
Abstract
Background:
Given the scarce evidence regarding the impact of preoperative nutritional status on surgical outcomes of patients with hepatocellular carcinoma, predictive powers of nutritional/inflammatory scores for short-term surgical outcomes in patients with hepatocellular carcinoma were investigated.
Methods:
Outcomes of 1272 patients with hepatocellular carcinoma were reviewed, and predictive powers of nine nutritional/inflammatory scores for short-term surgical outcomes were compared using the receiver-operating characteristic curve analysis. Clinical relevance of the best nutritional score was then studied in detail to clarify its utility as an alternative predictive measure for surgical risk of patients with hepatocellular carcinoma.
Results:
Receiver-operating characteristic curve analysis showed the controlling nutritional status score has the best performance in prediction of morbidity after hepatectomy for hepatocellular carcinoma (area under the curve, 0.593; 95% confidence interval: 0.552–0.635; p < 0.001), and multivariate analysis confirmed its correlation with the risk of any morbidity (odds ratio per +1 point, 1.17; 95% confidence interval: 1.08–1.27; p < 0.001) and major morbidity (odds ratio per +1 point, 1.14; 95% confidence interval: 0.99–1.27; p = 0.052). The undernutrition grade based on the controlling nutritional status score showed strong correlation with the degree of fibrosis in the liver (p < 0.001), platelet count (p < 0.001), and indocyanine green retention rate at 15 min (p < 0.001). In addition, the controlling nutritional status undernutrition grade well stratified the risk of postoperative morbidity especially in cirrhotic subpopulation (odds ratio, 1.17 per +1 point; 95% confidence interval: 1.05–1.29 for any morbidity and odds ratio, 1.20 per +1 point; 95% confidence interval: 1.03–1.40 for major morbidity).
Conclusions:
The controlling nutritional status score could be an alternative measure for underlying liver injury and the surgical risk of hepatocellular carcinoma.
Introduction
Meticulous preoperative workup is required for patients undergoing liver resection for hepatocellular carcinoma (HCC) because underlying livers are frequently injured and the risk of postoperative hepatic insufficiency is generally high. 1 Con-ventionally, Child-Pugh score 2 and Model for End-stage Liver Disease (MELD) score 3 have widely been used to estimate the risk of various treatments for cirrhotic patients, and most recently, albumin-bilirubin (ALBI) score 4 is increasingly used in various clinical situations to predict hepatic functional reserve and/or prognosis of patients with liver disease. However, these clinical variables are insufficient to precisely measure the actual metabolic function of the liver, and accordingly not appropriate to be used in the evaluation of minimum requirement of future liver remnant in the field of surgery for HCC.
In Eastern countries, indocyanine green (ICG) clearance test plays an important role in the evaluation of hepatic functional reserve and the risk of postoperative hepatic insufficiency in liver surgery. It has been reported that meticulous preoperative work-up using ICG clearance test and three-dimensional volumetry could safely expand conventional surgical criteria to secure the safety of surgery.5,6 However, because ICG test is not always available in many Western countries, there remains no standardized method for surgical risk evaluation in patient undergoing hepatectomy for HCC worldwide.
Recently, clinical impact of nutritional/inflammatory scores has actively been investigated and their efficacy in prediction of surgical risks and prognosis of patients has been reported in various gastrointestinal cancers.7,8 Because most patients with HCC are likely to have chronic metabolic disorders and concomitant malnutrition which are associated with hepatitis virus infection, alcohol abuse, or obesity, 1 perioperative nutritional status might predict the underlying degree of liver injury and could be an alternative measure for surgical risks in patients undergoing hepatectomy. However, there remains scarce evidence regarding the clinical impact of nutritional status on surgical outcomes of patients with HCC.
Therefore, this study sought to clarify the predictive powers of various nutritional/inflammatory scores for short-term surgical outcomes of patients undergoing hepatectomy for HCC and to investigate the potential utility of preoperative nutritional status for prediction of hepatic functional reserve and postoperative surgical risk of patients with HCC.
Methods
Study population
From a prospective database maintained by the Department of Gastroenterological Surgery, Toranomon Hospital, a total of 1288 consecutive patients who underwent curative liver resection for pathologically confirmed HCC from January 1995 to December 2018 were identified. Of these, 16 patients were excluded due to incomplete clinical records and the remaining 1272 patients were studied in detail. This study was conducted in accordance with the Declaration of Helsinki and the ethical guidelines for clinical study in Japan under approval of the Institutional Review Board at Toranomon Hospital (No. 1919).
Surgical indications and basic surgical procedures
Until 2013, surgical indication for HCC was based on the conventional algorithm that included the presence or absence of ascites, serum total bilirubin level, and the ICG retention rate at 15 min (i.e. Makuuchi’s criteria). 9 Since 2014, expanded criteria using ICG clearance rate of full-functioning future liver remnant estimated by a high-quality three-dimensional volumetry (Shindoh’s criteria)5,6 have been used as long as curative resection of hepatic tumor was thought to be technically feasible. Parenchymal transection was performed by clamp crushing method with LigaSureTM (Medtronic) or pre-coagulation method with MicrotaseTM (Alfresa Pharma Corporation, Japan) with or without Pringle’s maneuver. After removal of specimens, drainage tube was basally placed at the cut surface of the liver for the detection of postoperative bleeding or bile leakage.
