
Abstract
Background and objective:
Our aim was to assess long-term metal ion level changes and clinical outcome in patients with a Birmingham hip arthroplasty.
Methods:
For the purpose of this study, we identified all BHR hip resurfacing arthroplasty (HRA) and total hip arthroplasty (THA) operations performed in Turku University Hospital. A random coefficient model was used to compare the change between the first and last metal ion measurement. A Kaplan–Meier estimator was used to assess the survivorship of the BHR HRA and BHR THA with metal related adverse events (pseudotumor, elevated metal ions above the safe upper limit, revision due to metallosis), or revision due to any reason as endpoints with 95% confidence intervals (CIs).
Results:
BHR HRA was used in 274 hips (233 patients). In addition, we identified 38 BHR-Synergy THAs (38 patients). Operations were performed between 2003 and 2010. Median follow-up time was 14 years for BHR HRA (range: 0.6–17) and 11 years for BHR THA (range: 4.7–13). In the BHR HRA group, geometric means of Cr and Co levels decreased from 2.1 to 1.6 ppb and 2.4 to 1.5 ppb, respectively, during a 3.0-year measurement interval. Metal ion levels in the BHR THA group did not show notable increase. The survivorship of BHR HRA was 66% in 16 years and 34% for BHR THA at 12 years for any metal-related adverse event.
Conclusions:
Patients with a Birmingham hip device do not seem to benefit from frequent repeated metal ion measurements. The amount of patients with metal-related adverse events was relatively high, but many of them did not require surgery.
Introduction
The usage of metal-on-metal (MoM) hip implants has decreased substantially due to high revision rates. Nevertheless, approximately 1.5 million MoM hip implants have been implanted worldwide. 1 Despite of the high revision rates associated with metal bearing, majority of these implants are still in situ, and concerns remain regarding the adverse reaction to metal debris (ARMD) and blood metal ion levels in longterm. 2
As for MoM total hip arthroplasties (THAs), implant survival of most MoM hip resurfacing arthroplasty (HRA) brands have been poor compared to conventional bearing surfaces. 3 However, the Birmingham hip resurfacing (BHR HRA, Smith & Nephew, London, United Kingdom) device is still in scarce use especially in England and Australia4,5 due to satisfying outcome compared to other HRA brands.6,7 The 10-year overall survival rate for all HRA has been 86% while BHR HRA has 91% 10-year survival in Finland. 8
Regulatory authorities worldwide have recommended regular follow-up for MoM hip arthroplasty patients to detect metal bearing–related complications. Screening tools to detect ARMD consist of blood metal ion level measurements, hip imaging, and patient-reported outcome measure questionnaires. Soft tissue imaging (ultrasound, computed tomography (CT), metal artifact reduction sequence (MARS) magnetic resonance imaging (MRI)) have good sensitivity in detecting ARMD, but they are often too expensive and resource consuming to be used as a sole screening tool. Various safe upper limit (SUL) values for blood metal ion levels have been suggested to detect the failing MoM implants.9–13 However, recently SUL thresholds have been suggested to be implant specific.14,15
Our primary aim was to investigate if there is substantial change in the whole blood (WB) metal ion levels in long term after BHR HRA or BHR THA. Furthermore, we assessed clinical and imaging outcome for these implants and risk factors for revision surgery to optimize the follow-up.
Methods
We performed a retrospective cohort study to assess long-term blood cobalt (Co) and chromium (Cr) levels and clinical outcome in BHR HRA and BHR THA patients operated at our institution. BHR HRA consists of a trimmed femoral head, capped with a large-diameter modular BHR head covering and a BHR monoblock acetabular cup. BHR THA consists of a large-diameter modular BHR head, a large-diameter BHR monoblock acetabular cup and a Synergy femoral stem.
A routine screening program for MoM hips was used at our institution to detect patients with ARMD. The screening was performed in consensus with the follow-up protocol recommended by the Finnish Arthroplasty Society. 12 The screening included anteroposterior and lateral radiographs of the hip, WB Cr, and Co measurements and the Oxford Hip Score (OHS). 16 Furthermore, if patients had poor or moderate OHS score (below 33 points), or elevated WB Cr or Co concentration (above 5 ppb), they were referred to MARS-MRI. Patients with poor or moderate OHS or elevated WB ion measurements were also clinically evaluated by a senior orthopedic surgeon at our outpatient clinic. If patients had severe hip symptoms (pain, clicking, and swelling) or if a pseudotumor was detected in MRI, revision surgery was considered. In addition, if an asymptomatic patient had WB metal ion levels above 10 ppb, revision surgery was considered to minimize the risk of Co poisoning. Patients who were not admitted to revision surgery were scheduled for annual or biannual visits in our outpatient clinic. Blood samples from all participating patients were collected and analyzed using the same methods that we have described earlier in our previous publications.17,18
All data were obtained from the Turku University Hospital data lake and electronic medical records.
In this study, SULs of 4.6 ppb for Cr and of 4.0 ppb for Co were used based on earlier study by Van Der Straeten. 13 The proportion of patients exceeding the SUL values of Cr and Co in the repeated measurements were reported.
