
Abstract
Background and Aims:
Injuries involving major arteries are an important cause of mortality and morbidity, most often from road traffic accidents. Our aim was to study the outcome of major vascular trauma from traffic accidents in an entire population, including patients who die at the scene and those who reach hospital alive.
Materials and Methods:
This was a retrospective analysis of all patients who sustained major vascular trauma in traffic accidents in Iceland from 2000 to 2011. Patient demographics, mechanism, and location of vascular injury and treatment were registered. Injury scores were calculated and overall survival estimated.
Results:
There were 62 individuals (mean age 44 years, 79% males) with 95 major vascular traumas, giving an incidence of 1.69/100,000 inhabitants (95% confidence interval: 1.27–2.21). A total of 33 died at the scene and 8 during transportation to hospital but 21 (34%) reached hospital alive. Most patients who succumbed had thoracic major vascular traumas (76%) or abdominal major vascular traumas (23%). Mean new injury severity score for the 21 admitted patients was 44. A total of 18 were operated with vascular repair, 3 with endovascular stent graft insertion. The mean hospital stay for discharged patients was 34 days. Altogether, 15 of the 62 patients (24%) survived to discharge from hospital, with a 5-year survival of 86% for discharged patients.
Conclusion:
Every other patient with major vascular trauma following traffic accidents died at the scene and a further 13% died during transportation to hospital, most of whom sustained major vascular trauma to the thoracic aorta. However, one-third of the patients reached hospital alive and 71% of them survived to discharge, with excellent long-term survival.
Introduction
Annually, around 50 million individuals worldwide sustain severe injuries following traffic accidents, and a significant number either die or suffer significant morbidity related to major vascular trauma (MVT) (1). Traffic accidents are the leading cause of MVT in civilian practice and are the major cause of death in individuals aged between 15 and 29 years (1, 2). During the last decade, the incidence of MVT has increased in most parts of the world, mostly because of an increasing number of vehicle accidents.
Thoracic MVTs have the highest mortality and the thoracic aorta is the most commonly injured vessel, usually after blunt injury (3). Blunt-deceleration high-speed vehicle injuries can also affect renal, hepatic, and splenic arteries but the major cause of death from abdominal MVTs is exsanguination following abdominal aortic disruption (3).
Although up to 30% of patients die at the scene in vehicle accidents (4), few studies have focused on pre-hospital death due to MVT in road traffic accidents (5). Most studies on MVT have concentrated on morbidity and mortality in patients who survive to hospital admission, but in-hospital mortality ranges from 18% to 24% (6–9). In order to reduce the mortality and morbidity of MVTs from traffic accidents, it is very important to identify and evaluate the risk factors not only for patients who survive transportation to hospital but also for those who die at the scene.
We, therefore, wanted to study the incidence, risk factors, outcome, and treatment of patients who sustained MVT from road traffic accidents in the whole Icelandic population over a 12-year period, including the patients who died at the scene or during transportation to hospital.
Material and Methods
Study Design
This was a retrospective study involving all patients who sustained MVT in traffic accidents in Iceland between 1 January 2000 and 31 December 2011. The study was approved by the Icelandic National Bioethics Committee (VSNb2012070031/03.15). As individual patients were not identified, individual consent was waived.
Trauma Care in Iceland
In Iceland, with a mean population of 303,383 during the study and 319,575 inhabitants at the end of December 2011, primary trauma care is provided at Landspitali University Hospital in the Capital Region of Reykjavik, and also at seven smaller hospitals, including one in each quarter of the country (10). The second largest trauma unit, at Akureyri Hospital, is a trauma center that serves a population of around 35,000 (including around 17,000 living in Akureyri) in the northern and eastern parts of Iceland (Fig. 1).
