
Abstract
Background and Aims:
Long-term prospective data on patient-reported outcome after surgical treatment of pelvic ring injuries are scarce. This study aimed at describing results at 5 years post-surgery using validated outcome measures.
Patients and Methods:
Patients admitted for surgical treatment of pelvic ring injuries were prospectively included and asked to report their outcome at 1, 2 and 5 years post-surgery using two patient-reported outcome measures: the generic Short-Form 36 and the condition-specific pelvic discomfort index. Data were evaluated using mixed-effects linear models.
Results:
There were 108 patients (68 males and 40 females), mean age 38 years. Injury type according to the AO/OTA-classification was B-type in 68 patients and C-type in 40 patients. No domain of the Short-Form 36 reached norm values at 5 years post-surgery. Females reported a worse outcome than males concerning general health (p < 0.01) at 5 years. Recovery of physical function (p < 0.01), mental health (p = 0.04), and pain (p = 0.01) was observed for males at 5 years compared to earlier assessments, while females on the contrary described more pain at this time-point (p = 0.03). Mean pelvic discomfort index at 5 years was 27, indicating moderate residual pelvic discomfort overall. Males reported less pelvic discomfort than females at 5 years (p = 0.02) and improved when compared to results at 2 years (p = 0.02), while females did not. Influence of age, fracture type, and presence of associated injuries on patient-reported outcome was limited.
Conclusion:
Surgically treated pelvic ring injuries are associated with long-standing negative effects on patient-reported outcome. Males report a better outcome than females at 5 years post-surgery.
Keywords
Introduction
Early research concerning outcome after surgical treatment of pelvic ring injuries primarily focused on describing objective findings such as mortality rates and measures derived from clinical and radiographic examination (1–3). The evaluation of patient-reported outcome measures (PROMs) allows patients to describe their health status using generic and condition-specific instruments, and this has established itself as a standard when reporting outcome in orthopedic research. However, the existing literature concerning pelvic ring injuries is limited, due to a lack of prospective long-term data and the use of non-validated outcome instruments (4–6).
The objective of this study was to describe the long-term functional outcome in patients with surgically treated pelvic ring disruptions using validated generic and pelvis-specific outcome measures.
Patients and Methods
Study Design
In a prospective observational study, all patients referred to our institution for surgical treatment of pelvic ring injuries type B or C (AO/OTA classification) during a 5-year period were included. Patient gave their informed consent before inclusion, and the study was approved by the regional research ethics board. Patients under the age of 16 years and non-Swedish citizens were excluded.
Patients and Treatment
In total, there were 108 patients (68 males and 40 females), with a mean age of 38 years (16–85) available for the study. The pelvic ring injuries were classified according to the AO/OTA classification. There were 68 B-type and 40 C-type injuries. The most common injury mechanisms were motor vehicle accidents (MVAs, 44 patients), fall from height (29 patients), and crush injuries (15 patients). Associated injuries were seen in 79 patients (73%). The most frequently injured body region was thorax (39 injuries), followed by spine (36 injuries), lower extremity (33 injuries), abdomen (28 injuries), upper extremity (22 injuries), and head (21 injuries). Of the 108 patients, 47 (44%) had sustained a severe polytrauma indicated by an Injury Severity Score (ISS) of ⩾16. Median time from trauma until definitive surgery was 5 days (range 1–22). Demographics are summarized in Table 1.
Demographics of the study population.
