
Abstract
Background and Aims:
Lateral-only Kirschner-wire pinning of supracondylar humerus fracture is superior in avoiding surgery-related ulnar nerve injury. Their disadvantageous effects on stability may be a consequence of inappropriate surgical techniques. We analyzed whether the surgeon’s preference for lateral-only fixation is associated with his or her orthopedic competence. We also analyzed the surgical technique–related risk factors of redisplacement.
Materials and Methods:
All children, aged <16 years, with a distal humerus fracture in 2000–2009 were preliminary included (N = 861). Altogether, 24 of the 165 type-3 supracondylar fractures were operated by lateral-only pinning. Loss of reduction in the follow-up was the main outcome, while the close characteristics of the surgical technique and treating surgeon’s orthopedic competence were the explanatory variables.
Results:
Orthopedic surgeons used lateral-only method in 23.5% of the type-3 fractures (N = 16/68), and other surgeons in 8.2% (N = 8/97)(difference = 15.3%, 95% confidence interval = 4.6%–27.6%, p = 0.005). One-third of the lateral-only treated fractures (29.2%, 95% confidence interval = 12.6%–51.1%) redisplaced. Lateral-entry pins that crossed at the level of the fracture were associated with failure (87.5%), while no patient with appropriate pin configuration failed (difference = 87.5%, 95% confidence interval = 52.1%–97.8%). A shorter distance (<5 mm) between the entry points of the pins was associated with redisplacement (80% vs. 15.8%, difference = 64.2%, 95% confidence interval = 16.1%–86.9%). Open reduction (p = 0.07), insufficient (<4 mm) bone contact (p = 0.28), monocortical pins (p = 0.569), low diverging angle (p = 0.13) or parallel pins (p = 1.0), residual coronal displacement (p = 1.0), >5° changed Bauman angle (p = 0.11), rotational displacement (p = 0.25), and the experience or specialty of the surgeon were not associated with redisplacement.
Conclusion:
Lateral-only pins resulted in poor stability in one in three of the patients. Appropriate configuration of the pins was associated with good fracture healing, but crossing the pins at the fracture level and introducing them close to each other were associated with redisplacement. Surgeons with more orthopedic competence selected lateral-only fixation more usually.
Keywords
Introduction
Supracondylar humerus fractures are the most common type of elbow fractures, and there is a risk of long-term sequelae and treatment-related complications (1–3). One in three of them show completely displaced type-3 fracture, according to Gartland–Wilkins Classification (4). Kirschner-wire pinning in connection with closed reduction is the preferred method of treatment (5, 6). However, many recent studies have focused on surgical techniques to determine whether both medial and lateral cross pinning or lateral-only pinning is more effective (7). Due to its superiority in preventing surgery-related ulnar nerve injury, lateral-only pinning has been suggested as the preferred method by many (7–10). The incidence of ulnar nerve injury is 3%–6%, but up to 15% has been reported in connection to cross pinning (11–15).
The main disadvantage of lateral-only pinning is its poorer stability (16–18), while 40% less rotational stability and a two-fold higher probability of later carrying angle deformity have been found compared to cross pinning (14, 19). This is important because changed alignment and decreased motions of the elbow are in particular the main reasons for poor outcomes in the long term (2): Supracondylar humerus fractures are the childhood fractures that most frequently result in compensation claims for complications in Finland (1). Nevertheless, some surgeons have suspected that techniques used in lateral-only pinning are usually less acceptable when judged by current recommendations (14, 20). Introducing the lateral Kirschner wires in a divergent configuration may add the stability (21). Furthermore, maximal stability would be reached by positioning the pins far away from each other, achieving sufficient bone contact in both fracture fragments, and using bicortical instead of monocortical pins (22, 23). The educational background of the treating surgeon may also affect the outcomes, while less complications were found when completely displaced type-3 fractures were operated by orthopedic surgeons (24). Furthermore, Vallila et al. (1) reported lower risk of complications in those distal humerus fractures that had been treated in university hospitals instead of regional hospitals.
