
Abstract
Background:
The groin is a complex anatomical area with multiple structures that can be injured and cause pain. One condition with groin pain is the so-called “sports groin,” which can be treated with a groin hernia repair even though no hernia is present. The aim of this study was to assess the prevalence of chronic groin pain several years after a groin hernia repair performed in patients with a sports groin.
Methods:
This nationwide cohort study included adults who had a groin hernia repair for a sports groin through the years 1998–2011. The patients were identified through the Danish Hernia Database and in surgical records. Patients were asked to fill out four questionnaires several years after the repair: a visual analogue scale, the Activity Assessment Scale, the Inguinal Pain Questionnaire, and a questionnaire about treatment satisfaction.
Results:
Of 118 contacted patients, 71 gave informed consent and were included in the study (60%), and of these the response rate was 100%. The questionnaires were filled out median 14 years after surgery. Most of the patients were pain-free in the operated groin (87%), and only a few had physical impairment caused by groin pain (20%). Prior to surgery, 79% had groin pain that they could not ignore. Overall, 90% of the patients were satisfied with the treatment.
Conclusions:
Most patients were pain-free and without physical impairment several years after groin hernia repair for a sports groin and with high satisfaction rate.
Introduction
Long-standing groin pain is frequent, especially among athletes. 1 The anatomical complexity of the groin results in several possible targets for pathologies in a small area that can be the origin of the groin pain. For professional athletes, groin pain can end a sports carrier if treated improperly. One of the conditions that causes groin pain is the so-called sports groin, also called sports hernia. A sports groin is characterized by long-standing pain around the inguinal canal, and the pain is worsened by exercise, abdominal sit-ups, and by Valsalva’s maneuver.2,3 Pain caused by a sports groin is provoked by palpation of the inguinal area, and an inguinal bulge without herniation can also be present. Researchers have suggested different aetiologies, including tears in the transverse fascia, tears in the external oblique aponeurosis, 3 and compression of the genitofemoral nerve. 2 However, the precise pathology of a sports groin remains unclear.
At present, international consensus on how to treat sports groins is lacking. Nevertheless, the more frequent suggestion is to start with conservative treatment, and surgery can be considered if satisfying pain relief has not been achieved within 2−6 months.3,4 Whether conservative or surgical treatment is most efficient in relieving the pain remains insufficiently investigated, but previous studies have shown that groin hernia repair for a sports groin in Denmark is quite common.5,6 Initial conservative treatment followed by surgery can result in long sick leave, especially for athletes, with the associated cost for society and frustration for patients. Furthermore, surgery to treat sports groins needs to be effective in relieving the groin pain to overcome the risk of complications. Previous studies have shown good effect of surgical treatment, that is, groin hernia repair in patients with a sports groin, 7 but data on the long-term effects are lacking. Therefore, it would be of value to find out if groin hernia repairs are efficient in long-term relief of groin pain caused by a sports groin.
The aim of this study was to assess the prevalence of groin pain, degree of physical impairment, and treatment satisfaction several years after a groin hernia repair in patients suffering from a sports groin.
Methods
This nationwide cohort study is reported according to the STrengthening the Reporting of OBservational studies (STROBE) guideline. 8 Patients that have had a groin hernia repair for a sports groin had already been identified in previous studies5,6 and the present study evaluated groin pain several years after the repair by using multiple validated questionnaires.
In previous studies, we established the cohort by identifying adult patients in the Danish Hernia Database who have had a groin hernia repair in a groin with no hernia present from 1 January 1998 to 31 December 2011.5,6 Medical and surgical records of these patients were forwarded from public and private hospitals nationwide to identify patients with a sports groin. Patients were considered to suffer from a sports groin if their medical history included groin pain and if the surgical record described no hernia or other pathology that could explain the groin pain, except for tears in the transverse fascia or in the external oblique aponeurosis. 6 The groins were excluded if it was specified that no pain was present prior to surgery. If pain was not mentioned, we assumed that the patients suffered from groin pain because pain is an indication for groin hernia repair. The patients that were identified as having a sports groin from the previous study 6 were included in this study. None of the included patients had bilateral sports groins, and the outcomes are therefore reported on a patient-level.
