
Abstract
Introduction:
Despite improvements in the perioperative care during the last decades for oncologic colon resection, there is still a substantial risk for postoperative complications and mortality. Opportunities exist for improvement in preoperative risk stratification in this patient population. We hypothesize that the Revised Cardiac Risk Index, a user-friendly tool, could better identify patients with high postoperative mortality risks.
Methods:
A retrospective analysis of operated patients between the years 2007 and 2017 was undertaken, using the prospectively recorded Swedish Colorectal Cancer Registry, which has a 99.5% national coverage for all cases of colon cancer. Patients were cross-referenced with the Swedish National Board of Health and Welfare dataset, a government registry of mortality and comorbidity data. Revised Cardiac Risk Index (RCRI) scores were calculated for each patient and stratified into four groups (RCRI 1, 2, 3, ⩾ 4). A Poisson regression model with robust standard errors of variance was employed to correlate the 90-day postoperative survival with each level of the Revised Cardiac Risk Index.
Results:
A total of 24,198 patients met the study inclusion criteria. 90-day postoperative mortality increased from 2.4% in patients with RCRI 1 to 10.1% in patients with RCRI ⩾ 4 (p < 0.001). Adjusted 90-day postoperative mortality increased linearly with an increasing RCRI, where an RCRI of 2, 3, and ≥ 4 respectively led to a 46%, 80%, and 167% increased risk of mortality compared to RCRI 1 (p < 0.001).
Conclusions:
A strong association between an increasing Revised Cardiac Risk Index score and increased 90-day postoperative mortality risk was detected. The Revised Cardiac Risk Index may facilitate risk stratification of patients undergoing elective colon cancer surgery.
Introduction
Although the introduction of several perioperative protocols, including Enhanced Recovery After Surgery (ERAS), has improved surgical outcomes in the western world, complication rates following surgery for colorectal cancer remain high1, 2. Studies estimate that complication rates lie between 24% and 35%3, 4. Pre-existing cardiovascular, respiratory, metabolic, renal, and cerebrovascular comorbidities may be implicated in many postoperative complications, ultimately affecting the overall outcome5–9. Preoperative risk mitigation, vital to optimal surgical care, is possible only when the risk is identified. Risk stratification tools, such as the P-POSSUM score and the Charlson Comorbidity Index (CCI), ascribe surgical candidates a composite risk score but require many variables, which might limit their practical utility in a time-limited clinical context10, 11.
The Revised Cardiac Risk Index (RCRI) tool requires just six variables (a high-risk type of surgery, ischaemic heart disease, congestive heart failure, cerebrovascular disease, diabetes requiring insulin, and preoperative serum creatinine > 2 mg/dL). It can, therefore, be used easily at the point of care 12 . The RCRI estimates the risk of major postoperative cardiac complications for the patient undergoing noncardiac surgery. The tool was validated using a basket of noncardiac surgical procedures, confirming a positive correlation between increasing RCRI and increased incidence of adverse outcomes12,13. Although the RCRI was originally developed for prediction of major cardiac complications, it has subsequently been extensively researched and its application has been expanded from adverse cardiac events to all-cause mortality 13 .
Applying this tool to risk stratification prior to planned colorectal cancer surgery has not been described in the literature. Perioperative risk-mitigation strategies, guided by tools like the RCRI, may improve patient outcomes by better resource allocation and individualized perioperative monitoring or rehabilitation. Therefore, we aim to investigate the association between the RCRI and mortality following elective colon cancer surgery.
Methods
Data Collection
The principles of the Declaration of Helsinki 14 and STROBE guidelines were complied with while conducting this study (Supplementary Table). The sample population was obtained from the Swedish Colorectal Cancer Registry (SCRCR) 15 . Starting on 1 January 2007 and ending on 31 December 2017, all adult patients who underwent elective resection surgery for colon cancer were retrieved. Ethical approval was obtained from The Swedish Ethical Review Authority (reference number 2020-05643).