In this study, we focused on type-3 fractures and their lateral-only fixation and aimed to analyze the occurrence of redisplacement and the potential association of surgery-related factors (surgical technique) and surgeon-related factors (the experience and specialty of the surgeon) with redisplacement. We also aimed to evaluate whether the lateral-only method was selected based on the surgeon’s preference or other reasons.
Material and Methods
A population-based study was conducted in the geographic catchment area of Oulu University Hospital, Finland, over a 10-year period (2000–2009). There are no other pediatric trauma units in the area, and the study was thought to be inclusive. In the study period, supracondylar humerus fractures were operatively treated in the study center by pediatric surgeons and pediatric or adult orthopedic surgeons. Furthermore, some isolated cases were operated on by other surgeons after-hours during their on-call shift. Far advanced residents of pediatric surgery or orthopedics have occasionally operated childhood trauma patients independently during their on-call shift. The International Classification of Diseases (ICD) version 10 was used to identify all children aged <16 years with the diagnosis code S42.4 (N = 861). All primary radiographs of the children were comprehensively re-reviewed to find out supracondylar humerus fractures (N = 565). Altogether, 195 (34.5%) of them show type-3 fractures, and 24 were treated by means of lateral-only pinning (12.3%). Thirty type-3 fractures were treated non-operatively by closed reduction and casting, while 141 fractures were surgically fixed with medial and lateral crossing pins and, therefore, excluded from the study. However, before exclusion and in order to evaluate the potential effect of surgical specialty on selecting lateral-only fixation instead of crossing medial and lateral fixation, the educational background of surgeons of those 141 patients who were treated by crossing medial and lateral pinning was assessed.
The mean age of patients with type-3 fracture, who were treated by crossing pins, was 7.4 years (SD = 2.7), while the mean age of those treated with lateral-only pinning was 6.7 years (SD = 2.7) (p = 0.21). There were no open fractures among the lateral-only fixed patients, compared with two open fractures in patients treated by crossing pins (p = 1.0). The selection of the patients to lateral-only or crossing lateral and medial pinning was primarily based on the decision of the treating surgeon, and there was no recommended treatment protocol whether to fix with lateral-only or medial and lateral pins. The potential reason that the surgeon selected the lateral-only method was reviewed in operation notes. The association of the surgical specialty on the performed surgical procedure was analyzed in two groups: first, the surgeons who were involved in orthopedics in their daily work (pediatric and adult orthopedic surgeons) and, second, those who were not involved in orthopedics in their daily work (pediatric surgeons and other surgeons). The residents were respectively classified into these two groups, according to their specialization program; there was no difference in the rate of residents versus consultants in these two surgical specialty groups (p = 0.561).
Most fractures included in the study (N = 18, 75.0%) were on the left side. There were 13 boys and 11 girls. None of them had a specific preoperative neurological or circulation defect. None showed forearm compartment syndrome. Six had massive hematoma. The most common cause of injury was fall from >1 m (66.7%, N = 16). Seven (29.2%) had fallen from <1 m, and one was an unspecific injury. Among the injuries due to recreational activities, one-third were trampoline-related (N = 8, 33.3%). Horseback riding resulted in two injuries (8.3%). Fourteen cases were injured during an unspecified activity. Most of the injuries occurred outdoors (N = 19, 79.2%) (Table 1).
The characteristics of the patients, injuries, reduction and surgical technique of the patients <16 years of age with a type-3 supracondylar humerus fracture, treated by lateral-only pinning (N = 24).
