
Abstract
Background and objective:
Pilonidal disease is common, and it afflicts especially young adults, causing disability. Several types of treatment methods are applicable, but no consensus exists regarding the best method. The aim of our study was to assess the novel radial laser probe treatment in pilonidal disease and report the success rate and recurrence rate.
Methods:
We studied retrospectively 86 patients who, according to our hospital patient records, underwent radial laser probe surgery between January 2017 and September 2019.
Results:
In a mean follow-up time of 14 months, the success rate at 2 months was 86%. Most operations were done under local anesthesia on a day-surgery basis. The recovery time was rapid, and median sick leave was 12 days. Of those initially successfully treated, 3% developed a recurrence. Altogether 17% of the patients underwent a re-operation. Spillage of pus during surgery, however, reduced the success rate to 53%.
Conclusions:
Radial laser probe treatment is a quick, safe, and minimally invasive treatment choice for pilonidal disease, especially when no active infection is present.
Introduction
Pilonidal disease is an inflammatory condition in the gluteal cleft with an incidence of 26/100,000, with men affected at a rate 2.2-fold that of women. 1 Other risk factors include obesity, family history, local trauma, excess body hair, particularly in the gluteal cleft, and adolescence. 1 The etiology has been under wide dispute. Earlier, pilonidal disease was considered congenital. Although its congenital component is indeed of some importance, pilonidal disease is now mainly considered an acquired disease. 2 Although this condition was first described in 1833 by Herbert Mayo, still no consensus exists regarding the best treatment choice. 3
Traditionally, basic treatment of pilonidal disease has been excision of all skin and subcutaneous tissue involved, followed by either primary closure of the wound or open-wound treatment, both techniques requiring a long recovery time. 4 Several flap reconstructions described include Z-plasty 5 , Karydakis plasty 6 , Bascom flap 7 , Limberg flap 8 , or V-Y flap. 9 Recovery after flap-reconstructions is reportedly good, but these procedures are also associated with long hospital stays and rather long recovery times.
Minimally invasive surgery to ensure shorter hospital stays (and quicker return to normal daily activities) includes pit-picking, a simple operation with good short-term results 10 , and for simple pilonidal sinuses, a fibrin glue procedure that seems easy and effective. 11 Phenol has for several decades served as a minimally invasive treatment with promising results. 12 Only a few prospective randomized studies have compared differing operations, making it difficult to draw conclusions regarding which is superior.
In 2016, Dessily et al. 13 reported on a promising radial laser probe treatment (FiLaC™; Biolitec, Germany) for pilonidal disease with a success rate of 87.5% and recurrence rate of only 2.9%. Since then, a few other studies have reported similar results.14 –16
The aim of this study was to assess the novel radial laser probe treatment for 86 patients with pilonidal disease and report the success rate and recurrence rate.
Materials and methods
This study was conducted in accordance with the Declaration of Helsinki; its authorization number is HUS/333/2019, 9 September 2019.
Medical records were available for review of 86 patients who underwent the radial laser procedure at the Day Surgery Unit of the Abdominal Center, Helsinki University Hospital, Espoo, Finland, between January 2017 and September 2019. During this period, a total of 356 patients underwent some kind of pilonidal disease operation in the same unit. Medical records were reviewed at mean 14 months (range: 6–37 months) postoperatively.
All patients underwent surgery by four consultant-level surgeons and seven residents who were free to choose the most suitable operation technique for each patient. The radial laser probe treatment was a new method for all surgeons in the unit. Of the 11, 2 consultant-level surgeons who were acquainted with the radial laser probe technique trained the other 9 surgeons to use it. Of the 88 patients treated with the radial laser probe, 2 were excluded, because they were minors. The 86 adult patients above age 18, with a male predominance (68 male, 79%; 18 female, 21%), were treated with the radial laser probe. All patients were suitable for day surgery. The patients were evaluated at the out-patient clinic 2 months postoperatively.