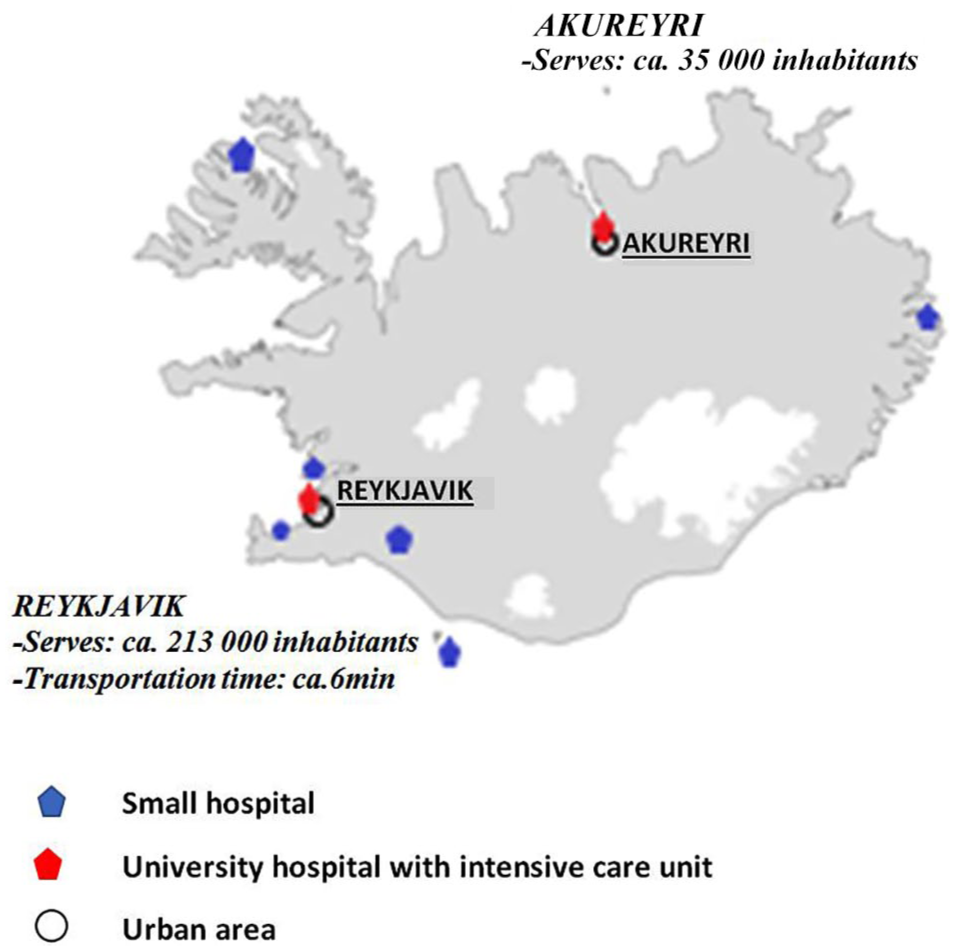
Trauma care in Iceland, hospitals, and transportation time. Primary trauma care is provided by Landspitali University Hospital in the Capital Region (Reykjavik) and also by seven smaller hospitals, including one in each quarter of the country. Landspitali is the only major trauma hospital in Iceland. The second largest hospital is Akureyri Hospital (10).
All medical specialities are represented at Landspitali, which offers all major trauma care with an Advanced Trauma Life Support (ATLS) certified trauma team. The patients are transported to hospital either in an ambulance staffed by a paramedic or in a helicopter/plane, escorted by a physician. Every year, over 25,000 trauma patients are treated at Landspitali, with around 60 of them presenting with severe injuries (i.e. injury severity score (ISS) above 15) (11).
In this study, injury sustained within Reykjavik and Akureyri was defined as urban trauma, but 50% of all major traffic accidents occur in the urban areas (12).
Study Population and Sources of Data
All patients ⩾18 years of age who sustained MVT in traffic accidents were included in the study. Traffic accident victims were defined as having injury from a motor vehicle accident, a motorcycle accident, or a bicycle accident–even including pedestrians. To capture all the cases of MVT, several databases were cross-checked, including a separate intensive care unit (ICU) database, and diagnosis and operation registries at Landspitali and all the regional hospitals. For patients who died at the scene of the accident or during transportation to hospital, the forensic autopsy databases of the Medical Examiner Office of Iceland and the Department of Pathology at Landspitali (where all the autopsies in Iceland are performed) were checked. For the same period, the Cause of Death Registry at Statistics Iceland was checked and compared with the clinical and autopsy databases.
We also checked a centralized trauma database at Landspitali that includes all patients admitted to the ICU from the emergency department (ED), together with computerized diagnosis and operation registries at Landspitali and the regional hospitals in Iceland. This search included the following ICD-10 discharge diagnoses: S15-18, S25-28, S35-38, S45-48, S75-78, and S85-88. Vascular injuries to the head or to solid organs in the abdomen or thorax (i.e. involving the cerebral or coronary arteries) were excluded.
Classification of Vascular Injuries and Injury Score
Vascular injuries were classified into five anatomical zones based on the location of the injury: (1) neck, (2) thorax, (3) abdomen, (4) upper limb, and (5) lower limb. The Abbreviated Injury Score (AIS 90 code) was then used to classify injuries. Baseline demographic information and clinical data were collected on a standardized data sheet from pre-hospital reports, patient charts, surgical reports, and autopsy descriptions if the patient had died within 30 days of the accident. The presence of signs of life (SOL) was registered during the pre-hospital phase and transportation of the patient, and also on arrival at the ED. SOL was defined as being at least one of the following: spontaneous respiratory effort, pupillary response, extremity movement, measurable or palpable blood pressure, or cardiac electrical activity. ISS and new injury severity score (NISS) (13–15) were calculated for all patients who were admitted to hospital. Based on the physiological status on first medical contact (Glasgow Coma Scale (GCS), respiratory rate, and systolic blood pressure), both the revised trauma score (RTS) and the chance of survival (PS) (using the trauma-injury severity score (TRISS) methodology) were calculated (16, 17).
