
Abstract
Background:
Thoracic duct chylous fistula is a rare complication following neck surgery, especially for malignant disease. Despite its low incidence, it can be a life-threatening postoperative complication increasing the risk of infection, bleeding, hypovolemia, electrolyte imbalance, and malnutrition. Currently, the management of thoracic duct fistula is not standardized yet. It can range from conservative to surgical approaches, and even when surgery indication occurs, there is no unanimous agreement on timing and operative steps, so the surgical approach still remains mostly subjective, in accordance with clinical conditions of the patients and with surgeon’s experience.
Aims:
The aim of the study was to search into Literature a common accepted behaviour in thoracic duct chylous fistula occurring.
Methods:
A literature review was carried out. Conservative treatments include fasting associated with total parental nutrition or low-fat diet, compressive dressings, and octreotide administration. If conservative treatment fails, in order to avoid dangerous consequences, functional repair of the thoracic duct injury with lymphovenous microanastomosis should be the preferred solution, rather than an approach that obliterates the thoracic duct or lymphatic–chylous pathways, such as thoracic duct embolization, therapeutic lymphangiography, and thoracic duct ligation.
Conclusions:
In our experience, patients undergone thyroidectomy and neck dissection for thyroid-differentiated cancer, who report an unrecognized thoracic duct chylous fistula after surgery, must be treated via integrated conservative and surgical treatment. A literature review about thoracic duct chylous fistula following neck surgery, focusing on the current management and therapeutic approach, was furthermore carried out, in order to delineate the actual therapeutic options in case of thoracic duct chylous fistula occurrence.
Introduction
Thoracic duct chylous fistula (TDCF) is an uncommon postoperative complication after neck surgery. The overall rate of thoracic duct lesions following neck dissection for head and neck cancers ranges from 0.62% to 6.2%. 1 Despite its low incidence, it can be a life-threatening postoperative complication increasing the risk of infection, bleeding, hypovolemia, electrolyte imbalance, and malnutrition, as well as resulting in delayed wound healing. In severe cases, TDCF can lead to chylothorax and mediastinal chylous fistula, which increases the risk of mortality.2 –4 Currently, no standard treatment guidelines in such complicate cases are reported. 1 Good clinical practice recommends conservative treatment as first approach especially for low flow fistula, proven to be solved in 66% of cases, as reported in the literature. 5 Conservative treatment includes fasting associated with total parental nutrition (TPN) or low-fat diet, compressive dressings, and octreotide administration. In case of complicated or high flow fistula, surgical treatment is the only curative approach to this potentially life-threatening complication. Several surgical strategies can be adopted, ranging from the direct ligation of the thoracic duct to muscle flaps creation, either in its cervical or thoracic tract. Other possibilities are the therapeutic lymphangiography, the duct embolization, and the creation of lymphovenous anastomosis.
In our experience, patients undergone thyroidectomy and neck dissection for thyroid-differentiated cancer, who reported an unrecognized TDCF after surgery, must be treated via an integrated conservative and surgical treatment. A literature review about TDCF following neck surgery, focusing on the current management and therapeutic approach, was carried out, in order to delineate the actual therapeutic options able to guide surgeons through the best clinical practice in case of TDCF occurrence. Patients at risk are those affected by thyroid nodular pathology consisting of a major lesion of the gland, when a III, IV, or V level lymphadenectomy may be needed.