Outcomes were assessed by questionnaires, which were a visual analogue scale (VAS) from 0 to 100 mm about pain “right now” when lying and when moving from a lying to a sitting position, use of daily pain-relieving medication due to groin pain, the Activity Assessment Scale (AAS), 9 and the Inguinal Pain Questionnaire (IPQ). 10 Furthermore, the patients were asked how satisfied they were with the treatment on a VAS from 0 to 100 mm, which have previously been recommended for patient satisfaction, 11 and if they would recommend this treatment to a friend (yes or no). We face-validated all questionnaires. The patient answered each question and described how they understood the question. The questionnaire was corrected if needed in-between each patient contact. The questionnaires were formed in the Research Electronic Data Capture (RedCAP) tool and sent to the patients with “E-boks.” E-boks is a safe national mail system where public authorities (including hospitals) can communicate with all citizens in the country. The patients were first contacted on 12 September 2019. Non-responders received up to three reminders with two weeks in-between each contact. Patients without E-boks were excluded. To avoid missing data, we contacted the patients by phone if they had not answered all the questions.
The primary outcome was the prevalence of mild to no groin pain postoperatively measured by the VAS when lying still and when moving from lying to sitting position. No pain to mild pain was defined as a VAS ⩽ 20 mm, 12 and this outcome was therefore handled as categorical data. Also, the median VAS scores when lying and when moving from lying to sitting position were assessed and handled as continuous data. The AAS consists of 13 questions with an ordinal Likert-type scale with five answer possibilities that ranges from “no pain” to “cannot do this activity because of pain” and also with an additional answer possibility: “never performing this activity for other reasons.” The data received from the AAS were handled as categorical data. The outcome based on this questionnaire measured prevalence of “physical impairment.” Physical impairment was defined as a score ⩾ 7.69% calculated as “((the sum of the scores / the minimum possible score sum) / the range of the score) × 100.” 13 Also, the crude rates for each question were assessed. The IPQ consists of 16 questions regarding pain before (one question) and after surgery (15 questions) with categorical answer possibilities. All patients should answer questions 1–3, which focus on pain preoperatively, pain right now, and pain within the last week. Question 4 was only answered by patients who no longer experience pain, and patients should recall when the pain stopped postoperatively. Questions 5–12 were only answered by patients who still experienced pain in the groin. Questions 5 and 6 are about frequency and length of pain periods during the last week, and questions 7–12 are about physical impairment after operation. Question 13 is about use of pain-relieving medication. Question 14 is about the ability to work, and questions 15 and 16 are about pain in the opposite groin. All data on the IPQ were handled as categorical data. Satisfaction was measured both on a VAS from 0 to 100 mm, presented as continuous data, and whether the patients would recommend the treatment to a friend or not, presented as binary categorical data.
For statistical analyses, IBM SPSS statistics version 22.0 (IBM Corp, Armonk, NY) was used. Continuous data were assessed for normal distribution with histograms. Because most of the continuous data were not normally distributed, median and range are presented throughout the article. Categorical data are presented as crude rates with 95% confidence intervals.
The Danish Data Protection Agency approved the study (VD-2018-258). According to Danish law, we did not need ethical approval for this special study design. Informed consent was provided by the patients when responding to the questionnaires.
Results
Through the years 1998–2011, 152 patients with a sports groin having surgery were identified in the previous studies.5,6 Of these, 34 were not signed up to E-boks either because they were dead or because they preferred receiving postal letters. A request to answer the questionnaires was sent to the remaining 118 patients. Of these, 71 patients chose to give consent (60%) and answered 100% of the questionnaires. Sixty of the 71 patients were men (85%). The median age at time of surgery was 41 years (range = 19–76), the median year of surgery was 2005 (range = 1998–2011), and the median time between surgery and answering the questionnaire was 14 years (range = 8–21). Of the 71 patients, 43 had a Lichtenstein repair (60%), 12 had other open repair without insertion of a mesh (17%), 9 had a laparoscopic repair with insertion of a mesh (13%), and 7 repairs were not specified (10%). Due to lack of requirements about which details to add in both the Danish Hernia Database and in surgical records, few repairs (7) were not specified. None of the patients had a re-operation during the follow-up. There was no significant difference between responders and non-responders according to age and time between surgery and receiving the questionnaire.
At the time of answering the questionnaire, 87% of the patients had a VAS-score ⩽ 20 mm when lying, and the median score was 0 mm (range = 0–81). When moving from a lying to a sitting position, 86% had a VAS-score ⩽ 20 mm, and the median score was 0 mm (range = 0–84). Nobody took daily pain-relieving medication.
