
Abstract
Background and objective:
In 2014 we introduced percutaneous internal ring suture as an alternative to open surgery for the treatment of inguinal hernia. This study aims to evaluate the introduction of the procedure at our institution.
Methods:
In total, 100 consecutive patients operated with percutaneous internal ring suture were compared with 100 consecutive patients operated with open surgery. The patients were operated from August 2014 until November 2017. Patient demographics, clinical history, operative time, time in theater, and postoperative complications were extracted from charts.
Results:
The mean operative time for percutaneous internal ring suture was 26.54 min and for open surgery 39.94 min, P < 0.0001. The total mean operative theater time for percutaneous internal ring suture was 108.95 min and for open surgery 118.4 min, P = 0.0343. During follow-up, two percutaneous internal ring sutures were operated for recurrent hernia. In the open surgery-group, three patients were operated for recurrent hernia, three for secondary testicular retention, and three for metachronous contralateral hernia.
Conclusions:
Even when established as a new technique, the percutaneous internal ring suture procedure is safe and results in shorter operative time and shorter theater time compared to open surgery.
Introduction
Inguinal hernia is one of the most common surgical conditions to occur during infancy, with a reported incidence between 0.8% and 5% 1 . The risk is higher in preterm infants 2 . The most common reason for children to develop a clinical inguinal hernia is a patent processus vaginalis (PPV) or canal of Nuck, leading to the development of a lateral/indirect inguinal hernia 3 . Medial/direct or femoral hernias are clinical rarities in the pediatric population and only occur in 1%–2% in reported series4, 5.
Pediatric surgeons have historically performed open surgery (OS) with excision or closure of the hernial sac as the treatment for inguinal hernia. Since the advent of laparoscopic surgery and advances in the size of laparoscopic instruments, several laparoscopic techniques have been proposed for the treatment of inguinal hernias in the pediatric population. The main arguments for using a laparoscopic approach is to reduce the risk of contralateral metachronous hernias as well as minimizing the risk of secondary testicular complications (iatrogenic ascent and testicular atrophy) 6 . Initially, laparoscopic repair was done in intraperitoneal manner, however, a trend toward higher hernia recurrence risk was observed 7 . An international survey suggests that the pediatric surgical community favors the open approach for unilateral inguinal hernia repair 8 . In 2006, Patkowski et al 9 described the extraperitoneal percutaneous internal ring suture (PIRS)-method with extracorporeal suturing of the internal ring. Extraperitoneal laparoscopically assisted suturing of the internal ring has proven to have a small risk of recurrence as well as being cosmetically acceptable, since it only involves an incision in the umbilicus 10 . In 2014 we introduced the PIRS-technique in our institution.
This study aims to evaluate the introduction of the PIRS-technique at our department regarding perioperative and postoperative complications, operative time, time consumption in theater, and discuss costs associated with the procedure.
Materials and Methods
Patients
The operative registry at the Division of Pediatric Surgery at Uppsala University Hospital was reviewed for our first 100 consecutive patients operated with PIRS-technique. The period involved August 2014 until November 2017. The operative registry was then searched in retrospect for patients operated with open surgical technique for inguinal hernia from November 2017 until 100 consecutive patients were identified. These patients were operated during the period January 2016 until November 2017. The 100 identified patients operated with OS were defined as the control group. As this was a retrospective study no randomization of patients was done.
The operative registry and the charts of these 200 patients were assessed in a structured manner extracting sex, age, weight, preoperative findings, surgeon, operative time, total time the operative theater was occupied, peri- and post-operative complications as well as reoperations. To make sure no reoperations at other hospitals were missed the patients’ electronical national charts were reviewed. During this assessment, it was found that one patient in the control group had several other procedures during the same anesthesia and was thus excluded from the study. Clinical follow-up time was 6 months postoperatively. No patients were lost to follow-up.