There is no evidence of increased risk in thyroidectomy performed with continuous intraoperative nerve monitoring (IONM). 6 A drainage placed in the omoclavicular triangle is absolutely necessary. In case of fistula occurrence, at day 1 after surgery, an important edema usually can be detected in the supraclavicular fossa and a clear serous material can be drained after 12–24 h from surgery. On postoperative day 2, the drainage usually becomes milky liquid and reaches 400 cc or even more; ultrasound draining assistance can be required if drainage is inadequate. A precise balance of quantity of drainage per day is absolutely necessary, as well as a physical–chemical examination of the drainage that must be performed and considered positive for triglyceride content. When a diagnosis of iatrogenic TDCF is reached, according to the literature, a conservative approach must be initially undertaken, if possible. 7 Compressive medication surrounding the neck and shoulders has to be packaged as well as the fasting start. A central vein has to be cannulated, in order to permit a proper and tailored TPN, in accordance with the current guidelines: lipids have to be avoided not to irritate the lymphatic system, patients must be supported with proteins, liquids, and carbs. Octreotide 0.1 mg subcutaneous infusion has to be administered three times per day. Staging can be performed by a computed tomography (CT) scan. The radiologic scan can also show that the quantity of pleural effusion and pO2 determination is useful for dyspnea monitoring. A thoracic surgeon consulting is useful to evaluate thoracentesis indication in order to improve the patients’ ventilatory capacity, if necessary. A lymphography can be performed if the conservative treatment is not curative, fistula flow can grow up to >1000 mL per day and a multidisciplinary equip must evaluate the necessity of a new surgical approach. An experienced endocrine surgeon, skilled in neck surgery, must be enrolled in the operating team. The cervical thoracic duct lesions are usually next to the common carotid artery, the internal jugular, and the vagus nerve, so dissection must be very careful. Such lesions can be clipped and/or sewed with non-absorbable suture thread. Moreover, we suggest to use a fibrin sealant that has proven to be effective in axillary dissection 8 and of course a new drainage. Octreotide infusion, TPN, and fasting continued after the second look surgery. A serous draining can continue even after surgery for 3–7 days. Nevertheless, a wait-and-see attitude is suggested. The fistula flow should start to decrease in the following postoperative day, and after 24 h silent drainage, patients can start oral feeding and without evidence of any chylous discharge, the drainage can be removed and after 48 h oral feeding and silent drainage, the patients can be discharged.