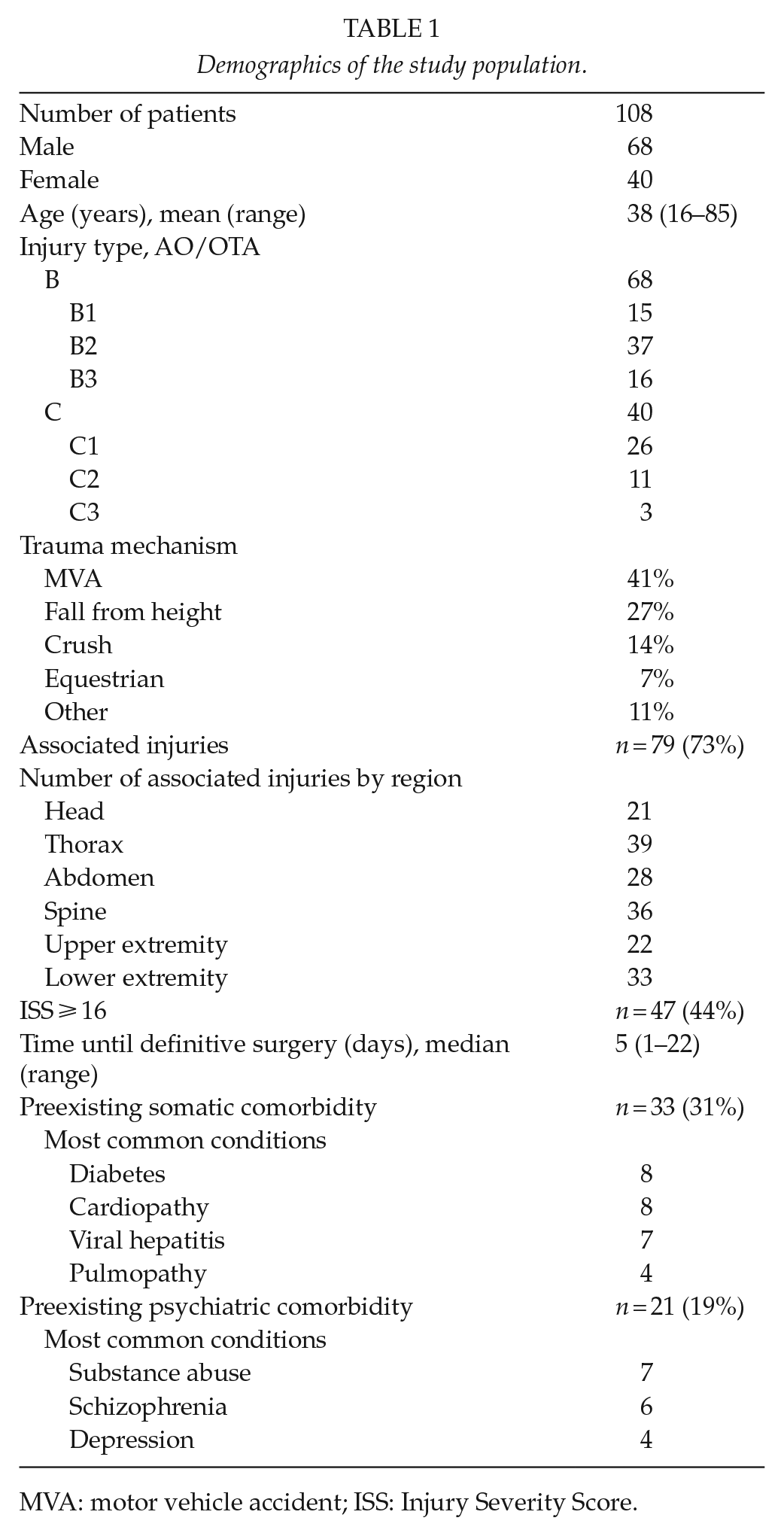
MVA: motor vehicle accident; ISS: Injury Severity Score.
Decision on surgery was based on clinical and radiological evaluation to assess pelvic instability. These evaluations were carried out by senior consultants in orthopedic trauma surgery. The surgical method of choice was open reduction and internal fixation (ORIF) in 22 patients, strictly percutaneous procedures with closed-reduction and fluoroscopy-guided screw placement in 35 patients, and a combination of ORIF and percutaneous procedures in 51 patients. One patient underwent early reoperation due to inadequate reduction.