Assessment of fibrosis status and short-term surgical outcomes
The histological classifications of the tumor and background liver were described based on the system of the Liver Cancer Study Group of Japan. 10 Fibrotic stage of the underlying liver was determined according to the classification proposed by Desmet et al. 11
All of the morbidities were determined within 90 days after surgery, including readmission. Severity of postoperative morbidity was determined according to the Clavien–Dindo classification 12 and Grade IIIa or greater complication was classified as major morbidity. Postoperative hepatic insufficiency was defined by peak total bilirubin >7 mg/dL 13 and the grade of liver failure was defined according to the definition of the International Study Group of Liver Surgery. 14 Refractory ascites and pleural effusion were defined as requiring drainage or additional use of diuretics.
Assessment of preoperative nutritional/inflammatory status
Preoperative nutritional/inflammatory status was scored the following nine indices using blood sample data obtained within 1 week prior to surgery considering the reported evidence and usability in clinical practice: Glasgow prognostic score (GPS), 15 modified GPS (mGPS), 16 controlling nutritional status (CONUT) score, 17 Naples prognostic score (NPS), 18 albumin-bilirubin (ALBI) grade, 4 platelet-albumin (PAL) grade, 19 neutrophil–lymphocyte ratio (NLR), 20 platelet–lymphocyte ratio (PLR), and lymphocyte–monocyte ratio (LMR) (see Supplemental Table 1 for details). CONUT score is calculated with albumin, lymphocyte, and cholesterol score. Four grades are defined by the total points of these three factors: normal (0–1 point), light (2–4 points), moderate (5–8 points), and severe (9–12 points).
Grades of “light,” “moderate,” and “severe” are gradually defined as poor nutritional states.
Statistical analysis
Continuous values were expressed as the median (range) and were compared using the Wilcoxon’s rank-sum test. Categorical variables were expressed as number (%) and were compared using the Fisher exact test or the chi-square test, as appropriate. A p-value less than 0.05 was considered statistically significant. All the statistical analyses were conducted using JMP software (version 12.2.0; SAS Institute Inc., Cary, NC) and IBM SPSS software (Ver. 23.0; SPSS Inc., IL, USA).
The most appropriate nutritional score for preoperative surgical risk assessment was determined among the nine tested nutritional scores using the receiver-operating characteristic (ROC) curve analysis for global and major postoperative morbidities. Then, its correlation with the short-term surgical outcomes was investigated with a multivariate analysis using logistic regression model with backward selection. Initially, all factors were included in the model. Then, factors that showed no or limited statistically significant association (p > 0.1) with any or major complication adjusted for the remaining factors in the model were deleted from the model in stepwise fashion.
Results
Baseline characteristics
The baseline characteristics of the study population are summarized in Table 1. Median age was 66 (28–89) years, and 956 (75.2%) patients were male. In total, 1096 (86.2%) cases were initial hepatectomy, and the distribution of ASA-PS class of the patients was as follows: 1 (n = 178, 14.0%), 2 (n = 995, 78.2%), 3 (n = 98, 7.7%), and 4 (n = 1, 0.07%). Six hundred fifty-five (51.5%) patients were cirrhotic and major hepatectomy was performed in 68 (5.3%) patients. Median operation time was 160 (28–703) min and median estimated blood loss was 250 mL (0–19,574 mL). Incidences of global morbidity, major morbidity, and in-hospital mortality were 23.7%, 6.5%, and 0.6%, respectively.
Baseline characteristics of the study population.
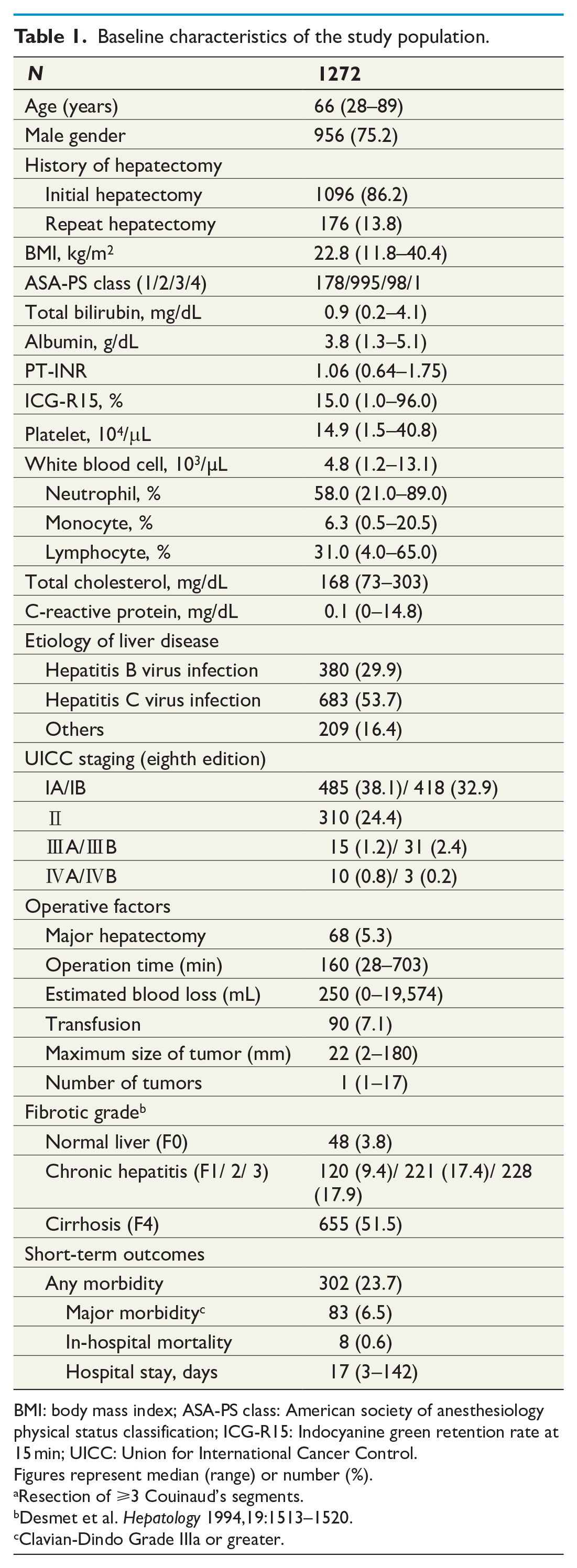
BMI: body mass index; ASA-PS class: American society of anesthesiology physical status classification; ICG-R15: Indocyanine green retention rate at 15 min; UICC: Union for International Cancer Control.