Surgical technique
All procedures were performed in the prone position. A single dose of 1.5 g of cefuroxime and 0.5 g of metronidazole was administered intravenously 30 min preoperatively. Hair removal from the operation site was done with razors. Local anesthetic was infiltrated into the operating area, to anesthetize the operation site as well as to protect the skin from the heat of the probe. The pit openings were identified and enlarged with a clamp. Sinus tracts were examined with a metal probe, and then all hairy material was removed with a small clamp and curette. The sinus tract was then treated with a radial laser probe (FiLaC) inserted into the sinus tract and 10 or 13 W energy was applied. The laser probe was withdrawn at a rate of 1 mm per second (from the tract). If the tract did not close after the first insertion and withdrawal, the procedure was repeated.
Anesthesia
The procedures were performed under local anesthesia (ropivacaine + lidocaine adrenalin; n = 73, 85%), total intravenous anesthesia (propofol + remifentanil; n = 4, 5%), or spinal anesthesia (bupivacaine + fentanyl; n = 9, 10%). The decision on which type of anesthesia to use was made between the surgeon, the patient, and the anesthesiologist. After the patients were discharged, oral ibuprofen and paracetamol served as postoperative painkillers.
Follow-up
All patients’ data were collected and analyzed from the patients’ medical records. Follow-up took place 2 months postoperatively, with the following data collected: patient demographics (age, gender, body mass index (BMI), American Society of Anesthesiologists score, cigarette smoking, alcohol consumption), type of anesthesia, spillage of pus from sinus tract during surgery, number of sinus pits, follow-up time after surgery, length of sick leave, healing rate at the first follow-up visit 2 months postoperatively, postoperative complications, interstitial fluid spillage after surgery, and recurrence rate.
Statistical analysis
The results are presented as mean with standard deviation unless otherwise stated. The Pearson chi-square test showed comparisons between groups. Two-sided p values <0.05 were considered statistically significant. Analyses were performed with IBM SPSS Statistics 25.
Results
For our 86 patients, mean follow-up time was 14 months (range: 6–37 months). Day surgery was successful for 84, and 2 patients stayed overnight in the hospital for personal reasons. At their follow-up visit, a total of 74 patients (86%) had healed, 2 months postoperatively. Tissue-fluid leakage from the wound appeared at a mean of 4 weeks (range: 0–8 weeks) postoperatively. The mean sick leave was 12 days (range: 7–18) (Table 1).
Characteristics of patients undergoing pilonidal disease laser surgery.
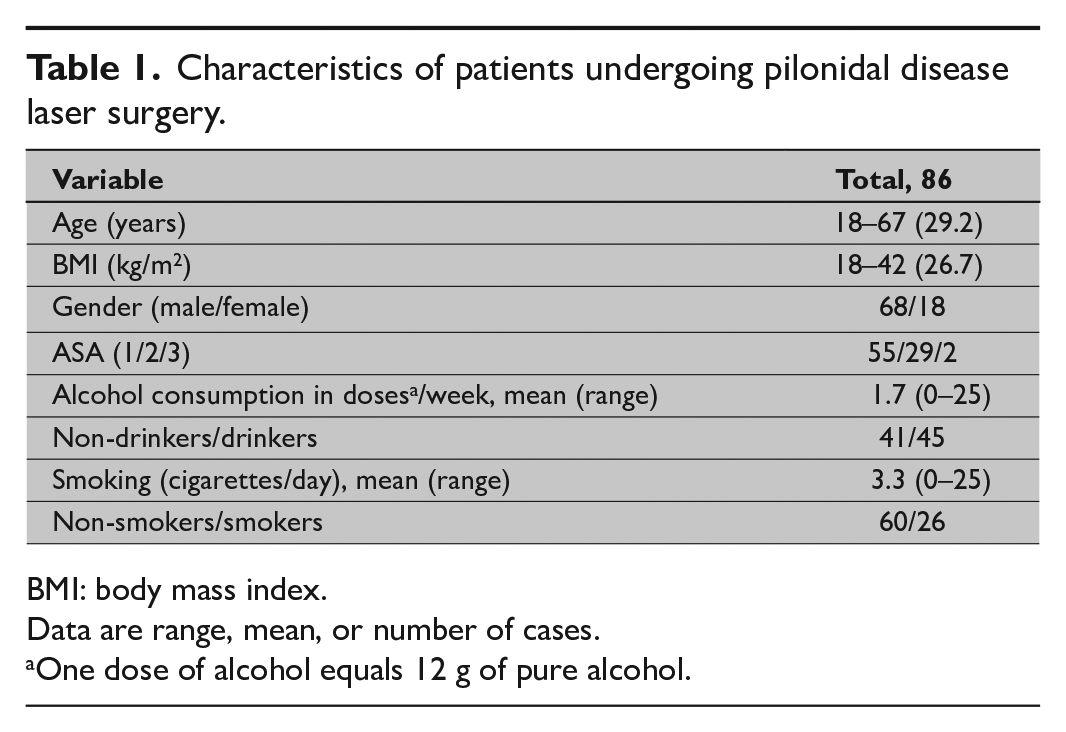
BMI: body mass index.