On the AAS, 80% had a physical impairment score ⩽ 7.69% when answering the questionnaire. For crude rates for the individual questions, see Table 1.
Pain prevalence based on the Activity Assessment Scale 9 when performing different activities.
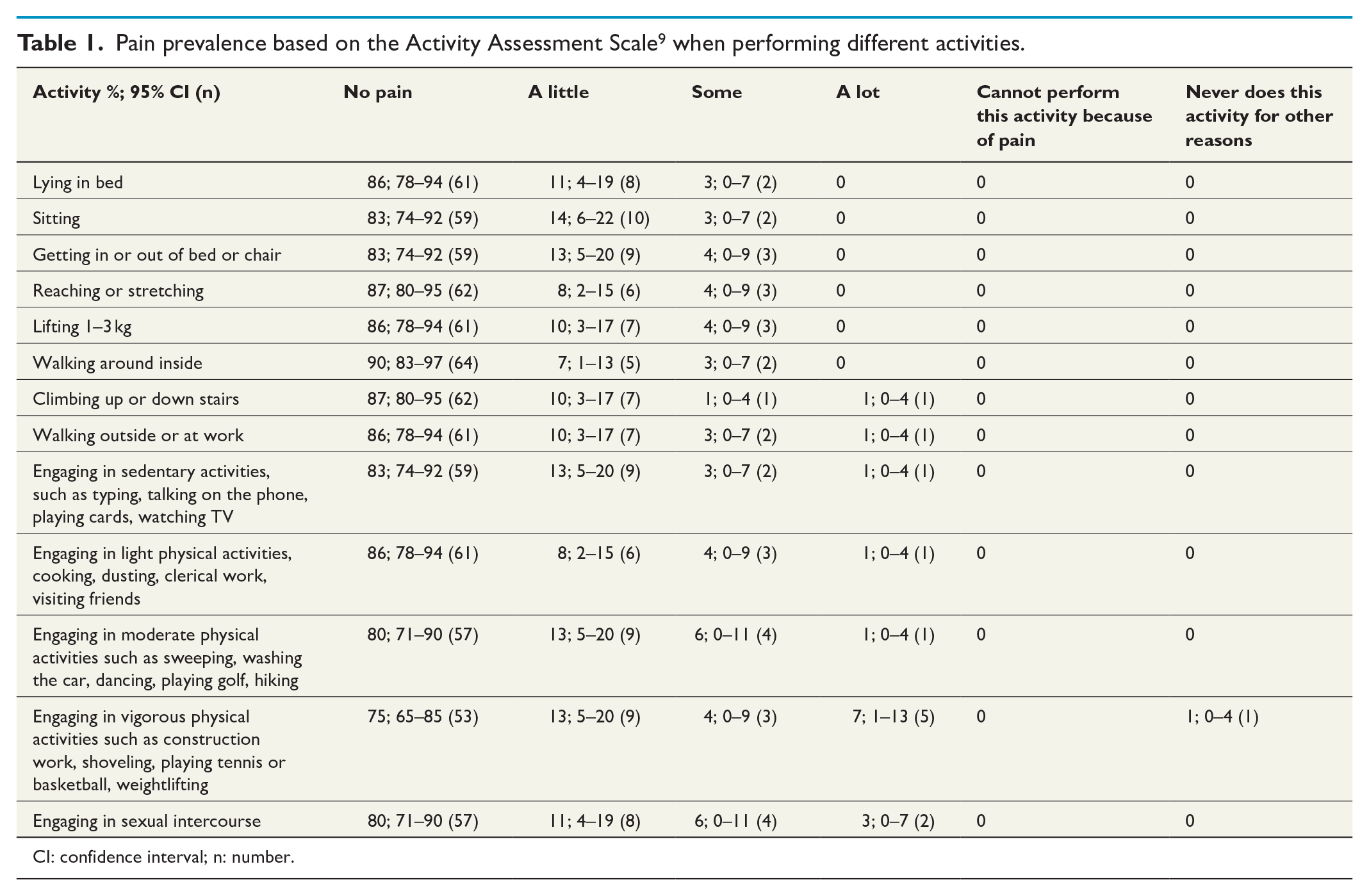
CI: confidence interval; n: number.
