
Abstract
Background and objective:
Preoperative localization of pathologic parathyroid glands is essential in the preparation of a parathyroidectomy. We evaluated the use of a C-11 methionine positron emission tomography/computed tomography scan in a 7-year period in selected patients with primary hyperparathyroidism. The indications to perform a C-11 methionine positron emission tomography/computed tomography were either persistent primary hyperparathyroidism after parathyroidectomy or inconclusive preoperative localization on ultrasound and sestaMIBI.
Methods:
A group of 36 patients was referred for a C-11 methionine positron emission tomography/computed tomography. Biochemical data, pathology, and results of sestaMIBI were collected retrospectively. The primary hyperparathyroidism patients were divided into two groups. In group 1 (N = 17), the C-11 methionine positron emission tomography/computed tomography was performed before parathyroidectomy. In group 2 (N = 19), the C-11 methionine positron emission tomography/computed tomography was performed after unsuccessful parathyroidectomy and before a reoperation.
Results:
Overall, in 30 of the 36 patients (83%), C-11 methionine positron emission tomography/computed tomography identified a true-positive pathologic parathyroid gland confirmed by an experienced pathologist, consistent with a positive predictive value of 91%. In group 1, 94% of the patients (N = 16) had pathologic parathyroid tissue identified by C-11 methionine positron emission tomography/computed tomography. This resulted in a clinical benefit in 13 patients (76%). In group 2, the benefit was slightly lower, as 74% of the patients (N = 14) had a true-positive C-11 methionine positron emission tomography/computed tomography scan resulting in a clinical benefit in nine patients (47%).
Conclusions:
In two selected groups of patients planned for an initial operation or reoperation of primary hyperparathyroidism and inconclusive conventional imaging, we found C-11 methionine positron emission tomography/computed tomography to give parathyroid surgeons a clinical benefit in the majority of cases, electing the patients for unilateral surgery.
Introduction
Primary hyperparathyroidism (PHPT) is diagnosed with increasing frequency worldwide, and parathyroidectomy (PTX) with resection of the pathologic parathyroid gland(s) is also performed more frequently in Denmark. 1 PTX is generally a procedure with a high rate of success and low morbidity.
Preoperative localization is essential to minimize the time and extent of parathyroid surgery. Hence, the unilateral approach is now more common than a bilateral exploration, showing good results. 2 Occasionally, there is no clear focus localized on ultrasound or Tc99m sestaMIBI scintigraphy (sestaMIBI). For this subgroup of patients, there are other imaging modalities available. Positron emission tomography (PET) in general offers a better spatial resolution compared to a parathyroid scintigraphy using single-photon emission computed tomography (SPECT), which is especially important for finding the small adenomas/hyperplastic glands. Multiple PET studies have shown a high variable sensitivity using different C-11 and F-18 tracers, such as C-11 methionine, F-18 fluorodeoxyglucose (FDG), F-18 fluorodopa (FDOPA), and F-18 fluorocholine. 3 However, to our knowledge, only a few studies have been using C-11 methionine positron emission tomography/computed tomography scan (MET-PET/CT) in addition to a primary inconclusive sestaMIBI,4–6 but the studies have limitations. Common limitations are variations in the previous scintigraphy, large variation in biochemical severity of PHPT, and lack of histological verification of MET-PET/CT findings.
At our institution, we have used MET-PET/CT for a decade in selected patients with PHPT with a good clinical outcome. The indications to perform MET-PET/CT were either persistent PHPT after unsuccessful PTX or lack of localization on ultrasound and sestaMIBI scintigraphy prior to surgery. In both cases, the MET-PET/CT was performed prior to operation to improve the rate of surgical success. In this study, we evaluated whether the current clinical use of MET-PET/CT is of advantage in a patient group with PHPT. To our knowledge, no other study has shown consistent data using MET-PET/CT in this group of patients after lack of localization on ultrasound and sestaMIBI scintigraphy, and the imaging results were confirmed by histology in all the included patients.
Methods
Patients and definitions
We performed PTX in a subgroup 41 PHPT patients during a period of 7 years, from January 2010 to February 2017 at Aarhus University Hospital. The group of patients all had a MET-PET/CT before initial surgery or reoperation based on an inconclusive sestaMIBI scintigraphy or unsuccessful primary operation. There were no patients with an MET-PET/CT, who were not selected for surgery.
