
Abstract
Objective:
Arteriosclerotic disease of the common femoral artery can be treated by surgical or endovascular intervention. Elderly patients are said to have a worse outcome if treated by surgical means; however, data to support this theory are missing.
Methods:
Retrospective analysis of all patients who underwent common femoral artery endarterectomy between March 2007 and July 2018 in our clinic. Group 1 included all patients <80 years and Group 2 included all patients ⩾80 years. Endpoints were patency rates, limb salvage, and overall survival.
Results:
During this time period, 977 common femoral artery endarterectomies were performed. Indication was claudication in 61.5% and critical limb ischemia in 38.5%. Group 1 included 805 cases (82.4%) and Group 2 included 172 cases (17.6%). Thirty-day mortality was 2.7% (Group 1 = 1.6% versus Group 2 = 7.6%; p < 0.001) and 30-day major amputation was 1.1% (Group 1 = 0.7% versus Group 2 = 2.9%; p = .043). Primary patency and secondary patency were 84.2% and 96.8%, respectively, after 7 years. Limb salvage (93.7%, Group 1 = 94.1% versus Group 2 = 91.8%; p = .088) and overall survival (52.0%, Group 1 = 59.1% versus Group 2 = 15.7%; p = .006) were significantly different after the same time period. Multivariable analysis showed female gender to be a risk factor for loss of primary patency. Age ⩾ 80 years and ulcer or gangrene were risk factors for death. Statin use was beneficial to survival.
Conclusions:
Common femoral artery endarterectomy is a safe procedure with excellent long-term results. Octogenarians have an increased risk for perioperative mortality and major amputation.
Keywords
Introduction
Common femoral artery endarterectomy (CFAe) is a well-established therapy to treat peripheral artery disease. Previous studies have demonstrated good short-term and mid-term patency rates1 –8. However, long-term results have been infrequently published. Moreover, the number of patients who were included in these reports is small. Only one study by two high-volume centers presented long-term data, including a representative number of patients 9 . The results of elderly patients were not analyzed in their report and remain still unclear. A current database analysis done by Siracuse et al. 1 confirmed the safety of endarterectomy in the majority of patients. In contrast, Nguyen et al. 10 concluded that endarterectomy is not a safe treatment, and patients should be selected carefully. There continues to be a relevant literature gap on CFAe. In addition, there is an ongoing debate regarding the treatment of the common femoral artery fueled by the advances in endovascular therapy. Advertised benefits are lower mortality and morbidity and a high technical success in endovascular treatment11,12.
The goal of this cohort study was to provide data on long-term efficiency of surgical treatment in common femoral artery lesions, especially in elderly patients. We hypothesized that octogenarians have similar results compared to younger patients.
Methods
We performed a retrospective analysis of all patients who underwent CFAe with patch in our hospital between March 2007 and July 2018. Patients who received CFAe in combination with bypass surgery or patients who had previous bypass surgery in which the common femoral artery was used for anastomosis were excluded. Previous CFAe and puncture of the common femoral artery for endovascular therapy of the aortoiliac or peripheral arteries, as well as coronary artery intervention were not exclusion criteria. Hybrid procedures comprising CFAe and endovascular treatment of the inflow or outflow vessels were also included. Data were documented by two vascular surgeons and one study nurse into a study database. The study was approved by the local ethics committee.
Only patients with clinical symptoms (claudication or critical limb ischemia) were treated. They received a duplex scan and a magnetic resonance angiography or computed tomography angiography before surgery. In some cases, digital subtraction angiography (DSA) was done via the contralateral common femoral artery or the brachial artery. A significant common femoral artery lesion was defined as a peak systolic velocity (PSV) greater than 2.5 m/s in the duplex scan and a diameter reduction of a minimum of 50% in the preoperative imaging. The surgical procedure was performed in a standard technique. In three cases, patients received regional anesthesia; in all other cases, general anesthesia was done. Through a lateral approach, the common femoral artery and the femoral bifurcation were exposed. Before clamping, the patients received 5000 IE heparin. When necessary, endarterectomy of the common femoral artery, the deep femoral artery, and the superficial artery was done simultaneously. Following endarterectomy, we routinely used bovine patches. In some cases, patches out of greater saphenous veins or occluded superficial artery were used. The surgeon decided what kind of patch material was used. If the preoperative diagnostics showed a stenosis or an occlusion of the iliac artery, the lesion was treated by endovascular means in combination with CFAe. In cases of critical limb ischemia, peripheral vessel lesions were treated additionally. A completion angiogram was performed before wound closure to evaluate the reconstruction. A duplex scan was performed before discharge and 6 months after the operation. If there were no signs of restenosis, patients were examined in 1-year intervals or event-based when clinical symptoms reappeared. All patients received an antiplatelet therapy after the operation (Aspirin 100 mg). If the patients had an indication for anticoagulation, they received aspirin and phenprocoumon.