Standard anteroposterior and shoot through lateral radiographs were used to assess anteversion and inclination angles of the cup. MARS-MRI images were evaluated by a musculoskeletal radiologist experienced in ARMD-related MRI diagnostics. Special attention was given to soft-tissue masses and periarticular fluid collections. Findings were graded using Hart pseudotumor classification. 19
We used the OHS—questionnaire to measure the functional outcomes of patients with BHR HRA or BHR THA during the follow-up. OHS has a scale of 0–48, with 48 being the best patient-reported outcome. A score below 26 was considered as a bad outcome, 27–33 points was considered to as a moderate outcome, 34–41 was considered as a good outcome, and 42–48 was considered as an excellent outcome. In addition, revision operations and reasons for revision surgery were checked manually from the patient records.
Ethics
The study was based on the national recommendation for systematic screening of MoM hip arthroplasty patients given by the Finnish Arthroplasty Society (2014). It was a register study, and the patients were not directly contacted. Therefore, approval by the local ethical committee was not needed.
Statistics
The individual change between two consecutive metal ion measurements from the same patient was modeled using a random coefficient model. Log-transformed ion values were used in conditional models due to positively skewed distribution of ion levels. Results were reported as geometric means and medians with range at the initial and control measurements for better interpretation. Spaghetti plots for naturally log-transformed ion values were generated to visualize individual changes in ion levels. A Kaplan–Meier estimator was used to analyze the overall survivorship function, with revision surgery as the endpoint with 95% confidence interval (CI). A separate Kaplan–Meier analysis was performed to assess the survivorship of the BHR HRA and BHR THA patients with metal-related adverse events (pseudotumor, elevated metal ions above the SUL, or revision due to ARMD) as endpoints with 95% CI. Wilcoxon rank sum test was used to compare the OHS scores and ion levels of patients with a radiologically diagnosed pseudotumor and patients without a radiologically diagnosed pseudotumor.