To avoid multiple scans from the same patients, we excluded any later MET-PET/CT (N = 5), ending up with a total of 36 scans. We divided the patients into two groups: group 1 included patients with an MET-PET/CT prior to any neck surgery (N = 17) and group 2 consisting of patients with an MET-PET/CT before reoperation after a former unsuccessful PTX (N = 19).
From the study cohort, we collected information including biochemistry, pathology reports, operation records, and information from the outpatient clinic. Postoperatively, all patients were recommended daily supplementation with calcium and vitamin D based on national guidelines according to age and gender.
For all patients, we collected biochemical data for more than 6 months postoperatively. Patients with elevated plasma ionized calcium (Ca2+ > 1.32 mmol/L) within the first 6 months after surgery were defined as having persistent hyperparathyroidism. Patients having plasma levels of Ca2+ below the lower limit of the reference interval (<1.18 mmol/L) were considered having hypoparathyroidism, if parathyroid hormone (PTH) did not increase in response to hypocalcemia within the first postoperative week. Patients were considered having chronic hypoparathyroidism, if PTH levels remained insufficient to normalize Ca2+ without treatment with active vitamin D 6 months after surgery.
Parathyroid scintigraphy
We used a single-phase, dual-isotope subtraction technique imaging protocol using a low-energy high-resolution (LEHR) parallel collimator (SIEMENS Symbia T16 dual-head gamma camera with a 16-slice CT). Patients were placed in a supine position with the head placed in a customized device and was scanned from the neck including all salivary glands down to the level of the inferior margin of the heart as for the PET scan. Initially, a thyroid scintigraphy was obtained by planar technique in an anterior projection (20 min, 256 × 256 matrix), 15 min after intravenous injection of 100 MBq of Tc-99m pertechnetate. Immediately after, the patient had an intravenous injection of 950 MBq of Tc-99m sestaMIBI and another planar image was obtained with the patient in the same position (15 min, 256 × 256 matrix). Finally, a tomography (SPECT) was performed immediately after recording the planar images (128 × 128 matrix, 32 views, 60 s per view) followed by a low-dose CT scan (Care Dose 4D, 150 mAs, 110 kV, rotation time 0.6 s, pitch 0.8). The latter was for attenuation purposes and anatomical overlay.
C-11 MET-PET
Patients were instructed not to take any food or water for at least 6 h before the scans. Patients were placed in a supine position on the scanner bed, and the head was placed in a customized device (Vac Fix Systems, Odense, Denmark) to minimize movements during the scan (Siemens Biograph 64). The C-11 methionine tracer was produced by standard methods 7 using the Aarhus PET Center’s 16.8 MeV PETtrace cyclotron (GE Medical Systems, Uppsala, Sweden). A minimum of 250-MBq (4.5 MBq/kg) C-11 methionine was injected intravenously 15–20 min before start of the scan. Patients were scanned from the neck including all salivary glands down to the level of the inferior margin of the heart as for the scintigraphy. Emission data were corrected for attenuation based on a low-dose CT (Care Dose 4D, 50 mAs, 120 kV, rotation time 0.5 s, pitch 1.0) and corrected for radioactive decay back to start of the scan. Reconstruction was performed using an iterative algorithm (4 iterations, 21 subsets) (Siemens Medical Systems), applying a Gaussian filter of 3-mm full width at half maximum (FWHM) resulting in three-dimensional images consisting of 336 × 336 voxels of 2.0 × 2.0 × 2.0 mm3 and a central spatial resolution around 5-mm FWHM. The images were corrected to standardized uptake values (SUVs).
Parathyroid adenoma localization
Interpretation of the parathyroid scintigraphy and C-11 MET-PET images was evaluated in a clinical setting and independently by at least one junior and one specialized nuclear medicine physician with experience in the field of nuclear endocrinology. For parathyroid gland localization, we used an in-house, predefined 10-position scale as shown in Fig. 1 in each of the scans. All other findings were specified in text. The report from the parathyroid scintigraphy also included the confidence level of each positive finding and was graded on a scale from 0 to 2. A grading from 0 to 1 was considered an insignificant contribution to the localization of the parathyroid adenoma, grade 0 being no findings and grade 1 being a possible pathologic parathyroid gland on a specific location. Grade 2 was given for a conclusive scan including an extracapsular parathyroid adenoma with a CT correlate, visible on the planar image as well, and placed along the known pathway of descent of the parathyroid glands from their origination. Same grading system was used to evaluate the C-11 MET-PET images.