Early results included morbidity and mortality within the first 30 days. Study endpoints were primary patency, limb salvage, and overall survival. They were defined according to Rutherford et al. 13 . Group 1 included all patients <80 years, and Group 2 included all patients ⩾80 years.
Statistical Analysis
Data are presented as mean ± standard deviation (SD) for continuous data and as absolute and relative frequencies for categorical data. Comparisons between both groups (<80 years versus ⩾80 years) were done using Student’s t-test or Pearson’s chi-squared test of independence, respectively.
Median follow-up was assessed by the reverse Kaplan–Meier method of overall survival (OS). OS was defined from the operation to death by any cause. OS was analyzed by the Kaplan–Meier method. Cumulative incidence function (CIF) of loss of primary patency, loss of secondary patency, or loss of limb salvage was computed using the competing risk analysis with death as a competing event. Uni- and multivariable Cox proportional hazards regression models were used to assess the association between OS and age and several further predictor variables. Hazard ratios (HR) and 95% confidence intervals were calculated. Fine and Gray’s proportional subdistribution hazards regression models were used to estimate the subdistribution hazard ratios (sHR) for all predictor variables on the remaining endpoints with death as a competing risk. The R software version 3.5.3 (The R Foundation for Statistical Computing) was used for statistical analyses using the following packages: tableone, cmprsk, timereg, riskRegression, currentSurvivial, and cr17.
Results
Overall, 863 patients were enrolled and underwent 977 common femoral artery endarterectomies during this time period. Both sides were treated in 114 patients. Out of these 977 limbs, 46 had a previous CFAe in a different hospital. Due to hemodynamic restenosis and recurrent clinical symptoms, patients had to undergo CFAe again. Indication was claudication in 601 cases (61.5%) and critical limb ischemia in 376 cases (38.5%). The median follow-up was 4.5 years. The complete follow
Patient characteristics and indication.
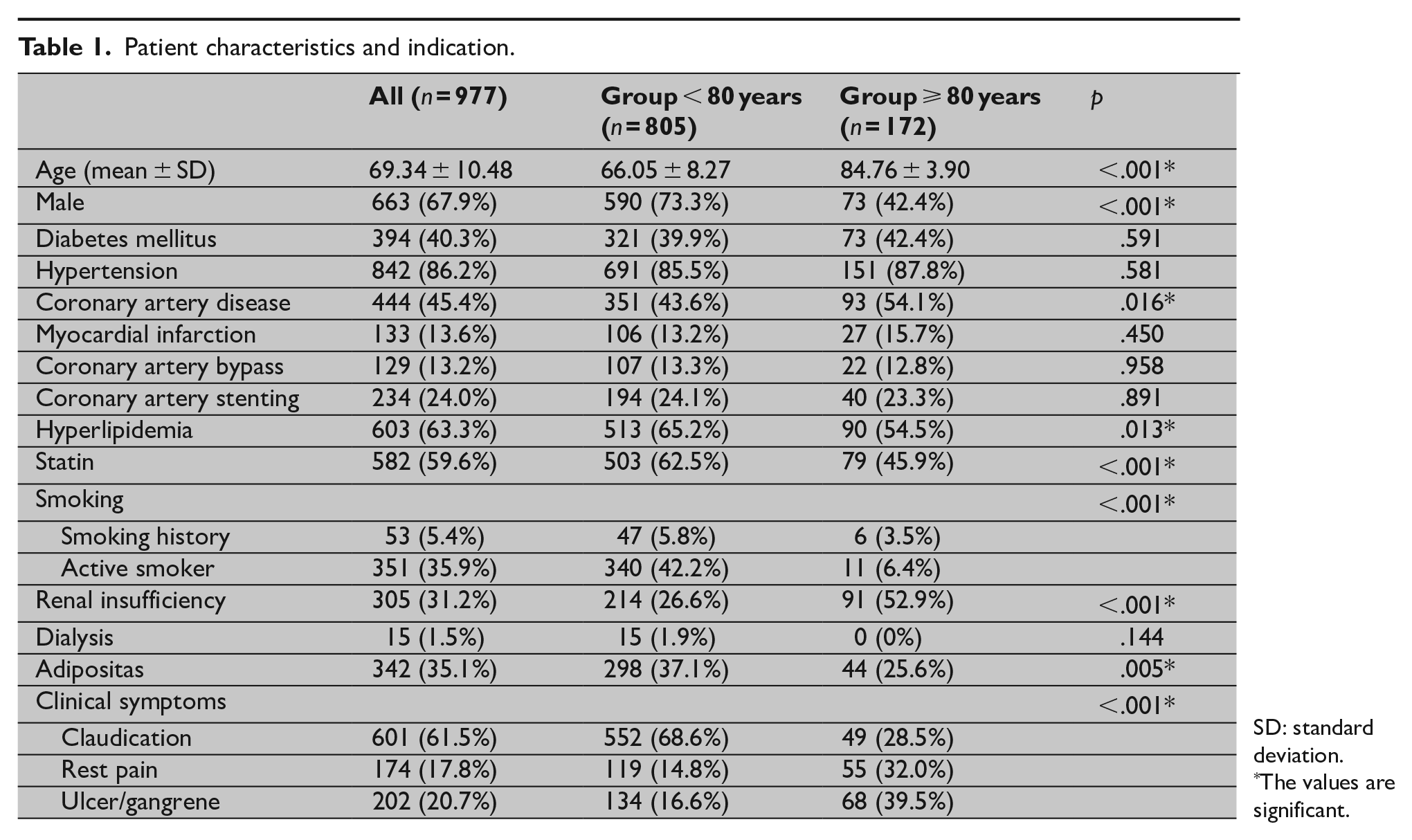
SD: standard deviation.
The values are significant.
Isolated endarterectomies and hybrid procedures were performed in both groups. Significantly more cases out of Group 1 received endarterectomy and endovascular therapy of the iliac arteries. Significantly more cases out of Group 2 underwent endarterectomy in combination with peripheral endovascular treatment. A bovine patch was used in most cases: direct closure of the artery without a patch was never done. The median operation time was 130 min without a statistical difference between the groups (Group 1 = 130 min versus Group 2 = 127 min; p = .551). The operative details are shown in Table 2, and the technical success was 100%.