Hazard ratios (HRs) with 95% CI for metal-related adverse events (pseudotumor, elevated metal ions above the SUL, or revision due to ARMD) were assessed using multivariable Cox regression analysis, adjusting for potential contributory factors age, sex, bilateral surgery, inclination angle, and anteversion angle. None of these variables were considered to be along causal pathway from exposure to outcome but were considered as confounders. The proportional hazards assumption for Cox analysis was evaluated with a statistical test based on scaled Schoenfeld residuals. 20
P-values lower than 0.05 in a two-tailed test were considered statistically significant in all analyses. All statistical analyses were carried out using the R statistical computing environment version 3.5.3. 21
R packages survival (version 3.2-10) and ggplot2 (version 3.3.3) were used for survival analysis and visualizations, respectively.
Results
BHR was the most common HRA device at our institution with 233 patients (274 hips). Fourty one patients had bilateral operation. In addition, we identified 38 patients who had a BHR-Synergy THA. There were no patients with bilateral BHR THA. BHR HRA operations were performed from 2003 to 2010 and BHR THA operations between 2007 and 2009. Median age of the patients was 53 years (interquartile range (IQR) = 10 years, range: 18–76). Eighty nine (33%) were female. The follow-up data from the patients were collected until November 2019 or eventual death. The number of deceased patients during the follow-up was 23. Median follow-up time for BHR HRA and BHR THA was 14 years (range: 0.6–17) and 11 years (range: 4.7–13), respectively. Patient characteristics are presented in Table 1.
Patient characteristics hipwise and patientwise.
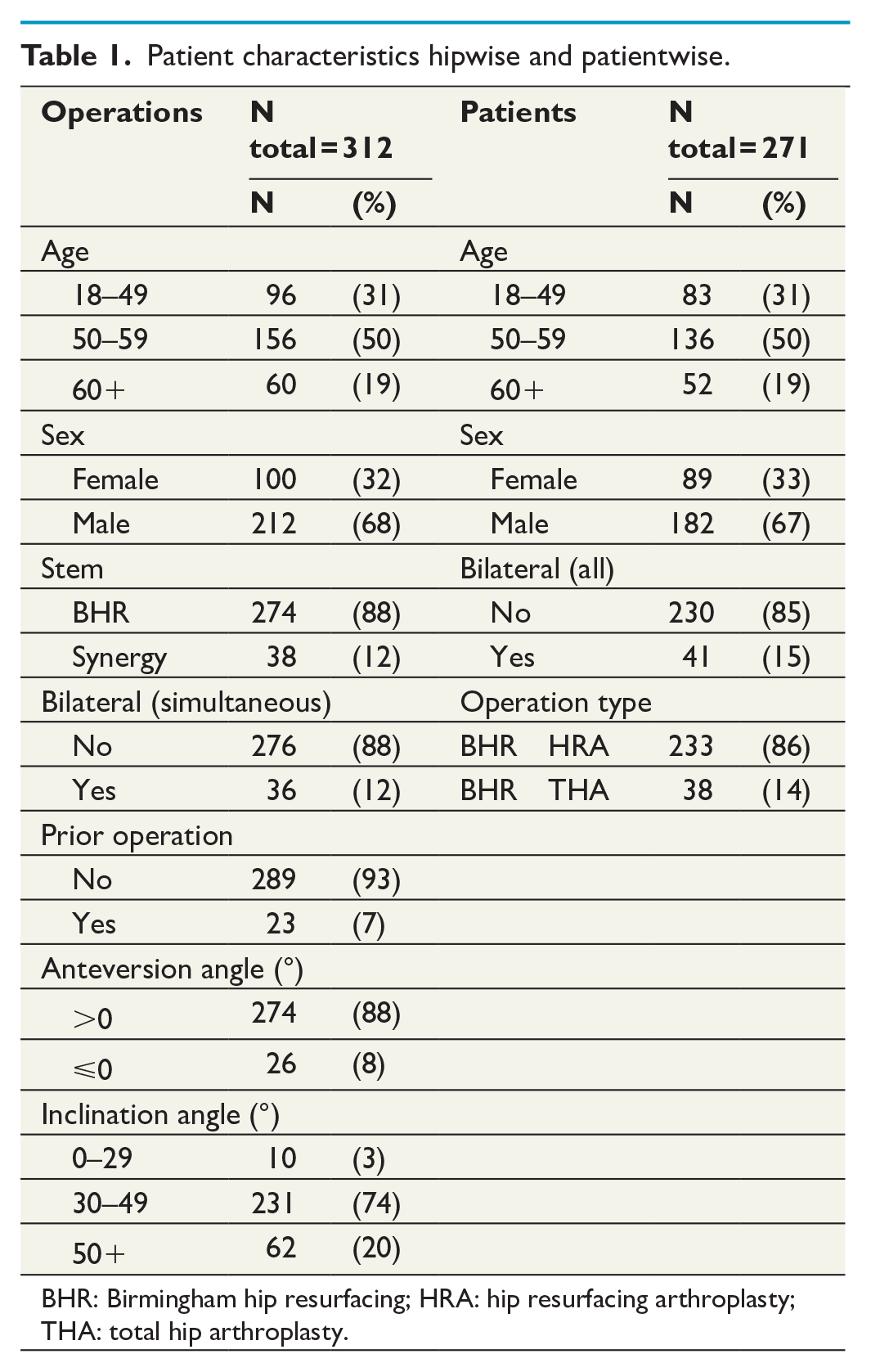
BHR: Birmingham hip resurfacing; HRA: hip resurfacing arthroplasty; THA: total hip arthroplasty.