Materials and methods
The authors performed a literature review, searching chylous fistula associated or not with chylothorax-related articles and case reports on PubMed database up to May 2019. The search terms used were “chylous,” “fistula,” “chylothorax,” “thyroidectomy,” and “thoracic duct” (Table 1).
Demographic, clinicopathological features, and patients’ management in papers selected for the review about thoracic duct fistula.
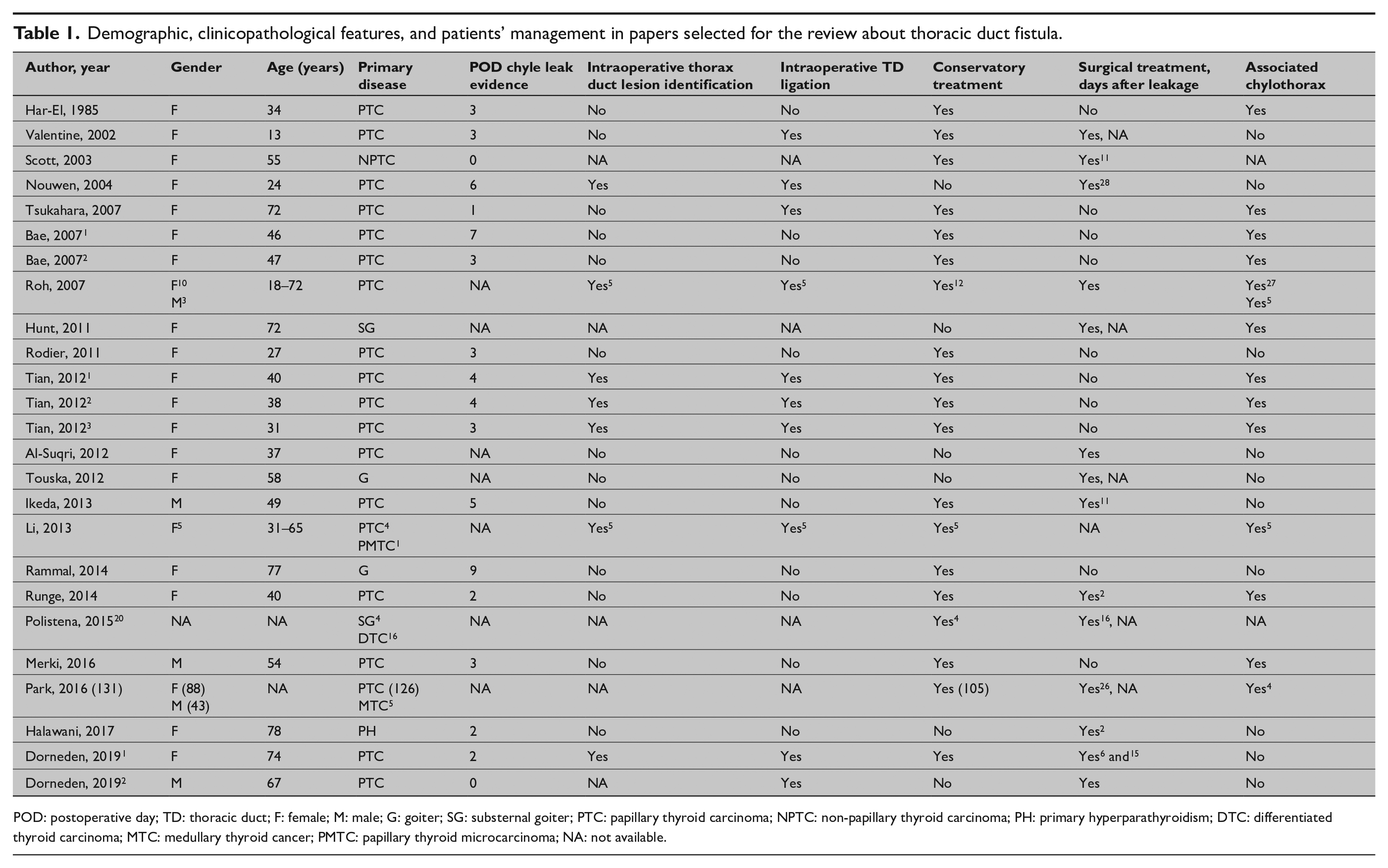
POD: postoperative day; TD: thoracic duct; F: female; M: male; G: goiter; SG: substernal goiter; PTC: papillary thyroid carcinoma; NPTC: non-papillary thyroid carcinoma; PH: primary hyperparathyroidism; DTC: differentiated thyroid carcinoma; MTC: medullary thyroid cancer; PMTC: papillary thyroid microcarcinoma; NA: not available.
Papers not including neck surgery or not describing a cervical lesion of the thoracic duct were excluded. The quality of the clinical studies examined was not an operative complication. Exclusion criteria were minimized due to the low number of papers treating this rarely described postoperative complication.
Using the PubMed database, a systematic review of the current literature was carried out, up to May 2019. The keywords search terms used were “thyroid surgery,” “Chylous fistula,” “neck dissection,” “neck surgery,” “lympho-node cervical dissection,” and “neck surgery.”
The various terms were substituted during the search. References of the more relevant articles were manually searched. The last research was concluded on 15 April 2019.
The search was carried out by two authors (G.G. and G.T.), and the obtained results were discussed with the senior author D.P. The following data were extracted from the included studies: gender, age, primary disease, postoperative day (POD) chyle leak evidence, intraoperative thorax duct lesion identification, intraoperative thoracic duct ligation, conservatory treatment, surgical treatment, days after leakage, and associated chylothorax.
The inclusion criteria of the study comprised the report of patients affected by TDCF worsening the postoperative of neck surgeries, either performed for the excision of thyroid gland lesions or parathyroid morbidities. All studies that failed to fulfill the established inclusion criteria and the not English language studies were excluded as well as the ones mentioning chylous fistula due to traumas.
Results
Twenty-six suitable studies were identified after the literature review. Four studies were excluded because written in non-English language (one Spanish, one Italian, one Polish, and one Japanese).9 –12 An article was excluded because the chylous fistula was consequent to a trauma chest lesion 13 (Fig. 1). Therefore, 21 studies responded to our inclusion criteria and were enrolled in the current review. The features of the 21 selected studies were summarized in Table 1.