Data are range, mean, or number of cases.
One dose of alcohol equals 12 g of pure alcohol.
The healing rate was 93% when no spillage of pus occurred during the operation, compared to 53% when such spillage occurred (p < 0.0001). During follow-up, three recurrences appeared at a mean of 8.5 months postoperatively. For the 12 patients whose wound had not healed at 2 months, a re-operation was planned, and 15 patients underwent a second operation. Re-operations were divided into four groups, with nine patients having an open-wound and negative pressure therapy, two having V-Y-plasty, two being treated with direct wound closure, and two undergoing a new radial laser probe operation.
Table 2 shows the healing rate 2 months postoperatively. No statistically significant difference emerged between senior and junior surgeons regarding healing rates. The finding that 13 patients (15%) had a BMI of 30 or above did not reveal any influence on their healing rate when compared to that of patients with a BMI < 30. Gender did not affect healing rates. Non-drinking patients’ healing rate was poorer than that of patients who consumed at least one dose of alcohol weekly. A majority of the patients were non-smokers; among the 26 (30%) smokers, 17 (20%) were considered heavy smokers, at 10 or more cigarettes per day. Among the latter, the healing rate was poorer (76%) at follow-up 2 months postoperatively than for non-smokers (88%), but not statistically significantly.
Pilonidal surgery healing rate at 2 months postoperatively.
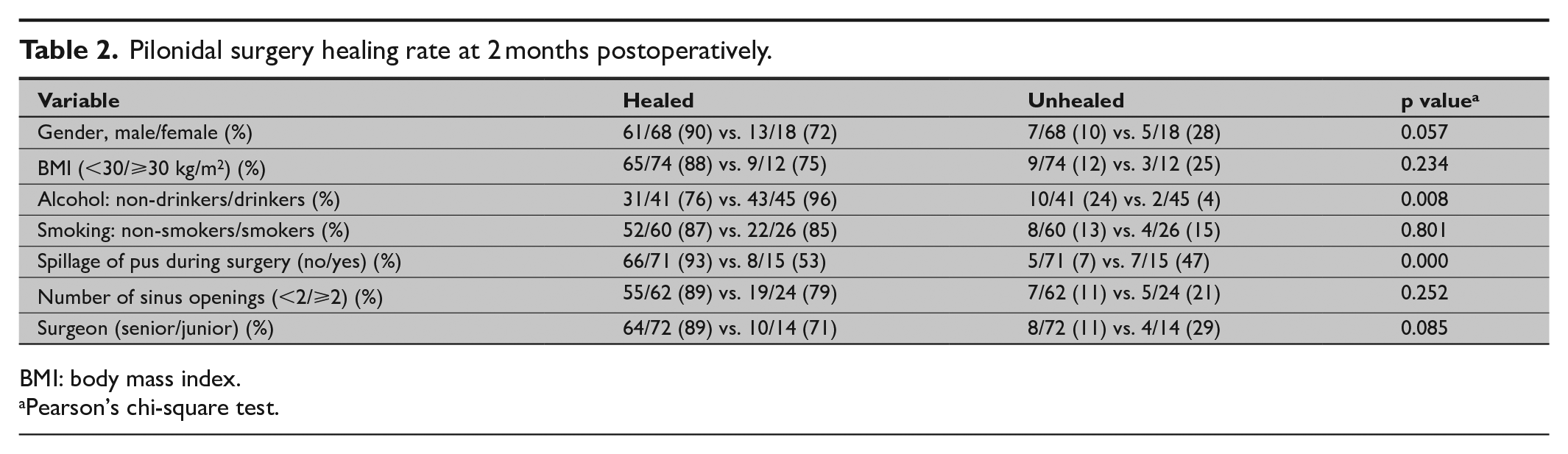
BMI: body mass index.
