
Abstract
Background:
Major abdominal surgery in older and frail patients is associated with considerable morbidity and mortality. Plasma albumin is routinely measured in the clinic and has been proposed as an indicator of frailty. This study aimed to investigate if plasma albumin is a predictor of mortality in older patients undergoing open abdominal surgery.
Materials and methods:
We conducted a single-center, register-based retrospective study of patients, aged ⩾60 years who underwent one of 81 open abdominal surgical procedures. Patients operated on during the period from January 1st, 2000 to May 31st, 2013 were consecutively identified in the Danish National Patient Registry. Plasma albumin was measured within 30 days prior to surgery and the primary endpoint was 30-day postoperative mortality.
Results:
3,639 patients were included of whom 68.2% underwent emergency surgery. The rate of severe hypoalbuminemia (plasma albumin < 28 g/L) was 43.4%. Preoperative plasma albumin was lower in patients with a fatal 30-day outcome (mean 20.6 g/L vs 30.1 g/L in survivors, p < 0.0001). Other independent predictive parameters of 30-day mortality were age, male sex, and emergency surgery. We present an algorithm including these four variables for the prediction of 30-day mortality for patients aged ⩾60 years undergoing open abdominal surgery.
Conclusion:
Preoperative plasma albumin is a predictor of 30-day mortality in patients above 60 years of age following open abdominal surgery. Assessment of plasma albumin in conjunction with other risk factors such as age, sex, and surgical priority may improve preoperative decision-making.
Introduction
Major surgery poses a considerable physiological challenge in older patients. Contributing factors include perioperative physiological surgical stress, declining physiological capacity, and an increased prevalence of comorbidities. Several studies have evaluated rates of postoperative complications and mortality in elderly patients undergoing abdominal surgery. Compared to younger counterparts, elderly patients more often develop postoperative cardiac, respiratory, renal, or cognitive dysfunction, and these complications are more severe than in younger patients (1). In a retrospective study of 4000 patients aged beyond 50 years and undergoing non-cardiac surgery, increasing age was associated with both postoperative complications and early death (2). Another study evaluated mortality and postoperative complications after non-cardiac surgery in 26,648 patients aged beyond 80 years as compared with half a million patients of younger age (3). Thirty-day mortality rates were 8% and 3%, respectively. The older patients more frequently experienced postoperative complications, and the related mortality was higher for all categories of serious adverse events.
The concept of frailty is being giving increasing awareness and considered important for the estimation of post-surgery risks. Although the exact definition of frailty is debated, the condition is characterized by decreased physiological reserve across multiple organ systems. This makes a frail patient more vulnerable at even minor surgical stress (4). Velanovich et al. (5) reported an association between the degree of frailty measured as the number of accumulated age-related deficits and morbidity as well as mortality. In a recent paper, the same modified frailty index was used. Among 117,064 patients who underwent colectomy, there was a clear association between the frailty index and mortality after both laparoscopic and open abdominal surgery (6).
Data on hypoalbuminemia and mortality following open major abdominal surgery in patients with advanced age are still sparse. A tool is lacking for an easy estimation of postoperative mortality and improvement of the clinical decision-making. This study aimed to investigate if the plasma level of albumin (P-Alb) may serve as a reliable and independent predictor of early mortality after open abdominal surgery in patients above 60 years of age. Secondly, our aim was to define an algorithm for risk prediction of a fatal postoperative outcome within postoperative day 30.
Material and Methods
We conducted a register-based retrospective study at the Digestive Disease Center, Bispebjerg Hospital, University of Copenhagen, Denmark. This is a public non-insurance–driven department serving a population of approximately 430,000 inhabitants from central Copenhagen.