Figures represent median (range) or number (%).
Resection of ⩾3 Couinaud’s segments.
Desmet et al. Hepatology 1994,19:1513–1520.
Clavian-Dindo Grade IIIa or greater.
Clinical relevance of the CONUT score among patients undergoing hepatectomy for HCC
Table 2 summarizes the results of ROC analysis for predictive powers of various nutritional/inflammatory indices for postoperative morbidities. Among the nine tested variables, the CONUT score (area under the curve (AUC), 0.593; 95% confidence interval (CI): 0.552–0.635; p < 0.001) showed the best performance in prediction of the global incidence of morbidity after hepatectomy for HCC. Multivariate analysis confirmed that the CONUT score is an independent predictor for any morbidity (odds ratio (OR) per +1 point, 1.17; 95% CI: 1.08–1.27; p < 0.001) and major morbidity (OR per +1 point, 1.14; 95% CI: 0.99–1.27; p = 0.052) (Table 3).
Predictive powers for preoperative nutritional/inflammatory indices for postoperative morbidity after hepatectomy for HCC.
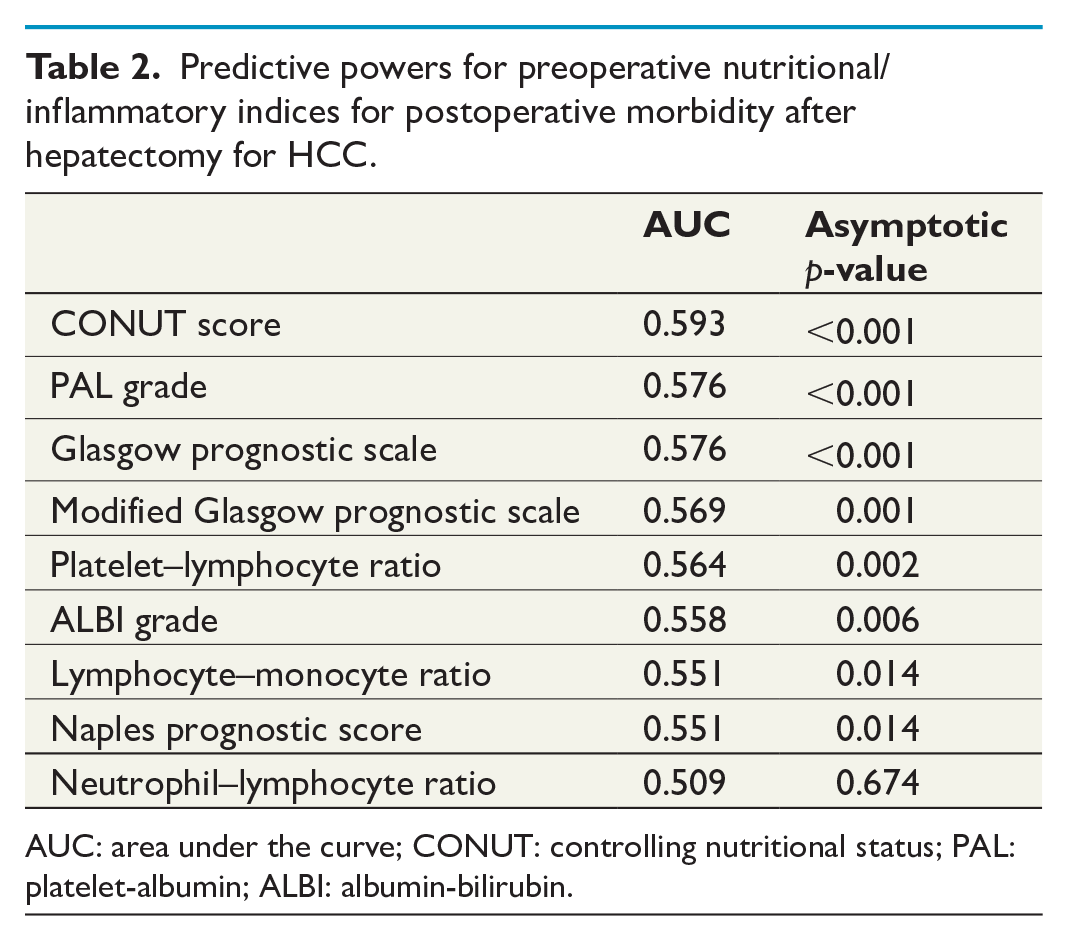
AUC: area under the curve; CONUT: controlling nutritional status; PAL: platelet-albumin; ALBI: albumin-bilirubin.