The protocol for thromboprophylaxis was low-molecular-weight heparin (enoxaparin, 40 mg s.c./day) for a minimum of 10 days post-surgery. Intravenous cloxacillin (2 g × 4) was used as per-operative antibiotic prophylaxis. Medical records pertaining to the initial treatment and subsequent follow-up of the pelvic injury were retrieved at 5 years post index surgery and carefully examined for complications. As many patients were referred from other regions of the country, medical charts from the referring hospitals were also retrieved at this time-point and scrutinized for complications.
Treatment complications
Postoperative wound infections were reported in 10 patients, of which 7 were superficial and resolved with antibiotic treatment alone. The remaining three were deep infections necessitating secondary debridement surgery. Non-surgical infections were reported in 17 patients, the most common manifestations being pneumonia (9 patients) and urinary tract infection (5 patients). Concerning thromboembolic complications, two pulmonary embolisms were diagnosed, while no case of deep vein thrombosis was reported.
Follow-Up
The patients were followed up with PROMs at 1, 2 and 5 years post index surgery. The instruments used were the generic quality of life (QoL) instrument Short-Form 36 (SF-36) and the condition-specific pelvic discomfort index (PDI) (7, 8). These outcome instruments were distributed via postal mail to the patient’s current location. In case of no response, they received one reminder.
Radiological examinations of the pelvis were performed pre- and post-surgery and during the course of healing. A final radiological examination was conducted at 2 years post-surgery at the referring center, and images were then digitally transferred to our hospital for centralized assessment. The protocol consisted of plain radiographs including frontal, inlet, and outlet views of the pelvis. Displacement of the posterior aspect of the pelvic ring was measured and categorized by two examiners as displacement of less than 5 or 5 mm or more according to the German pelvic study group (9). In addition, implant integrity and position were evaluated.
Patient-Reported Outcome Instruments
Short-Form 36
The SF-36 is a widely used generic QoL instrument comprising 36 questions about eight different domains concerning functional outcome: physical functioning (PF), physical role functioning (RP), bodily pain (BP), general health (GH), vitality (VT), social role functioning (SF), emotional role functioning (RE), and mental health (MH). Raw data are collected and transposed to subscores for each domain ranging from 0 (worst) to 100 (best) (7). The SF-36 has been tested for validity and reliability against an average Swedish population (10).
A Swedish age- and sex-matched population norm was used for comparison.
Pelvic discomfort index
The PDI is a condition-specific instrument for estimating discomfort from the pelvic region after surgical treatment of pelvic ring injuries. It consists of six questions regarding issues with pain, walking, hip motion, leg sensation, scar tissue from the pelvic region, and sexual problems. Each question is graded on a six-level scale, ranging from no discomfort to very severe discomfort.
Upon completion, an index is calculated which ranges from 0% pelvic discomfort (best) to 100% pelvic discomfort (worst). Suggested categorization of discomfort is minimal (0%–20%), moderate (21%–40%), severe (41%–60%), very severe (61%–80%), and extremely severe or possibly exaggeration of symptoms (>80%). The instrument has been developed and validated for use in surgically treated pelvic ring injuries and acetabular fractures (8, 11).
Statistics
Mixed-effects linear models, using all available observations, were used to analyze the SF-36 and PDI data to determine changes in health status over time. The model included variables such as gender (male/female), age (above/below median), fracture type (B/C), and presence of associated injuries to investigate if any of these factors influenced outcome. The mixed-effects models were set up using a repeated measures design assuming an unstructured covariance matrix with time of measurement (1 year or 2 or 5 years post index surgery) entered as a factor variable. If a significant time, covariate, or interaction effect was present for a certain test, the analysis was followed up by pairwise comparisons using model-predicted least square means to pinpoint where differences were present.
Student’s t test was used to compare SF-36 results to norm data. Pearson’s chi-square test was used to examine outcome with respect to residual posterior displacement of the pelvis.