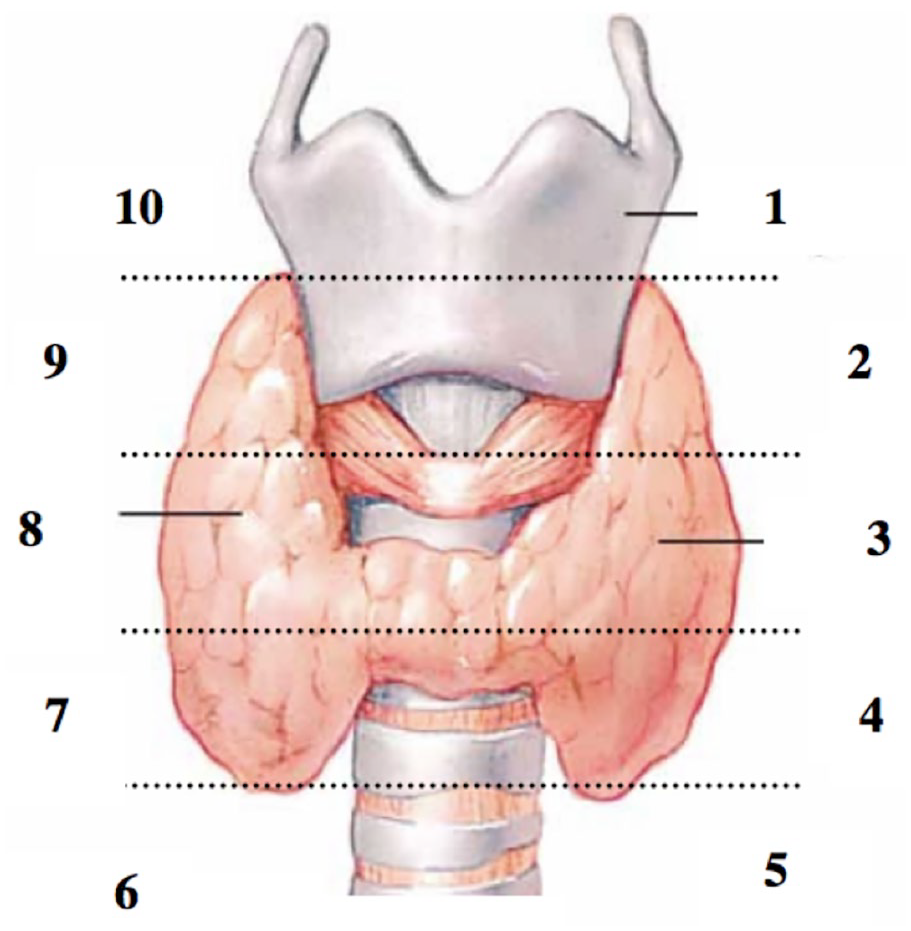
Predefined 10-position scale as indicated above, dividing each thyroid lobe into five parts: 1, above upper pole of the left thyroid lobe; 2, upper third of the left thyroid lobe; 3, middle third of the left thyroid lobe; 4, lower third of the left thyroid lobe; 5, below the lower pole of the left thyroid lobe; 6, below the lower pole of the right thyroid lobe; 7, lower third of the right thyroid lobe; 8, middle third of the right thyroid lobe; 9, upper third of the right thyroid lobe; and 10, above upper pole of the right thyroid lobe. All findings within the thyroid gland (intrathyroid parathyroid gland) and findings with an ectopic position are not included in this numerical system.
A positive result was defined as a pathological parathyroid gland at the position described on MET-PET/CT and/or parathyroid scintigraphy ±1 position (see Fig. 1). Hence, a pathologic uptake at position 4 (posterior to the lower third of the left thyroid lobe) was classified true positive if there was a pathologic gland in position 3, 4, or 5 (from middle third to below the lower pole of the left thyroid lobe) (Fig. 2).