A total of 223 patients (193 BHR HRA and 30 BHR THA) with one or more metal ion measurements during the follow-up were identified. One hundred and seventy one BHR HRA and 19 BHR THA patients had two or more metal ion measurements (BHR HRA: median = 2 (range: 2–6), BHR THA: median = 3 (range: 2–5)). If a patient had more than two consecutive metal ion measurements, the first and the last of the measurements were used to assess change. The median time from the first metal ion measurement (initial measurement) to the last (control measurement) was 3.0 years (range: 0.8–6.8 years), and it was considered as the measurement interval. The mean time from the index operation to the initial metal ion measurement was 7.5 years (range: 3.9–14). For staged bilateral patients, this was calculated from the date when the second hip was operated. The follow-up data were collected until 28.10.2019. Twelve patients with BHR HRA did not have inclination or anteversion angle data. Furthermore, 151 hips had been imaged using MARS-MRI, and 192 patients (175 BHR HRA and 17 had BHR THA) had completed the OHS questionnaire postoperatively.
Geometric mean of Co decreased from 2.1 ppb (range: 0.2–122) to 1.6 ppb (range: 0.1–100, p < 0.001) and similarly the geometric mean of Cr decreased from 2.4 ppb (range: 0.7–56) to 1.5 ppb (range: 0.2–63, p < 0.001) during the 3.0 years measurement interval in the BHR HRA group. Metal ion levels in the BHR THA group did not show notable increase. Differences in metal ion levels and p values are demonstrated in Table 2.
Differences in Co and Cr ion levels (ppb).
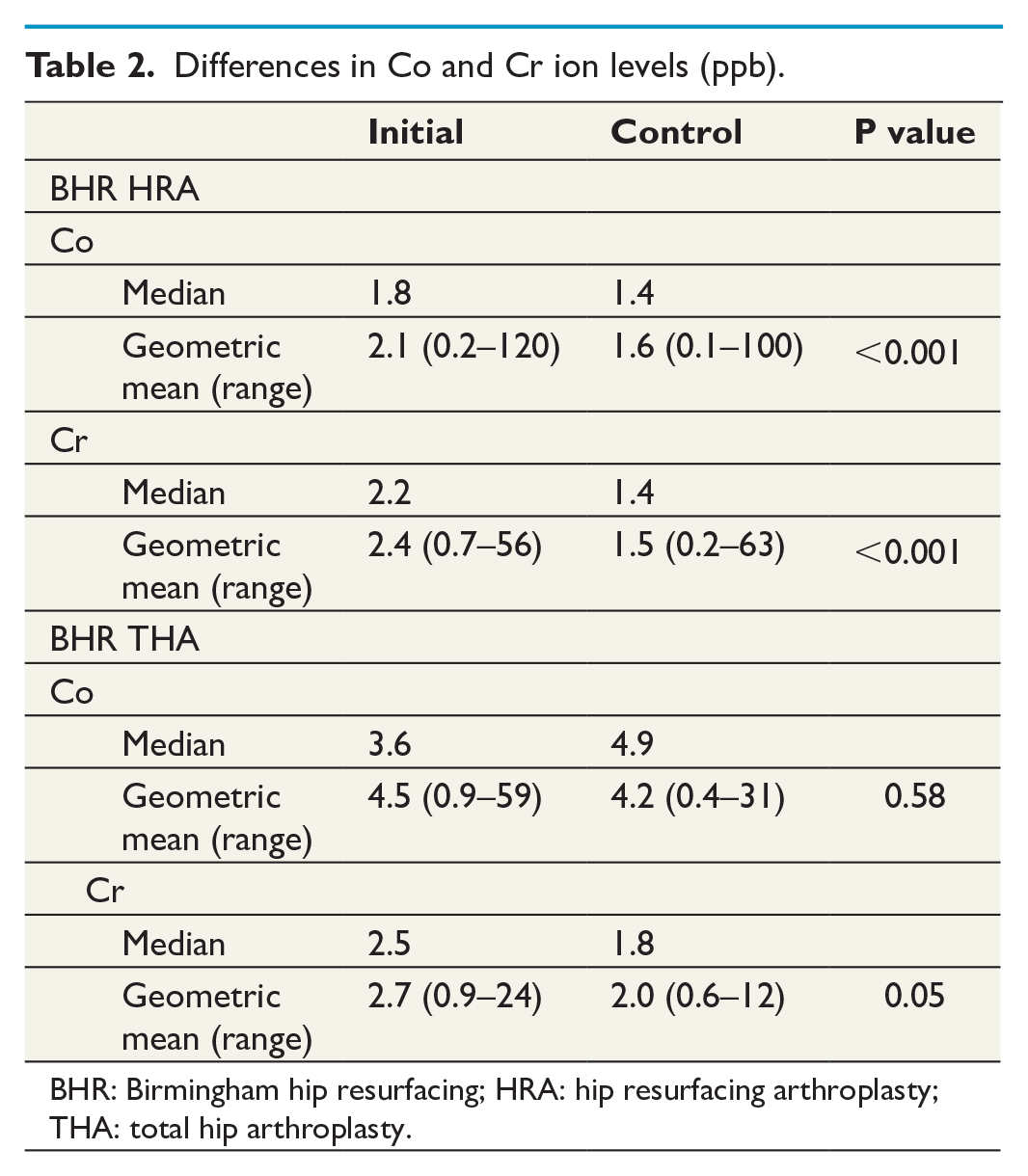
BHR: Birmingham hip resurfacing; HRA: hip resurfacing arthroplasty; THA: total hip arthroplasty.
In the whole cohort, Co values were above the SUL in 55 patients (25%) in the first measurement and above the SUL in 41 patients (22%) in the last measurement. In a similar manner, Cr values were above the SUL in 32 patients (14%) in the first measurement and above the SUL in 21 patients (11%) in the last measurement. Overall, 26 patients had ion levels above 10 ppb during follow-up and 12 of them eventually had a revision (10 patients had a revision due to ARMD). Change of individual Co and Cr values are presented in Fig. 1.
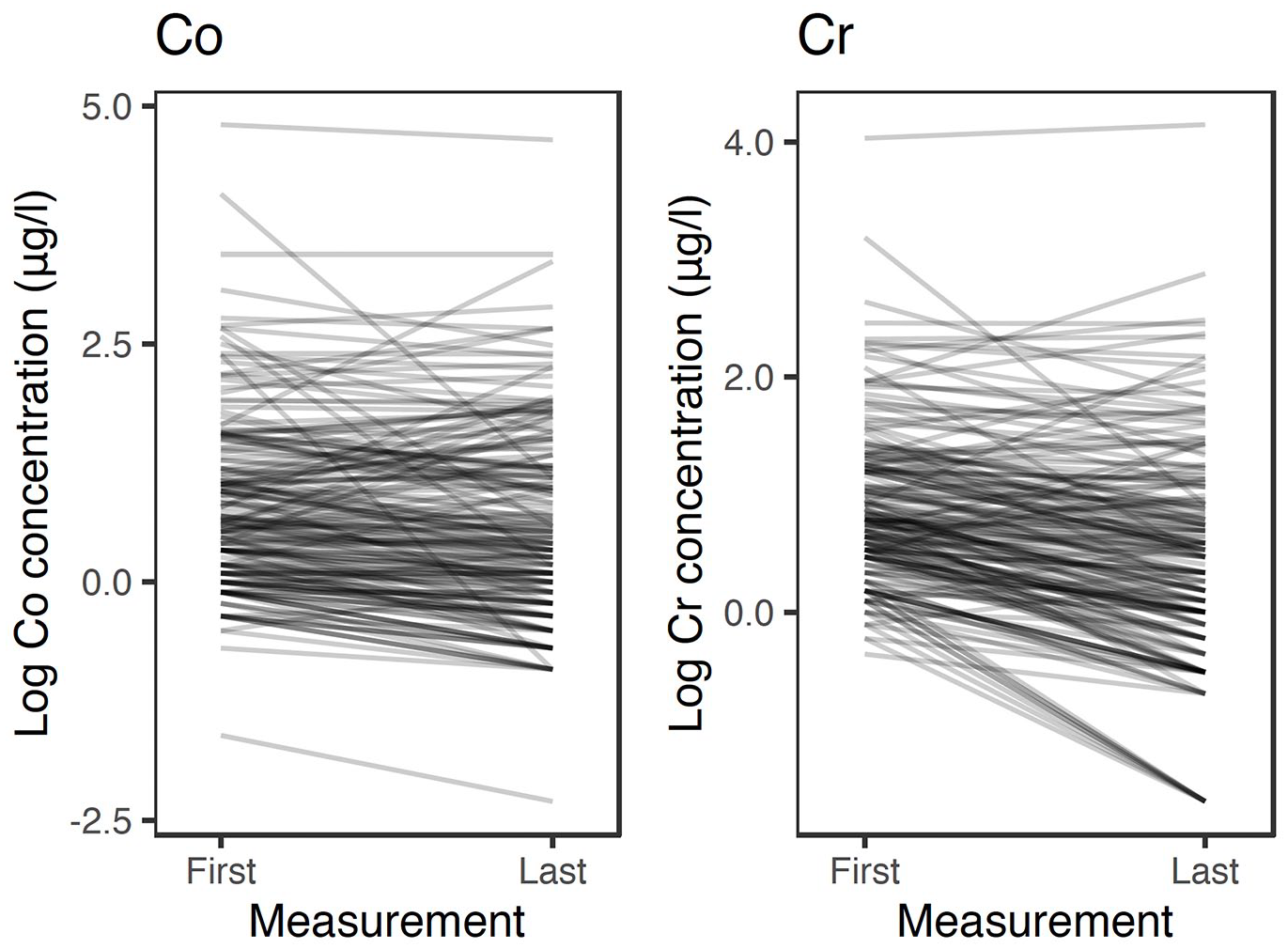
Naturally log-transformed spaghetti plots for individual Co and Cr values for all patients.