On the IPQ, 79% had pain that they could not ignore preoperatively, and 39% had pain that prevented them from performing daily activities. At the time of answering the questionnaire, 72% were pain-free. For pain-scores before and after operation, see Table 2. For those with no pain at the time of answering the questionnaire (51 patients), 67% experienced pain relief within 1 month after the surgery. For those who still had pain in the operated groin at the time of answering the questionnaire (22 patients), 55% felt pain once during the last week, and the pain episodes lasted between one minute and one hour for more than half of the patients (54%). For the impact on daily life, see Fig. 1. In general, the patients did not experience groin pain impacting their daily lives in the operated groin. The area where it did have some impact was during sport activities where nine patients (45%) experienced difficulties because of pain in the operated groin. Of the 22 patients who were not pain-free, three had taken painkillers because of pain in the operated groin during the last week. None of the patients who still had groin pain in the operated groin had been on sick leave from work due to groin pain during the last two months. Regarding “pain right now” and “pain during the last week” in the non-operated groin, 63 reported no pain in the non-operated groin (89%), 6 (8%) and 5 (7%), respectively, reported pain that could easily be ignored, and 2 (3%) and 3 (4%) reported pain that could not be ignored but that did not affect daily activities.
Pain prevalence based on the inguinal pain questionnaire10 preoperatively and at the time of answering the questionnaire.
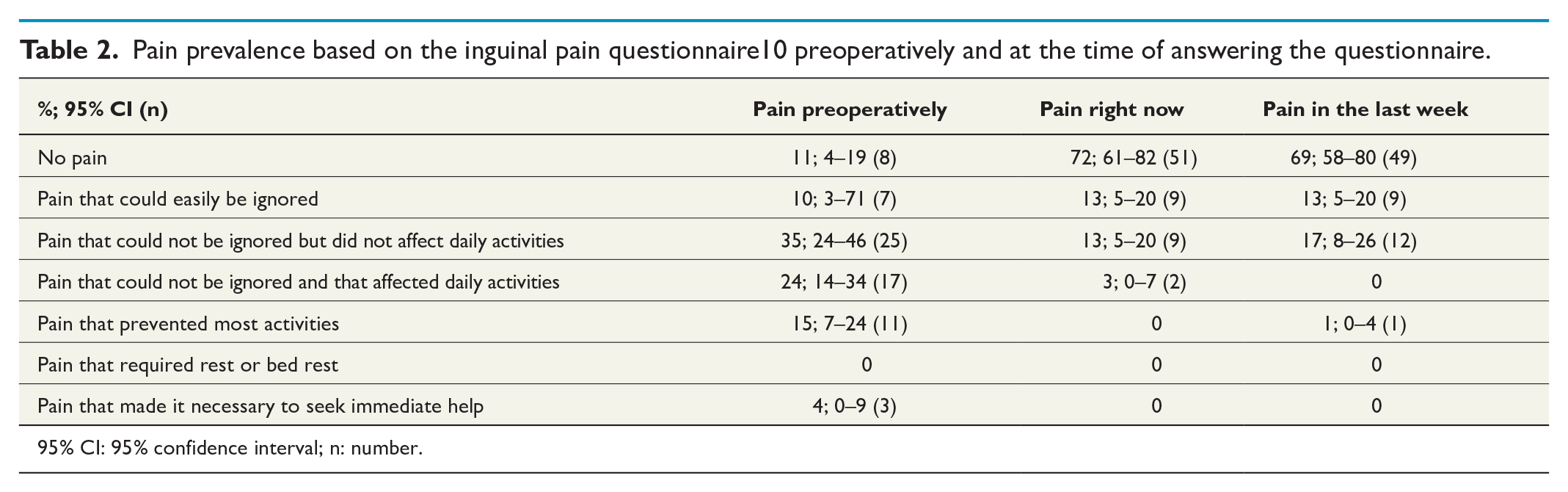
95% CI: 95% confidence interval; n: number.