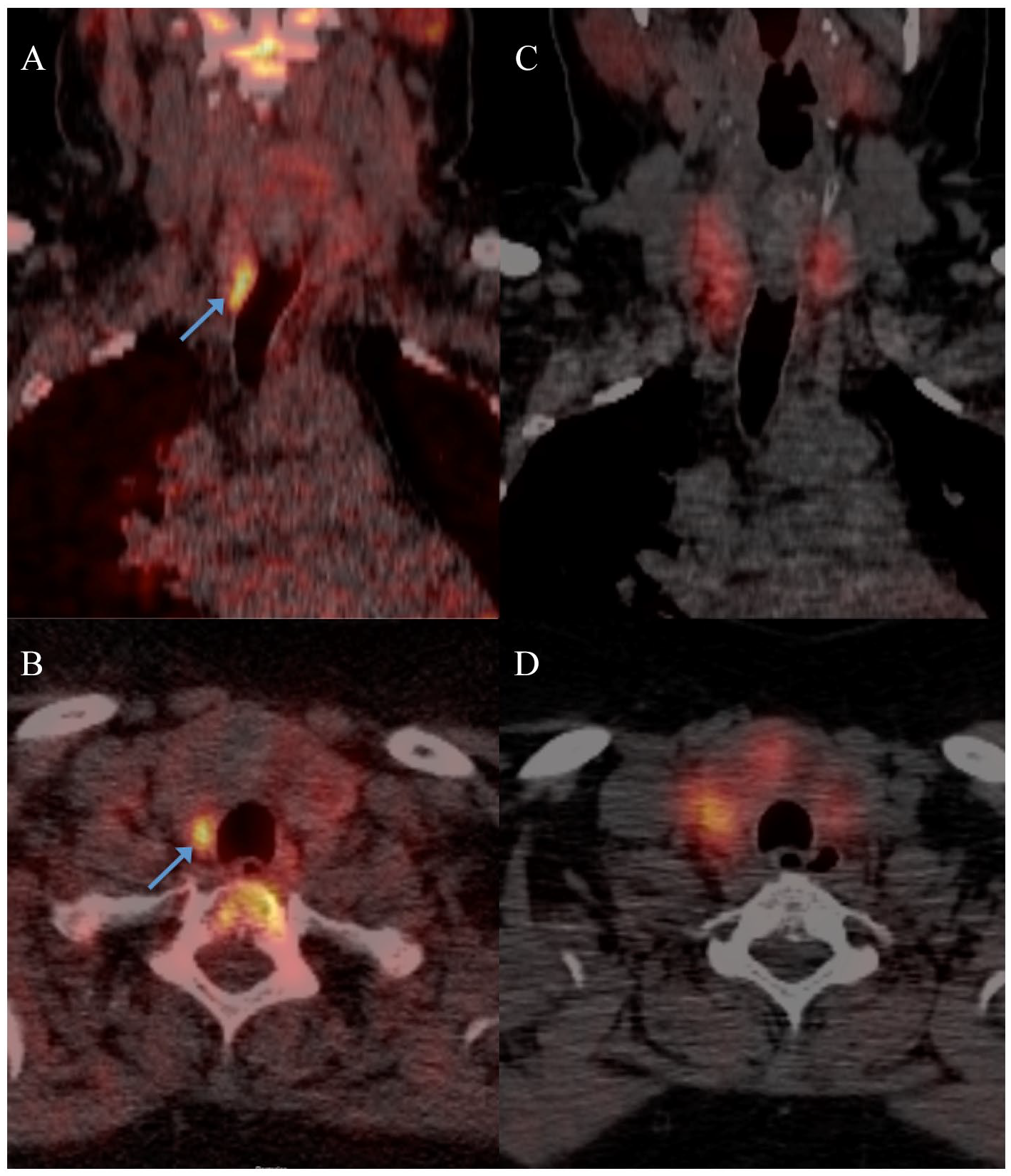
C-11 methionine PET superimposed on a non-diagnostic CT showing intense methionine uptake in the nodule in the lower third of the right thyroid lobe as indicated above (position 7, i.e. lower right quadrant) (A, coronal section; B, axial section). The Tc-99m sestaMIBI SPECT-CT scan showed no focal uptake (C, coronal section; D, axial section).
Ethics
The study was performed in accordance with Helsinki II Declaration. Informed consent was obtained from each subject.
Average radiation dose for the parathyroid scintigraphy was 10 mSv for the combined examination including Tc-99m pertechnetate and Tc-99m sestaMIBI (9 mSv) and a low-dose CT (1 mSv). Average radiation dose for the PET/CT scan was 3.5 mSv for the combined examination including C-11 methionine (2.5 mSv) and a low-dose CT (1 mSv). In total, the patients had a dose of 13.5 mSv for the combined scans. No complications to the procedures were observed. The retrospective study was approved by the local departments responsible for clinical treatment of PHPT and approved by the Danish Data Protection Agency.
