
Abstract
Although advances in knowledge and technology have improved outcomes in surgical cardiac patients over the last decade, complications following cardiac operations still remain to be potentially fatal. Gastrointestinal complications, in particular, tend to have high rates of reintervention and mortality following cardiac surgery, with ischemia and hemorrhage being two of the commonest underlying causes. The intention of this review is to identify which risk factors play important roles in predisposing patients to such complications and to gain better insight into the pathogenesis of the sequelae. Furthermore, strategies for prevention have been discussed to educate and increase awareness of how adverse cardiac surgical outcomes can be minimized.
Introduction
Complications from the gastrointestinal (GI) system are uncommon but yet potentially grave consequences of cardiac surgery. The average incidence of GI complications following cardiac surgery is reported to be between 1% and 2% and associated with an overall mortality of 30% (1). These complications can range from mild nausea and vomiting to fulminant hepatic failure. The total blood flow through the splanchnic circulation is typically 20%–25% of cardiac output in the resting state (2). Hence, hypoperfusion of the abdominal viscera is likely to be a crucial factor contributing to the development of most, if not all, GI complications (3). The outcomes associated with these complications tend to be poor as well as prolonging in-hospital stay, they increase the needs for diagnostic or therapeutic reintervention via gastroscopy, colonoscopy, and laparotomy, all of which carry their own individual complications (4). The aim of this review is to explore the risk factors and mechanisms through which these complications arise and highlight which strategies can be implemented before, during, and after cardiac surgery to prevent them.
Mechanisms of Bowel complications post-cardiac surgery
It is important to be aware of the different risk factors associated with GI complications so that at-risk patients can be identified. This helps with the facilitation of increased close monitoring of these patients, before, during, and after surgery resulting in better patient outcomes. There are a range of risk factors which can be broadly divided into preoperative, intraoperative, and postoperative (Table 1).
Risk factors which increase likelihood of individuals to gastrointestinal complications following cardiac surgery.
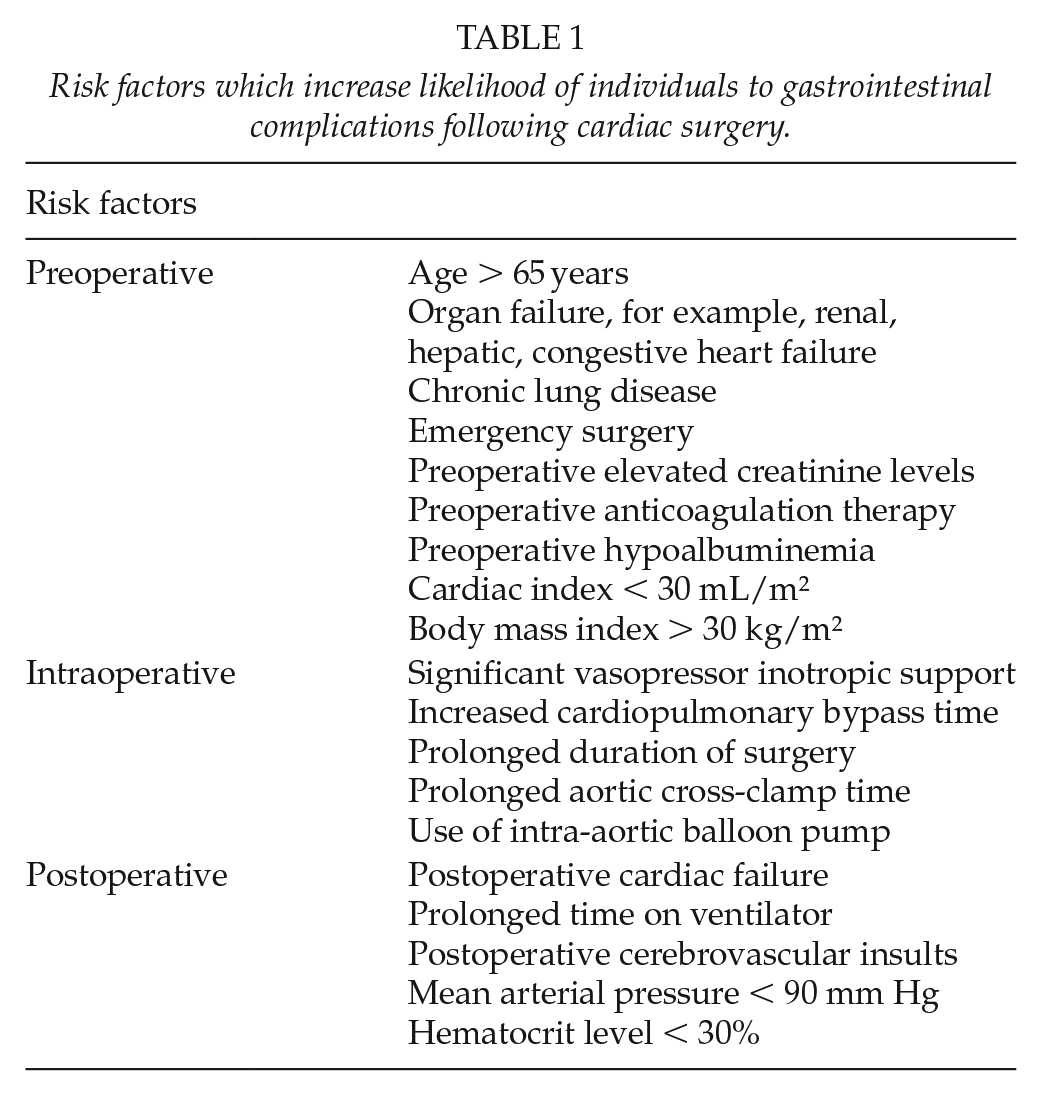
Risk Factors