Out of the 151 hips with MARS-MRI imaging, we identified 62 hips (41%) with radiologically diagnosed pseudotumor. Of these, 24 were Hart 1, 10 Hart 2A, 23 Hart 2B, and 5 Hart 3. If patients had repeated MARS-MRI imaging, we reported the one with the highest grade pseudotumor. Eighteen hips with a pseudotumor had more than one MARS-MRI done. In eight hips, the size and grading of the pseudotumor remained similar. In one hip, the pseudotumor was no longer visible in the repeated MARS-MRI. In three hips, pseudotumors had decreased in size in the repeated MARS-MRI. On the other hand, in five hips, the pseudotumor had increased in size in the repeated MRI, and in one of these hips, the grade of the pseudotumor was higher in the repeated MARS-MRI. In addition, 26 hips had repeated MARS-MRI with normal initial MARS-MRI images. New pseudotumor was detected in five hips, while the repeated MARS-MRI was normal in 21 hips. Patients with a radiologically diagnosed pseudotumor presented with significantly higher maximum Co (p < 0.001) and Cr values (p < 0.001) than patients without a pseudotumor. Patients without a radiologically diagnosed pseudotumor had a median Co of 1.8 ppb (IQR and median Cr of 2.2 ppb (IQR = 1.8)) while patients with a radiologically diagnosed pseudotumor had median Co of 5.8 ppb (IQR = 10.5) and median Cr of 4.2 ppb (IQR = 4.7).
Implant survival with revision for any reason as the endpoint
We had an overall implant survival of 83% in 16 years for BHR HRA and 87% for BHR THA at 12 years with revision for any reason as the endpoint. Fourty hips of 274 were revised in the BHR HRA group, and 5 of 38 hips were revised in the BHR THA group (Fig. 2). ARMD was the most common reasons for revision in both BHR HRA and BHR THA groups (10 (25%) and 3 hips (60%), respectively). Other reasons for revision in BHR HRA group were: periprosthetic fracture (7 hips), loosening of the cup (7 hips), loosening of the femoral component (5 hips), mechanical impingement (4 hips), infection (2 hips), implant mal-alignment (2 hips), pain (1 hip), grossly elevated metal ions (1 hip), and leg length discrepancy (1 hip). Other reasons for revision in BHR THA group were infection and pain (1 hip each).
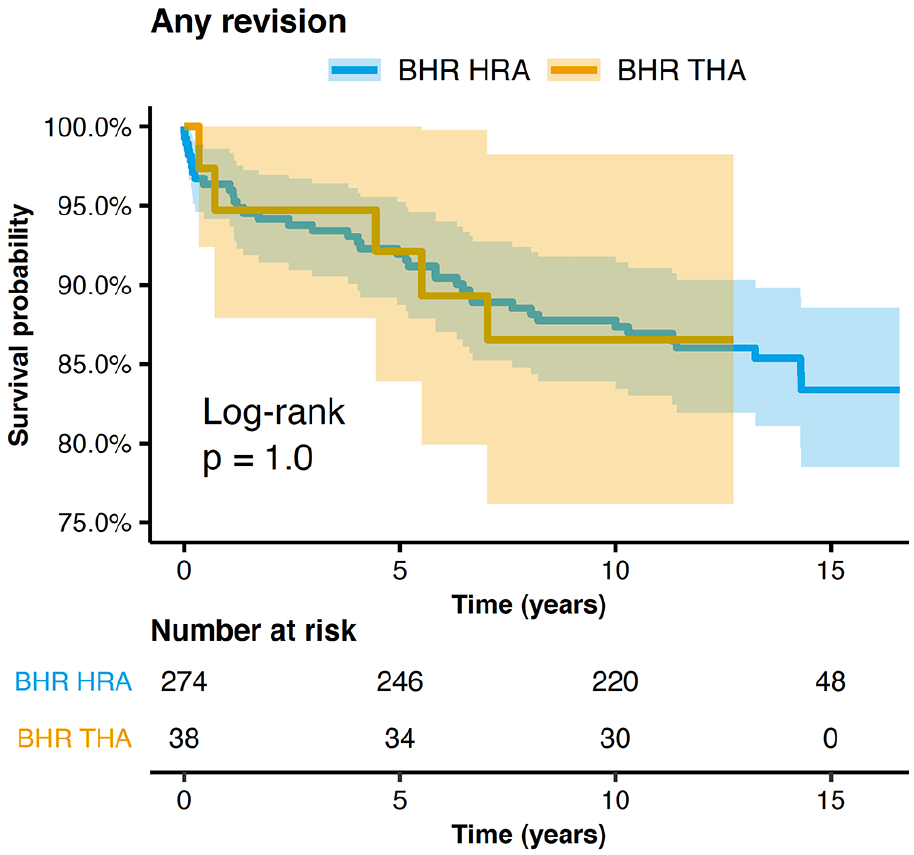
A Kaplan–Meier estimator for both BHR HRA and BHR THA with revision surgery as the endpoint with 95% CI.