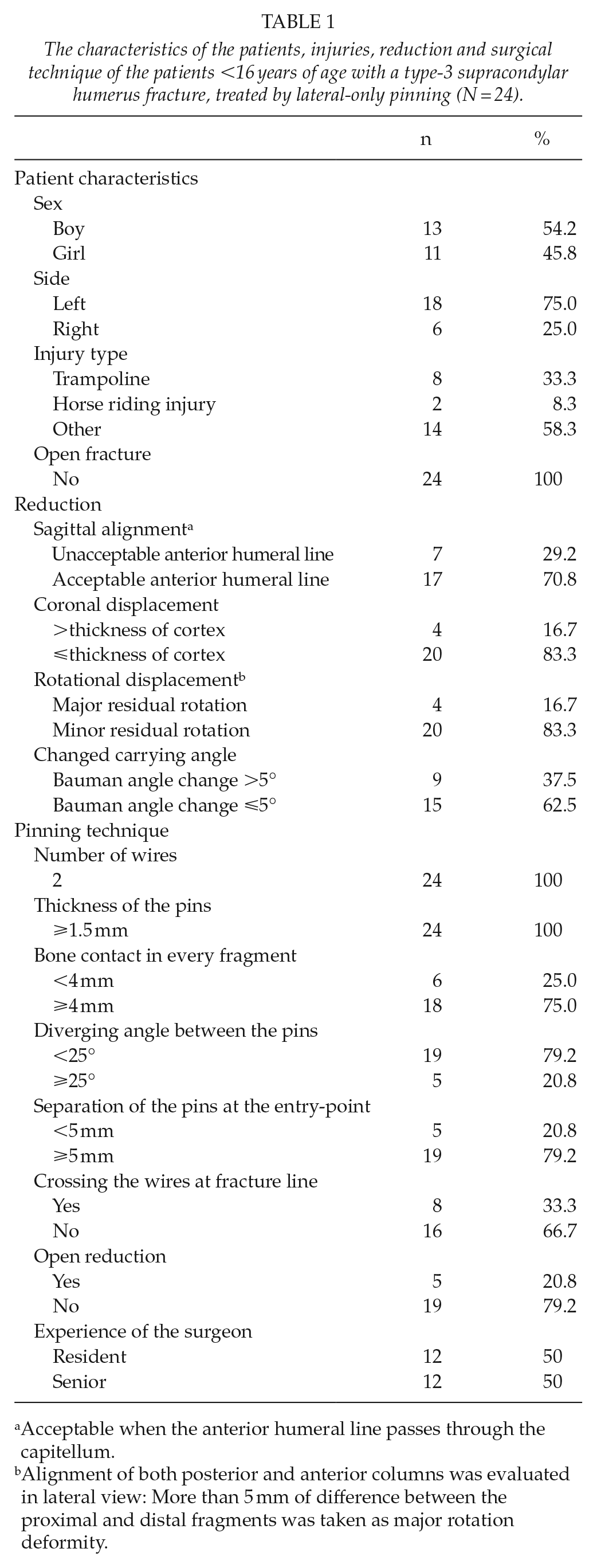
Acceptable when the anterior humeral line passes through the capitellum.
Alignment of both posterior and anterior columns was evaluated in lateral view: More than 5 mm of difference between the proximal and distal fragments was taken as major rotation deformity.
Radiographs were systematically re-reviewed, and surgical techniques used in the primary operations were comprehensively analyzed. The number of Kirschner wires was determined. Wire thickness (in millimeters) was measured in radiographs or collected from operating room charts. There were no calibration measures in most radiographs, and therefore, <1.5 mm versus ⩾1.5 mm was compared, appreciating the inaccuracy in measuring. The distance between the entry points of the pins at the level of bone tissue was gaged in millimeters. The angle between the pins was measured in degrees. A divergent angle greater than 25° was considered the minimum satisfactory configuration. Completely parallel wires were analyzed separately. Crossing the pins at the fracture level within the distance of <2 mm was considered biomechanically insufficient (22). Sufficient bone contact (⩾4 mm) around the pins at any fragment was determined. Bicortical fixation was appreciated over the monocortical fixation, and all wires not penetrating the medial humeral cortex were considered monocortical (25). Crossing the olecranon fossa with a pin was determined to be allowable and not documented separately (25). An acceptable reduction in perioperative fluoroscopy prints or radiographs taken immediately postoperatively was determined as follows: The anterior humeral line was required to pass through the middle-third of the capitellum in the lateral projection. Coronal plane displacement greater than a thickness of a single bone cortex and Bauman angle change >±5° were regarded as unacceptable, while 72° was set as the reference (26). Rotation was categorized as acceptable when both anterior and posterior columns were aligned in the lateral view. However, a certain amount of malrotation is generally accepted because there is considerable rotation movement in the shoulder (20). Therefore, a difference of >5 mm or more than two thicknesses of the humerus cortex was considered disproportionate (26) (Fig. 1). The operating surgeon’s experience level (i.e. resident vs. consultant) and the surgical specialty (pediatric or adult orthopedists vs. pediatric or other surgeons) were reviewed. Despite the quality of reduction, any change in reduction during follow-up was considered to indicate insufficient stability and set as the main outcome variable (redisplacement: yes/no).