Operative data.
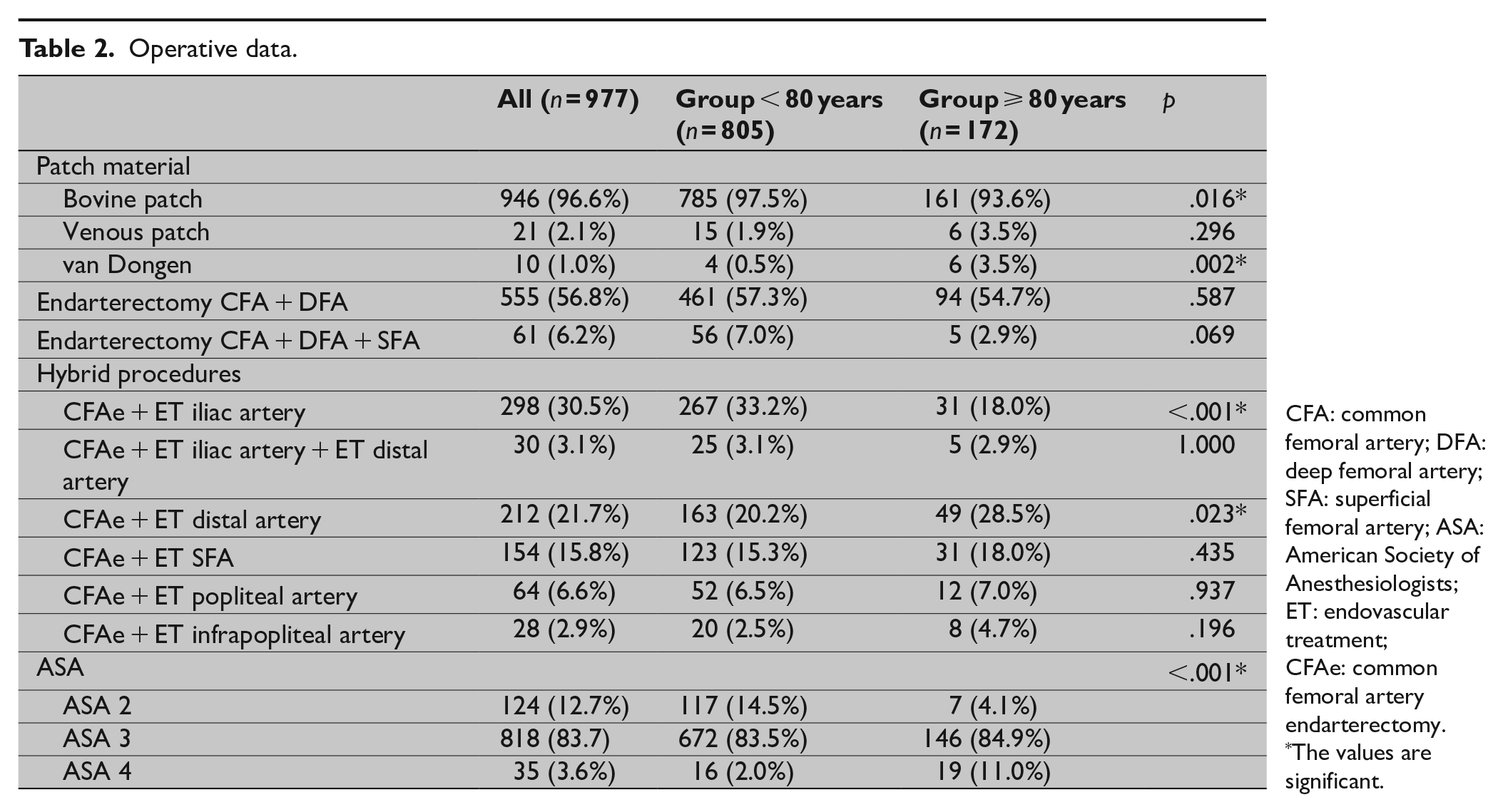
CFA: common femoral artery; DFA: deep femoral artery; SFA: superficial femoral artery; ASA: American Society of Anesthesiologists; ET: endovascular treatment; CFAe: common femoral artery endarterectomy.
The values are significant.
Thirty-Day Results
Thirty-day mortality was 2.7% (Group 1 = 1.6% versus Group 2 = 7.6%; p < .001). Out of these 26 cases, the source of death was heart failure (n = 7), pneumonia (n = 3), stroke (n = 1), and multiple organ failure (n = 9). In six cases, the cause of death was not related to the operation (cancer, mesenteric ischemia, and cirrhosis). A major amputation was required in 1.1% (11 cases). Indication for amputation was an extensive gangrene of the extremity. The outflow was impossible to improve in these patients. An acute bleeding complication with a need for surgical revision was seen in 15 cases (1.5%), without a significant difference between the groups. An early wound infection occurred in eight cases (0.8%; Group 1 = 0.4% versus Group 2 = 2.9%, p = .004). The median hospital stay was 7 days (Group 1 = 7 days versus Group 2 = 9 days, p < .001). The mortality and morbidity data are shown in Table 3.
Thirty-day mortality and morbidity.