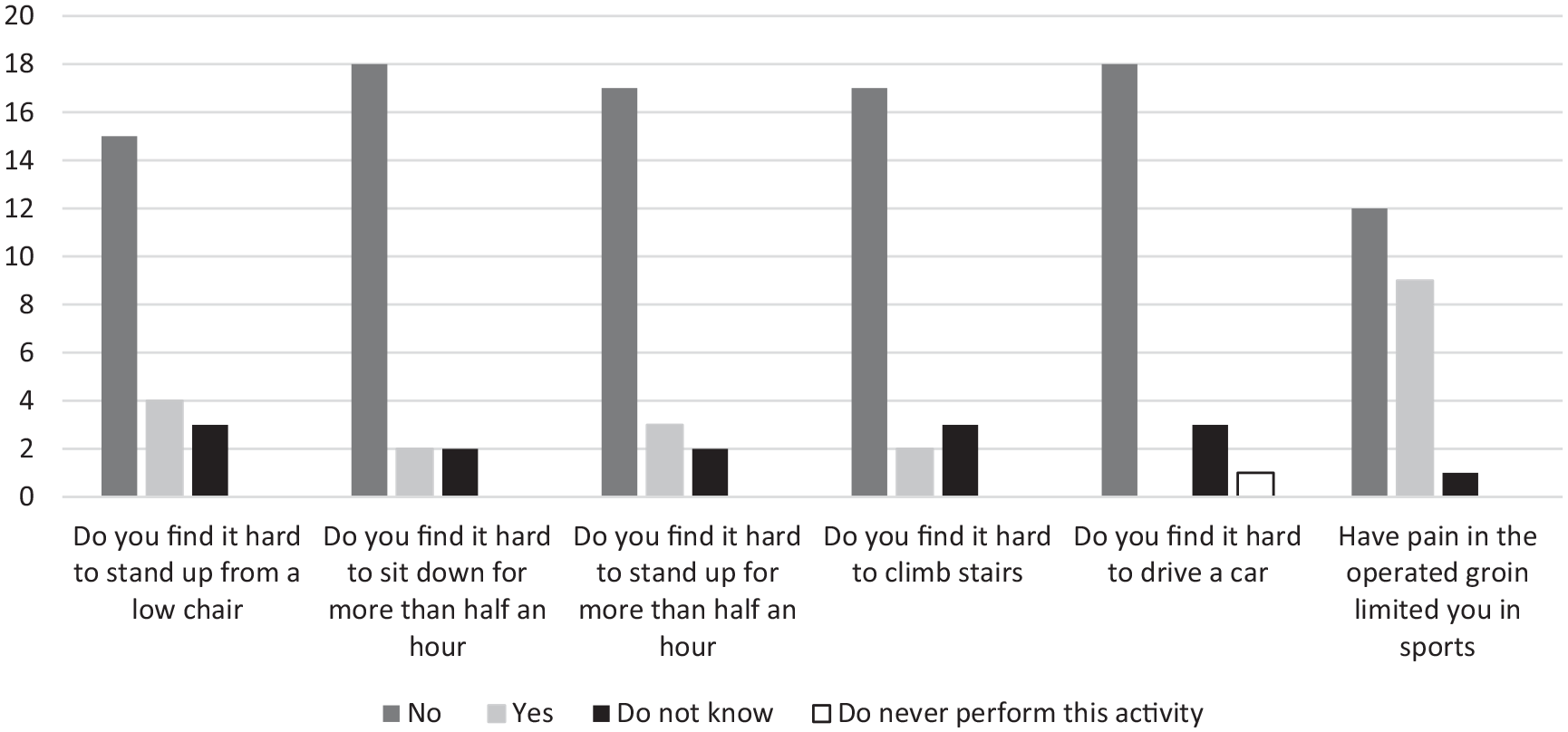
Impact of pain in the operated groin on daily life for the patients who still experienced pain after the operation based on the inguinal pain questionnaire.10 The vertical axis represents number of patients.
The median reported satisfaction was 90 mm (range = 0–100). Of the 71 patients, 53 (75%) would recommend the treatment to a friend.
Discussion
This nationwide cohort study assessed groin pain, physical impairment, and satisfaction with treatment in patients several years after groin hernia repair for a sports groin. Preoperatively, most of the patients had groin pain that they could not ignore. When completing the questionnaire, most of the patients had no pain or mild groin pain, and they had no physical impairment. For patients who were pain-free at the time of answering the questionnaires, most experienced pain relief within 1 month after surgery. Patients who still experienced pain typically only experienced it once during the last week and the pain lasted less than 1 hour. None of the patients reported sick leave for the last 2 months because of groin pain, and an overwhelming part of the patients were satisfied with the treatment.