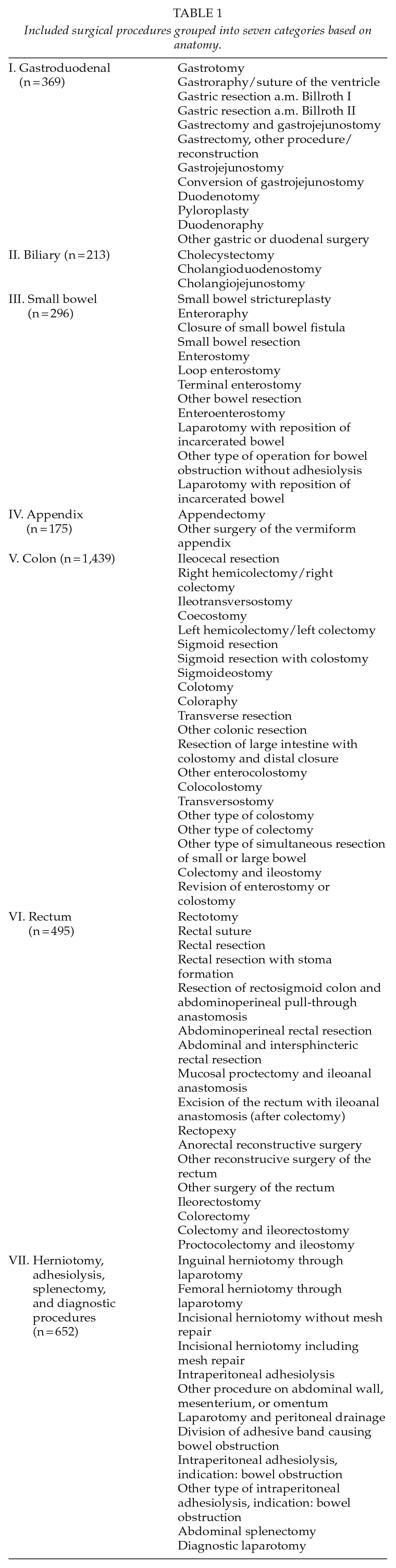
All Danish citizens have a unique, 10-digit civil registration number indicating date of birth and gender. This personal identification number is registered in all public records, making it possible to link information from national registries with almost complete follow-up. All contacts and admissions to Danish hospitals are registered in the Danish National Patient Registry. Using data from this registry, we included all patients (n = 4,426) aged ⩾60 years who underwent open abdominal surgical interventions during the period from January 1st, 2000 to May 31st, 2013 at Bispebjerg Hospital. Only the first surgical procedure during the inclusion period was assessed. A total of 81 types of surgery according to the NOMESCO Classification of Surgical Procedures were grouped into seven categories depending on the anatomical location of the procedure (Table 1) (7). We excluded patients undergoing more than one of the 81 procedures or a reoperation within 30 days. Additionally, we excluded patients with a temporary civil registration number, missing information regarding surgical priority, trans-anal surgery, or lacking assessment of P-Alb within 30 days prior to the operation. This left 3,639 patients for analysis (Fig. 1). Data were merged with data from the civil registration system holding information on demography, vital status, and emigration.
Included surgical procedures grouped into seven categories based on anatomy.
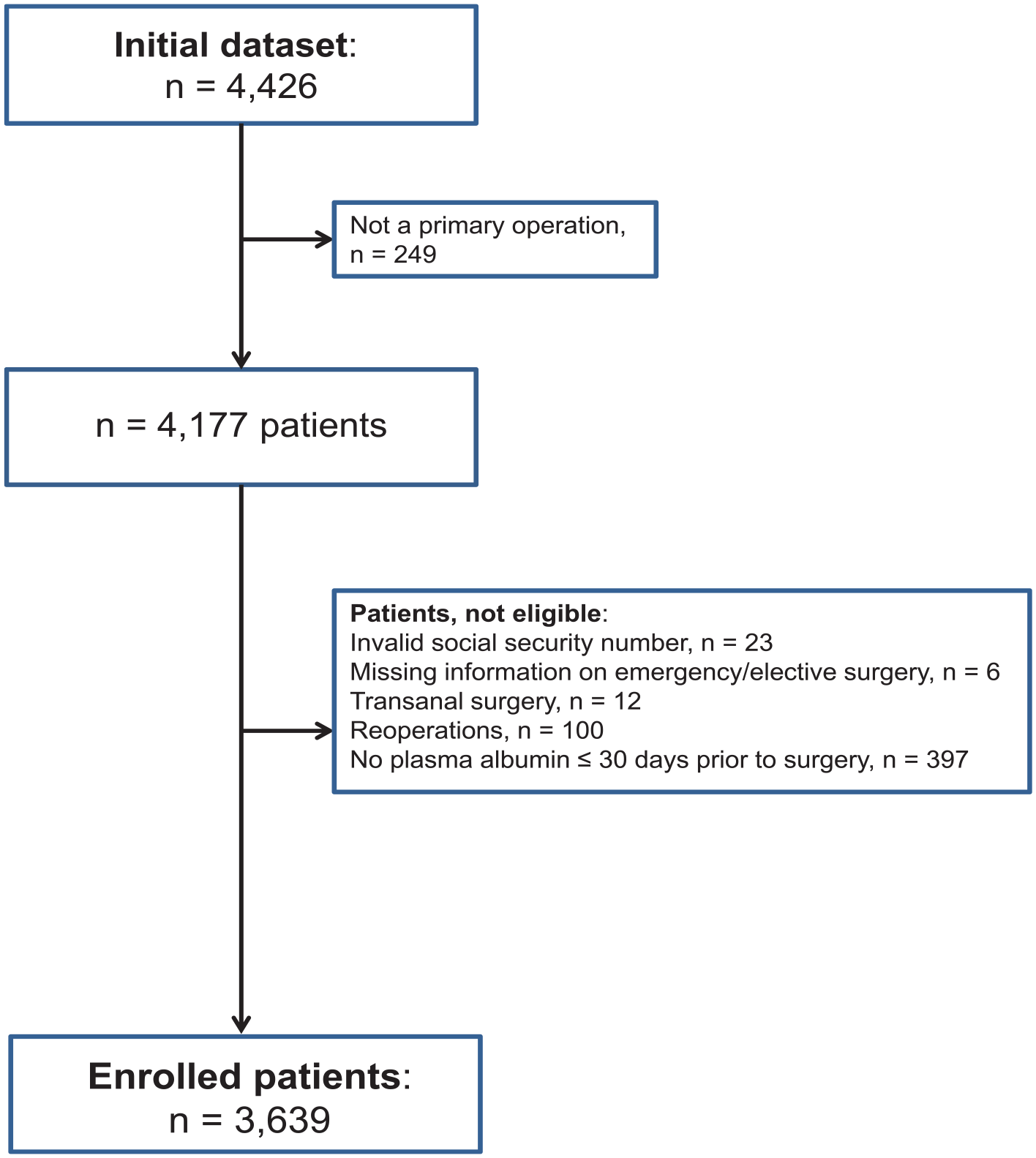
Flow chart illustrating the inclusion and exclusion of patients.