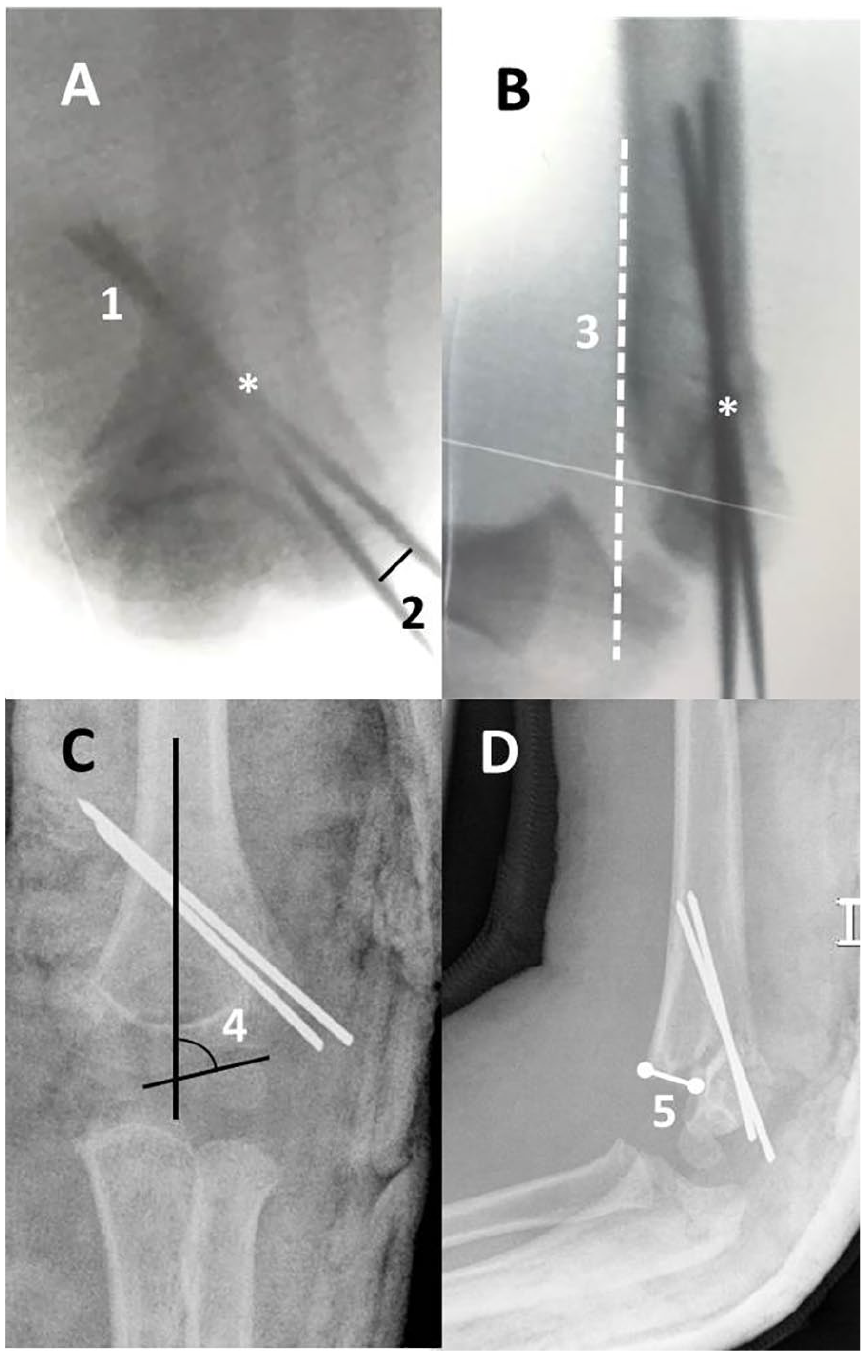
A, B) The figure demonstrates a 5-year-old boy who suffered from a type-3 supracondylar humerus fracture that was fixed by percutaneous lateral-only Kirschner-wire pinning. C, D) The reduction was lost in the follow-up. The white star points out that the pins were crossing just at the level of the fracture line. The white “1” refers the bicortical fixation, while both pins penetrate the rear cortex. “2” shows the separation of the entry points of the pins. “3” is the anterior humeral line that should pass through the capitellum. “4” is the Bauman angle, and “5” is the disproportion of fracture fragments as measured in the lateral view and indicates the rotational deformity.