Predictive factors for postoperative morbidities.
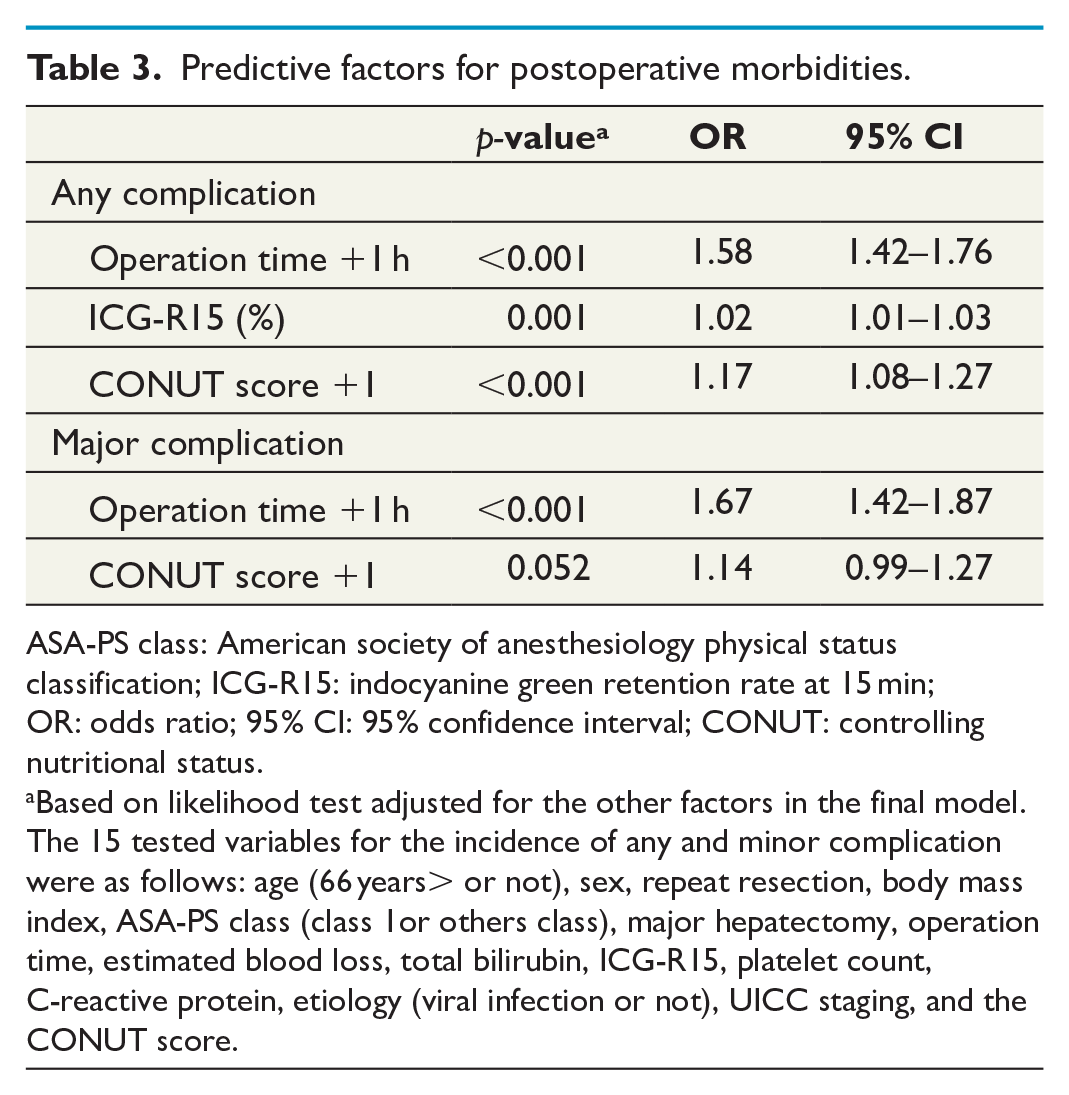
ASA-PS class: American society of anesthesiology physical status classification; ICG-R15: indocyanine green retention rate at 15 min; OR: odds ratio; 95% CI: 95% confidence interval; CONUT: controlling nutritional status.
Based on likelihood test adjusted for the other factors in the final model.
The 15 tested variables for the incidence of any and minor complication were as follows: age (66 years> or not), sex, repeat resection, body mass index, ASA-PS class (class 1or others class), major hepatectomy, operation time, estimated blood loss, total bilirubin, ICG-R15, platelet count, C-reactive protein, etiology (viral infection or not), UICC staging, and the CONUT score.