Outcome Parameters and Follow-Up
The primary outcome analyzed was all-cause long-term mortality (overall survival) and neurological outcome using the Glasgow Outcome Scale (GOS) and the American Spinal Injury Association (ASIA) Impairment Scale (18, 19). Short-term mortality was defined as death before reaching hospital, or death within 30 days of injury. Long-term survival was defined as survival from the day of the index event until death or end of follow-up. Individuals who died before arrival at hospital were excluded from survival calculations. Information on survival of all patients was available from Statistics Iceland and was 100% complete. Two foreign visitors were excluded from long-term survival analysis but were included in short-term data.
End of follow-up was 31 December 2015. Mean and median follow-up of patients who arrived at the hospital alive was 6.1 and 6.5 years, respectively (range: 9.4–11.8). Normal neurological outcome was defined as functional status without any major sequelae and the ability to perform activities of daily living without difficulty.
Statistical Analysis
Microsoft Excel (Office 16) was used for descriptive statistics, both for continuous and categorical variables; further statistical analysis was done using R software version 3.3.2. Incidence was calculated according to the age and gender distribution of the population as derived from National Statistics Iceland, standardized to the World Health Organization (WHO) European Standard Population. Annual percent change and also differences in incidence according to residency were estimated with Poisson regression. Continuous variables are expressed as mean ± standard deviation (SD) and categorical variables as percentage. Student’s t-test was used for continuous variables, and the Chi-square test and Fisher’s exact test were