Preoperative risk factors are many. Vascular risk factors include co-morbid triple vessel coronary artery disease and peripheral vascular disease (5). These can specifically increase the chance of intestinal ischemia (5). Organ failure can also increase the chance of bowel complications (4). These include renal failure, congestive heart failure, hepatic failure, and chronic lung disease (4, 6). Preoperative high creatinine levels and anticoagulation therapy are also factors that have been found to be of higher incidence among those with GI complications following cardiac surgery (6). One recent retrospective study found that, following open heart surgery, GI complications were more likely in those with hypoalbuminemia, a cardiac index < 30 mL/m2 and a BMI > 30 kg/m2 (6). There are also various intraoperative risk factors. The use of significant vasopressor inotropic support, cardiopulmonary bypass (CPB), and prolonged duration of surgery put patients at an increased risk of intestinal ischemia (5). Specific lengths of CPB time found to increase the risk of GI complication such as CPB time > 120 and > 140 min (4, 6). Vasopressin therapy in particular has been found to be a risk factor for ischemic colitis (7).
Postoperative risk factors of developing intestinal ischemia include an increased need of blood transfusion postoperatively (5). In addition, using intra-aortic balloon counterpulsation for low cardiac output results in an increased chance of mesenteric ischemia (5, 8, 9). Other significant factors include postoperative cardiac failure (specifically creatinine > 200 μmol/L), prolonged time on a ventilator, having had a cerebrovascular insult (CVI), mean arterial pressure (MAP) < 90 mm Hg, and hematocrit level < 30% (6, 9). Significantly, cardiac surgery has been found to be associated with a high risk of acute renal failure (ARF) with up to 30% of patients undergoing cardiac surgery experiencing ARF (10). An interesting finding from one large retrospective study was that, despite advanced age previously being associated with an increased risk of intestinal ischemia, it was not found to be a risk factor in this study (9). However, there have been other studies that have found patient of older age, particularly those aged above 65 years, is in fact a risk factor for bowel complications post-cardiac surgery (4). Thus, there is still uncertainty regarding whether older age is a risk factor. Emergency cardiac surgery has also been found to increase the likelihood of GI complications postoperatively (6,11).
Pathophysiology
The GI organs receive 20%–25% of the body’s cardiac output and accounts for 20% of the oxygen needs in a healthy person. The main blood supply to these organs include the coeliac artery (which supplies the liver, stomach, abdominal esophagus, spleen, superior duodenum, and superior pancreas), superior mesenteric artery (which supplies the distal duodenum, jejuno-ileum, ascending colon, and part of the transverse colon) and inferior mesenteric artery (which supplies the large intestine from the splenic flexure to the upper part of the rectum), all of which branch from the abdominal aorta (12).