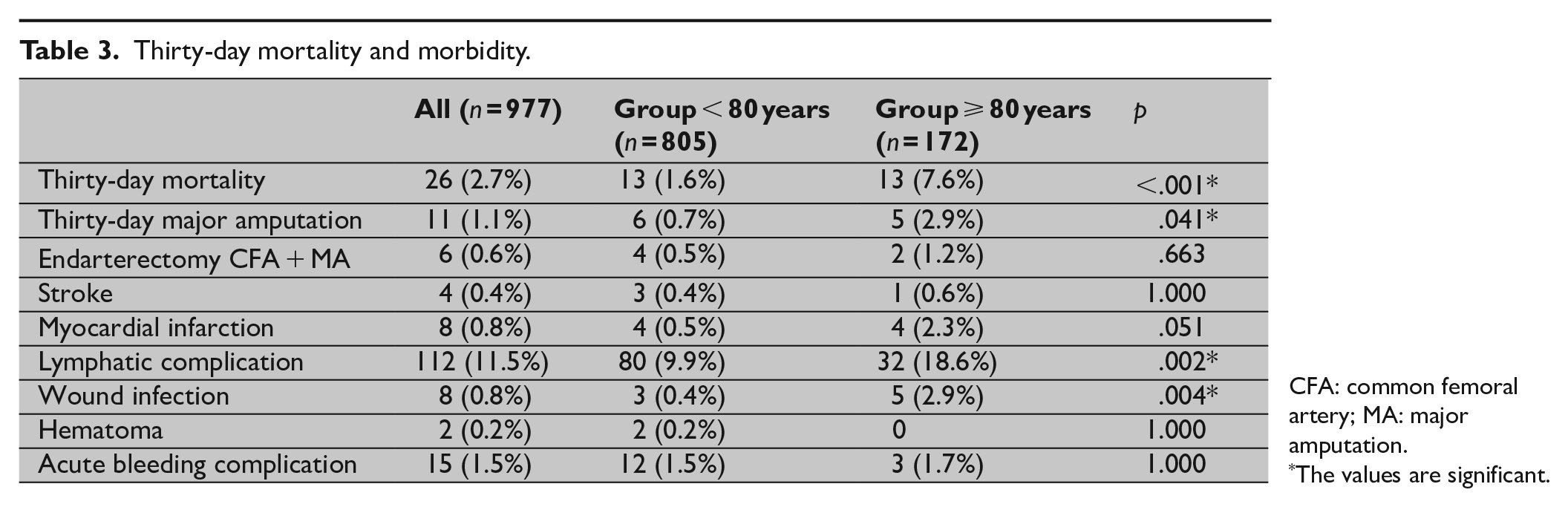
CFA: common femoral artery; MA: major amputation.
The values are significant.
Long-Term Results
Seven years after operation, the primary patency was 84.2% (Group 1 = 83.3% versus Group 2 = 88.8%, p = .052; Fig. 1) and the secondary patency was 96.8% (Group 1 = 96.6% versus Group 2 = 97.9%, p < .001), respectively. Limb salvage was 93.7% (Group 1 = 94.1% versus Group 2 = 91.8%, p = .088; Fig. 2), and overall survival was 52.0% (Group 1 = 59.1% versus Group 2 = 15.7%, p = .006; Fig. 3), respectively. A degeneration of the common femoral artery to an aneurysm was seen in three cases (0.3%) during the observation period. The artery was replaced by a prosthetic graft. A restenosis was seen in 31 cases (3.2%) and was treated by re-endarterectomy in 28 cases. In the remaining three cases, a re-endarterectomy was not possible and a prosthetic graft was performed. In addition, 92 bypass grafts with a common femoral artery anastomosis were necessary during the follow-up due to progress of peripheral arterial occlusion disease.