P-Alb was obtained from the local laboratory system, CSC LABKA IITM (CSC, Denmark), from December 1st, 1999 to June 28, 2013. P-Alb was analyzed on venous blood samples at the Department of Clinical Biochemistry, Bispebjerg Hospital, University of Copenhagen, Denmark. In cases with more than one P-Alb measurement within 30 days prior to the operation, the sample closest to the operation was chosen. Moderate hypoalbuminemia has been defined as 28–35 g/L and severe hypoalbuminemia as P-Alb <28 g/L (8). The following data were obtained: date of hospital admission, priority of admission/surgery (elective vs emergency), type of operation, and time of discharge.
Permission for this study was granted by the Danish Data Protection Agency (ID: 2007-58-0015). No permission from the regional Ethical Committee was needed, as the study was registry-based.
Statistical Analysis
The primary endpoint was 30-day mortality. Differences between baseline values of the two groups were analyzed using parametric, non-parametric, or categorical statistical methods depending on data nature. Categorical data were analyzed using the chi-square test, and differences between continuous data were compared using unpaired t-tests. Cox proportional hazard models were used to determine hazard ratios (HRs) for 30-day mortality according to levels of P-Alb. HRs were adjusted for confounders, including age, gender, and elective versus emergent surgery. Finally, we used logistic regression to develop a prognostic algorithm. Statistical level of significance was defined as p < 0.05 with 2-tailed tests.
P-Alb was rounded to the nearest concentration divisible by two (10, 12, 14, etc., g/L) for a graphical presentation of the distribution of number of patients and mortality plotted against preoperative P-Alb.
Data analysis was performed using the SAS program version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
The Cohort
The baseline characteristics of the patients are presented in Table 2. Patient mean age was 76.4 years, and 61% were females. Mean P-Alb was 28.2 g/L, equaling hypoalbuminemia. Only 574 (15.8%) patients had normal P-Alb. Almost half of the patients (n = 1,578; 43.4%) had severe hypoalbuminemia.
Patient baseline characteristics.
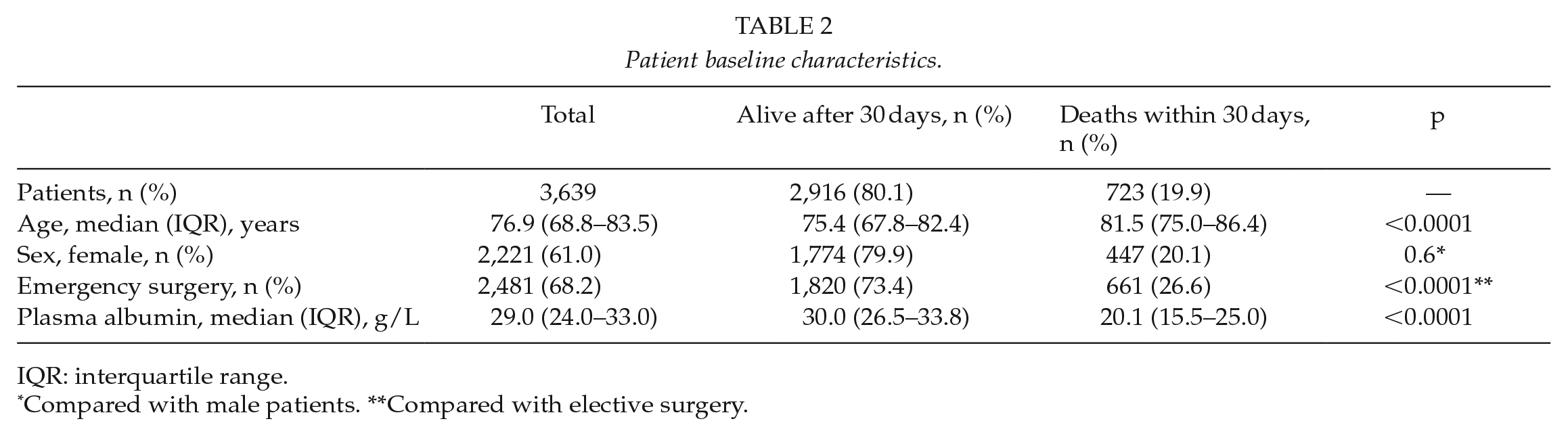
IQR: interquartile range.