The groups differed preoperatively statistically in sex distribution, weight, and recurrent hernia as indication for surgery. The reason for this was that when introducing the PIRS-technique, somewhat older patients were selected as well as patients with recurrent hernias and females. During the PIRS-procedures, 17 PPVs were identified and operated at the same time. This increased the number of bilateral hernias operated in the PIRS-group from 18 to 35 compared to 11 in the open group. The demographic data for all patients can be found in Table 1.
Demographic and perioperative data for all patients, a P-value < 0.05 was deemed significant and is labeled with an * and bold font.
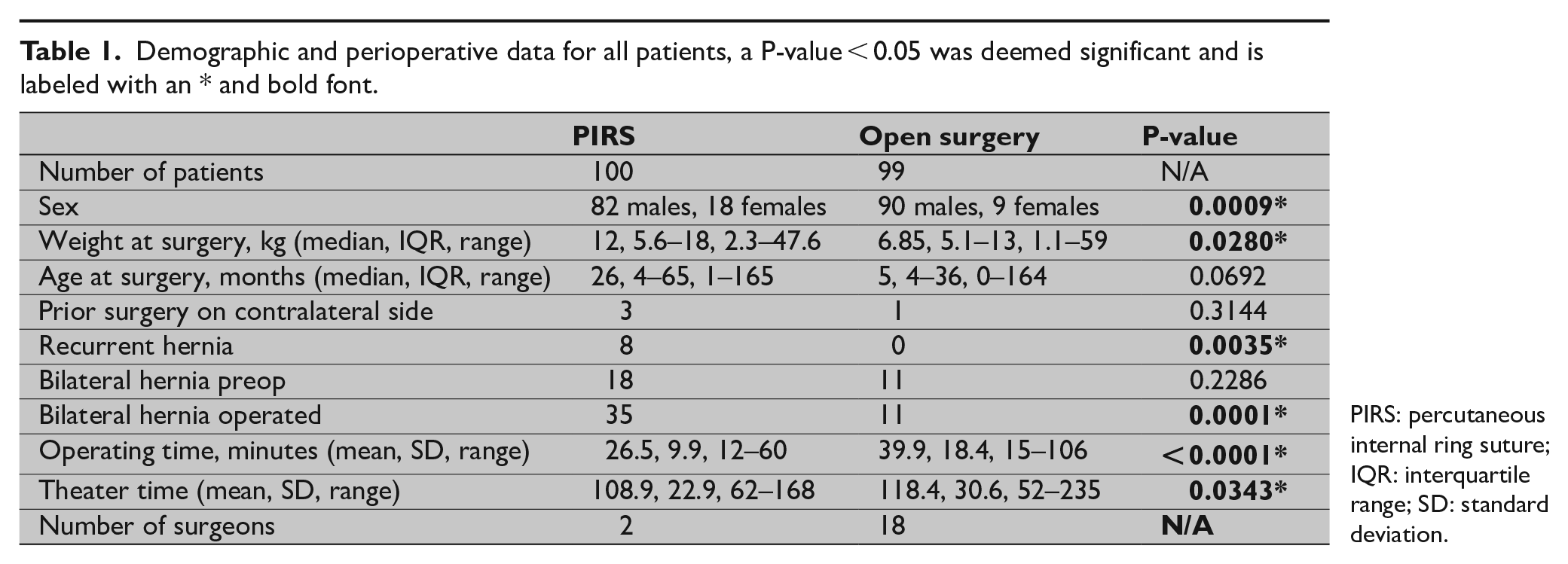
PIRS: percutaneous internal ring suture; IQR: interquartile range; SD: standard deviation.