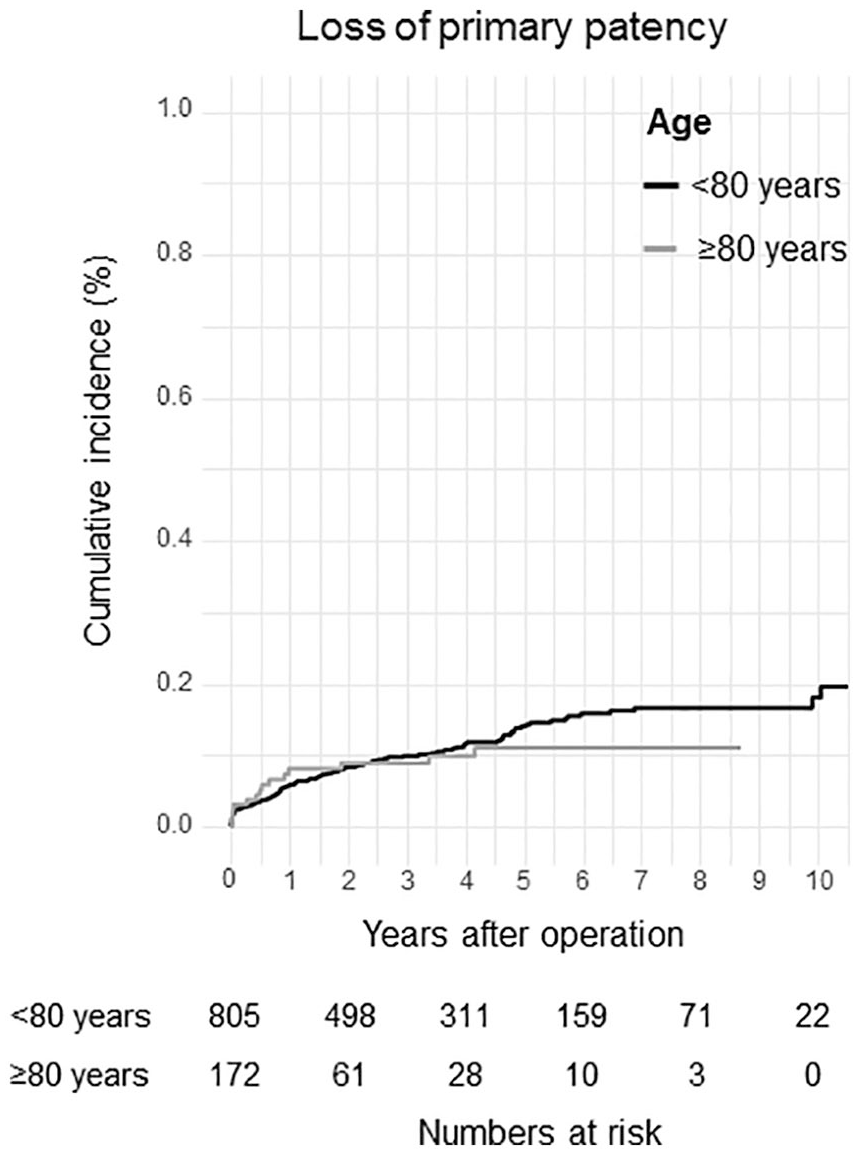
Loss of primary patency.
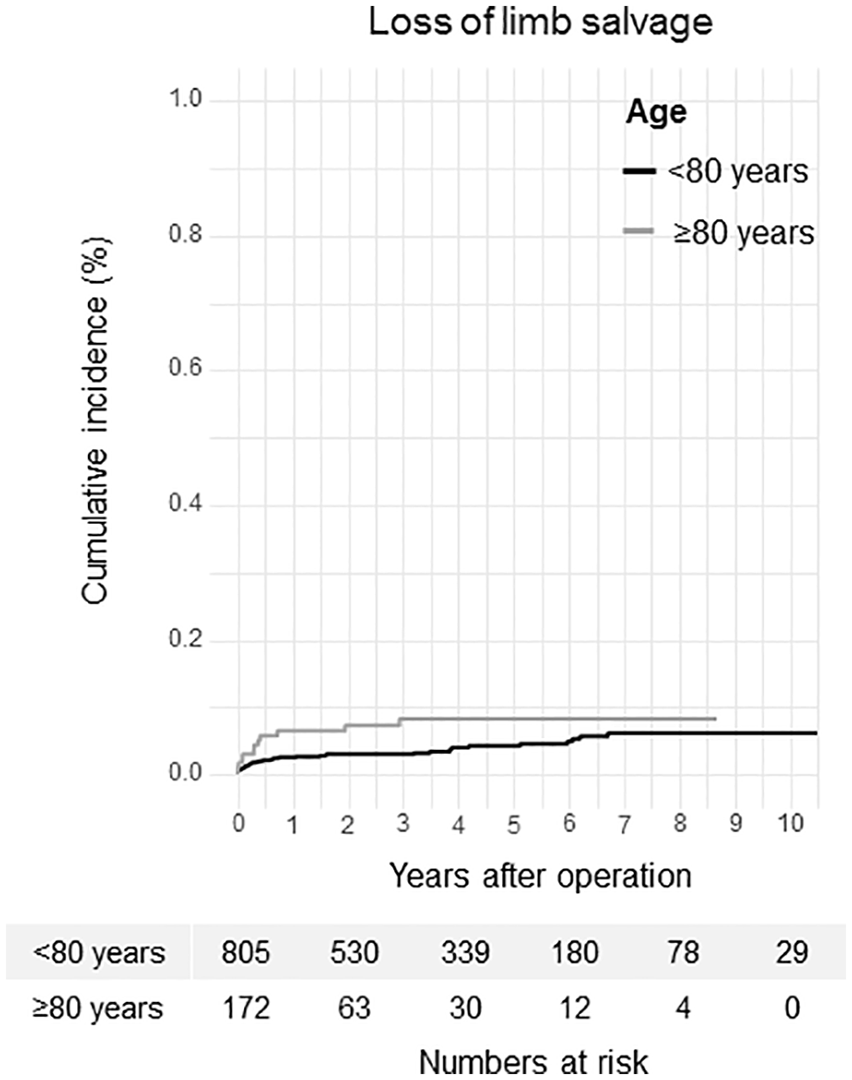
Loss of limb salvage.