Survival with any metal-related adverse event (pseudotumor in MARS MRI, elevated metal ions above the SUL, or revision due to ARMD) as the endpoint
The overall survival of the hips in terms of metal-related adverse events (pseudotumor, elevated metal ions above the SUL, or revision due to ARMD) was 63% at 16 years. For BHR HRA separately, it was 66% in 16 years and for BHR THA, it was 34% at 12 years from the operation (Fig. 3). The total number of metal-related adverse events during our follow-up was 98.
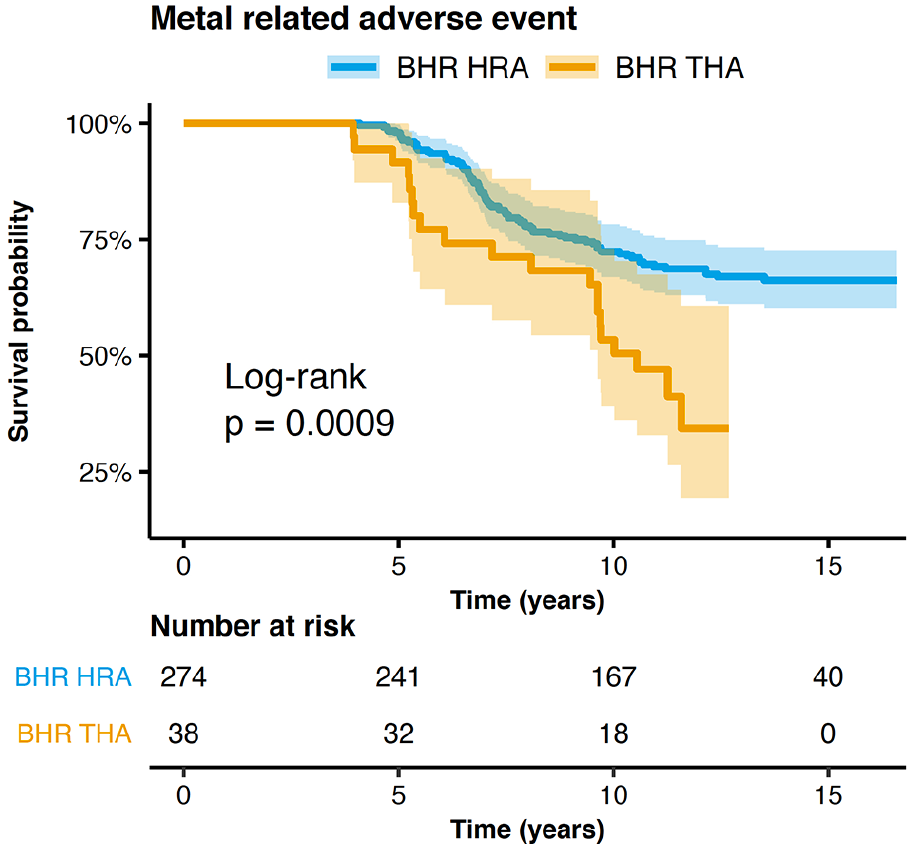
A Kaplan–Meier estimator for both BHR HRA and BHR THA with metal-related adverse events as the endpoint with 95% CI.
Overall, 175 out of 192 patients (91%) had good to excellent OHS scores postoperatively. In BHR HRA group, 161 patients out of 175 reported a good to excellent outcomes, while only 6 patients (4.9%) reported having a bad outcome. In BHR THA group, 13 patients (77%) out of 17 had an excellent outcome, and 3 patients (20%) reported a bad outcome. Patients without a radiologically diagnosed pseudotumor (n = 148) had a median OHS score of 46 (IQR = 7, range: 2–48), while patients with a radiologically diagnosed pseudotumor (n = 44) had a median OHS score of 44 (IQR = 9, range: 3–48). The difference between OHS scores was statistically significant (p = 0.03).
In Cox multivariable regression analysis, cup retroversion was associated with increased risk of adverse events when compared to cups that were in anteversion with an HR of 3.9, and the difference was statistically significant (p < 0.0001). Cox multivariable regression analysis data with 95% CI is presented in Table 3.
Cox multivariate regression analysis data with 95% CI.