The SCRCR was used to determine hospital admission date, age, sex, cancer stage, cancer location, American Society of Anesthesiologist (ASA) classification, neoadjuvant therapy, type of surgery and operative method, date of surgery, and hospital discharge date. The SCRCR database was cross-referenced with the registries maintained by the Swedish National Board of Health and Welfare using the patients’ social security numbers: the National Patient Registry was used to collect information about patient comorbidities and the Cause of Death registry was used to acquire data for the time of death. Comorbidity data were used to calculate both the RCRI and the Charlson Comorbidity Index11,12. Diagnoses, using International Classification Codes (ICD), prior to date of admission were used to reflect each patient’s comorbidity data.
Calculating the RCRI
The presence of high-risk surgery, ischaemic heart disease, congestive heart failure, cerebrovascular disease, renal insufficiency, and diabetes mellitus was used to calculate the RCRI, with each variable counting as one point, if present. In the original RCRI proposed by Lee et al. 12 , preoperative treatment with insulin for diabetic patients and a preoperative serum creatinine > 2 mg/dL would have been used rather than the presence of diabetes mellitus and renal insufficiency. These modified factors were proposed and tested by Lindenauer et al. 16 and have been used frequently in published studies and guidelines (Table 1). All patients received at least one point on the RCRI since, according to the original article by Goldman et al. 17 , intraperitoneal surgery is considered high-risk surgery.
Parameters used in the RCRI according to the modified RCRI.
Source: From Lindenauer et al. 16 .
Statistical Analysis
Patients were divided into four cohorts: RCRI 1, 2, 3, and ⩾ 4 12 . Clinical characteristics were summarized and compared between these cohorts. Normally distributed continuous variables were presented with a mean ± standard deviation (SD), while non-normally distributed variables were presented using median and interquartile range (IQR). Categorical variables were reported as counts and percentages. To determine the statistical significance of differences between continuous variables, an analysis of variance was performed if the data were normally distributed. Otherwise, a Kruskal–Wallis H test was used. Pearson’s chi-square test or Fisher’s exact test were used to determine the statistical significance of differences between categorical variables. The primary outcome of interest was 90-day postoperative mortality.
A Poisson regression model with robust error of variance was undertaken to determine the association between the RCRI and 90-day postoperative mortality. The analysis was performed while adjusting for age, sex, neoadjuvant therapy, cancer stage, type of surgery, operative method, and comorbidities not included in the RCRI. Results are presented as incidence rate ratios (IRRs) with 95% confidence intervals (CIs).
Statistical significance was defined as a two-sided p-value of < 0.05. Analyses were performed using the statistical programming language R (R Foundation for Statistical Computing, Vienna, Austria) 18 .
Results
Twenty-four thousand one hundred and ninety-eight patients met the study inclusion criteria. Patients with a higher RCRI score tended to be older (RCRI ⩾ 4: 77 ± 7 years vs RCRI 1: 71 ± 12 years, p < 0.001), predominantly male (RCRI ⩾ 4: 68.2% male vs RCRI 1: 45.6% male, p < 0.001), less fit for surgery by comparing the proportion of patients with an ASA score ⩾ 3 (RCRI ⩾ 4: 88.4% vs RCRI 1: 20.1%, p < 0.001), and have more comorbidities (RCRI ⩾ 4, CCI ⩾ 7: 98.3% vs RCRI 1, CCI ⩾ 7: 9.0%, p < 0.001). Neoadjuvant therapy was mostly used in patients with lower RCRI scores (RCRI ⩾ 4: 0.4% vs RCRI 1: 2.0%, p < 0.001). Stage 2 cancer was the most common in all cohorts but increased in prevalence with a higher RCRI score (RCRI ⩾ 4: 43.6% vs RCRI 1: 37.3%, p < 0.001). Stage 1 cancer also increased in prevalence with higher RCRI scores while stage 3 and 4 decreased. Right- and left-sided hemicolectomies and sigmoid resections were the most common type of surgery in all cohorts. Open surgery tended to be preferred to laparoscopic surgery in all groups (Table 2). Every registered comorbidity increased in prevalence with higher RCRI scores (Table 3).
Patient demographics and clinical characteristics stratified by RCRI score.