The causes of GI complications are multifactorial, but the primary hypothesis is that reduced cardiac output results in visceral hypoperfusion associated with CPB causing mucosal ischemia and necrosis. This is due to alterations in splanchnic perfusion during cardiac surgery. An important sequence of CPB is the increase in systemic vascular resistance associated with non-pulsatile perfusion. The loss of pulsatility in the renal arteries alongside the reduction in MAP during the CPB surgeries leads to activation of the Renin–Angiotensin–Aldosterone System (RAAS). Activation of the RAAS results in the conversion of angiotensinogen to angiotensin I and then angiotensin II. Angiotensin II is a potent, selective mesenteric vasoconstrictor which has a high affinity for the peptide hormone on splanchnic vascular smooth muscle resulting in mesenteric vasoconstriction. It is important to note that, however, angiotensin II may not be the only candidate that mediates mucosal hypoperfusion during CPB (13).
Another important theory to mention is the fact that CPB can result in the release of inflammatory mediators, such as C5a, thromboxane (A2 and B2), and leukotrienes, which have been found to be mesenteric vasoconstrictors in animal models and hence contribute to the hypoperfusion of the GI organs (13). Much of this research has been conducted in animal models such as that by Douget et al. (14). The use of a rat model in this study found that CPB lead to mesenteric endothelial dysfunction and a systemic inflammatory response which may increase the risk of mesenteric ischemic events during cardiac surgery (15). Another important factor is the role of the complement system during CPB. The complement system mainly the alternative cascade are activated during CPB, and the complement protein C5b-9 specifically has a role in mediating systemic inflammatory reactions caused by CPB (15). During CPB, it has been found that there is a large and increased amount of free radicals being produced which results in higher amounts of systemic oxidative stress (16). This phenomenon of oxidative stress is a key factor contributing toward GI disease (17). For this reason, it is vital that oxidative stress is minimized during cardiac surgery, in order to help reduce and prevent GI complications. CPB can also cause microemboli formation. These emboli can go onto cause multi-organ dysfunction by obstruction blood vessels. One example being that they can cause bowel ischemia as a result of obstruction of the bowel’s blood supply. One technique that has been found to successfully eradicate gaseous microemboli is hypobaric oxygenation (18).
Specific Complications
The mechanisms described above have a significant impact on the abdominal viscera and can lead to potentially fatal outcomes. Table 2 summarizes the specific GI complications which occur in surgical cardiac patients.
Specific gastrointestinal complications following cardiac surgery and the reported overall incidence from individual studies.
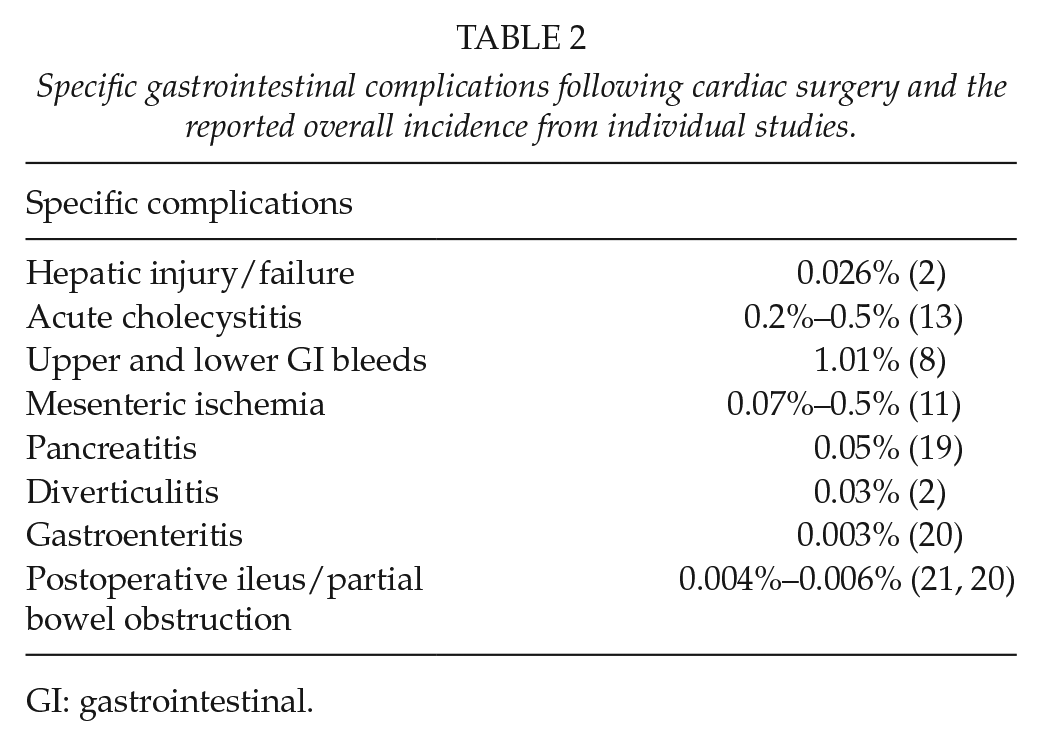
GI: gastrointestinal.