Given these results, clinical relevance of the CONUT score was further investigated as a potential alternative measure for hepatic functional reserve and surgical risk prediction. First, the population was classified into following four undernutrition grade based on the CONUT score: 18 normal (0–1 point), light (2–4 points), moderate (5–8 points), and severe (9–12 points). Baseline characteristics of these four groups are compared in Supplemental Table 2.
Aside from the variables included in the CONUT score (i.e. albumin, lymphocyte, and total cholesterol), poor nutrition status was associated with multiple factors, including older age, female gender, higher ASA-PS class, and other general parameters associated with hepatic function. Of note, the CONUT undernutrition grade was strongly correlated with the degree of fibrosis in underlying livers (Fig. 1), and platelet count and ICG retention rate at 15 min (ICG-R15) were significantly correlated with the undernutrition grade, as well (Fig. 2). Although there was no significant difference in the extent of hepatectomy (p = 0.144) and operation time (p = 0.801) among the groups, estimated blood loss (p = 0.019) and transfusion rate (p < 0.001) linearly increased as the nutritional status got poorer.
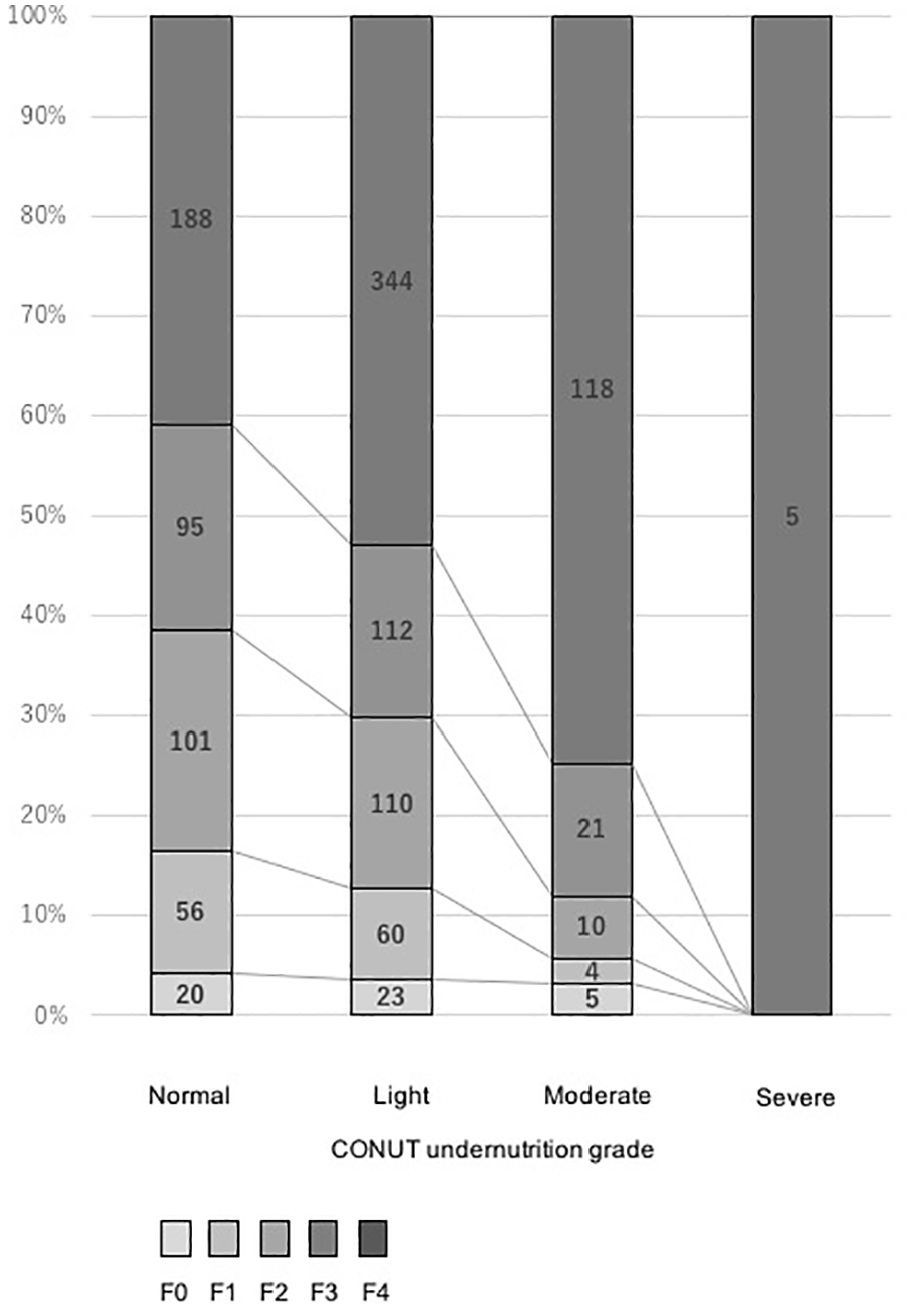
Correlation between the increased CONUT undernutrition grade and fibrotic status (F) of underlying liver (F0: no fibrosis, F1: fibrous portal expansion, F2: few bridges or septa, F3: numerous bridges or septa, F4: cirrhosis).