Pearson’s chi-square test.
Discussion
In earlier radial laser probe studies13 –16, the healing rate has been around 90%. In our study, a similar 86% healed during follow-up. The radial laser probe procedure is easy to learn and in most cases possible to perform under local anesthesia on a day-surgery basis. Postoperative recovery is short, and long sick leaves can be avoided, an important benefit, since most patients are young adults of working age.
Many differing techniques are reported of for pilonidal disease treatment. Open-wound treatment, direct wound closure, and different kinds of flap techniques often require a long recovery time and a long sick leave.5 –9 For a simple pilonidal sinus, it is unnecessary to perform surgery requiring a long recovery.
The radial laser probe procedure was a new method in our hospital, so to start, we had no exact data on the length of sick leave that would prove adequate. Our median sick leave lasted 12 days. At the follow-up visit taking place at 2 months, many patients reported having been ready to return to normal activities in only a few days following surgery, which is in line with previous findings.14,16
Non-drinking patients had statistically worse healing rates than did drinkers. The reason for this is unclear. A search of the literature did not reveal any explanations. The small number of patients in this study together with slightly more patients with intraoperative spillage of pus in the non-drinking group (22% vs. 13%) may partially explain this finding.
Smoking and obesity are generally considered risk factors in surgery, although this is still controversial in pilonidal sinus surgery. Al-Khayat et al. 17 retrospectively analyzed 94 patients with pilonidal disease undergoing excision and primary closure. In their study, both obesity and smoking were associated with an unacceptably high postoperative infection rate compared with that of non-smokers; smoking and obesity in that study were both independent risk factors for wound infection. In another retrospective study, smoking was a significant risk factor for postoperative wound infection after Karydakis flap and “pit-picking” surgery. 18 However, Sievert et al. 19 in their retrospective study among members of the German military undergoing excision of pilonidal disease with open-wound or primary closure found neither smoking nor obesity to be risk factors. Previous laser probe studies failed to report on smoking or obesity.13–16 In our study, with a majority of the patients being non-smokers, no difference in wound healing emerged between smokers and non-smokers. Among heavy smokers, however, the healing rate was lower than for non-smokers, a difference not statistically significant. The small number of patients in our study may explain why smoking, as a risk factor, did not reach statistical significance. Nor did obesity influence wound healing, with only 13 (15%) patients being obese (BMI > 30). One explanation may be our small number of obese patients.
There are two major limitations to this study, namely the small number of patients as well the retrospective nature of this study. However, our results show that the healing rate was 53% among patients when spillage of pus occurred during surgery, whereas the healing rate was 93% when there was no spillage of pus during surgery. This indicates that a radial laser probe procedure is most appropriate for simple pilonidal sinuses. And also, this finding is useful when planning prospective randomized studies to evaluate this new method more thoroughly.
Conclusion
The radial laser probe operation seems to be a suitable method to cure pilonidal disease, with good recovery rates and only a few recurrences. This operation is possible to perform under local anesthesia, in most cases on a day-surgery basis, and the recovery time is short. Complicated cases with acute pus spillage seem, however, unsuitable for this kind of surgery. To determine which minimally invasive method is the best for pilonidal disease would require randomized prospective studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.