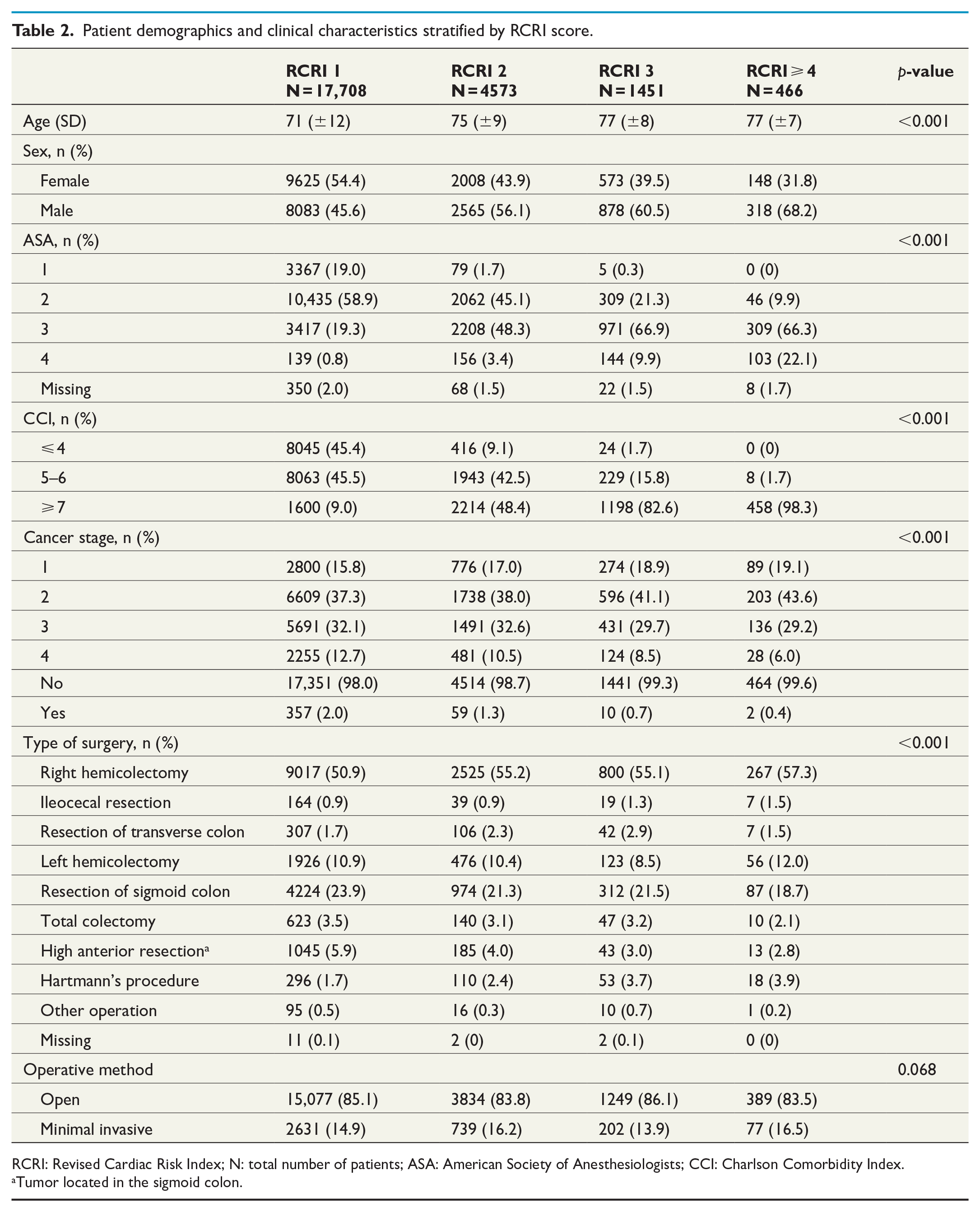
RCRI: Revised Cardiac Risk Index; N: total number of patients; ASA: American Society of Anesthesiologists; CCI: Charlson Comorbidity Index.