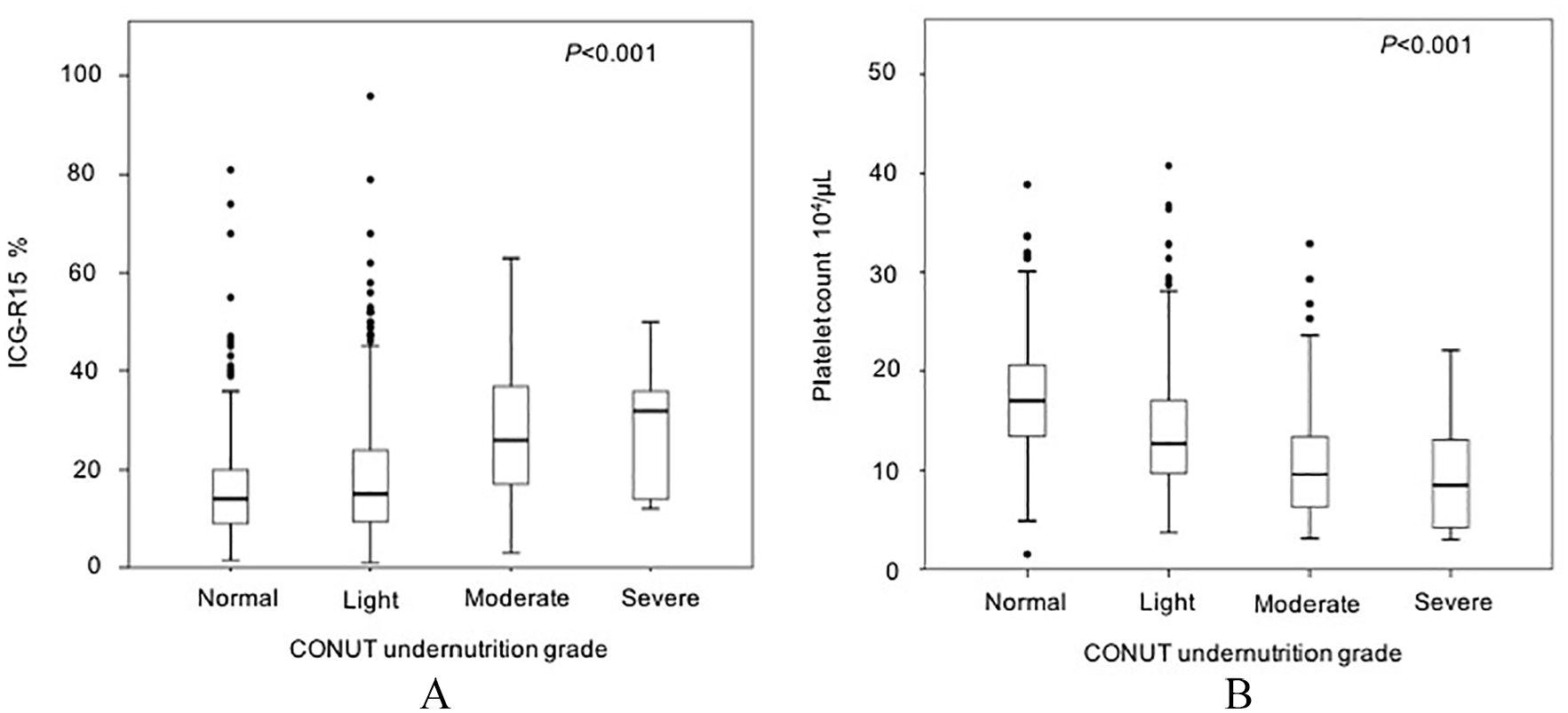
(A) Correlation between the increased CONUT undernutrition grade and increased indocyanine green retention rate at 15 min (ICG-R15). (B) Correlation between the increased CONUT undernutrition grade and decrease in platelet count.
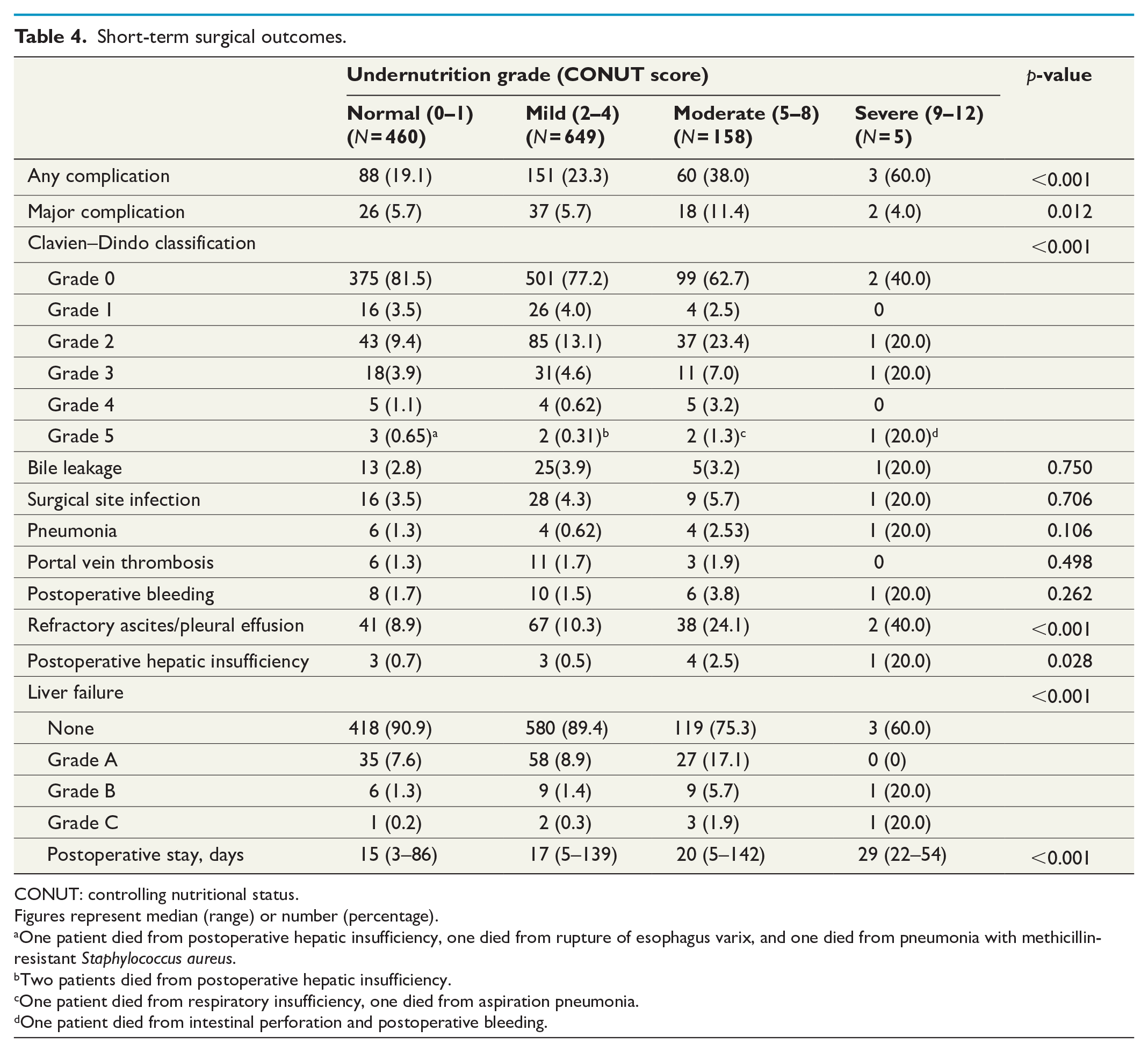
The incidence of postoperative morbidities and length of postoperative stay were significantly correlated with the undernutrition grade (Table 4). Particularly, refractory ascites/pleural effusion (p < 0.001), postoperative hepatic insufficiency (p = 0.028), and higher grade of liver failure (p < 0.001) were significantly frequent in patients with severe nutritional status.
Short-term surgical outcomes.
CONUT: controlling nutritional status.
Figures represent median (range) or number (percentage).
One patient died from postoperative hepatic insufficiency, one died from rupture of esophagus varix, and one died from pneumonia with methicillin-resistant Staphylococcus aureus.
Two patients died from postoperative hepatic insufficiency.
One patient died from respiratory insufficiency, one died from aspiration pneumonia.
One patient died from intestinal perforation and postoperative bleeding.
Significance of the CONUT undernutrition grade according to the status of underlying liver
When stratifying the population based on the underlying liver status (cirrhosis, n = 655 versus non-cirrhosis, n = 617), tendency toward increased incidence of any and major morbidities in poorer nutritional status was also confirmed in both non-cirrhotic patients (normal, 16.2% and 5.2%; light, 22.6% and 6.9%; moderate, 22.5% and 7.5%; p = 0.179 and p = 0.148, respectively) and cirrhotic patients (normal, 23.4% and 6.4%; light, 23.8% and 4.7%; moderate, 43.2% and 