Compared with male patients. **Compared with elective surgery.
Descriptive data on operation categories are shown in Table 3. Colonic procedures were the most frequent and performed on almost 40% of the patients. Patient age or P-Alb did not differ significantly between the operation categories. Most patients underwent emergency surgery (n = 2,481; 68.2%).
Patient characteristics including 30-day mortality according to surgical category.
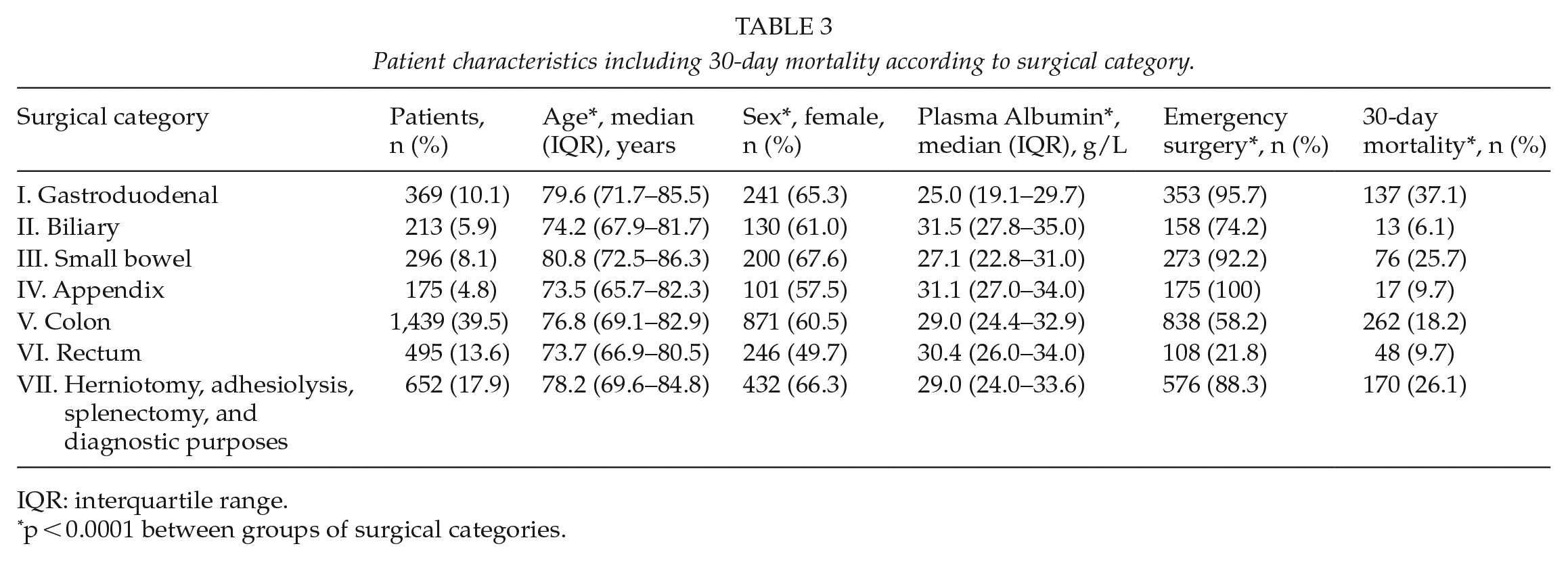
IQR: interquartile range.
p < 0.0001 between groups of surgical categories.
The overall 30-day mortality was 19.9%. Mortality was significantly higher for the patients undergoing emergency (26.6%) than elective surgery (5.4%, p < 0.0001). Patients with a fatal outcome were older (mean age 80.5 vs 75.5 years, p < 0.0001). Mortality differed significantly according to operation category with the highest value (37.1%) after gastroduodenal surgery (Table 3). Preoperative P-Alb was significantly lower for patients with a fatal outcome within the first postoperative 30 days as compared with survivors (median 20.6 versus 30.1 g/L, p < 0.0001). We found a close association between P-Alb and 30-day mortality (Fig. 2). The mortality rate was almost 100% in the approximately 2% of the patients who had a P-Alb of 10 g/L. The lowest mortality was among patients with a P-Alb of 32 g/L.