Values of p < 0.05 were considered significant.
Results
Radiology
At 2 years post-surgery, a radiological examination was performed in 93 of the 105 patients (89%) available for follow-up. There were no non-unions. Posterior displacement was <5 mm in 69 patients (74%) and ⩾5 mm in 24 patients (26%). There were no differences in outcome between these groups regarding the SF-36 domain physical functioning (p = 0.83) and PDI (p = 0.75) at 5 years post-surgery.
Implants remained unchanged in 71 patients and had changed position in 10 patients. Changes were considered minor and not clinically relevant in all these cases.
Complete removal of implants had been undertaken in 10 patients, and partial removal was performed in 2 cases. More females (n = 9) than males (n = 3) underwent implant removal.
Patient-Reported Outcome
Of the initial 108 patients, 3 patients died within 1 year after the index surgery, leaving 105 patients available for follow-up at 1 year post-surgery. Of these, 80 patients (76%) responded to the outcome measures. At 2 years post index surgery, an additional patient had died. Of the remaining 104 patients, 79 (76%) completed the questionnaires. Between 2 and 5 years post-surgery, 3 patients died, leaving 101 patients available for follow-up at 5 years post-surgery. Of these, 78 patients (77%) responded.
SF-36
At 5 years post-surgery, none of the SF-36 domains reached the levels of an age- and sex-matched population norm. (Table 2).
Median values for each domain of the SF-36 at 1, 2 and 5 years post-surgery compared to values of a sex- and age-matched Swedish norm population.
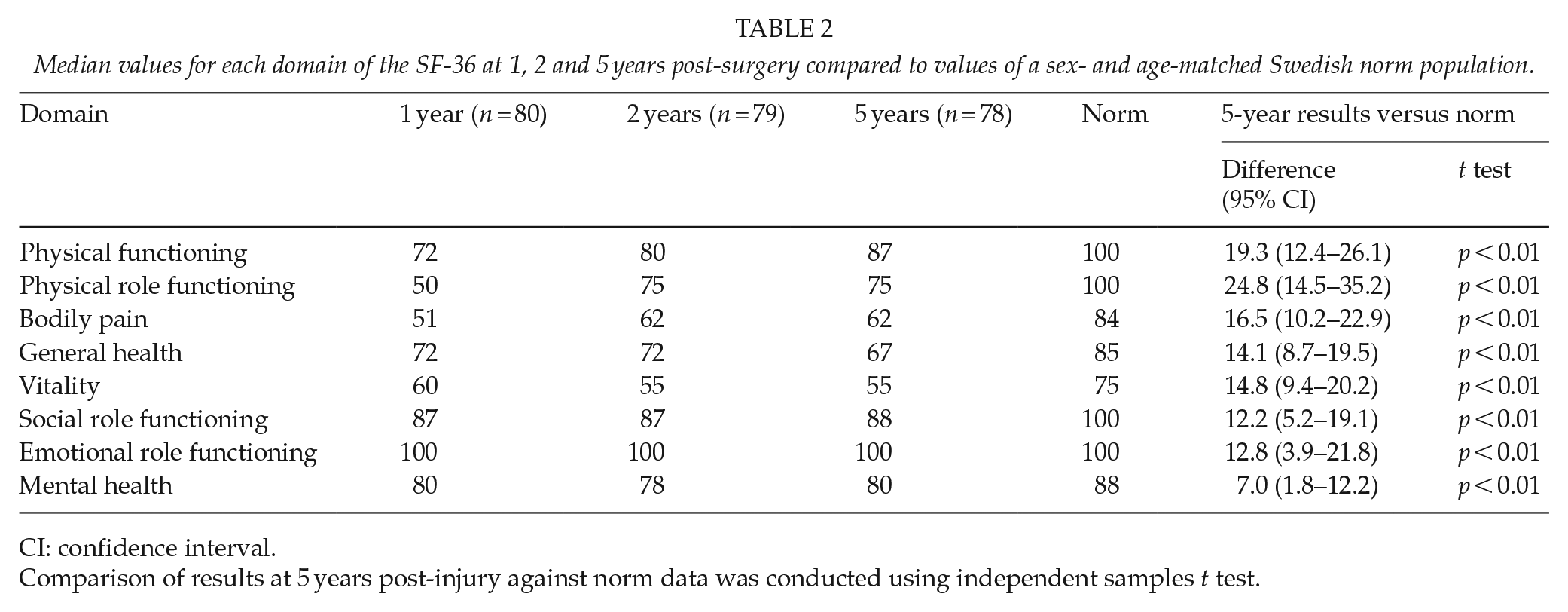
CI: confidence interval.