Tumor located in the sigmoid colon.
Comorbidities stratified by RCRI score.
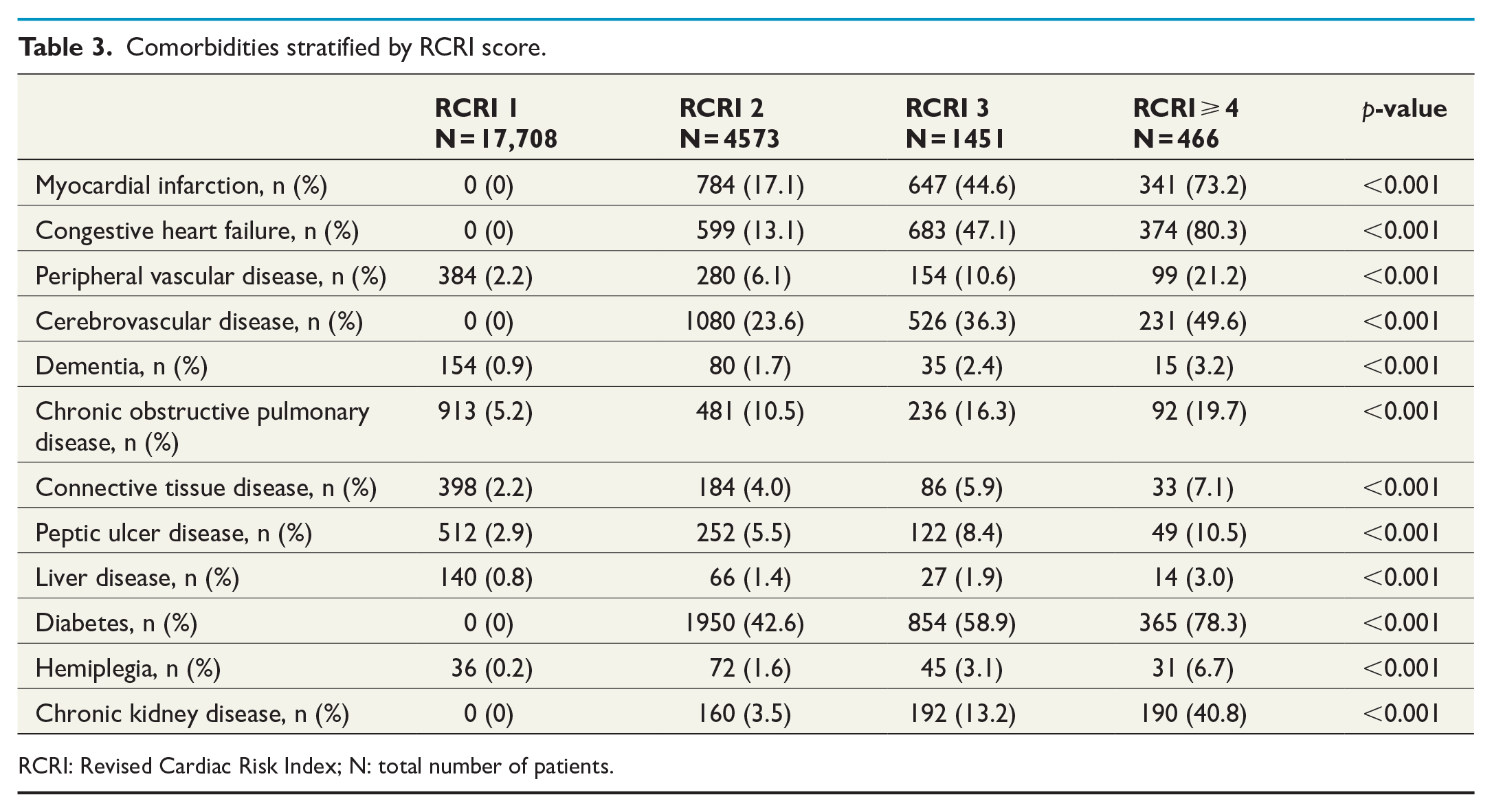
RCRI: Revised Cardiac Risk Index; N: total number of patients.