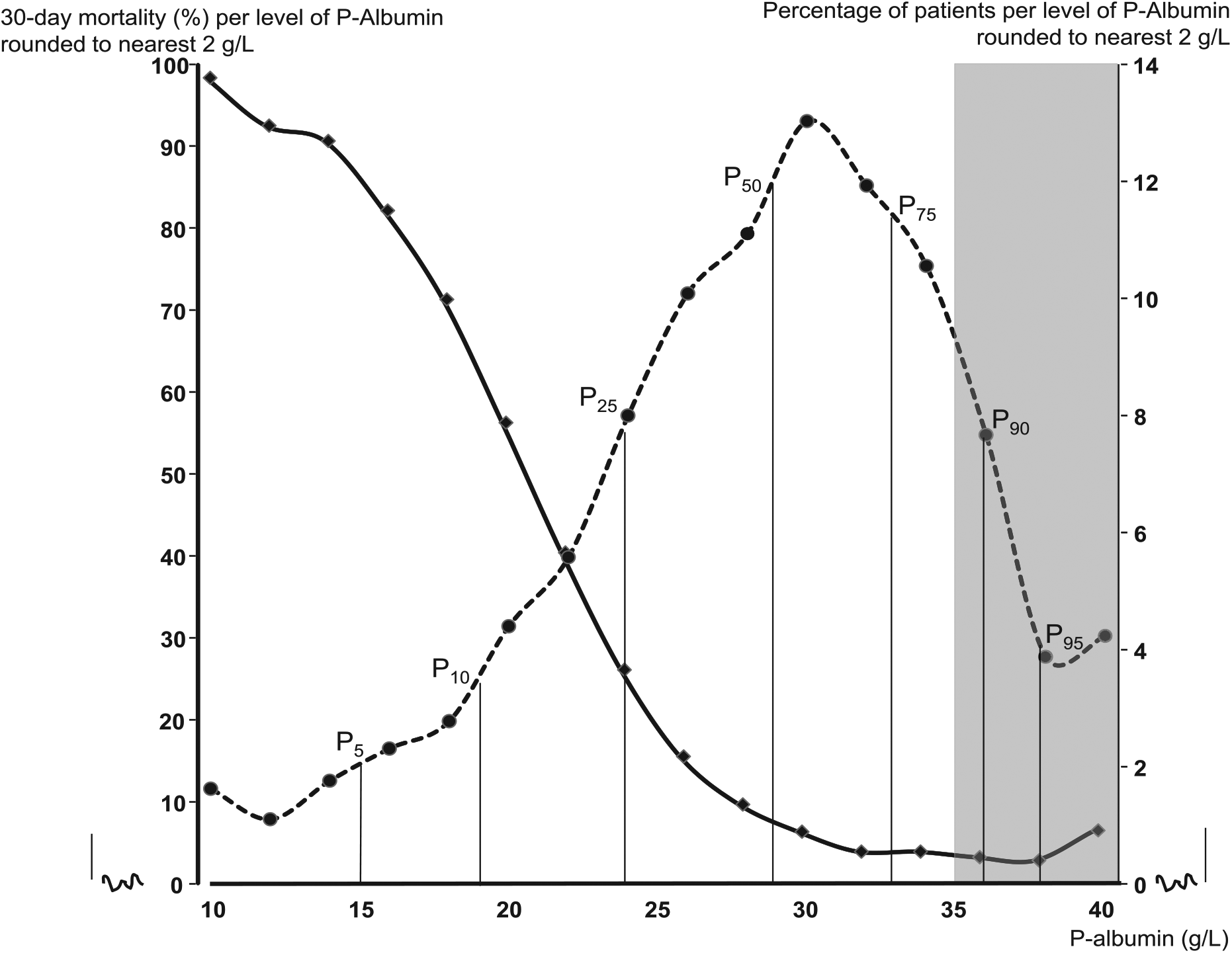
Plasma albumin and 30-day mortality. Left y-axis and full line: 30-day mortality (%) per level of P-albumin rounded to the nearest 2 g/L. Right y-axis and dotted line: rate of patients (%) per level of P-albumin rounded to the nearest 2 g/L. The gray box illustrates the P-albumin reference interval. For the patient distribution (dotted line), the 5, 10, 25, 50, 75, 90, and 95 percentiles are shown. P0 = 5 g/L, P100 = 49 g/L. Total number of patients: n = 3,639. Patients deceased: n = 723.