Comparison of results at 5 years post-injury against norm data was conducted using independent samples t test.
The mixed-effects linear models demonstrated improvement in physical functioning at 5 years post-surgery compared to earlier assessments (p < 0.01). Physical role functioning also improved at 5 years compared to results at 1 year post-surgery (p < 0.01). For the remaining six domains, no statistically significant changes were found between time-points.
The setup of the mixed-effects models allowed for examining the impact on outcome of variables gender, age, fracture type, and presence of associated injuries.
Gender
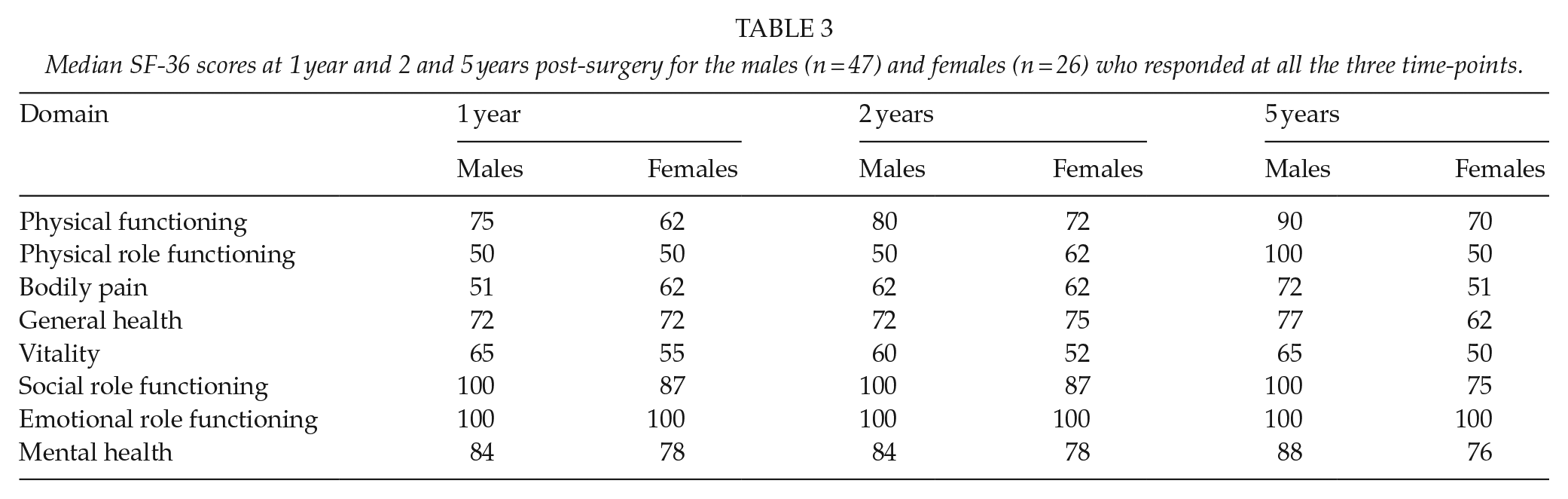
It was found that males improved in physical functioning between 2 and 5 years post-surgery, while females did not. Females demonstrated a worsening in bodily pain at 5 years compared to results at 1 year post-surgery, while males on the contrary demonstrated a recovery between these time-points. Concerning the domain general health, females estimated a worse outcome at 5 years post index surgery compared to males and had also deteriorated compared to earlier measurements, while males had not. For remaining domains, no significant influence of gender could be demonstrated, although a tendency for females to estimate lower scores than males was present in every SF-36 domain at 5 years post-surgery (Table 3).