12.7%; severe, 60.0% and 40.0%; p < 0.001 and p = 0.007, respectively) (Supplemental Fig. 1a). Median length of hospital stay was linearly correlated with the undernutrition grade, regardless of the underlying liver status, as well: normal, 14 days; light, 16 days; moderate 18 days (p < 0.001) for non-cirrhotic patients and normal, 17 days; light, 18 days; moderate, 22 days; severe, 29 days (p < 0.001) for cirrhotic patients, respectively (Supplemental Fig. 1b).
The tendency toward the increased risk of surgery in poorer nutritional status was much more evident in cirrhotic patients and multivariate analysis for the subgroup of patients with cirrhosis confirmed that the CONUT score is an independent predictor for both any morbidity (OR, 1.17 per +1 point; 95% CI: 1.05–1.29; p = 0.004) and major morbidity (OR, 1.20 per +1 point; 95% CI: 1.03–1.40; p = 0.020) (Supplemental Table 3).
Discussion
This study compares the performance of reported nutritional/inflammatory scores for estimating surgical risk of patients undergoing hepatectomy for HCC. ROC analysis revealed that the CONUT score shows relatively high performance compared to the other reported scores, and multivariate analysis confirmed that the CONUT score is independently correlated with both any and major postoperative morbidities. The CONUT undernutrition grade was strongly correlated with the fibrotic status of the underlying livers. Platelet count and ICG-R15 were linearly correlated with the undernutrition grade, as well. Incidences of postoperative morbidities and length of hospital stay were significantly correlated with the CONUT undernutrition grade, regardless of the fibrotic status of the underlying livers, while the difference was more evident in cirrhotic patients.