Assessment of possible selection bias
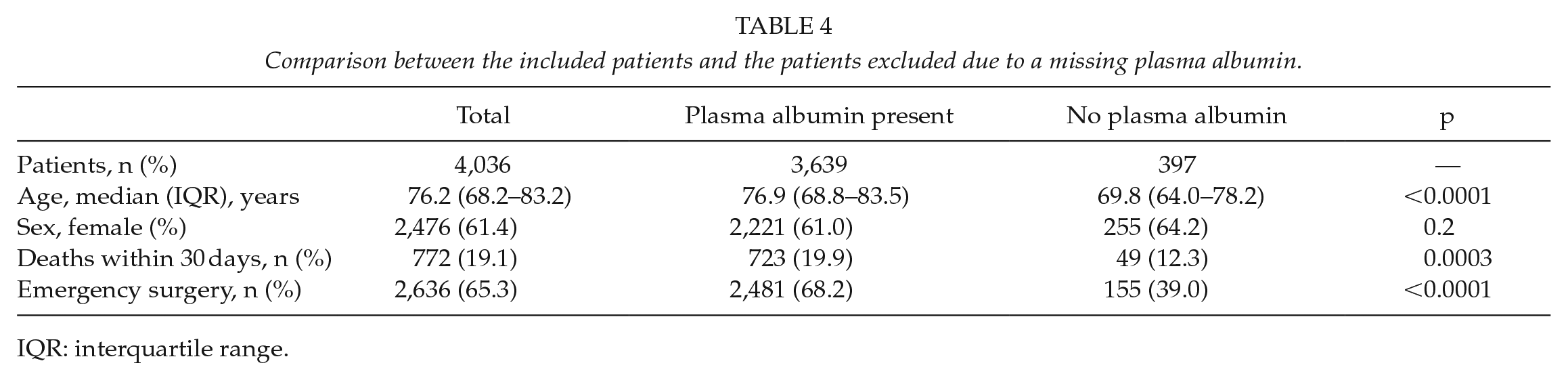
We compared the included patients having a P-Alb measurement with the excluded patients not having a P-Alb measurement. There was no difference in the female/male proportion between the two groups. However, the excluded patients without a P-alb measurement were younger, had a lower 30-day mortality, and had a lower proportion of emergency surgery (Table 4).
Comparison between the included patients and the patients excluded due to a missing plasma albumin.
IQR: interquartile range.
Multivariable Assessment of Risk Factors Predicting 30-Day Mortality
We calculated HRs for 30-day mortality for P-Alb, age, sex, and surgical priority (Fig. 3). P-Alb was almost as strong in predicting mortality as emergency surgery. A 5-g/L decrease in P-Alb was associated with a HR of 2.32 (95% confidence interval (CI): 2.20–2.45, p < 0.001) for 30-day mortality. Other independent predictors of 30-day mortality in this model were emergency surgery (HR = 2.83, p < 0.001) and male sex (HR = 1.33, p = 0.0003).
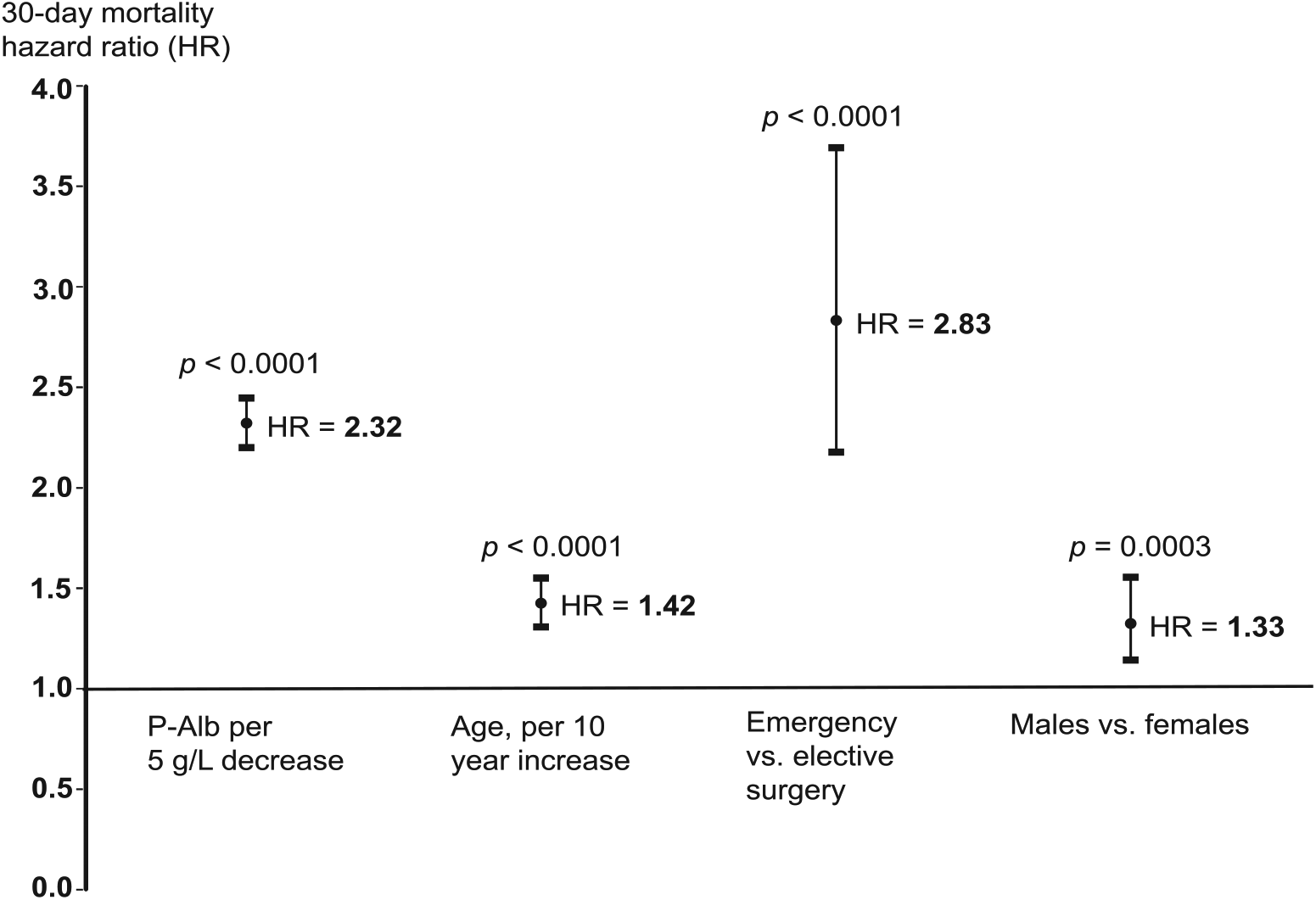
Adjusted hazard ratios (HRs) for 30-day mortality, including 95% confidence intervals. Total number of patients: n = 3639. Patients deceased: n = 723. P-Alb: plasma albumin.