Statistics
We used Stata 13.1 for statistical analyses. Biochemical data were described using means and range. For differences between groups, we used the Wilcoxon rank sum test for the non-parametric data and student t test for parametric data. For categorical data, we used the chi-square test for difference between groups. A value of p < 0.05 was considered statistically significant.
Results
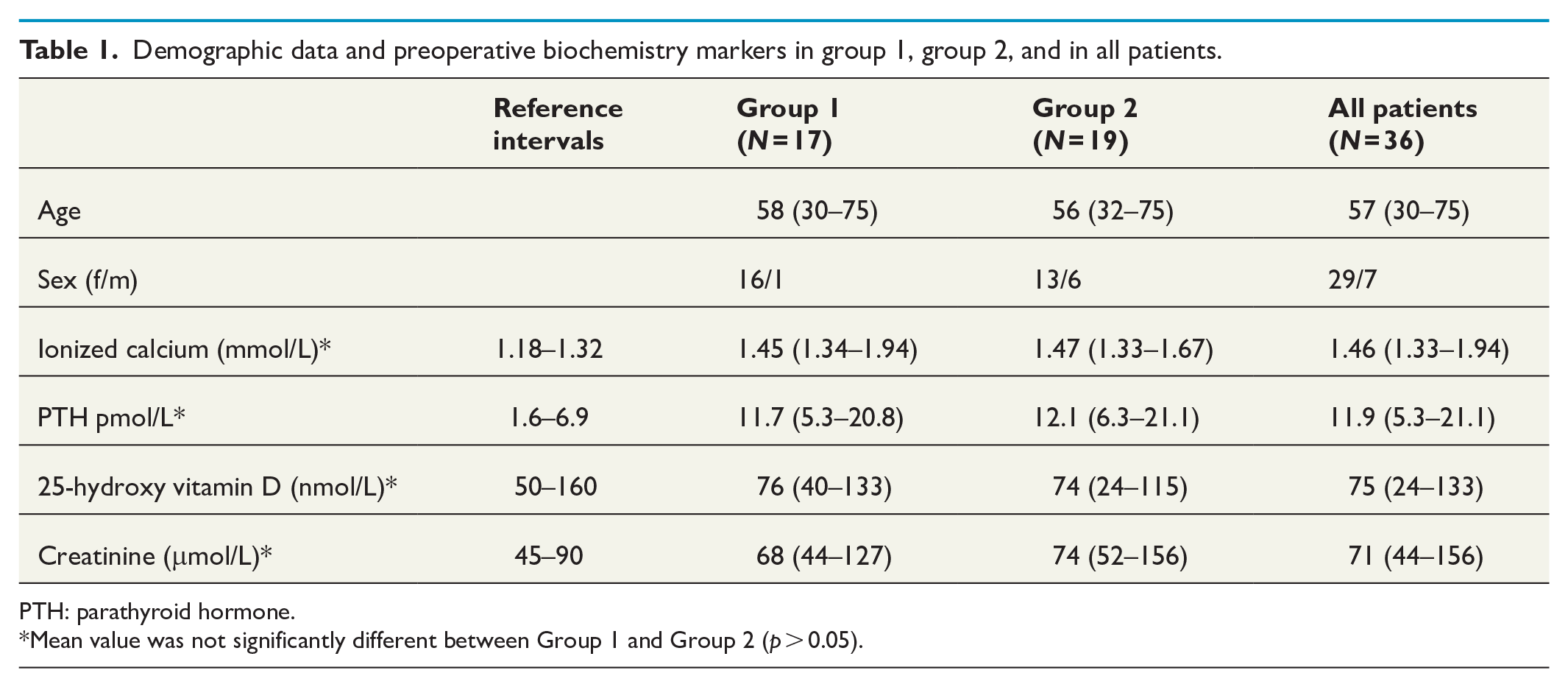
Preoperative demographic data are shown in Table 1. In all patients, preoperative values of ionized calcium were between 1.33 and 1.94 mmol/L, with an average of 1.46 mmol/L (reference 1.18–1.32 mmol/L). The average level of PTH was 11.9 pmol/L (reference 1.6–6.9 pmol/L) and 25-hydroxy vitamin D was 75 nmol/L (reference 50–160 nmol/L). The values did not differ significantly between groups.
Demographic data and preoperative biochemistry markers in group 1, group 2, and in all patients.
PTH: parathyroid hormone.
Mean value was not significantly different between Group 1 and Group 2 (p > 0.05).