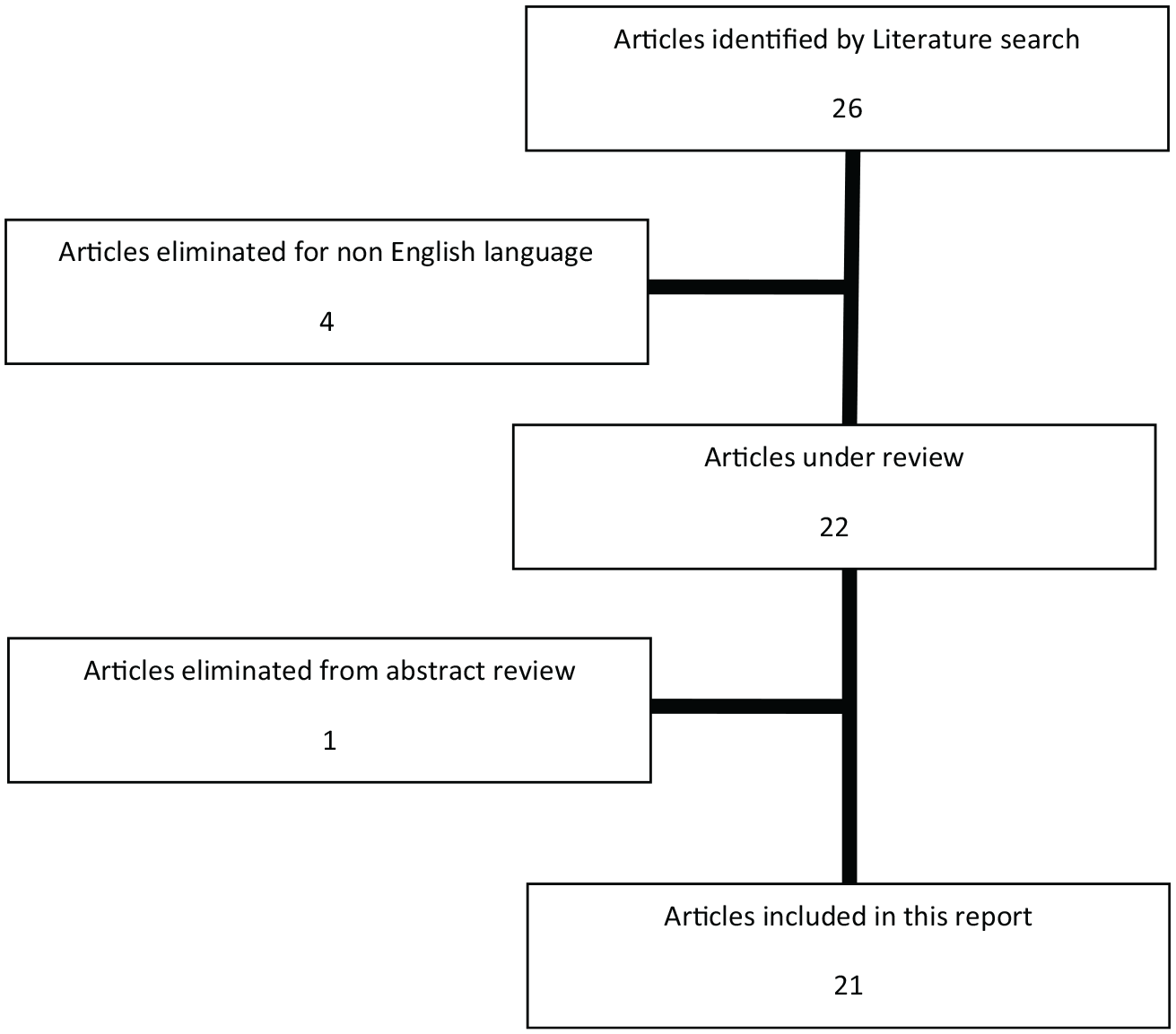
Flowchart of the paper selection process for the review.