Crude 90-day postoperative mortality was significantly higher at RCRI ⩾ 4 compared to RCRI 1 (RCRI ⩾ 4: 10.1% vs RCRI 1: 2.4%, p < 0.001; Table 4). When adjusting for relevant covariates, RCRI 2 had a 46% increased incidence of 90-day postoperative mortality compared to RCRI 1 (adjusted IRR (95% CI): 1.46 (1.20–1.77), p < 0.001), RCRI 3 had an 80% increased incidence (adjusted IRR (95% CI): 1.80 (1.38–2.35), p < 0.001) and RCRI ⩾ 4 had an 167% increased incidence of postoperative mortality (adjusted IRR (95% CI): 2.67 (1.87–3.81), p < 0.001; Table 5).
Crude outcomes stratified by RCRI score.
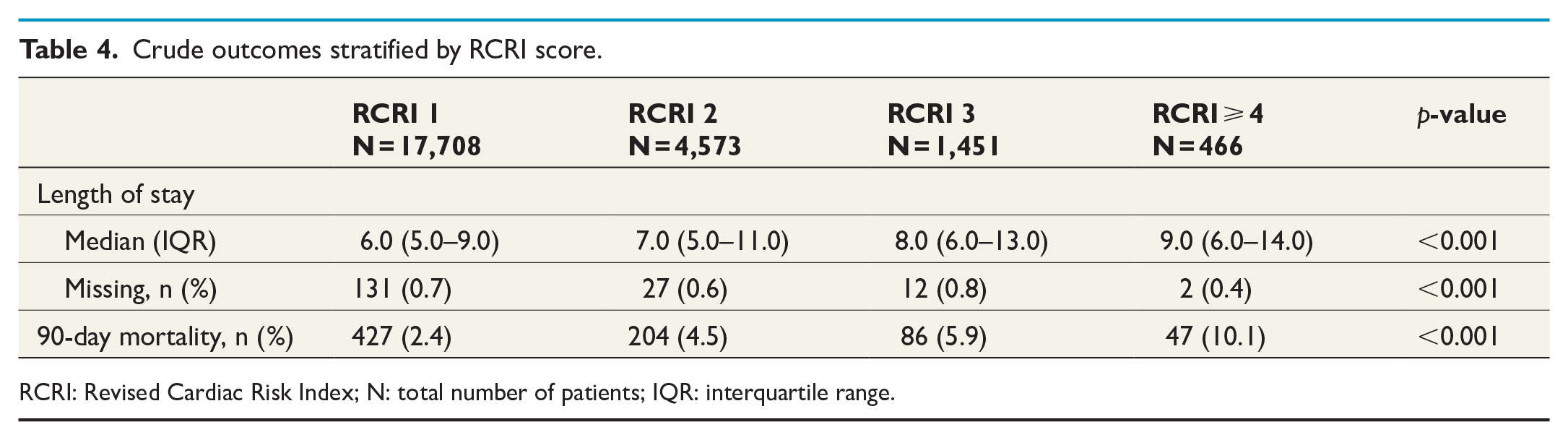
RCRI: Revised Cardiac Risk Index; N: total number of patients; IQR: interquartile range.
Incidence rate ratio for 90-day mortality after elective colon cancer surgery.