Surgical Technique, PIRS
The procedure was performed under general anesthesia. Pneumoperitoneum was established using an open technique through the umbilicus and a 5-mm trocar was placed. A 1-mm incision was then made with a nr 11 scalpel just above the inner opening of the inguinal canal. Under laparoscopic-guided vision a 22-gauge spinal needle with a 3:0 polypropylene suture passing within the needle returning outside to create a loop was introduced from the lateral side at the internal ring, continuing pre-peritoneally under laparoscopic vision. Special care was taken to avoid injury to the spermatic cord and testicular vessels while catching the peritoneum all the way from a 12 o’clock position to the 8 o’clock position in right sided operations, leaving the loop in situ. The needle was removed and reintroduced with a solitary 3:0 polypropylene suture from the 12 o’clock position advancing pre-peritoneally to the 8 o’clock position counter clockwise to encircle the complete inguinal ring, threading the solitary suture through the previously introduced loop. The loop was then removed, fetching the solitary suture which is subsequently tied extracorporeally, closing the internal ring under laparoscopic control. In left sided operations, initial advancement was done from 12 o’clock to 4 o’clock counter clockwise, followed by advancement from 12 o’clock to 4 o’clock clockwise. Fascial closure at the umbilicus was done using polyglactin thread. Skin closure was performed using either histoacryl adhesive or absorbable intracuticular suture. In three cases, an additional 5-mm trocar was placed to manipulate bowels that obstructed the view.
Two surgeons (first and last author) were primary operators during these procedures. Both are specialists in pediatric surgery.
Surgical Technique, Open Surgery
The procedure was performed under general anesthesia. An incision was placed over the external opening of the inguinal canal. The funicle was identified and mobilized up into the wound. The hernial sac was thereafter identified and separated from the vas deferens and testicular vessels. The sac was dissected free from surrounding structures under tension and then suture ligated using polyglactine thread. The inguinal canal was not opened. If the sac was large it was partially resected, if small it was wholly resected. The subcutis was then adapted with resorbable suture and the cutis closed with intracuticular suture or histoacryl adhesive. If a contralateral hernia had been noted preoperatively, a similar procedure was performed on that side as well.
Eighteen different surgeons were primary operators during the open procedures (including the surgeons also performing PIRS). Twelve procedures were performed by specialists in general surgery and eight by pediatric surgeons in training. At all these procedures a specialist in pediatric surgery was present. The 79 remaining procedures were performed by specialists in pediatric surgery.
Ethical Considerations
The study was approved by the Regional Ethical Committee at Uppsala University, Uppsala, Sweden, dnr 2018/042. The approval did not require individual patient/family consent since the study was based on register data.
Statistical Methods
Data were examined for normality by plotting histograms. Values are presented as mean (standard deviation (SD)) when distributed according to normality and median (interquartile range (IQR)) when not distributed according to normality. Two-tailed Fisher’s exact test was used to compare proportions. The Mann–Whitney U-test was used for unpaired comparisons. A P-value of less than 0.05 was considered statistically significant. Statistica 13.2 software (Dell; Tulsa, OK, USA) was used for the statistical analyses.
Power calculation showed that each group needed to include at least 50 patients to be powered to show differences in theater time of 10 min. With 100 patients in each group the study was sufficient in size.
Results
Operative Findings, Operative Time, and Theater Time for All Patients
In 17 PIRS-procedures, a contralateral patent inguinal canal was found and subsequently closed, raising the number of bilateral operations in the PIRS-group to 35. The mean operative time was 26.5 (SD 9.9) min for PIRS and 39.9 (SD 18.4) min for OS (P = 0.0000). The mean theater time for PIRS was 108.9 (SD 22.9) min and for OS 118.4 (SD 30.6) min (P = 0.0343). See Table 1 for details.
Operative Findings, Operative Time, and Theater Time in Relation to Male Sex
In male patients, a contralateral patent inguinal canal was found and subsequently closed in 10 PIRS-procedures, increasing the number of bilateral operations in the PIRS-group to 23 in comparison to 11 in the open group.
The mean operative time was 26.1 (SD 8.9) min for PIRS and 41.2 (SD 18.6) min for OS (P < 0.0001). The mean theater time for PIRS was 108.1 (SD 20.4) min and for OS 118.4 (30.6) min (P = 0.0343). See Table 2 for details.