Statistical Analysis
The occurrence of loss of reduction was calculated. The effect of surgeons’ professional education, experience, and surgical techniques on stability was compared in two groups: redisplacement versus no redisplacement. The results were presented proportionally with a 95% confidence interval (95% CI) for differences and analyzed using the standard normal deviate (SND) test to determine the difference of proportions of independent variables. A Student’s t test was used to test the differences in mean ages and immobilization times between two groups. The mean, range, and SD were reported for continuous variables. Logistic regression was used to calculate the effect of shorter distance between the pins at the entry point and crossing the pins at the fracture line on the stability of fixation. Statistical analyses were carried out using IBM SPSS Statistics software version 25 (IBM Corp., Armonk, NY) and StatsDirect software version 2.7.9 (StatsDirect Ltd., England). All p-values were two-tailed, and the threshold of statistical significance was set at p < 0.05.
Ethical Aspects
Institutional approval for the study was obtained in advance: The patients were not contacted during the study, and no ethical board evaluation was required.
Results
Preceding Factors of Lateral-Only Fixation
There were 24 type-3 supracondylar humerus fractures that were treated by means of lateral-only fixation. For comparison, crossing medial and lateral pin fixation was used in 141 type-3 fractures. Pediatric or adult orthopedists operated on 68 type-3 fractures and used lateral-only procedure in 16 (23.5%) of them. Pediatric and other surgeons treated altogether 97 patients and used lateral-only method in 8 patients (8.2%) (difference = 15.3%, 95% CI = 4.6%–27.6%, p = 0.005).
In almost all of the patients (83.3%, N = 20/24), lateral-only procedure had been the primary intention, according to the surgeons preference. Only in four isolated cases, lateral-only fixation had been the secondary option, and unplanned selected during the operation: In three cases, crossing medial and lateral fixation was first performed, but the pins were immediately removed and lateral pins were inserted in the same operation; in one case, two lateral and one medial Kirschner wires were first planned, but due to satisfactory stability of the first two lateral pins, no more medial fixation was performed.
Occurrence of Redisplacement
One-third of lateral-only fixed type-3 supracondylar humerus fractures redisplaced (29.2%, 95% CI = 12.6%–51.1%). Four were on the left side, and three on the right side (p = 0.300). Four of the patients were boys, and three were girls (p = 0.659).
Acceptable Reduction
Most fractures (N = 19, 79.2%) were reduced in an anatomic or acceptable position. One in five (20.8%) were surgically fixed in inferior reduction but were still not associated with redisplacement (p = 0.126). Most (N = 19, 79.2%) were reduced by closed means, and five required open reduction.
Details of the Surgical Technique
All fractures were fixed with two pins that were ⩾1.5 mm thick. One-third (N = 8, 33.3%) of the fractures were fixed by inserting the pins in a divergent configuration. Most pins were invergent (58.3%, N = 14), and in two cases, they were parallel. The mean angle between the diverging pins was 19.0° (SD = 15.9°), and 12.9° (SD = 8.1°) in inverging pins. In 33.3% of the cases, the pins crossed at the level of the fracture. The mean pin separation at the fracture line was 4.5 mm (range = 0–16 mm, SD = 4.1 mm). The mean separation of the pins was 6.8 mm (range = 3.0–12.0 mm, SD = 2.3 mm) at the lateral cortices and 14.0 mm (range = 0–44.0 mm, SD = 13.3 mm) at the medial cortex.