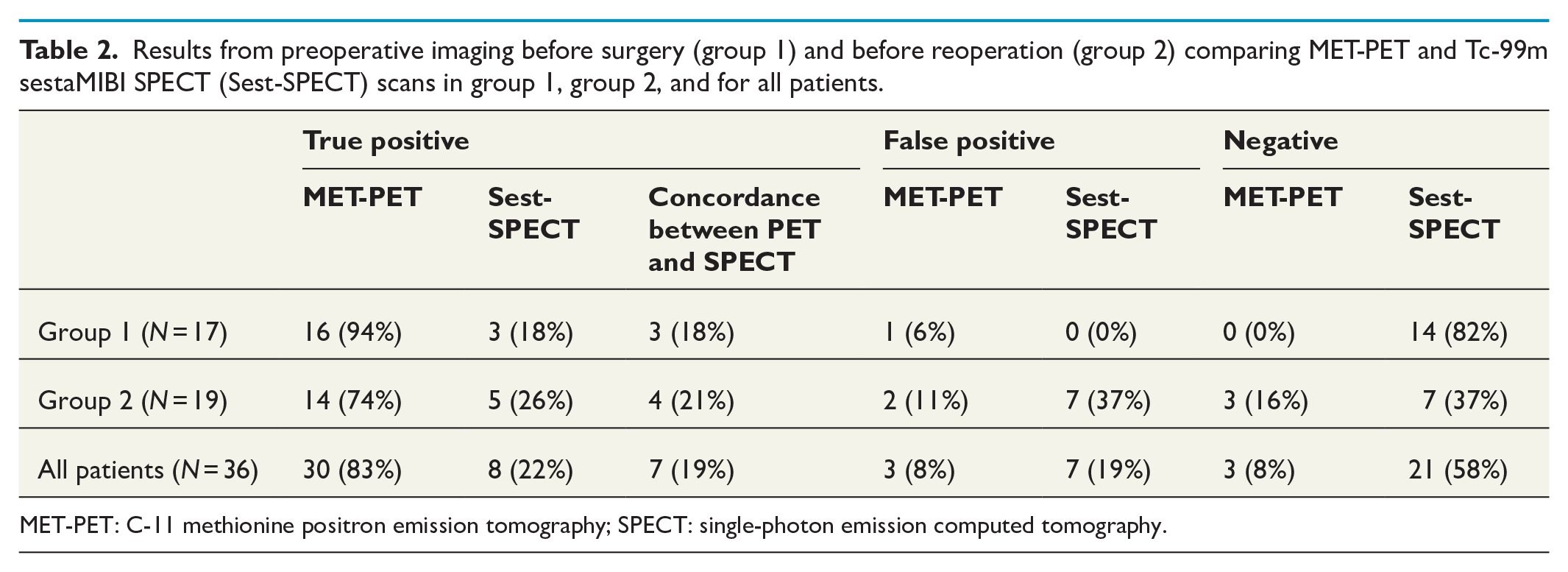
In all patients, localization of pathologic parathyroid tissue was true positive in 30 of the 36 MET-PET/CT scans (83%) (Table 2), and false positive in three patients (8%), of which two patients were diagnosed with thyroid cancer and one with a reactive lymph node. In three patients (8%), MET-PET/CT did not identify any potential focus of pathologic parathyroid tissue. Overall, the MET-PET/CT had a positive predictive value (PPV) of 91%, and a sensitivity of 91%.
Results from preoperative imaging before surgery (group 1) and before reoperation (group 2) comparing MET-PET and Tc-99m sestaMIBI SPECT (Sest-SPECT) scans in group 1, group 2, and for all patients.
MET-PET: C-11 methionine positron emission tomography; SPECT: single-photon emission computed tomography.
As the two subgroups were identified by an inconclusive preoperative localization, the proportion of true-positive findings in all patients was very low (22%) with the majority of scans being negative without any findings.
Occasionally, parathyroid identification is difficult due to structural thyroid disease. Hence, we also evaluated the thyroid structure in all patients apart from one with a previous total thyroidectomy. In remaining 35 patients, the thyroid structure was normal in 3 patients, with diffuse goiter in 1 patient, nodular goiter in 18 patients, and multinodular goiter in 13 patients.