Liver resection is a mainstay for radical treatment of solitary or small HCC.21,22 Since the complexity of surgery and the severity of liver cirrhosis are well-known risk factors for mortality and morbidity in hepatectomy for HCC, various studies have been conducted to establish a new evaluation method of surgical indications.5,9,23,24 Makuuchi’s criteria, 9 widely used in Japan, focused on the value of ICG-R15 as an effective predictor of the safety limit of the extent hepatectomy among patients with HCC. 25 With recent development of a high-quality three-dimensional volumetry 26 and portal vein embolization, 27 the conventional criteria have been expanded to safely achieve an appropriate extent of resection for cure. 5 However, one of the big issues in surgical management of HCC worldwide is a regional difference in the quality of preoperative workup regarding the risk estimation for surgery and lack of standardized evaluation method for hepatic functional reserve for such high-risk procedure. Nevertheless, as we presented in this study, nutritional/inflammatory scores actually have close relation with the degree of histopathologic injury in underlying liver and may offer information about the risk of surgery, especially the risk of liver failure after hepatectomy. However, care should be paid in interpretation of the present results considering the minimal number of patients in the severe group classified according to the CONUT score.
As we have shown in Table 2, the performance of nutritional/inflammatory scores for prediction of surgical risk was not so different among the tested nine indices partly because most of the nutritional scores use similar parameters such as albumin or lymphocyte. Indeed, ALBI score is increasingly used as an alternative measure for hepatic functional reserve in the field of hepatology. 4 However, the major practical issue of this score includes its complex calculation using logarithm and arbitrary cut-off points at 25 percentile and 90 percentile for grading, though its performance in prediction of hepatic functional reserve has been validated in various studies.28,29 From a practical standpoint, priority of a grading system should be placed on a simplicity, usability, and reliability of the score as long as similar performance is obtained. Ideally, continuous variables directly reflecting the hepatic functional reserve such as ICG clearance test or 99m Tc-galactosyl serum albumin scintigraphy would be preferable. Given the encouraging results in the present analysis, however, nutritional scores using general laboratory data, including the CONUT score, could be an alternate measure to be used for risk stratification of patients prior to surgery for HCC.
The CONUT score was originally reported as a screening tool for nutritional status. 17
Although previous studies showed that the CONUT score had been associated with long-term outcomes of the patients with HCC, 30 the clinical evidence regarding the CONUT score in preoperative assessment remains insufficient. The CONUT score consists of three parameters: serum albumin level, lymphocyte count, and total cholesterol concentration, which reflect host protein synthesis, immune function, and lipid synthesis, respectively. Given these nutritional/immunological statuses may be closely associated with liver function and susceptibility to infection after high invasive procedures, it is reasonable that the CONUT score presented the best performance for predicting short-term surgical outcomes of patients with HCC among the tested nine indices. Although the malnutritional status evaluated with the CONUT score may partly reflect the degree of injury in underlying livers as confirmed in Fig. 1, multivariate analysis confirmed that the CONUT score is associated with short-term surgical outcomes independent from fibrotic status of the liver. As confirmed in subgroup analysis according to the status of underlying livers, the CONUT score further stratified the risk of postoperative morbidities especially in patients with cirrhosis. It was also important finding that other nutritional scoring systems such as PAL and GPS showed high predictive performance of postoperative morbidity in the present analysis.
The limitations of the current analysis include its single center, retrospective design and inherent selection bias in the study population. Therefore, we need careful interpretation for small number in the “severe” grade. However, the current analysis was performed using a prospectively collected database of patients who were treated under the constant surgical policy in a high-volume center specialized for the treatment of HCC. In addition, it is difficult to evaluate the impact of perioperative nutritional support on surgical outcomes in the present cohort. Future investigation, including a prospective study, would be needed to clarify the impact of perioperative nutritional management as a part of enhanced recovery after surgery. Nevertheless, given the potentially encouraging outcomes that the CONUT score could efficiently predict both the degree of hepatic injury and surgical risks of patients undergoing hepatectomy for HCC, the present results may warrant multicenter study to validate its utility and efficacy in risk stratification of patients with HCC.
In conclusion, the CONUT score could be an alternative preoperative measure for underlying liver injury and surgical risk of patients undergoing hepatectomy for HCC. The present results may warrant future multicenter study to establish a more sophisticated, reliable method for risk stratification and perioperative management of patients with HCC.
Supplemental Material
sj-pdf-1-sjs-10.1177_14574969211061953 – Supplemental material for Preoperative nutritional score predicts underlying liver status and surgical risk of hepatocellular carcinoma
Supplemental material, sj-pdf-1-sjs-10.1177_14574969211061953 for Preoperative nutritional score predicts underlying liver status and surgical risk of hepatocellular carcinoma by Ryosuke Umino, Yuta Kobayashi, Miho Akabane, Kazutaka Kojima, Satoshi Okubo, Masaji Hashimoto and Junichi Shindoh in Scandinavian Journal of Surgery
Footnotes
Author contributions
R.U., Y.K., and J.S. contributed to the study concept and design, and analysis and interpretation of data; J.S. contributed to critical revision and study supervision. All authors contributed to acquisition of data, drafting of the article, and final approval of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from Okinaka Memorial Institute for Medical Disease.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.