Median SF-36 scores at 1 year and 2 and 5 years post-surgery for the males (n = 47) and females (n = 26) who responded at all the three time-points.
Age
Older patients (above median age) estimated a lower physical functioning than younger (below median age) when analyzing all available observations. The effect was estimated to a difference of 0.4 points per year. No other influence of age on SF-36 results could be demonstrated.
Fracture type
Patients with C-type injuries estimated lower general health overall compared to B-type injuries. No other influence of fracture type on SF-36 results was found.
Associated injuries
The presence or absence of associated injuries was not found to affect outcome in any domain of the SF-36.
The results of the mixed-effects linear models used to analyze SF-36 data are summarized in Table 4.
Summary of results from the mixed-effects linear models for SF-36 and pelvic discomfort index (PDI).
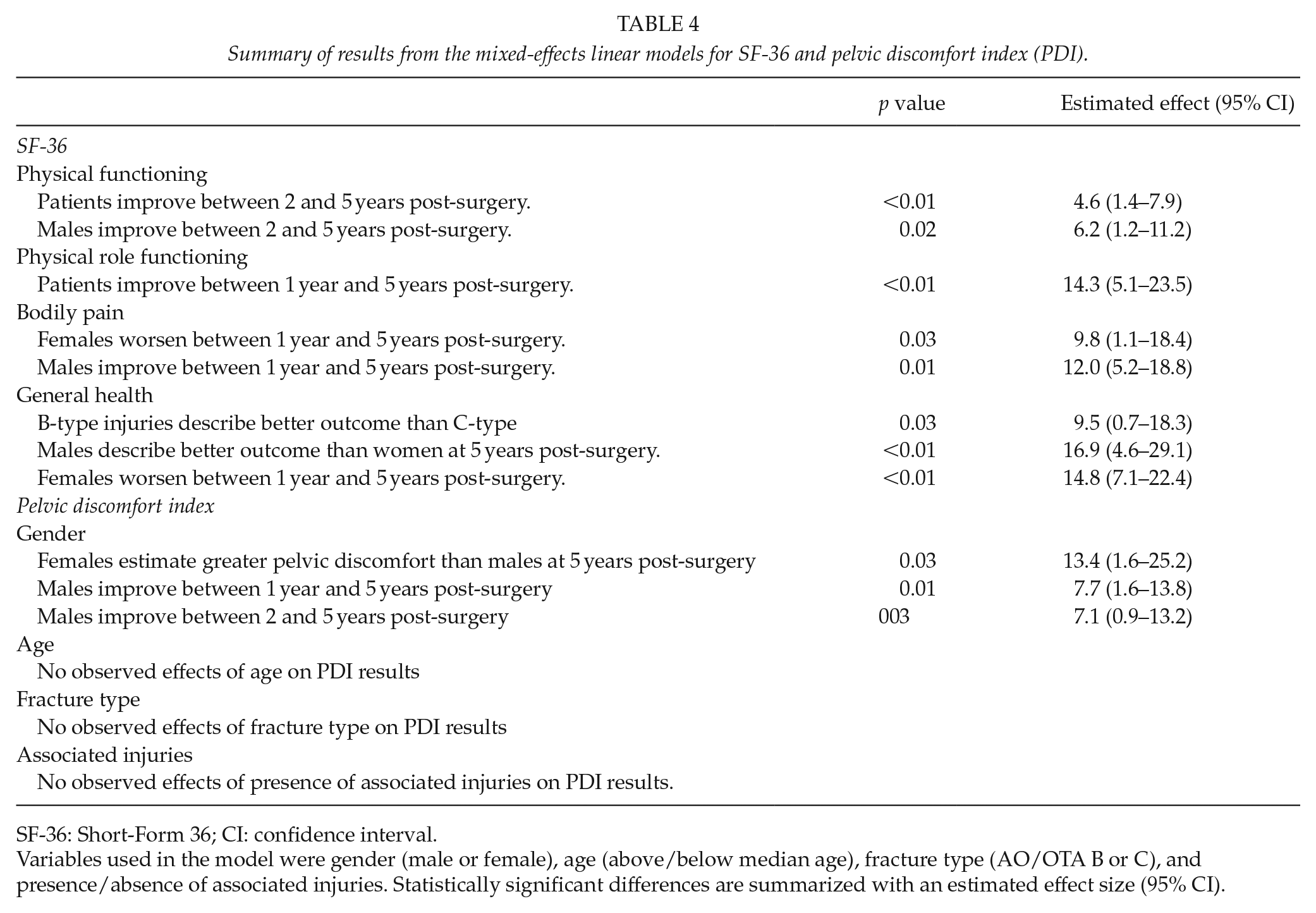
SF-36: Short-Form 36; CI: confidence interval.
Variables used in the model were gender (male or female), age (above/below median age), fracture type (AO/OTA B or C), and presence/absence of associated injuries. Statistically significant differences are summarized with an estimated effect size (95% CI).
Pelvic discomfort index
Mean score at 5 years post-surgery was 27, indicating moderate residual pelvic discomfort overall. The PDI was largely stable when comparing results of the entire study population at 1, 2 and 5 years post index surgery. No significant improvement or worsening in patient-reported pelvic discomfort was observed at 5 years post-surgery compared to earlier measurements.
Examining the influence of variables such as gender, age, fracture type, and presence of associated injuries, it was found that females reported a higher level of pelvic discomfort at 5 years compared to males (p = 0.03). Males recovered over time with less pelvic discomfort at 5 years compared to results at 2 years (p = 0.03). Females reported an increase in pelvic discomfort at 5 years post-surgery, although this change was not found to be statistically significant (Table 4).