In group 1 with an inconclusive parathyroid scintigraphy, 16 of the 17 patients (94%) had a pathologic parathyroid gland identified by MET-PET/CT scans with a histological confirmation (true positive), whereas one scan (6%) showed a false-positive result. This was a clear benefit for 13 patients (76%) allowing the operation to be unilateral. In the remaining three patients, resection of the identified pathologic parathyroid gland was not sufficient to cure the disease due to multiglandular disease and more glands had to be resected. One patient in group 1 with lithium intake for several years had persistent mild PHPT despite previous thyroidectomy and resection of two parathyroid glands with hyperplasia. The remaining 16 patients in group 1 had normal plasma levels of PTH and Ca2+ 6 months after PTX and were considered as being successfully treated. In this group, there were no cases of infection, bleeding, or paresis of the recurrent laryngeal nerve.
In group 2, 14 MET-PET/CT scans (74%) were true positive, 2 (11%) were false positive, and 3 (16%) were without any pathologic uptake. All 19 patients had at least one previous parathyroid operation with or without a unilateral thyroid resection. After the second operation, persistent disease was still remaining in four patients: one patient due to an intrathoracic adenoma removed later by lateral thoracotomy, one patient due to multiple ectopic autoimplants after an insufficient primary operation at another department, and two patients with mild persistent disease despite resection of hyperplastic glands. The first two patients could retrospectively be seen on MET-PET/CT, whereas the last two patients were negative on MET-PET/CT. The remaining 15 patients were considered as being successfully treated by the PTX. Postoperatively, one patient had paresis of the recurrent laryngeal nerve and four patients had hypoparathyroidism evaluated after 6 months. Three of these four patients all had previous resection of two or three glands, whereas the last patient also had a total thyroidectomy due to thyroid cancer. There were no cases of infection or bleeding.
Discussion
This retrospective study investigates the value of adding an MET-PET/CT following an inconclusive conventional imaging method for preoperative localization of pathologic parathyroid glands in a selected group of patients diagnosed with PHPT. In general, we found the MET-PET/CT valuable as an adjunct after inconclusive standard imaging in the preoperative parathyroid localization, showing an overall PPV of 91% and a sensitivity of 91%.
In this study, we had a high number of patients with multinodular goiter (37%) or thyroid nodules (52%). This could be one of the reasons for the negative/inconclusive Tc-99m sestaMIBI scintigraphy as reported in other studies besides the size of the adenoma/hyperplastic glands.8–10 However, despite the high prevalence of structural thyroid disease, it did not affect the interpretation of the MET-PET/CT scans significantly as indicated by the high PPV and low rate of negative MET-PET/CT scans. The results from this study are similar to PPVs and sensitivities found in other imaging studies using MET-PET/CT for preoperative localization of pathologic parathyroid glands. 3 In this review, the authors found a pooled sensitivity of 77% for detection of a lesion in the correct quadrant (range from 44% to 91%) in 14 MET-PET/CT studies including 327 patients (364 lesions).
Three selected studies,4–6 comparable to our study using a selected group of patients with negative or inconclusive conventional imaging prior to an MET-PET/CT scan, showed a pooled sensitivity of 81%, which is comparable to the current results. However, the studies showed divergent sensitivities of 54% and 84% in the group of patients with prior neck surgery. All three studies had limitations with lack of histological confirmations of the PET findings and various imaging protocols in one study. 4
Today, there is a tendency toward a more proactive surgical approach, meaning that the sestaMIBI and consequently the MET-PET/CT will be performed in an earlier stage of the disease, potentially presenting more of a challenge for the imaging methods. Challenges of MET-PET/CT are the false-positive findings. It is well known that MET-PET/CT is not a highly selective tracer for parathyroid adenoma, so the interpretation of the images requires an experienced reader to distinguish parathyroid adenomas from other benign or malignant pathologies such as reactive lymph nodes close to the path of parathyroid descent. Focal pathology within the thyroid gland might cause false-positive findings, such as thyroid cancer or hyperplastic thyroid adenomas. False-negative results could be related to the size of the adenoma, since PET in general is not a high-resolution technology such as magnetic resonance imaging (MRI) and some CT scanners, although new scanner technology shows higher sensitivity and resolution. However, in this study, we did not have adenoma weight measured as a standard. Thus, it was not possible to relate the weight of the adenoma to the results of the MET-PET/CT.