Hepatobiliary System
Fulminant hepatic failure is a serious complication related to cardiac surgery and has been described to carry an incidence of 4% in those with GI complications and rises to 10% in patients receiving CPB (19). Individual separate studies, however, seem to predict the incidence of hepatic injury, from all GI complications, to be far less. One study found that out of 3158 patients, 36 suffered from GI complications. 2 patients of those 36 endured hepatic failures, manifesting as progressive cholestatic jaundice, deranged liver functions test values, and uncorrectable coagulopathy (22). Another study which identified 4 patients out 33 with GI complications post-cardiac surgery with hepatic failure, 50% died following further hepatic dysfunction and ultimately multiple organ failure (21). Rodriguez et al. (1) found the overall incidence of hepatic failure in all patients’ post-cardiac surgery to be 0.026%, consequently proving to be uncommon. The combination of hemodilution and oxidative stress from CPB seems to play a large role in hepatic injury (19, 21). Furthermore, episodes of reduced perfusion can shunt blood away from the abdominal viscera and toward areas of higher priority, reducing flow to the hepatic circulation and causing centrilobular sinusoid ischemia (19, 21). Hyperbilirubinemia is also common following cardiac surgery with CPB (23). This can range from mild to persistent marked hyperbilirubinemia, the latter increasing mortality. A study by Farag et al. aimed to find factors, which increased severity of hyperbilirubinemia, causing marked worsening of liver function. CPB was identified to be the most significant cause of postoperative mortality due to hyperbilirubinemia (23). As well as hepatic failure, acute cholecystitis is a known complication of cardiac surgery with an incidence of between 0.2% and 0.5% (24). Ischemia once again plays a role in underpinning the mechanism behind this, aggravating mucosal injury and encouraging bacterial intrusion through the anatomical layers of the gallbladder. Recognition and diagnosis of acute cholecystitis tends to be delayed due to the lack of any obvious signs and symptoms and hence mortality can range between 65% and 100% (24).
GI bleeds
The most common GI consequences following cardiac surgery are GI bleeds, accounting for 33% of all GI complications (1). An Australian study by Shin and Abah (20) identified that 21 out of 61 patients with GI complications post-cardiac surgery had significant GI bleeds (11). Of those, 13 had upper GI bleeding, 5 with lower GI bleeding, and 3 with combined upper and lower GI bleeding, conveying upper GI bleeds being the more common of the two. These patients were managed via endoscopy and CT angiogram guided embolization, but overall mortality still came to be 38%. Upper GI bleeds seem to be more prevalent than lower GI bleeds and this is supported in various studies (25, 26). A study by Krawiec et al. found that the overall incidence for GI bleeding post-cardiac surgery was 1.01% and 78% of those patients who had an upper GI bleed. Endoscopy showed the most important cause to be duodenal ulceration, followed by gastric ulceration, gastric erosion, duodenal erosion, and Mallory–Weiss tears. A key limitation of this study, however, was that only bleeds that required endoscopic intervention were included and medically resolved smaller bleeds were not (25). Another study found 0.9% of cardiac operations to be complicated by upper GI hemorrhage with stress ulceration to be a key cause. In total, 90% of those undergoing cardiac surgery were known to be taking aspirin and warfarin, both of which can increase risks of bleeding (26). Ischemia can impair gastric and duodenal mucosal defense mechanisms causing stress ulceration and the extent of ischemia depends on duration of CPB and aortic cross-clamp time (26).