Development of a Prognostic Algorithm
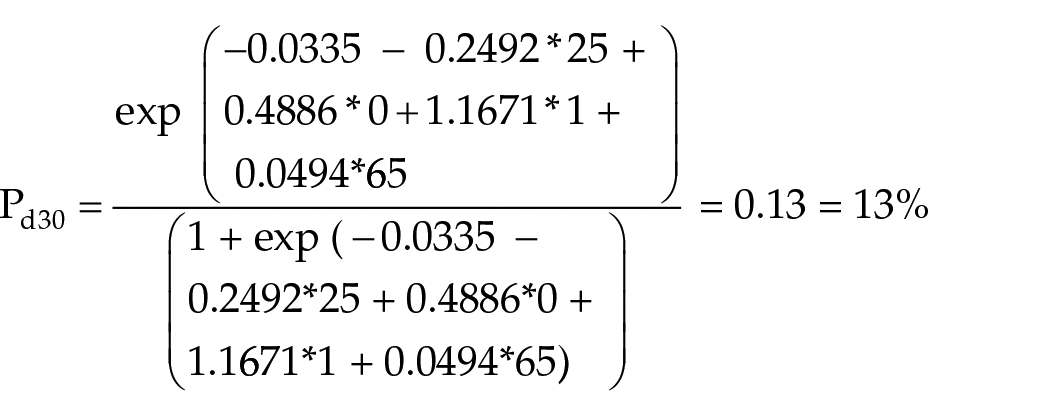
Using logistic regression, we developed an algorithm predicting the risk of 30-day mortality (Pd30), based on P-Alb (given in g/L), sex (0 for females, 1 for males), priority (0 for elective, 1 for emergency), and age (in years)
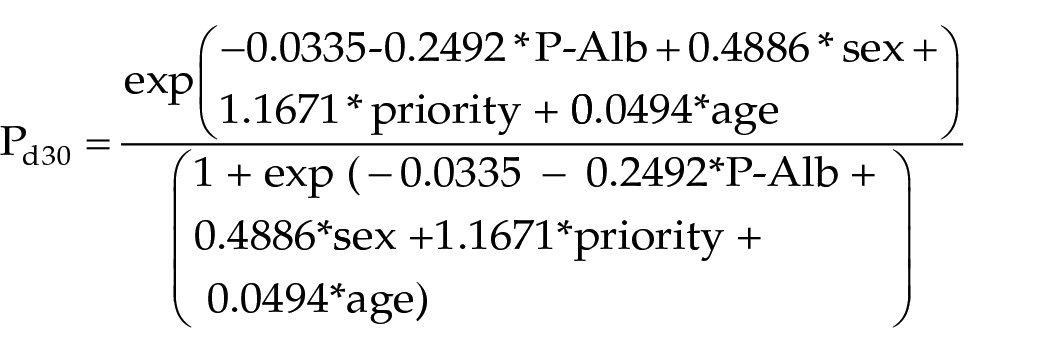
Example: a 65-year-old female patient. P-Alb = 25 g/L. Priority: emergency
Discussion
This study demonstrated that the plasma concentration of an easily available biomarker correlated with postoperative mortality after open abdominal surgery in patients above 60 years of age. Even after adjustment for age, sex, and emergency surgery, P-Alb clearly predicted 30-day mortality in this population. We developed an algorithm as a prognostic tool for surgeons to guide them in their preoperative decision-making. This algorithm can help identify which patients who are at increased risk of death following open abdominal surgery and who could potentially benefit from either conservative treatment or in the case of an inevitable operation, focused perioperative care.