We used a single-phase, dual-isotope subtraction technique imaging protocol for the sestaMIBI scintigraphy with no late imaging at approximately 90 min, as seen in other centers (dual time point imaging). It is our experience that most foci (about 98%) are visible on the early images (unpublished data). It is also well known that many parathyroid adenomas wash out activity over time, which may reduce the diagnostic accuracy by using late images. A paper published by our center (Rasmussen et al.) 11 reported a PPV of 81% for the parathyroid scintigraphy in 88 patients using dual time point imaging. In a recent cohort consisting of 84 patients, we found a similar PPV (73%) with mean values of ionized Ca of 1.49 ± 0.18 mmol/L (mean ± SD) (data not published).
PET, in general, offers a better spatial resolution as compared to a parathyroid scintigraphy using SPECT, which is especially important for finding the small adenomas/hyperplastic glands. In general, the C-11 isotope is known to have a lower image quality as compared to the F-18 isotope,12,13 which could affect the detection rate for finding parathyroid adenomas, when comparing C-11 methionine to F-18 choline and F-18 FDG. However, the current and other studies using MET-PET/CT for preoperative localization of pathologic parathyroid glands report similar false-positive and false-negative results 3 as compared to studies using F-18 choline PET.14–18 Other tracers such as F-18 FDG19–23 show highly variable sensitivity and PPV and are generally not used for preoperative localization of pathologic parathyroid glands.
Better imaging protocols for MET-PET/CT may improve the detection rate. Contrast-enhanced CT may improve the diagnostic accuracy. However, this is not supported by a study by Andersen and colleagues. 24 In 138 patients, a diagnostic CT was added to a sestaMIBI scintigraphy and showed no significant change in diagnostic accuracy. In another study by Sandqvist and colleagues, 25 the sensitivity for detecting small adenomas by adding contrast-enhanced CT to 99mTc-MIBI SPECT/CT in preoperative localization diagnostics was significantly improved (0.81 versus 0.90; p = 0.003) in a large cohort of patients (N = 192), of which 149 patients could be related to surgery and histopathology. The specificity of non-contrast-enhanced SPECT/CT was similar to contrast-enhanced SPECT/CT (0.96 versus 0.98; p = 0.077). This was supported by a study by Komek and colleagues. 26 A systematic review and meta-analysis by Wan and colleagues 27 has studied 4D CT for the localization of hyperfunctioning parathyroid glands in comparison to a dual-phase 99mTc-MIBI SPECT with or without contrast-enhanced CT. The study showed similar values of specificity when comparing SPECT/CT with and without contrast-enhanced CT and a slightly better sensitivity, although not significant (0.87 versus 0.78; p = 0.125). 4D CT showed a borderline better sensitivity (0.85 versus 0.68; p = 0.048), but a lower specificity (0.93 versus 0.98; p = 0.014) compared to SPECT/CT without contrast-enhanced CT.
We have recently performed image quality control using our new generation of dynamic PET scanners (Siemens Biograph Vision 600), using dynamic whole-body MET-PET in five patients with different body mass indices (BMIs), and we found that imaging from 15 to 20 min pi. was optimal for image quality (visual inspection of signal-noise ratio) with adjustments of the time per bed position for patients with either a low or a high BMI (less resp. higher time per bed position) (data unpublished). However, this was not performed in our prior generation of PET scanners (Siemens Biograph 64 Truepoint), although we did regular evaluation of reconstruction parameters to optimize image quality. All patients included in this study were scanned using the Siemens Biograph 64 Truepoint.
Limitations of this study are the small sample size and the retrospective design. There was also a selection bias toward patients with negative imaging. Accordingly, this study only describes the added value of MET-PET/CT in highly selected patients and not in a general group of patients with hyperparathyroidism. But this is also the group of patients, where there is a need for a better imaging modality. A combined PET-MRI is currently getting available in many imaging centers for research and clinical use. At our institution, we have scanned two patients with C-11 methionine in combination with MRI using our newly installed GE Signa PET/MR scanner and shown promising potentials (one-stop shop). At this time, we have no data to support MRI to be superior to CT, but hopefully, we can present some more solid data in the future, as this might improve the detection rate for finding parathyroid adenomas, especially in the group of patients with an unsuccessful PTX and in patients with a suspicion of small adenoma(s) or multiglandular disease. However, better protocols for respiratory gating are needed to get better MRI images.
In conclusion, MET-PET/CT shows an overall high sensitivity of 91% and a high PPV of 91% in a subgroup of patients presenting mild to moderate PHPT with a negative or inconclusive sestaMIBI. This is important for both patients and surgeons in the preoperative planning of a PTX.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.