None of the variables such as age, fracture type (B/C), or presence of associated injuries were found to have an influence on reported pelvic discomfort.
Neurologic Injuries
Analysis of neurologic sequelae was not a primary objective of the present study. Hence, no routine neurophysiological examination was performed to allow for a systematic evaluation of permanent neurologic injury. Using the PDI question regarding problems with leg sensation as a marker of neurologic injury, 30 of 78 patients (38%) described no problems with affected leg sensation whatsoever at 5 years post-injury. Twenty-seven patients (35%) reported very little to moderate problems. Severe to very severe problems with leg sensation was reported by 21 of 78 patients (27%) at this time-point. There were no reoperations due to neurologic injury.
Discussion
The results in the present study indicate that the negative impact on patient-reported outcome after surgical treatment of pelvic ring injuries is substantial and long standing, with patients failing to reach norm values in all eight domains of the SF-36 at 5 years post-surgery. This impairment is coherent with findings in earlier literature (12–16). However, even at 5 years post-surgery, a slow recovery of physical functioning was observed with improvement still noticeable at 5 years post-surgery. Studies with shorter follow-up will miss this encouraging change.
Females reported a worse functional outcome than males at 5 years following surgical treatment of pelvic ring injuries. This relationship was observed for both the generic (SF-36) and the condition-specific (PDI) outcome measure. Such an association between gender and long-term patient-reported outcome has only scarcely been reported in current literature concerning pelvic ring injuries (17) and studies concerning patient-reported outcome following major trauma (18). Our findings are in coherence with these studies. Notably, outcome for males and females in the present study was largely similar at 1 year and 2 years post-surgery and then diverged at 5 years post-surgery. Although it is not possible to define where in the time-span differences occurred, there is a possibility for studies with a shorter follow-up than 5 years to miss this change.
