good level.
In a study by Park et al., 9 32% of patients above 75 years of age had severe complications and in studies including all age groups, the proportion of major complications has been 20%–40%.25,26 Among aged, overall postoperative morbidity may be even more crucial. The CoCoI offers a more detailed tool to evaluate the accumulation of multiple complications. Recently a study by Ricci et al. 27 reported a median CoCoI level for pancreatic surgery of 21 for all age groups. Both incidence of severe complications and median CoCoI were comparable in this study. The patient selection leading to a relatively homogeneous and fit patient population probably explained why none of the preoperative scores predicted severe complications, despite the high NPV values among patients with low-risk preoperative features according to the indices.
Severe complications were associated with preoperative normal hemoglobin and over 1000 mL bleeding intraoperatively. Only four patients with low hemoglobin values experienced severe complications, which prevented detailed analysis of the findings, which could be attributed to coincidence.
A vein resection showed a trend toward a risky short-term prognosis and accumulation of complications. The safety of vein resection has recently been active researched, but no obvious risk in the aged has been reported. 28 In this study population, only five patients underwent vein resection, which inhibits the generalization of the finding. However, in a patient with a locally advanced or borderline resectable tumor likely to be undergoing a vein resection, more intense efforts should be devoted to perioperative evaluation and rehabilitation.
Among the aged, complications or even just problems with insulin therapy may result in hospitalization of a previously active patient. Median hospital stay at the operating hospital was 11 days, which was at the same level as reported previously from Finnish pancreatic centers in Ahola et al. 26 Still, one-fifth of the patients experienced hospitalization over 60 days. This was associated with severe complications, infectious complications, POPF, but not with CoCoI or preoperative scores. The NPV for not returning home after 8 weeks were low if a patient did not present high-risk scores in preoperative indices. However, the PPVs for returning home were also high if a patient had a high-risk feature, demonstrating the challenges of preoperative evaluation. The finding that both POPF and infectious and severe complications may delay returning home is most likely explained by the fact that these often occur in the same patients. All in all, potentially long postoperative rehabilitation period is not easy to predict preoperatively, and postoperative quality of life can be affected even among fit patients if complications emerge.
A study published in Finland reported 1-year survival rate of 70% after PDAC. 29 In this study, 1-year survival was at the same level despite high age. Still, despite successful surgery, not all PDAC patients (66%) were enrolled for adjuvant therapy and were able to gain the best treatment combination of surgery and oncologic therapy. However, Park et al. 9 reported that surgery also resulted in better prognoses among patients above 75 years of age than oncological therapy alone. This emphasizes that it is reasonable to offer pancreatic surgery if the patient enjoys good physical performance status.
Good physical performance status in this study was associated with the survival of at least 1 year. In Finland, the life expectancy at the age of 80 is 8 years, and those who are physically fit can be expected to live considerably longer. 30 This suggests that, especially among patients with a high-risk premalignant disease, surgery can be beneficial for aged patients in excellent health. Among these patients, even more quality life years can be gained than among PDAC patients.
The weakness of this study is the small sample size and the retrospective nature of this study. During the study period, there was no specific, systematic preoperative screening program in use for aged patients in Tampere University Hospital. However, the patients were evaluated in an MD meeting prior to their visit in the outpatient clinic. Evaluating the treatment selection process from the beginning and judging the possibility of undertreatment would require detailed analysis including patients not offered surgery. This was out the scope of this study, but further studies may enlighten the matter. Although the process was not standardized, this did not lead to excessive postoperative mortality or morbidity and the overall results were at good level. These results were explained by the good overall performance status of the patients. Still, the low number of severe complications impeded the statistical analysis and interpretation.
The strength of this study was the fact that all aged patients undergoing pancreatic resection between 2012 and 2019 were included. This approach yields reliable results describing the real-life experiences of aged patients. The scores selected for this study (CFS, ChCoI, CoCoI, GNIR, and SMI) were defined retrospectively. The data for these were well documented in the patient files and the scores can be considered reliable. Although no data on possible supportive nursing facilities arranged postoperatively were available for this study, the data on the patient’s location at 2 months could be tracked from hospital databases. This offered an insight into the patients’ postoperative recovery. The fact that the patients were operated on in a high-volume center prevents the generalization of the results to every hospital.
Despite the active research, the beneficial prognostic factors for survival with PDAC or the progression of premalignant lesions remain unknown. With current perioperative treatment, including modern anesthesia and intensive care, most patients can be successfully managed for 30 or even 90 days even after complications from pancreatic surgery. This stresses the importance of a longer perspective on postoperative outcome and the ability to return to a sufficient quality of life. This study shows that the preoperative prediction of prolonged postoperative rehabilitation is challenging even among the fit aged. Still, when a patient is fully informed and preoperative frailty is mild, this study shows that the risks inherent in pancreatic surgery are tolerable. However, more accurate prognostic tools for patient evaluation and improved methods for perioperative rehabilitation are needed for major pancreatic surgery.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969221083136 – Supplemental material for Preoperative measures predicting outcome after pancreatic resection in aged patients
Supplemental material, sj-docx-1-sjs-10.1177_14574969221083136 for Preoperative measures predicting outcome after pancreatic resection in aged patients by Reea Ahola, Antti Siiki, Irina Rinta-Kiikka, Ismo Laitinen, Anne Antila, Esa Jämsen and Johanna Laukkarinen in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors thank Virginia Mattila for proofreading the article and statistician Mika Helminen for commenting on the analysis. The authors also thank for the support and funding from State Research Funding (VTR), Finland and the Sigrid Jusélius Foundation, Finland. Funding played no role in study design, data collection, data analysis, article preparation, or publication decisions.
Author contributions
R.A. and A.S. participated in the study design; R.A. and I.L. performed data collection; I.R.-K. performed radiological reanalysis; R.A., A.S., I.R.-K., E.J., and J.L. performed analysis and interpretation; R.A., A.S., E.J., J.L., I.R.-K., I.L., and A.A. participated in reviewing and editing; E.J. and J.L. supervised the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors appreciate the support and funding from State Research Funding (VTR), Finland and the Sigrid Jusélius Foundation, Finland. Funding was not involved in the study design, data collection, data analysis, manuscript preparation, or publication decisions.
Context and relevance
Patients with Clinical Frailty Scale below 5 do not present major predominance of postoperative complications after a pancreatic resection but may need hospitalization for more than 2 months.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.