The Association of Surgery-Related and Surgeon-Related Factors with Redisplacement
All but one (N = 7/8, 87.5%) of the lateral-only fixed cases with pins crossing at the level of the fracture (N = 7) failed. In turn, all but one (N = 16/17) among those with good pin configuration remained stable, while only one (N = 1/17, 5.9%) redisplaced. All redisplaced fractures (N = 7/7, 100%) were fixed by crossing the pins at the fracture (difference = 94.1%, 95% CI = 55.3%–99.0%, p < 0.001). Crossing the pins at the fracture level significantly increased the risk of redisplacement (95% CI of Odds Ratio (OR) 5–39,202, p = 0.007). A shorter distance (< 5 mm) between the entry points of the two pins also was associated with redisplacement when compared to those with longer distances (57.1% vs. 5.9%, difference = 51.2%, 95% CI = 13.9%–80.5%, p = 0.008). Close entry-points increased the risk of redisplacement (95% CI of the OR 2–263, p = 0.017).
Insufficient (<4 mm) bone contact at the fracture fragments (p = 0.172), monocortical instead of bicortical pins (p = 0.569), a low diverging angle between the pins (p = 0.367) or even parallel pins (p = 1.0), residual displacement on the coronal plane (p = 1.0), a changed Bauman angle (p = 0.430), and residual rotational displacement (p = 0.25) were not associated with redisplacement. There was no gender difference in the redisplacement rate (p = 0.13). The fractured elbows were immobilized with an above-the-elbow cast for a mean of 29 days in the redisplacement group (SD = 1.5 days), compared to 28 days in the reference group (SD = 0.8) (p = 0.639) (TABLE 2).
Unstable surgical fixation determined by changed reduction in the follow-up, analyzed by reduction and surgical technique characteristics (N = 24).
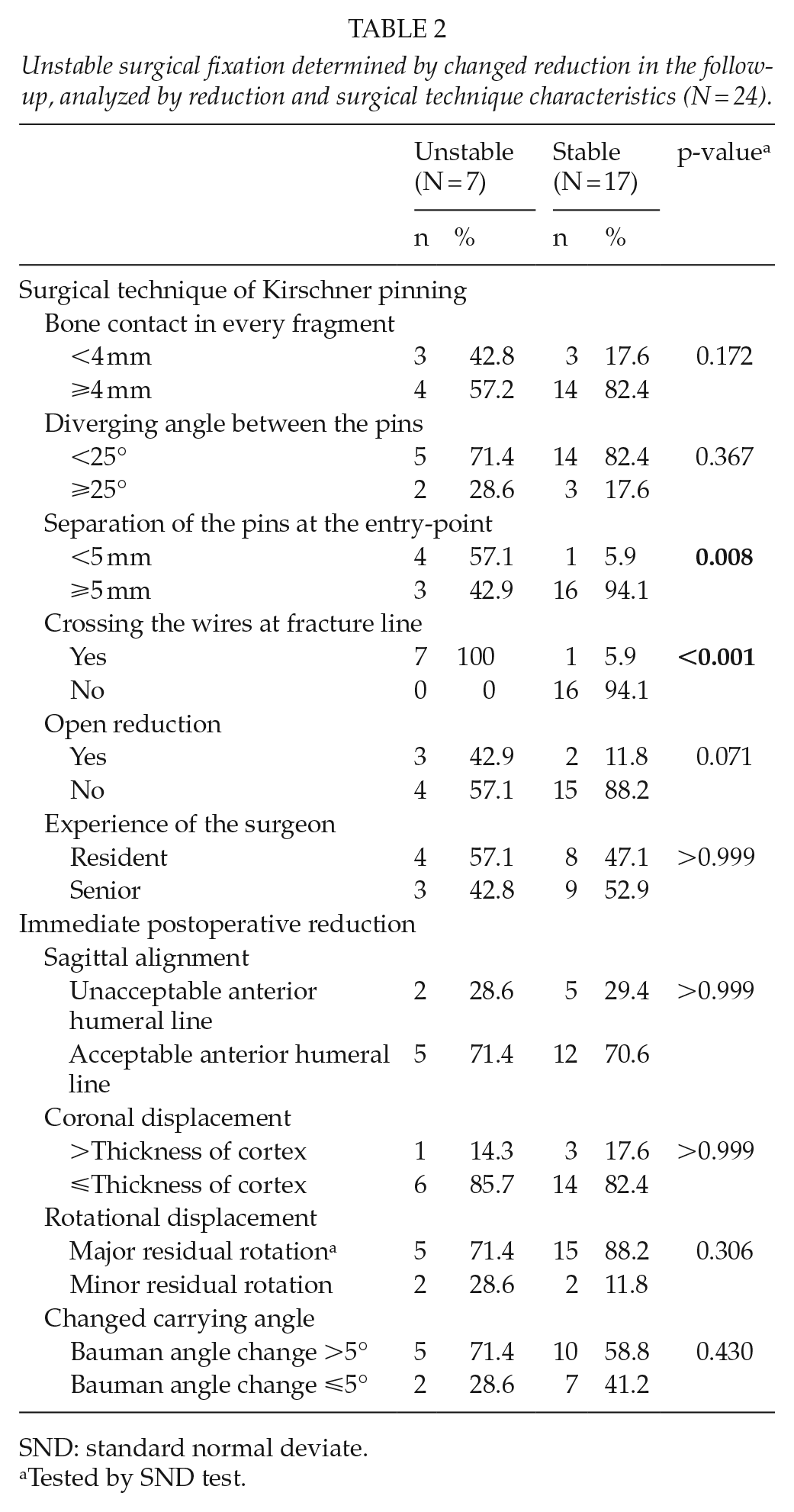
SND: standard normal deviate.
Tested by SND test.
In this study, redisplacement was seen in 37.5% of the patients (3/8) treated by pediatric or other surgeons, compared with 25.0% (4/16) of the cases treated by pediatric or adult orthopedists (difference = 12.5%, 95% CI = –24.0% to 50.6%, p = 0.407). The expertise of the operating surgeon (resident vs. consultant) was not associated with redisplacement (p = 1.0).
Reoperation