Speculating on the reasons behind the difference in outcome between genders, there is a multitude of potential influencing factors. One question that could be raised is whether the impact of deterioration in reproductive health, which has been demonstrated both in males (19–21) and females (22–24) following pelvic ring injuries, has a greater effect on self-reported outcome for the latter. The rate of cesarean sections is increased in females who have suffered pelvic ring injuries, although the reasons for this are largely unknown (25). Hence, obstetric issues might influence reported outcome in younger females who have suffered a pelvic ring injury. In the present study, we also found that females (n = 9; 23%) were more likely to undergo subsequent implant removal than men (n = 3; 4%), although we were unable to establish the reasons for this.
Psychological factors could also help explain the different outcome between genders, as studies have shown that females are more likely to develop depression and post-traumatic stress disorder following trauma (18, 26). However, it seems reasonable that this would influence the results at an earlier stage in follow-up and not demarcate itself at 5 years post-trauma as in the present study. It is also important to emphasize that while interesting, the demonstrated outcome discrepancy between genders should be interpreted carefully. Results may be influenced by confounding factors. For example, that the outcome instruments used could behave differently between genders. This has been exemplified by studies examining the use of SF-36 in healthy populations, where females reported more negative change than males over time as well as poorer health in general, with the exception for general health perceptions (27). In conclusion, further studies are needed to confirm this gender discrepancy and investigate potential underlying reasons and their implications.
Notably, variables such as age and fracture type had only a limited impact on patient-reported outcome in the present study and presence or absence of associated injuries had none. This is contradictory to previous studies that have reported an unfavorable outcome in patients with associated injuries such as concomitant lower extremity fracture or nerve injury. (17, 28) However, discrepancies in study design, demographics, treatment modalities, and follow-up protocol make comparisons difficult. It should be noted that these variables are relatively broad; there are, for example, a vast number of different associated injuries, and some of them might and might not have the potential of influencing PROMs.
Strengths and Limitations
We believe that the strengths of this study lie in the prospective design, the true consecutive series of patients included, and the use of validated outcome measures. However, there are several limitations that must be considered. Given the 5-year follow-up and the demographics of the study population with one-fifth of patients suffering from preexisting psychiatric comorbidity such as substance abuse and schizophrenia, we consider the response rate acceptable. However, there is a risk for selection bias that must be considered. There are also different types of response bias, such as acquiescence and social desirability that might influence the results.
Another aspect that should be considered is the possibility for patients to adapt to a new level of functioning post-injury, which may change their values or internal standard of measurement. That could affect their self-reported QoL, making interpretation more difficult. This adaptation is referred to as response shift (29). The study design did not allow for determining whether a response shift was present, but the possibility for such an effect should be considered (30).
The mixed-effects linear model used for statistical analysis of PROM data allowed for examining the influence of variables such as age, gender, fracture type, and presence of associated injuries on outcome. However, to avoid risk of overfitting the model, some variables of interest had to be left out. For example, we did not examine the influence of residual posterior displacement using this model. Our study was also too small to allow for comparison of outcome in subsets of injury patterns. These two factors have previously been demonstrated to influence outcome (3, 17). Furthermore, as previously mentioned, the data concerning neurological injuries in our study were also limited.
Future studies could be directed toward examining the influence of above variables in detail. The aim of the present study, however, was to describe the long-term patient-reported outcome after surgical treatment of pelvic ring injuries overall.
Conclusion
Surgically treated pelvic ring injuries are associated with long-standing negative effects on patient-reported outcome, with patients failing to reach population norm values in all domains of the SF-36 at 5 years post-injury. Males report a better outcome than females at 5 years post-injury and also report improvement between 2 and 5 years, while women on the contrary report deterioration.
Footnotes
Authors’ Note
This study was approved by the regional ethics board in Uppsala, Sweden. Approval number: 2006/140.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.