Ischemic Bowel
An important complication of cardiac surgery is mesenteric ischemia or infarction. A study by Yap et al., which included 68,214 patients from seven cardiac surgical centers from 1980 to 2011, determined that the incidence of post-cardiac surgical bowel ischemia range from 0.07% to 0.5% and the morality ranges from 59% to 64%. Mesenteric ischemia (also known as bowel ischemia) is a life-threatening condition. Patients often present non-specifically due to reduced cardiac output and gut ischemia. The main perioperative risk factors are advanced age and peripheral vascular disease. The main intraoperative risk factors include the CPB time and prolonged cross-clamp of the appropriate vessel. With respect to the postoperative risk factors postoperative blood loss, postoperative renal failure and the use of inotropes were determined to be significant risk factors for the development of mesenteric ischemia in cardiac surgery patients (27). A recent paper from the World Society of Emergency Surgery (WSES) on acute mesenteric ischemia emphasized the importance of urgent diagnosis of the condition through CT angiography followed by surgery to resect necrotic intestine (28). A similar paper by Björck et al. described the European Society for Vascular Surgery (ESVS) clinical practice guidelines for patients with diseases of the mesenteric arteries and veins. These guidelines emphasize the importance of the need to develop a biomarker for intestinal ischemia to aid in the management and diagnosis of the condition (29).
Pancreatitis
Acute pancreatitis is another complication post-cardiac surgery. It is an inflammatory disorder with a variety of etiologies (e.g. gallstones, pancreatic malignancy, and endoscopic retrograde cholangiopancreatography). Patients often present with epigastric pain, back pain, nausea and vomiting, abdominal distension, and signs of circulatory failure (shock). They are then investigated by looking at levels of serum amylase or lipase and using a computerized tomography (CT) scan. Management of these patients is often conservative using nasogastric drainage, fluid resuscitation, and analgesia (12). The incidence of acute pancreatitis varies from 0.05% to 19% depending on the type of cardiac surgery. A study by Chung et al. (30) determined that checking serum lipase in patients after cardiac surgery and remaining vigilant for signs and symptoms of pancreatitis after cardiac surgery will help prevent pancreatitis or detect it earlier on for more efficient management. A further study by Leppaniemi et al. emphasized the importance of identifying patients with severe acute pancreatitis who are at risk of pancreatic infection and peripancreatic necrosis and may need to be managed operatively. They provide evidence-based guidelines for the diagnosis, antibiotic treatment, and management of severe acute pancreatitis (31).
Diverticulitis
Diverticulitis is a rarer complication following cardiac surgery with an overall incidence of 0.03% in all post-cardiac surgery patients (1). Diverticulitis involves the formation of diverticula (pouches of the colonic mucosa that have herniated through the muscularis propria) in the large bowel, particularly within the sigmoid colon. The pathophysiology underlying the development of diverticulitis post-cardiac surgery is not well understood but is thought to be due to hemodynamic changes, vasopressor use, and splanchnic hypoperfusion during CPB. These factors all lead to tissue ischemia and diverticular infection. Diverticulitis presents with pain in the left lower quadrant of the abdomen and fever. The disease is classified using Hinchey classification of diverticulitis into four stages and management involves fluid resuscitation, bowel rest, antibiotic therapy, percutaneous drainage, and colon resection (32).
Gastroenteritis
One large study which looked at GI complications from 5382 patients over almost a 10-year period found that 61 out of the 5382 patients experienced GI complications and among these, 17 patients experienced gastroenteritis post-cardiac surgery (0.003) (11). Clostridium difficile (CD) was confirmed in three of these patients (11). There were no patient deaths from the 17 who had gastroenteritis (11). In this study, there were found to be 19 patients who had partial bowel obstruction/ileus post-cardiac surgery, with no deaths (0.004) (11). CD infection among patients with gastroenteritis following cardiac surgery has been found to be associated with longer amount of time spent in intensive care, longer hospital stay, and longer amounts of time being mechanically ventilated (33). From this, we can deduce that by introducing prophylactic measures to try and reduce CD infections post-cardiac surgery, it may result in better patient outcomes.