Discussion
Thoracic duct lesion is a rare event that occurs after neck surgery, mostly after cervical–lateral dissection for malignant diseases.14,15 In some patients, it can be associated with chylothorax even if the primary thoracic duct injury occurs in the cervical region after neck dissection. In the literature, a few cases are reported about iatrogenic TDCF alone or associated chylothorax; therefore, the choice of the best treatment results largely subjective and influenced by surgeon’s experience. 16
The omoclavicular triangle is a well-known anatomic area investigated during lateral lymphadenectomy. Different anatomic structures, such as thoracic duct, lymph-nodes, brachial plexus, transverse cervical and suprascapular veins and arteries, subclavian artery, the terminal part of the external jugular vein, and the phrenic nerve can be recognized and potentially injured while dealing with this area. 1 Therefore, cervical lymphadenectomy, as an advanced demolition procedure, may lead to significant morbidity due to potential damage to critical loco-regional structures.17,18 A lymphatic lesion usually occurs at the junction of the left jugular and subclavian vein at the level of confluence with the thoracic duct. Symptoms of the chylous leak will be negligible if a small lymphatic route is injured that spontaneously heals in a few days, usually with the appearance of a vicarious draining system. Conversely in case of a major vessel damage, an evident chylous fistula can worsen postoperative outcome of surgery for thyroid carcinoma. 19
The authors performed a literature review, searching chylous fistula associated or not with chylothorax-related articles and case reports on PubMed database up to May 2019 (Table 1). Papers not including neck surgery or not describing a cervical lesion of the thoracic duct were excluded. Quality of the clinical studies examined could not represent the exclusion criteria, due to the low number of papers treating this rarely described postoperative complication.
Merki et al. 20 , in their case report and systematic review about chylothorax incidence in thyroid surgery, found that the injury of the thoracic duct and the consequent chylous fistula have a literature-reported incidence extremely variable (from 1% up to 6%), probably for the rarity of this event. Moley et al. described a higher incidence, up to 8.9%, of chylous fistula after neck dissection, in particular after thyroidectomy with thoracic approach 21 or in patients previously undergone to neck radiotherapy. It was also observed that radical dissection of the left side of the neck leads to a higher rate of duct damage than functional dissection. It usually occurs because the thoracic duct runs on the left side of the neck in the 92% of the patients and during radical neck dissection, particularly during lymphadenectomy nearby the jugular vein, the risk of damage is high. 22
The management of thoracic duct fistula is not standardized yet. It can range from conservative to surgical approaches, and in case of surgical indication, there is no unanimous agreement on timing and operative steps, so it remains mostly subjective, highly depending on patients’ clinical conditions and on surgeons’ experience. When a chyle leak lesion is evident at surgery, it is certainly suggested to be treated, at the same time, by suture ligation with non-absorbable material. 23 Conversely, when it is postoperatively demonstrated, conservative treatment is usually successful and best encouraged in patients affected by a low flow fistula, whose definition is unfortunately still debated (500–1000 cc). The conservative treatment consists in fasting, TPN, pressure dressing, and administration of somatostatin.24,25 Sharkey et al. 26 demonstrated the effectiveness of octreotide infusion as directly operating on vascular somatostatin receptors to minimize the excretion of lymphatic fluid. Rodier et al. reported in their cases that conservative treatment can still be chosen for high flow fistulas with curative intent, also in case of daily drain of 2000 cc of chylous liquid. 27
Fasting with associated TPN is both useful for chylous fistula and for chylothorax resolutions as shown in one of the TDCF cases reported by Har-El et al. 28 The chylous flow is, in fact, markedly increased after meals, especially if they have a high rate of long-chain fatty acid, that have to be avoided in order to decrease the production and flow of lymph and chyle, replenishing fluid and electrolytes losses, and preventing malnutrition. Options for nutritional care are low-fat diet or fat-free diet, enteral nutrition with a specific formula, parenteral support without oral intake, or combination of the above. Remaining issues raised by the literature concern the best nutritional approach for any specific patient type, how long nutritional management should be carried out, what level of lymphatic or chyle output is acceptable, or whether medium-chain fats should be avoided or included in the nutritional regimen.1,29,30
Dorneden et al. hypothesized that the negative pressure wound therapy can also be successful to treat low flow chyle fistulas when the pressure value is set relatively low to avoid the increase of fistula flow, and when blood vessels are certainly unharmed and far from the lesion, in order to avoid iatrogenic bleeding. 31