Several years after operation, 87% of the patients had only mild or no groin pain. This is an important discovery since former studies have found a rapid decline in groin pain after groin hernia repair in groins considered to suffer from a sports groin,14,15 and our results show long-lasting pain relief after surgery. Compared with conservative treatment, surgery has previously been found to relieve the pain faster and more efficiently in a randomized clinical trial and a systematic review including cohort studies and randomized trials.7,14 Considering that one of the risks of having a groin hernia repair is postoperative chronic groin pain,16,17 87% of patients with no or mild pain is a quite positive result. This corresponds to the measured 10%–12% frequency of postoperative chronic groin pain after a groin hernia repair.18,19 It is, therefore, a reasonable assumption, that a groin hernia repair in a groin with a sports groin is a very successful treatment when 87% of patients being long-term pain-free after operation. Thus, it may be argued that there was close to 100% treatment effect, taking the expected finding of chronic pain after the hernia procedure per se into account.
Prior to surgery, 78% had pain that could not be ignored, and 15% were prevented from certain physical activities because of this. Even though there is a high risk of recall bias about the precise degree of pain, it is plausible that most patients had some degree of pain since this typically is a requirement for groin hernia repair. Several years after surgery, 80% did not have substantial physical impairment according to the AAS. A previous randomized clinical trial and a cohort study in patients with sports groin, which mainly included athletes, found that 70%–97% had physical impairment measured as unable to participate in sport prior to surgery, and 84%–97% came back to full sport activity within 12 months postoperatively.14,15 Our study represents the general population and not mainly athletes; therefore, the ability to return to sport would not have been a valuable assessment and we chose not to examine this. We found the satisfaction rate to be 90%, and 75% would recommend the treatment to a friend. This is a high satisfaction rate that stands in line with literature about surgical treatment of a sports groin14,15 and further confirms that the high satisfaction rate is long-lasting.
This study has several strengths. First, the study was based on previously well-described questionnaires, which makes it easier to compare the results with the literature. Second, it was a nationwide study with a variety of patients including patients from different age groups, different levels of daily activity, and different levels of sporting activity, resulting in high external validity. Third, the results include measures of pain, physical impairment, and patient satisfaction, resulting in a broad measure of how successful the treatment has been. Last, we chose questionnaires that mainly focus on pain right now or recent pain instead of preoperative pain or pain in the immediate postoperative period to limit the risk of recall bias as much as possible.
The study also has limitations. First, a 60% response rate is rather low though it is generally accepted that it is the minimum sufficient response rate in cohort studies. 20 Second, asking the patients about preoperative pain and when the pain disappeared many years after the repair has a risk of recall bias. Regardless, we chose to include the retrospective questions included in the IPQ to enable a comparison between pain before and after surgery. Due to the risk of recall bias, we chose not to include questions about how long patients had groin pain before surgery, nor if they tried conservative treatment preoperatively. Third, it would add strength to the study to compare the patients with a group of patients treated conservatively, but since there is no database with conservatively treated patients, this was not possible in the present study design. Fourth, the patients were treated with different types of surgery, and we could not evaluate whether one surgery type was more efficient than another due to the limited number of patients. Fifth, we have no information on why some patients chose not to answer our questionnaires, and we cannot assess whether there is a risk of selection bias, which is a problem in all questionnaire studies with response rates lower than 100%. Finally, the patients were identified in previous studies5,6 based on having had a groin hernia repair in a groin without having a groin hernia, on findings during preoperative physical examination, and on findings during surgery. Since the amount of information included in the medical and surgical records varied, not all patients were well-described, and this may include a risk of misclassification.
The assumption that the pain from a sports groin in some patients is caused by a weak posterior inguinal wall that allows a bulge to compress the genitofemoral nerve2,15 could explain why a groin hernia repair relieves the pain even though no hernia is present. Taking our results into consideration, we believe that patients with long-standing groin pain who does not respond to 4–6 months of conservative treatment, including rest from sport, physiotherapy, and possibly non-steroidal anti-inflammatory drugs, should be offered a groin hernia repair. However, when looking at systematic reviews on the subject, it is clear that randomized controlled trials that compare surgery and conservative treatment are lacking. 7
In conclusion, an overwhelming part of the patients was still pain-free several years after groin hernia repair for a sports groin, and most patients were satisfied with the treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.