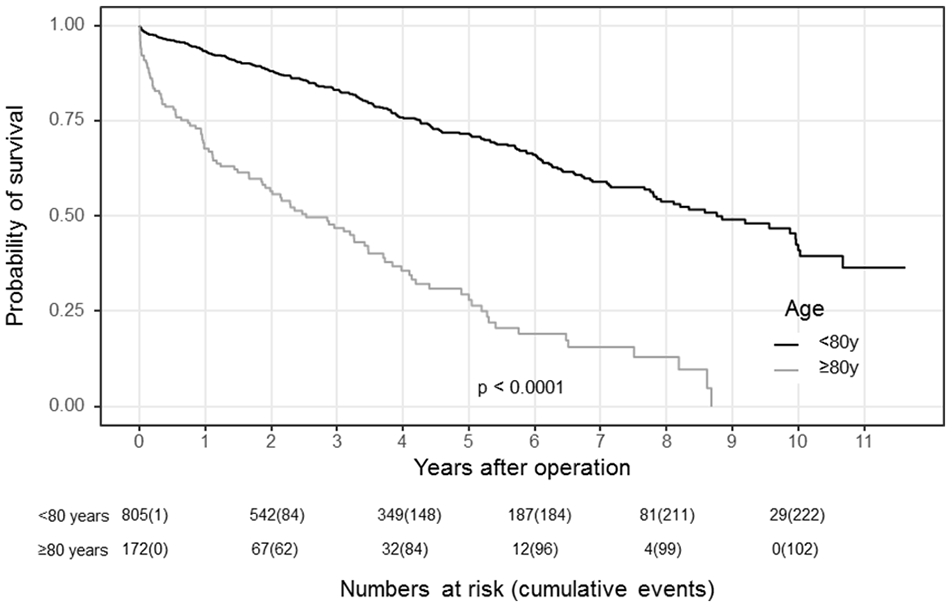
Probability of survival.
In the univariate analysis, female gender (sHR 1.61 (1.12–2.38); p = .011) was the only risk factor for loss of primary patency. Ulcer or gangrene (sHR 16.36 (7.33–36.51); p < .001), renal insufficiency (sHR 2.54 (1.42–4.53); p = .002), and dialysis (sHR 4.53 (1.41–14.54); p = .011) were risk factors for limb loss. Age > 80 years (HR 4.12 (3.24–5.23); p < .001), rest pain (HR 2.48 (1.88–3.27); p < .001), ulcer or gangrene (HR 3.59 (2.79–4.63); p < .001), coronary artery disease (HR 1.45 (1.17–1.81); p = .001), renal insufficiency (HR 2.18 (1.74–2.72); p < .001), and dialysis (HR 2.64 (1.40–4.95); p = .003) were associated with an increased risk for death, whereas the statin use (HR 0.68 (0.54–0.84); p < .001) was protective of survival. In the multivariate analysis, female gender (sHR 1.85 (1.12–2.78); p = .003) was the only risk factor for primary patency again, whereas ulcer or gangrene (sHR 13.96 (5.75–33.93); p < .001) was the only risk factor for major amputation. Age > 80 years (HR 2.22 (1.66–2.97); p < .001), rest pain (HR 1.96 (1.46–2.64); p < .001), and ulcer or gangrene (HR 2.06 (1.52–2.79); p < .001) were risk factors for death. Again, the statin use was beneficial (HR 0.71 (0.55–0.92); p = .009) to survival.