In the past decades, the drainage output appeared to be the best indicator of unsuccessful conservative treatment, as high flow fistulas were more likely to be surgically managed. Even timing was discussed. Several authors described that a 2-week conservative treatment time should be awaited before considering surgery.5,32 According to the current literature, if conservative treatment fails, operatively duct ligation should be the preferred solution 5 in order to avoid dangerous consequences such as redistribution of flow producing distal complications. Different occlusive strategies are available such as thoracic duct embolization, therapeutic lymphangiography, thoracic duct ligation, loco-regional flaps, and associated techniques. In multiple centers, for high-output chyle fistulas and for recurrent fistulas, thoracic duct ligation is the preferred and proven effective technique, with full symptom resolution and no recurrence or associated complications. 33 Thoracic duct ligation has been reported as successful with a rate of 88% in Itkin et al. series 34 ; however, there are still concerns related to the consequences of the flow blockage in the thoracic duct as probable leg swelling and chylous ascites. Moreover, one case of secondary chylothorax due to the rise of the intraductal pressure intrathoracically after the cervical ligation of thoracic duct was also described. 28 Therefore, functional repair techniques might be preferred and, when technically performable, lymphovenous microanastomosis should be the intervention of choice, so far.35,36 The tailored functional repair (i.e. the duct repair or its anastomosis with venous structures) of the thoracic duct lesions burdening all kinds of thoracic surgeries allows less potential complications due to the lymphatic stasis often related, instead, to the occlusive techniques as thoracic duct embolization or ligation.35,36
The prevention of thoracic duct lesions seems to be important when approaching a surgical operation with high risk of incidence of this pathology. Chakedis and Phay et al. described the possibility to identify the thoracic duct during lateral ND using indocyanine green (ICG) and near-infrared (NIR) imaging; they tried the technique in six patients undergoing lateral modified radical ND and it successfully identified the thoracic duct in five of them (83.3%).37 –40 In the near future, this intraoperative procedure could not only represent an important tool helping surgeons to avoid lymphatic vessels lesions, but also an important tool for intraoperative assessment of unidentified thoracic duct injuries.
Conclusion
The different possible clinical presentations of the challenging thoracic duct injuries require an appropriate multidisciplinary approach by experienced teams. Even if rare, the occurrence of injuring the cervical tract of the thoracic duct in surgeries as neck dissection has to be contemplated and suspected when high quantities of serum are drained postoperatively. A proper examination of the drained liquid should always be practiced according to this suspicion. Considering the literature data, once the diagnosis is reached, conservative treatment is strongly suggested in low-output fistulas and it could at least be considered in high-output fistulas; surgery should be approached in case of conservative therapeutic failure, rapid decrease of general conditions, or systemic inefficiency.
Footnotes
Acknowledgements
The authors acknowledges the Avenia NUnit of Endocrine Surgery—University of Perugia, Perugia, Italy. He has participated substantially in conception, design and execution of the study and with his clinical, surgical and professional experience.
Author contributions
All authors contributed significantly to the present research and reviewed the entire manuscript. D.P. participated substantially in conception, design and execution of the study and in the analysis and interpretation of the data, and also participated substantially in the drafting and editing of the manuscript. G.G. participated substantially in conception, design and execution of the study and in the analysis and interpretation of the data, and also participated substantially in the drafting and editing of the manuscript. G.T. participated substantially in conception, design and execution of the study and in the analysis and interpretation of the data. C.G. participated substantially in conception, design and execution of the study and in the analysis and interpretation of the data. S.P. participated substantially in conception, design and execution of the study and in the analysis and interpretation of the data. L.B. participated substantially in conception, design and execution of the study and in the analysis and interpretation of the data. R.R. participated substantially in conception, design and execution of the study and in the analysis and interpretation of the data. L.D. participated substantially in conception, design and execution of the study and in the analysis and interpretation of the data. All authors have read and approve the final manuscript.
Availability of data and materials
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.