The occurrence of reoperation was 12.5% (N = 3). Of those who had lateral-only inserted pins that crossed at the fracture line, 37.5% required reoperation. In turn, none of the 16 patients with adequate pin separation at the fracture level required reoperation (p = 0.009).
Discussion
There is no agreement about lateral-only pinning in treating unstable type-3 supracondylar humerus fractures. In this comprehensive population-based study, we found that approximately one-third (29.2%) of lateral-only fixed type-3 fractures lost reduction. Such a high rate of fixation failure would be alarming in any fracture or patient group. The issue is particularly important in children population, while the incidence of supracondylar fractures has increased by 30% since 2000 (27), and their in-hospital treatment is increasing (28). Nevertheless, the poor stability found in this study was not surprising; lateral-only pinning has been reported to be 40% weaker biomechanically when compared with crossing medial and lateral pinning (19).
It was previously suggested that limitations in surgical techniques explain the poor stability of lateral-only pinning (29). We found a high rate of faults in techniques in general, when compared with the current recommendations: Crossing the pins at the fracture line, which is cautioned against, was usual (33.3%), and one in five (20.8%) had a poor divergent angle between the pins (<25°). One in four showed incomplete (<5 mm) bone contact around the fracture. We found that crossing the pins at the fracture level and introducing the pins too close to each other were associated with redisplacement. These two were very important findings of the study; in particular, crossing the pins at the fracture line should never be accepted. The mechanical support is weak when fixating pins are close to each other; in particular, torsional moment is minimally resisted when the implants cross just in the fracture. For comparison, none of the type-3 fractures fixed appropriately using two lateral-only pins that did not cross at the fracture level lost reduction. As an advantage, we found no short-term ulnar nerve complications when lateral-only pinning was used, which is in agreement with the literature (8, 10, 12, 26).