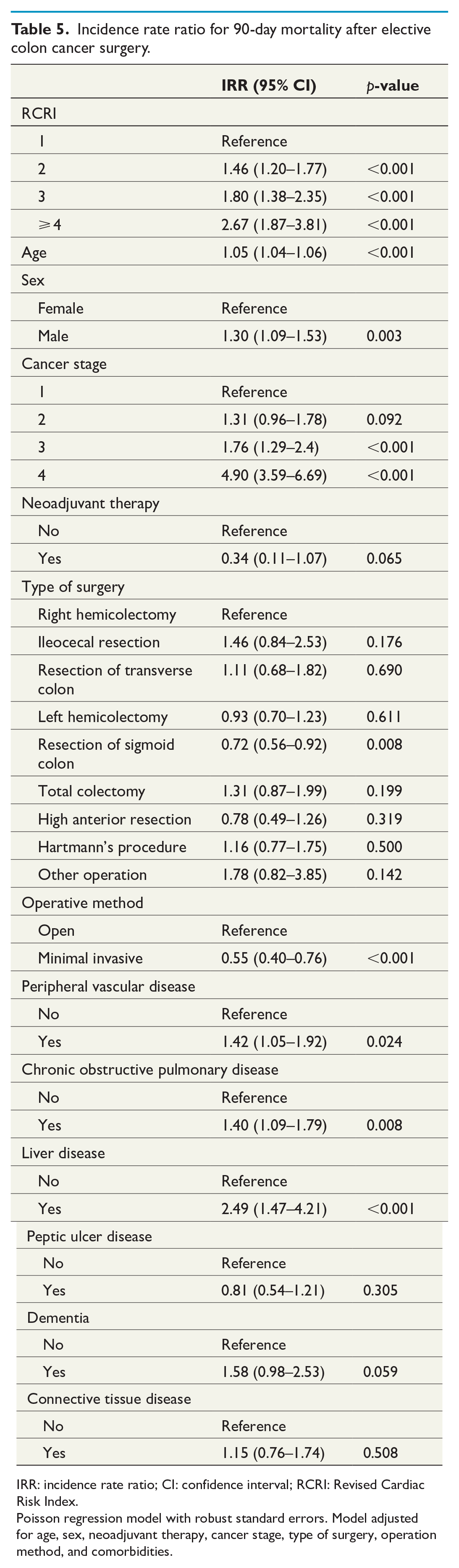
IRR: incidence rate ratio; CI: confidence interval; RCRI: Revised Cardiac Risk Index.
Poisson regression model with robust standard errors. Model adjusted for age, sex, neoadjuvant therapy, cancer stage, type of surgery, operation method, and comorbidities.
Discussion
Our outlined results show a strong association between an increasing RCRI and mortality. 90-day postoperative mortality increased from 2.4% in patients with the lowest cardiac risk to 10.1% in patients with an RCRI ⩾ 4. The association between the RCRI and postoperative mortality was strengthened following our Poisson regression analysis. The applicability of the RCRI in the context of noncardiac surgery has previously been validated; however, this is the first study to date that investigates the tool’s use explicitly in patients subjected to elective oncologic colon resections.
The RCRI was first published by Lee et al. 12 in 1999. Lee et al. 12 outlined the superior diagnostic performance of the RCRI, compared to other tools including ASA class and the original cardiac risk index with an area under the receiver operating characteristic (ROC) curve of 0.777 ± 0.023, for the prediction of major cardiac complications. More recently, the RCRI has been used not only to assess the likelihood of postoperative cardiac complications but also the risk of cardiac death and all-cause mortality; and several previous studies have assessed its external validity in noncardiac surgery 13 . The bulk of existing literature, however, has pooled noncardiac surgical specialties and procedures together in their analyses without investigating whether the RCRI may be more or less appropriate for some types of noncardiac surgery. The need for more specialty-specific studies is demonstrated by Ford et al. 13 , whose meta-analysis was limited by available subgroup analyses. This is of relevance since the RCRI has shown low predictive value in the context of vascular surgery 13 .
Why is risk prediction important? Myocardial injury following noncardiac surgery contributes substantially to postoperative mortality. It has demonstrated significant associative links with 30-day surgical outcomes 6 . Patients with pre-existing ischaemic heart conditions are at particular risk of cardiovascular complications and death. Not unexpectedly, the incidence of major cardiac events shows a progressive increase as the RCRI increases 19 . A proportional relationship between increasing RCRI and in-hospital mortality after noncardiac surgery was demonstrated by Lindenauer et al. 16 . A review by Devereaux et al. 20 outlined that approximately 4% of patients with some form of cardiac risk or cardiac condition experience a major perioperative cardiac event and that there is a mortality rate of up to 25% in patients suffering a myocardial infarction after noncardiac surgery.