Albumin is the most abundant plasma protein in humans. The synthesis of albumin by the hepatocytes is primarily controlled by the colloid osmotic pressure and dietary protein intake. Albumin serves as a transporter molecule for a range of substances and is the major contributor to the colloid osmotic pressure. The half-life of the 585 amino acid and 66-kDa molecule in plasma is 15–19 days. Albumin is a reverse acute-phase reactant leading to low P-Alb in malignancy, chronic infections, or other chronic conditions (9). P-Alb has traditionally been viewed as a valid indicator of protein malnutrition (10). This has been questioned, however, as albumin more correctly reflects pathology. Ongoing inflammation negatively affects the synthesis of albumin and upregulates decomposition of the protein and the vascular permeability of the protein thereby decreasing P-Alb (11). Albumin depletion also occurs due to hepatic disease, increased gastrointestinal/urinary loss, or burn injury. Decreased P-Alb is not commonly the only triggering cause of oedema and ascites. The fluid displacement normally occur secondary to increased vascular permeability (10). There are thus several potential pathophysiological mechanisms to explain the increased mortality reported in patients with low preoperative P-Alb (12,13). An elevated P-Alb can be seen with dehydration or falsely from prolonged tourniquet time (10).
Simple and inexpensive tools for the prediction of postoperative complications and early death are warranted and ideally include basic preoperative biochemical analyses. P-Alb is routinely measured at admission prior to surgery. Hypoalbuminemia was associated with increased mortality and morbidity in patients undergoing general surgery (9). In a series of 1,097 cases of radical cystectomies, hypoalbuminemia was associated with increased 90-day mortality after adjustment for sex, age-adjusted Charlson score, clinical stage, and neoadjuvant chemotherapy (14). Among 2,894 patients who had pancreaticoduodenectomy, preoperative hypoalbuminemia was a significant predictor of postoperative mortality which increased from 0.9% at P-Alb >35 g/L to 7% for levels less than 25 g/L (15). In a prospective observational multicentre study of 54,215 patients undergoing non-cardiac surgery, there was an exponential increase in mortality from 1% to 29% corresponding to serum-albumin levels of >46 g/L and <21 g/L, respectively. The albumin level was the strongest predictor for mortality and morbidity (12). Mosfeldt et al. (16) reported an increased rate of 3-month mortality in hip fracture patients with P-Alb <34 g/L. Recently, Fisher et al. (17) looked at simple biochemical analytes in 455 hip fracture patients older than 60 years. P-Alb <33 g/L was identified as an independent predictor of in-hospital death with an odds ratio of 2.07.
Hypoalbuminemia and adverse clinical outcomes such as septicemia and mortality have been linked in different settings including intensive care and trauma in patients beyond 55 years of age (18). Hypoalbuminemia was a strong predictor of 30-day mortality in patients acutely admitted with medical conditions (19). Our study, that is large and register-based, provides information about patients undergoing a broad range of open abdominal surgical procedures. In addition, the findings are easily applicable at the surgical wards by use of the proposed risk assessment algorithm.
The 397 patients excluded due to missing values of P-Alb were younger, had a lower 30-day mortality, and the proportion of emergency surgery was lower. They thus appear to be in better health and would presumably have higher values of P-Alb than the included patients. This might have introduced an underestimation of the effect of low levels of P-Alb.
Furthermore, the exclusion of 100 patients undergoing a reoperation within the first 30 postoperative days may have resulted in under-reporting of the mortality rate. Access to information on comorbidities, body mass index, and smoking status would have been valuable, but was not an option in this study. Moreover, it remains unclear if the results can be extrapolated to the increasing rates of patients subjected to laparoscopic surgery. The study may be confounded by the fact that some pathologies, such as cancer, are linked to both hypoalbuminemia and increased mortality. In this study we were not able to distinguish between deaths directly linked to the operation or to factors unrelated to it. Finally, we did not include potentially confounding factors like perioperative complications, blood loss/transfusions, operative time, and surgeon’s experience.
The preoperative level of P-Alb is a predictor of 30-day mortality in patients aged beyond 60 years following open abdominal surgery. We present a test where P-Alb in conjunction with other risk factors such as age, sex, and type of surgery can be used as an aid and guidance in the preoperative decision-making. We are aware that other risk calculators exist, e. g. the American College of Surgeons Surgical Risk Calculator. However, we offer a much simpler and quickly applicable tool for risk estimation.
How a prognostic tool could be used would depend on many factors including the set-up and resources at a given hospital. However, being able to identify high-risk patients before surgery, especially in emergency surgery, would permit a focused perioperative care to try to reduce mortality, e. g. a transfer to the intensive care unit immediately after surgery. For elective surgery, an operation could be postponed, allowing for treatment of comorbidities, optimization of nutritional status, and so on. These types of strategies have been shown to reduce mortality in hip fracture patients (20).
In conclusion, preoperative P-Alb is a predictor of 30-day mortality in patients above 60 years of age following open abdominal surgery. Assessment of P-Alb in conjunction with other risk factors such as age, sex, and surgical priority may improve preoperative decision-making.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.