Discussion
The safety and efficacy of CFAe is described in previous studies4,8,9,14. To our knowledge, this study is one of the largest single-center series on CFAe and confirms the results of these reports.
The overall perioperative mortality was similar to that described in the literature 15 . However, octogenarians had a significantly increased mortality compared to younger patients in our study. Nguyen et al. 10 in their report described six independent predictors for perioperative death, in which age was one of the predictors. Ballotta et al. 7 reported a perioperative mortality of 0% after CFAe. All endarterectomies were done under regional anesthesia. They concluded that maybe the smaller risk of this kind of anesthesia and a quick surgery was related to their results. Kang et al. 14 also reported a perioperative mortality of 0%; they used regional or local anesthesia in nearly two-thirds of their patients. However, the patient cohort was limited in both studies, and our operation time was similar. Endovascular therapy of the common femoral artery promises a low early mortality compared to surgical treatments 12 . A database analysis including over 1000 patients who were treated by endovascular means showed a mortality of 1.6% within the first 30 days 16 . The German CRITISCH Registry showed no difference in mortality between octogenarians and younger patients after endovascular therapy 17 . An analysis of the literature and our recent results shows that age seems to have an influence on mortality, even in patients treated by surgery. Despite a predominant use of general anesthesia, the 30-day mortality was low in our patients. But still, on the basis of the literature, regional or local anesthesia should be used when possible, especially in elderly.
Major amputation within the first 30 days was also higher in octogenarians. Critical limb ischemia was the predominant indication in this group, and a further improvement in the outflow was not possible. In contrast, indication in our younger group was predominantly claudication. This fact must be considered when interpreting our results. Critical limb ischemia was detected as an important risk factor for limb loss and death in univariate and multivariate analyses, which is similar to the literature 18 . The long-term limb salvage was also significantly lower in our elderly group. However, as previously mentioned, critical limb ischemia was the most frequent indication in this group.
Statin use was protective of survival in our results. Stavroulakis et al. 19 in their multicenter study described lower rates of mortality and an increased amputation-free survival for statin use in patients with peripheral occlusion disease. However, such an influence on patency rates and limb salvage was not seen in our analysis. Early graft failure and significantly reduced primary patency loss are described in women with peripheral artery disease20, 21 . Female gender was detected to be a risk factor for reduced primary patency in uni- and multivariate analyses.
No significant difference in primary patency and secondary patency was seen between the groups. Both patency rates were excellent. Wieker et al. 9 reported a primary patency of 78.5% and a secondary patency of 89.1% after 7 years, which is similar to our results. Ballotta et al. 7 described a higher primary patency after the same time period. However, they stated in their limitations that the small number of patients may have affected their results. In regard to patency rates, the results of octogenarians are similar to younger patients. These findings correlated with other operative or endovascular treatments for peripheral arterial occlusion disease 22 . Patency rates for endovascular treatment of the common femoral artery are still sobering; 73% after 1 year are reported for primary patency12,23. Bath and Avgerinos 11 described a higher primary patency for routine stenting. However, the common femoral artery is an area of flexibility and so there is a high risk for stent fractures. In addition, long-term data on endovascular treatments of the common femoral artery are still missing.
The retrospective character of our study is one of the limitations. An ankle–brachial index was not done routinely, so we cannot include data on this. The majority of patients were treated under general anesthesia, so our results should be interpreted in this light.
Conclusion
CFAe has excellent long-term patency rates and is a safe procedure. The perioperative mortality is higher in octogenarians. Probably, regional anesthesia can reduce the risk of death. Statin use seems to have a protective influence on long-term survival; female gender was associated with reduced primary patency.
Footnotes
Author Contributions
C.U. contributed to writing, conception and design, analysis and interpretation, data collection, statistical analysis, and approval of the manuscript. H.G. contributed to writing, conception and design, data collection, and approval of the manuscript. F.Z. contributed to statistical analysis, analysis and interpretation, and approval of the manuscript. S.W. contributed to data collection, analysis and interpretation, and approval of the manuscript. T.B., I.T., and M.S. contributed to conception and design, analysis and interpretation, and approval of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.