This study shows an overall 90-day mortality rate of 3.16% (n = 764) in patients undergoing elective surgery for colon cancer. Furthermore, the outlined analyses support a strong association between the RCRI and mortality in the context of colon cancer surgery. Our multivariable regression model demonstrates an increased 90-day postoperative mortality risk collinear with increasing RCRI. This demonstrates a strong relationship between an increasing RCRI and the likelihood of death, doubling the risk-increase with every point-increase. As expected, our regression model also strongly associated increasing age, advanced cancer stage, and comorbidities such as liver and pulmonary disease, with fatal outcome. Such results are in line with previous findings and confirm our hypothesis5,7,9.
Although mortality-specific prediction tools exist, there is no universally accepted quick-and-easy instrument allowing surgeons and anaesthetists to make bedside or clinic-based predictive assessments. The importance of applying risk indices like the RCRI or the American College of Surgeons’ National Surgical Quality Improvement Program (NSQIP) surgical risk calculator (SRC) for patients undergoing noncardiac surgery is stressed by The American College of Cardiology and American Heart Association (ACC/AHA) most recent guidelines 21 . There are pros and cons to both indices, and the NSQIP SRC has shown to be superior to the RCRI for vascular surgery 22 . The NSQIP SRC also predicts a broader range of outcomes up to 30 days following surgery. The NSQIP SRC lacks sufficient external validation, however, and its 21-point patient-specific variables render it impractical. Thus, some clinical investigators recommend the RCRI over NSQIP SRC 22 . On the contrary, our results, including all-cause mortality up to 90 days after surgery, suggest that the RCRI might be used for risk predictions beyond the hospital admission. In addition to its external validation and applicability to clinical contexts, the RCRI also offers a straightforward method of communicating overall risk to patients, enabling patient involvement and shared decision-making.
Several factors limit our study. Although validated, the SCRCR has inherent registry limitations relating to preoperative medical treatment for comorbidities, instigated preoperative optimization, and postoperative complications. Therefore, the results should be interpreted cautiously, pending future research. Furthermore, the interpretation of the data should be limited to elective resection surgery for colon cancer only. This study excludes all emergency cases, and our findings may not be regarded as transferrable to emergent colon surgery. While the results indicate a strong correlation between increasing RCRI and the risk of 90-day mortality, the authors are unable to conclude anything about the strength of the predictive power of the RCRI in the context of all-cause mortality following colon cancer surgery.
Conclusion
The RCRI is an easy and rapid predictive tool for risk stratification of patients undergoing elective colon cancer surgery. Our results outline a plausible association between increasing cardiac risk and 90-day postoperative mortality. Therefore, we believe that the RCRI should be considered routinely in this patient group’s preoperative assessment. Patients with an elevated RCRI should be treated as high-risk patients and would most likely benefit from preoperative cardiac assessment and prehabilitation as well as closer postoperative attention. The authors encourage future studies investigating whether such an approach may lead to improved survival in this surgical area.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969211037588 – Supplemental material for The Association Between Revised Cardiac Risk Index and Postoperative Mortality Following Elective Colon Cancer Surgery: A Retrospective Nationwide Cohort Study
Supplemental material, sj-docx-1-sjs-10.1177_14574969211037588 for The Association Between Revised Cardiac Risk Index and Postoperative Mortality Following Elective Colon Cancer Surgery: A Retrospective Nationwide Cohort Study by Rebecka Ahl Hulme, Maximilian Peter Forssten, Arvid Pourlotfi, Yang Cao, Gary Alan Bass, Peter Matthiessen and Shahin Mohseni in Scandinavian Journal of Surgery
Footnotes
Author Contributions
Study design by S.M., R.A.H., and P.M.; data collection by S.M., R.A.H., A.P., G.A.B., and P.M.; analysis and interpretation of data by S.M., R.A.H., M.P.F., and Y.C.; and article drafted by S.M., R.A.H., and G.A.B. All authors have critically reviewed and accepted the submitted version of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from The Swedish Ethical Review Authority (reference number 2020-05643). The principles of the Declaration of Helsinki and Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were complied with while conducting this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.