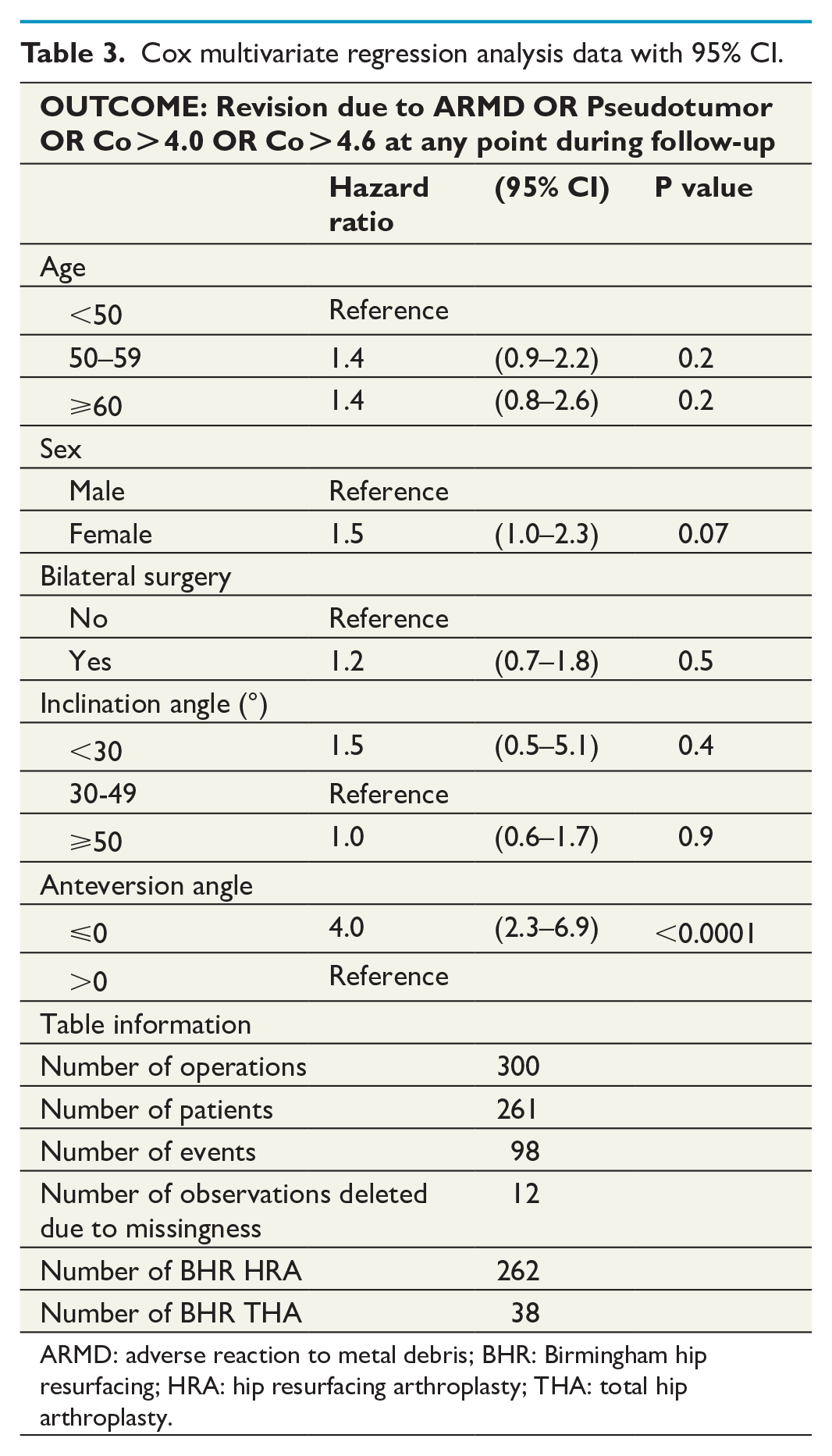
ARMD: adverse reaction to metal debris; BHR: Birmingham hip resurfacing; HRA: hip resurfacing arthroplasty; THA: total hip arthroplasty.
Discussion
The aim of this study was to assess long-term blood Co and Cr levels and clinical outcome for patients with BHR HRA or BHR THA. WB Co and Cr levels in BHR patients stayed mostly below the SUL. Furthermore, we noted a statistically significant decrease in both Co and Cr levels during median follow-up time of 14 years in BHR HRA group. Metal ion levels in BHR THA group did not show notable increase during a follow-up of 11 years. The amount of patients with metal-related adverse events was relatively high, but many of them did not require surgery.
Our results regarding decreasing ion level trends are in line with previous studies. Van der Straeten et al. studied WB Co and Cr change in patients with well-functioning BHR implants. Overall, Co and Cr levels decreased significantly in their cohort at 10–13 years in asymptomatic patients. 22 Also, patients with unilateral or bilateral ReCap-M2A-Magnum MoM THA had decreasing ion levels in long-term follow-up. Authors discussed that these patients might not benefit from repeated metal ion measurements on as short as a 2-year interval.17,18 Even when the high-risk articular surface replacement (ASR) implants were assessed, Reito et al. reported that patients with a unilateral ASR HRA might not benefit from repeated metal ion measurements on a 1-year interval. However, high-risk ASR XL THA patients did benefit from repeated metal ion measurements in order to detect patients with ARMD. 9 National guidelines recommend regular WB metal ion measurements in the follow-up of patients treated with MoM implants. However, performing regular metal ion measurements for all MoM hip patients is both expensive and resource consuming.12,23 Based on our study and earlier literature, 2-year interval seems rather short for repeated ion measurements in patients with BHR HRA or BHR THA device. For long-term follow-up, for example, 5-year interval might be more appropriate.