Postoperative Ileus and partial bowel obstruction
Another large study, which looked at 881 children who underwent cardiac surgeries, found that 31 of these patients had GI complications (34). There were 5 (16%) children who had postoperative ileus (34). There have been found to be a variety of risk factors of patient developing a sudden and severe CD infection post-cardiac surgery. These include the transfusion of large amounts of blood products, preoperative ventilation, cross-clamp time > 130 min, and co-morbid conditions including type 2 diabetes mellitus (35). By identifying these high-risk patients, CD infection could be prevented or its severity reduced. Postoperative ileus and partial bowel obstruction are relatively common complications following cardiac surgery. One large study, which looked at 4288 patients following CPB surgery, found that 59 of these patients had GI complications and 36% of them (21 patients) had paralytic ileus (36). Another large study looking at 1360 patients who underwent CPB surgery, 0.21 developed GI complications (29 patients), with paralytic ileus being the most common complication (12 patients) (37).
Prevention
GI complications after cardiac surgery are rare but have significant morbidity and mortality; hence, it is important to recognize them early and treat them as appropriate.
Risk Stratification Models
Preoperative risk stratification is an important part of any surgical procedure and aims to reduce mortality and morbidity by identifying and assessing factors which may contribute to poor prognostic outcomes. The European System for Cardiac Operative Risk Evaluation (EuroSCORE) is one scoring system used to predict in-hospital mortality, direct costs, postoperative complications, and postoperative length of stay in hospital following cardiac surgery (38). The EuroSCORE can successfully predict some specific complications post-cardiac surgery, such as sepsis, renal failure, and respiratory failure; however, it fails to predict other major complications such as stroke, myocardial infarction, and GI complications (38). A newer scoring model, named the GI complication score (GICS), was proposed by Andersson et al. (39) and aimed to predict complications arising specifically from abdominal viscera following cardiac surgery. The study was able to successfully validate this model and GICS showed to have good predictive ability for GI complications (39). Although risk stratification models are effective, cheap, and easy to use, a key limitation of them is that healthcare professionals may become over-reliant on their use and miss broader risk factors not considered in the original design of the model.
Perioperative Preventative Measures
There is ongoing debate as to whether routine use of prophylactic proton pump inhibitors (PPIs) can reduce GI complications, particularly stress ulcers and hemorrhagic events. A study by Shin and Abah (20) was marginally in favor of acid suppression drugs due to the high morbidity and mortality associated with GI bleeding following cardiac surgery. However, these drugs have also been demonstrated to increase the risk of hospital-acquired pneumonia (20). Another study by Bhat et al. argued against the use of acid suppression drugs as PPIs were found not to significantly alter the incidence of postoperative hemorrhagic events. This may be because the formation of stress ulcers is thought to be due to splanchnic hypoperfusion and ischemia rather than pH related (40). These conflicting views warrant further studies in order to deduce the efficacy of prophylactic PPI therapy prior to cardiac surgery. A review article by Allen suggested a number of potential preventive measures including preoperative honing of an hemodynamic state with careful attention to hypovolemia, anemia, and cardiac output; intraoperative monitoring and maintenance of adequate cardiac output; monitoring of GI perfusion via ultrasound of mesenteric blood flow and measurements of intestinal transport functions (41). There are a limited number of measures which can be taken postoperatively to reduce GI complications. One study found that early aspirin therapy post-coronary bypass surgery to be linked to a 62% reduction in the incidence of bowel infarction along with a reduction in mortality and other ischemic complications involving the GI tract (42). Since CPB appears to play a crucial role in the pathophysiology behind these complications, modifications to CPB may help to reduce the likelihoods of them occurring. CPB is a form of extracorporeal circulation which facilitates cardiac surgery on the heart and great vessels. A case control study by Zhang et al. analyzed 206 patients who had GI complications following CPB surgery from 2000 to 2007 compared to 206 matched control patients. The results of this study suggested that GI complications could be reduced by maintaining a higher perfusion pressure and shortening the time on CPB and ventilation (43).
Conclusion
GI complications still remain a significant cause of mortality following cardiac surgery. Hypoperfusion of the abdominal viscera and the stresses associated with the use of CPB seem to play key roles in the pathogenesis. There are many risk factors which may predispose an individual to fall victim to these complications and it is crucial for clinicians to be aware of them in order to appropriately carry out risk stratification and minimize poor prognostic outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
No ethical approval is required as no patient identifiable information is shared.