In this research, we found that lateral-only procedure was usually chosen by the preference of the treating surgeon, without some special reason. We also found that the surgeons who are familiarized with orthopedics in their own office-hour works more usually selected lateral-only fixation, compared to the surgeons whose expertise was not within orthopedics. This sounds reasonable, while it is technically more difficult to reach satisfactory stability by using lateral-only method; this may have prevented other surgeons to choose lateral-only fixation, while medial and lateral crossing fixation is easier to be performed, and biomechanically stronger. However, accepting that lateral-only fixation is weaker, we still found in this inclusive study that there was no redisplacement if the lateral-only pins were appropriately inserted. Furthermore, there were no surgery-related ulnar nerve injuries in lateral-only operations. In a recent research, Saarinen and Helenius (24) reported less lateral-only fixation but better outcomes among orthopedic surgeons. We found no difference in redisplacement between the groups of surgeons; however, the study settings and hospital circumstances are different, and the findings are not straight comparable. In general, satisfactory stability is always a minimum requirement in orthopedics, and there may be several methods to achieve it; faultless medial and lateral fixation is undoubtedly better than technically deficient lateral-only fixation, which associated with complications in this research.
The population-based setting was strength of the study: All patients with a distal humerus fracture were preliminarily included. There was a recognized number (N = 861) of cases in the geographic catchment area during the study period (2000–2009). They all were reviewed, and radiographs of the primary treatment, as well as follow-up postoperative radiographs, were available for all cases. This study focused on the technical characteristics of lateral-only treatment, and no comparison of treatment methods was in the study plan; however, subgroup analyses of baseline characteristics were performed between the type-3 cases who were treated with lateral-only (N = 24, 14.5%) versus crossing medial and lateral pins (N = 141, 85.5%) to evaluate the selection of the patients. There were no statistically significant differences in patient age (7.4 years in the crossing medial and lateral pins group vs. 6.7 years in the lateral-only pins group; p = 0.21) or injury severity (two open fractures vs. no open fractures, respectively, p = 1.0) between these treatment groups: Albeit not being randomly selected population regarding lateral-only pinning, we conclude that the study cohort is representative of the normal child population that suffered type-3 supracondylar fractures in this region during the study period. Furthermore, among other baseline characteristics, the orthopedic competence of operating surgeons was evaluated of all operatively treated type-3 fractures in order to further describe lateral-only fixation. As strength, any redisplacement was considered as a certain sign of instability. Reoperation was analyzed but not considered the primary outcome due to indications for reoperation are heterogeneous.
The retrospective nature of the study is a limitation. However, the aim was to evaluate of effect of substandard treatment on the stability of type-3 fractures, and a randomized trial of such technical deficiencies cannot be performed. The treating physician decided between lateral-only and traditional pinning for each patient. It is possible that lateral-only pinning was performed still more often but failed instantly, and a conversion to cross pinning occurred during the same operation: These potential cases were not reached to the study due to recoding the operation in the registry according to the final procedure. We also understand that the final study population was not large, despite the 10-year study period; 861 distal humerus fracture cases were preliminarily reviewed, but a minority of them met the criteria.
Conclusion
Surgeons with more orthopedic competence used lateral-only fixation more frequently. Appropriate configuration of the pins was associated with good fracture healing, but crossing the pins at the fracture level and introducing them close to each other were associated with redisplacement. These technical limitations should never be accepted in unstable type-3 supracondylar humerus fractures.
Footnotes
Acknowledgements
Alma and K.A. Snellman Foundation, Vasa Foundation of Physicians, Finska Läkaresällskapet, Foundation of Pediatric Research, and Emil Aaltonen Foundation have supported the study.
Author Contributions
J.H. has contributed in data collecting, analyzing, and writing; T.P. has contributed in statistics and writing; W.S. has contributed in reviewing the article; and J.-J.S. was initiative to the study and has contributed in all.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.