MARS-MRI in our study was performed only to patients with poor or moderate OHS scores, symptomatic hip, or elevated WB Co or Cr ion levels. Thus, the reported high prevalence of pseudotumor in MARS-MRI does not represent the whole cohort of patients. Ideally, we would have had MARS-MRI images from all the patients with a BHR hip implant. As expected, levels of both Co and Cr were higher in patients with a radiologically diagnosed pseudotumor. Only 3 out of 17 pseudotumors increased in size in repeated MRI. Relatively high prevalence of pseudotumors in MARS-MRI of BHR patients have been reported previously, but the data concerning the subject is scarce. 19 Bisschop et al. reported a prevalence of 28% for pseudotumors in CT scans of BHR HRA patients, and majority of these (72.5%) were asymptomatic. 24
Regarding to the OHS score, majority of the patients in our study reported good to excellent scores after the BHR implantation. Comparably, Matharu and colleagues reported a total of 1394 OHS questionnaires with excellent outcomes, pre-operative OHS score improving from pre-operative 19–46 at the latest visit. 25 In our study, patients with a radiologically diagnosed pseudotumor reported inferior OHS scores when compared to patients without a radiologically diagnosed pseudotumor, although the difference was not necessarily clinically significant. Unfortunately, our patients do not have pre-operative OHS values. Kwon et al. found out that asymptomatic MoM HRA patients with a pseudotumor may have even lower OHS scores than patients without a pseudotumor (41 and 47 points, respectively). 26 However, this correlation between symptoms and pseudotumor incidence is not clear. 27
The survival of BHR HRA was 83% at 16 years and that of BHR THA 87% at 12 years in our material. This is in line with Finnish Arthroplasty Register which reports a revision rate of 13% for BHR at 15 years. 7 The Australian registry reports a slightly better survival with BHR HRA with 7% revision rate at 10 years and 10% at 15 years. 28 In a similar manner, NJR reports a revision rate of 8% at 10 years and 11% at 15 years for BHR HRA. 6
In the short- to mid-term follow-up, BHR HRA and BHR THA seemed to have equally good survival rates with 95% and 97% at 6 years, respectively. 29 However, in the long-term follow-up BHR THAs revision rates increase to 18% at 10 years, which is higher than for majority of the other MoM THA or HRA brands.7,28 We did not notice this increased revision rate compared to BHR HRA in this study. The amount of BHR THA was rather small, though. Due to the previously reported high risk of ARMD and revision surgery, the implantation of BHR THA is no longer recommended. 30
Sole revision rate might not tell the whole truth about adverse events or functional failure. Therefore, we assessed separately survival with any metal-related adverse event (pseudotumor in MARS-MRI, elevated metal ions above the SUL, or revision due to ARMD) as the endpoint. It seems that we had considerable amount of metal-related adverse events, although most of them did not require revision surgery. This is especially true with the BHR THA.
Cup positioning has been reported to be a risk factor for increased wear and metal bearing–related complications. Excessive anteversion, insufficient anteversion or increased cup inclination increase the risk of posterior edge loading and impingement in MoM implants, which can lead to excess wear.31,32 In our study, only the retroversion of the acetabular cup was associated with an increased risk for metal-related complications, although bilateral surgery or cup inclination did not have an effect. There is some evidence that pseudotumors do not have to necessarily be associated with high wear or increased metal ion levels, and they can occur in well-positioned implants, suggesting that patient susceptibility has an important role in the development of pseudotumors. 33
We acknowledge that our study had several limitations. First, the measurement interval was relatively short. Longer follow-up might change the course. Another limitation was that some patients with poor clinical outcome may have been revised before any metal ion measurements were done. Furthermore, all patients did not go through MARS-MRI or fill in OHS questionnaire which might have skewed the results. Our results are implant specific, and therefore not generalizable to other MoM devices. In this study, we used SUL values suggested by Van Der Straeten et al. (2013) for unilateral HRA implants. We used this SUL value for both unilateral and bilateral BHR HRA and unilateral BHR THA patients for better interpretability.
Conclusion
We found that WB metal ion levels decrease during the long-term follow-up in BHR patients. Patients with a well-functioning BHR hip may not necessarily benefit from routine metal ion measurements on a 2-year interval. The amount of patients with a metal-related adverse events was relatively high, although revision surgery was not always needed.
Footnotes
Acknowledgements
The authors thank nurse Mari Järvinen, who is responsible for managing the MoM hip follow-up in Turku University Hospital.
Authors contributions
K.T.M. and M.S.V. designed the protocol and methods. K.T.M. performed the surgery, recorded the intraoperative data, and arranged the follow-up of the patients. M.S.V. analyzed the data and did the statistics. S.P., K.T.M., and M.L. collected the data. S.P., M.L., I.L., P.L., and K.T.M. wrote the manuscript. All authors contributed to the revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M.S.V. reports funding from the Academy of Finland (grant no. 322123). No benefits in any form have been received related directly to this article.