Demographics and perioperative data for all male patients, a P-value < 0.05 was deemed significant and is labeled with an * and bold font.
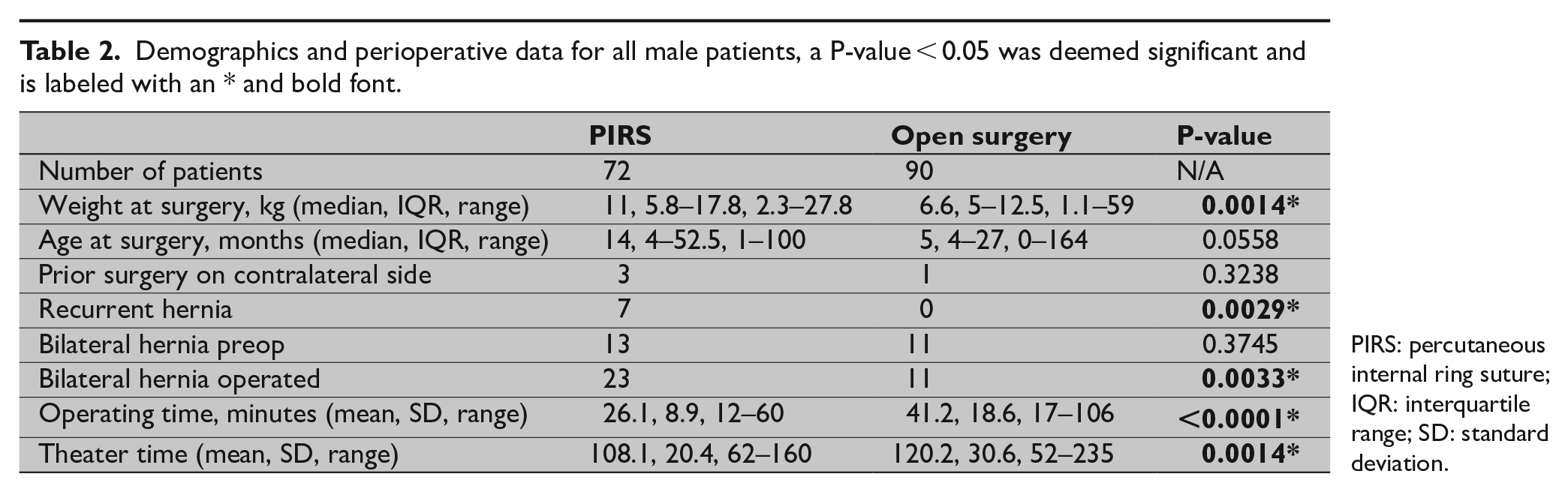
PIRS: percutaneous internal ring suture; IQR: interquartile range; SD: standard deviation.
Operative Findings, Operative Time, and Theater Time in Relation to Female Sex
In female patients, a contralateral patent inguinal canal was found and subsequently closed in seven of the PIRS-procedures, increasing the number of bilateral operations in the PIRS-group to 12. None of the females operated with OS had bilateral hernias.
The mean operative time was 27.8 (SD 12.6) min for PIRS and 27.4 (SD 12.3) min for OS (P = 0.9859). The mean theater time for PIRS was 112.4 (SD 28.2) min and for OS 100.78 (SD 27) min (P = 0.3758). See Table 3 for details.
Demographics and perioperative data for all female patients, a P-value < 0.05 was deemed significant and is labeled with an *and bold font.
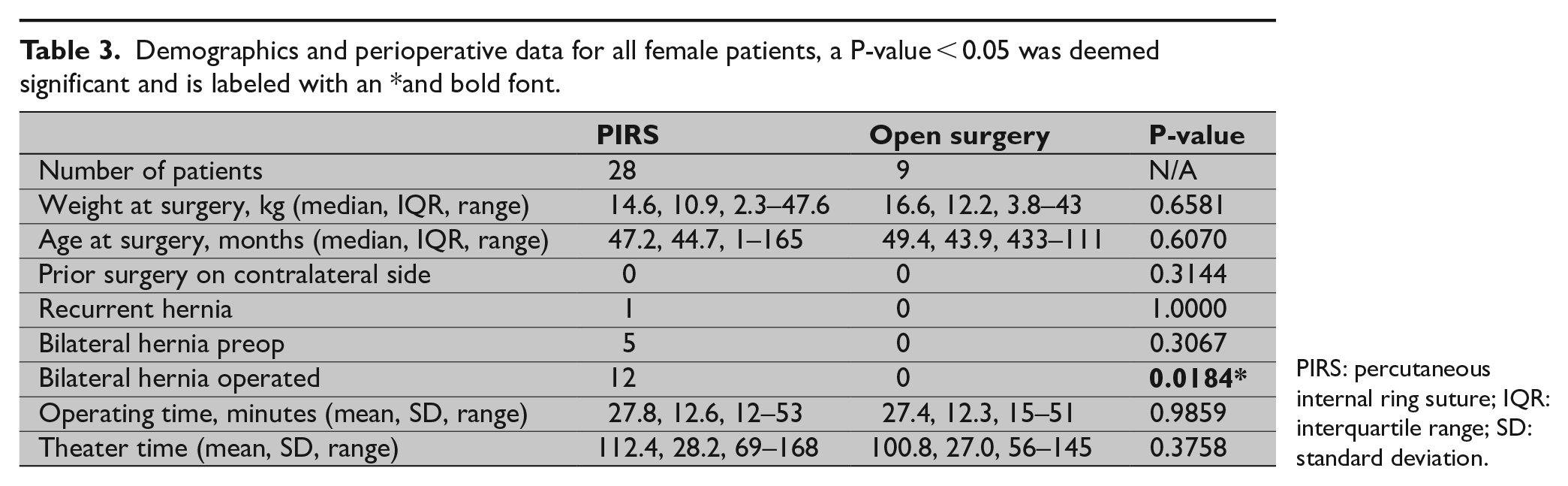
PIRS: percutaneous internal ring suture; IQR: interquartile range; SD: standard deviation.
Operative Time and Theater Time in Relation to Bilateral Hernias
Twenty-nine patients were diagnosed with bilateral hernias preoperatively and a total of 46 patients were operated when including the 17 contralateral PPVs that were diagnosed and operated during PIRS-procedures.
The mean operative time for patients with preoperatively diagnosed bilateral hernias was 31.79 min for PIRS and 71.55 min for OS (P < 0.0001). The mean theater time for PIRS was 117.06 min and for OS 146.72 min (P = 0.0700).
The mean operative time for all patients operated bilaterally (including contralateral PPV) was 32.3 min for PIRS (P < 0.0001). The mean theater time for PIRS was 118.2 min and for OS 146.72 min (P = 0.0295).
Perioperative Complications
No perioperative complications occurred in either group.
Postoperative Complications and Need for Reoperation
During the follow-up time period, two PIRS were operated for recurrent hernia. In the OS group, three patients were operated for recurrent hernia, three have been scheduled for operation of secondary testicular retention, and three have been operated for metachronous hernia. Hence, two patients in the PIRS-group have needed reoperation in comparison of nine in the open group (P = 0.0322).
Discussion
In this study, the extraperitoneal approach of internal ring suturing using the PIRS method had shorter operative and theater time as well as having fewer complications than the traditional open surgical method.
The laparoscopic approach for inguinal hernia repair has previously been estimated to be marginally more expensive than the open approach in a study by Chan and colleagues (11), where laparoscopic intracorporeal suturing of internal ring was compared to OS. In a Japanese study, the laparoscopic approach was more expensive than traditional OS, however, in that study operative times were longer in the laparoscopic group and the surgical technique involved two ports and distinct laparoscopic instrumentation 12 . In this study, operative and theater times were shorter for PIRS-procedures compared to OS. PIRS utilizes fewer laparoscopic instruments than intracorporeal suturing and we often use our more than 10-year old 5-mm laparoscopes and our more than 15-year old laparoscopic rig for the PIRS-procedures. Hence, the cost of PIRS should be less than that of laparoscopic intracorporeal suturing. It is probably on par with, or even lower, than the cost of OS. The study was however not designed to specifically analyze the total costs of surgery and we refrain from further analysis of the economic aspect.
This study is a small and retrospective single-center study with limitations to be taken into consideration. Differences in patient demographics (sex, age, weight) are explained by initial patient selection toward older boys, girls, bilateral hernias, and recurrent hernias. Initially, the differences were more polarized, but during the course of the study period these differences were alleviated, and at the end of the period, patients down to a weight of 2.3 kg were operated with PIRS. Only two dedicated surgeons were primary operators on the PIRS-patients, whereas 18 different surgeons were the main operators in the open group. When looking at this one has to remember that the PIRS-group includes the whole learning curve of the two PIRS-surgeons whereas only 20 of the 99 open surgeries were performed by surgeons on their learning curve. The study was powered to look at the differences in OR- and theater time. It was not powered to look at differences in the occurrence of complications. Therefore, we only interpret the results regarding complications as an indication of that there were no obvious differences.
Considering aforementioned limitations, our study shows that introduction of the PIRS-technique under Swedish conditions seems safe. No perioperative complications occurred and the number of postoperative complications were less for the PIRS-group. PIRS also has the potential to save operating time, especially for patients with bilateral hernias. The operating time for female patients in our series was, however, similar between the two groups (keeping in mind that 12/28 were operated bilaterally in the PIRS-group) and one can therefore argue that there is a smaller gain for female patients being operated with PIRS. However, laparoscopy provides the possibility to examine the inner genitalia which diminishes the need for chromosome testing for female patients with bilateral hernias or hernial sacs where the ovaries have been noted.
The incidence of contralateral PPV at operation has been estimated to be 21%–47% as deduced from laparoscopic studies 7 . The overall incidence of metachronous contralateral inguinal hernia has been estimated to be 6%–7%, with risk factors being initial left sided hernia and contralateral PPV in children aged 0–19 years13, 14. About 25% of children with contralateral PPV developed metachronous inguinal hernia within 2 years in a prospective study by Koivusalo et al 15 , while the rate was 11% in the study by Maddox and Smith 16 . We opted to close all contralateral PPVs to minimize risk of metachronous inguinal hernias. The need for closure of asymptomatic PPVs remains controversial 17 . According to Kokorowski et al, three asymptomatic contralateral PPVs needed to be closed to prevent one metachronous inguinal hernia, while Wenk et al deduced that 17 contralateral inguinal explorations are needed to prevent one metachronous inguinal hernia13, 18. Long-term studies on the outcome of asymptomatic PPV closure are still lacking. Further studies are also warranted on whether the risks of complication of asymptomatic PPV closure outweigh the risks of additional surgery of contralateral metachronous hernia. Our decision to close the asymptomatic PPVs that we found during laparoscopy is therefore debatable.
Laparoscopic repair of inguinal hernias in children is an established proven method, with at least comparable results to traditional OS 17 . Randomized controlled trial (RCT) studies comparing laparoscopic to open techniques are relatively scarce in the literature and since the laparoscopic techniques vary slightly, direct conclusions regarding operative times and costs remain vague11, 15, 19 –21. In our hands, PIRS seems safe and required less operative-resources and had distinct advantages over OS.
In conclusion, the introduction of PIRS is safe and has the potential to save both operating time and theater time even under the surgeons’ learning curve.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Regional Ethical Committee at Uppsala University, Uppsala, Sweden, dnr 2018/042.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The ethical approval did not require individual patient/family consent since the study was based on register data.