used for categorical variables. Odds ratios (ORs) for predictors of short-term mortality (<24 h or 30-day mortality) were estimated with logistic regression. Cases of death before arrival at hospital were excluded from the risk analysis. Long-term survival was estimated using Kaplan-Meier analysis and difference in survival according to gender was estimated by log-rank test.
Results
Patient Demographics and Incidence
During the 12-year study period, 62 patients fulfilled the study criteria of sustaining MVT following a traffic accident; the total number of MVTs was 95, which included 77 injured arteries and 18 veins (Table 1). Two of the patients were foreign travelers. This gives an incidence of MVT following a traffic accident of 1.69 per 100,000 inhabitants (95% CI: 1.27–2.21) for the entire 12-year study period (Fig. 2), 2.70/100,000/year (95% CI: 1.96–3.64) for men and 0.65/100,000/year (95% CI: 0.32–1.20) for women. A significant fall in the incidence rate of MVT was observed during the course of the study: from 2.87/100,000 in the year 2000 to 0.94/100,000 in 2011, with an annual mean percent change (APC) of 0.92 (p = 0.0272).
Injured arteries and veins in patients with major vascular injuries following traffic accidents in Iceland, 2000–2011.
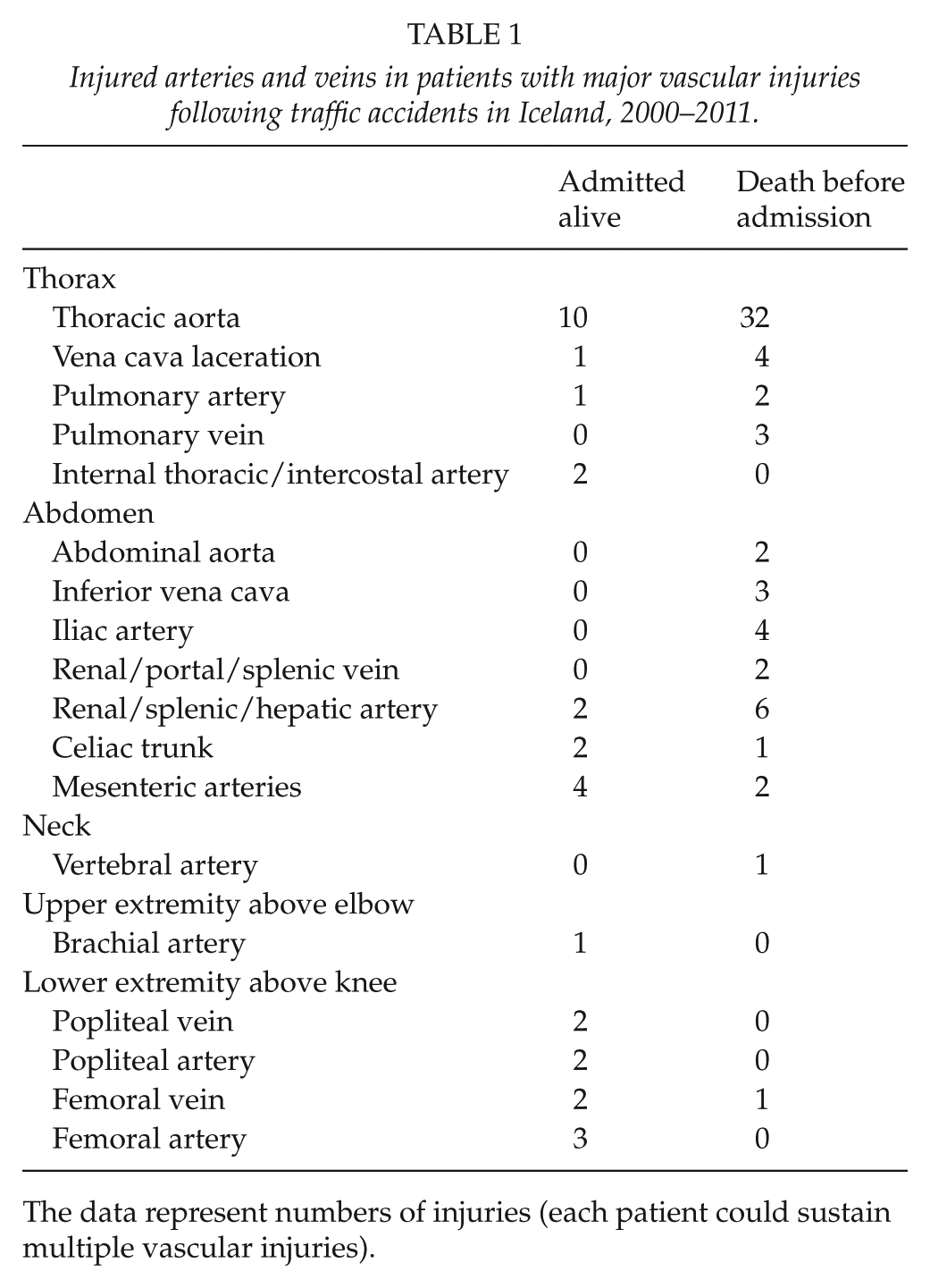
The data represent numbers of injuries (each patient could sustain multiple vascular injuries).
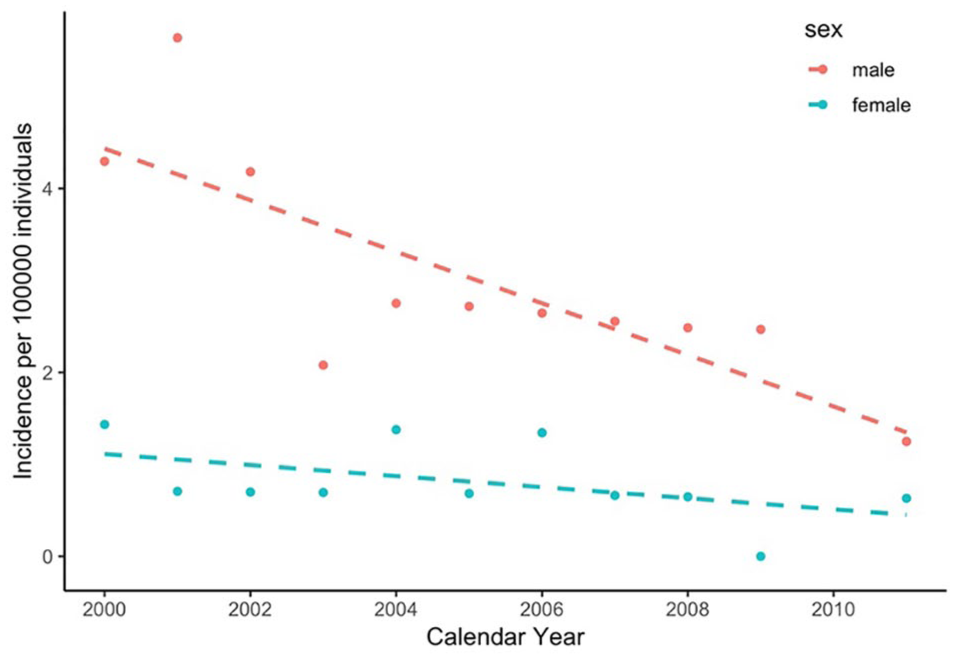
Incidence rates of major vascular trauma following traffic accidents in males (red) and females (blue) in Iceland, 2000–2011.
The baseline patient characteristics are given in Table 2. The mean age was 44 ± 18 years: 43 ± 17 years for the 49 men and 49 ± 20 years for the 13 women.
Baseline characteristics of patients with major vascular trauma following traffic accidents in Iceland, 2000–2001.
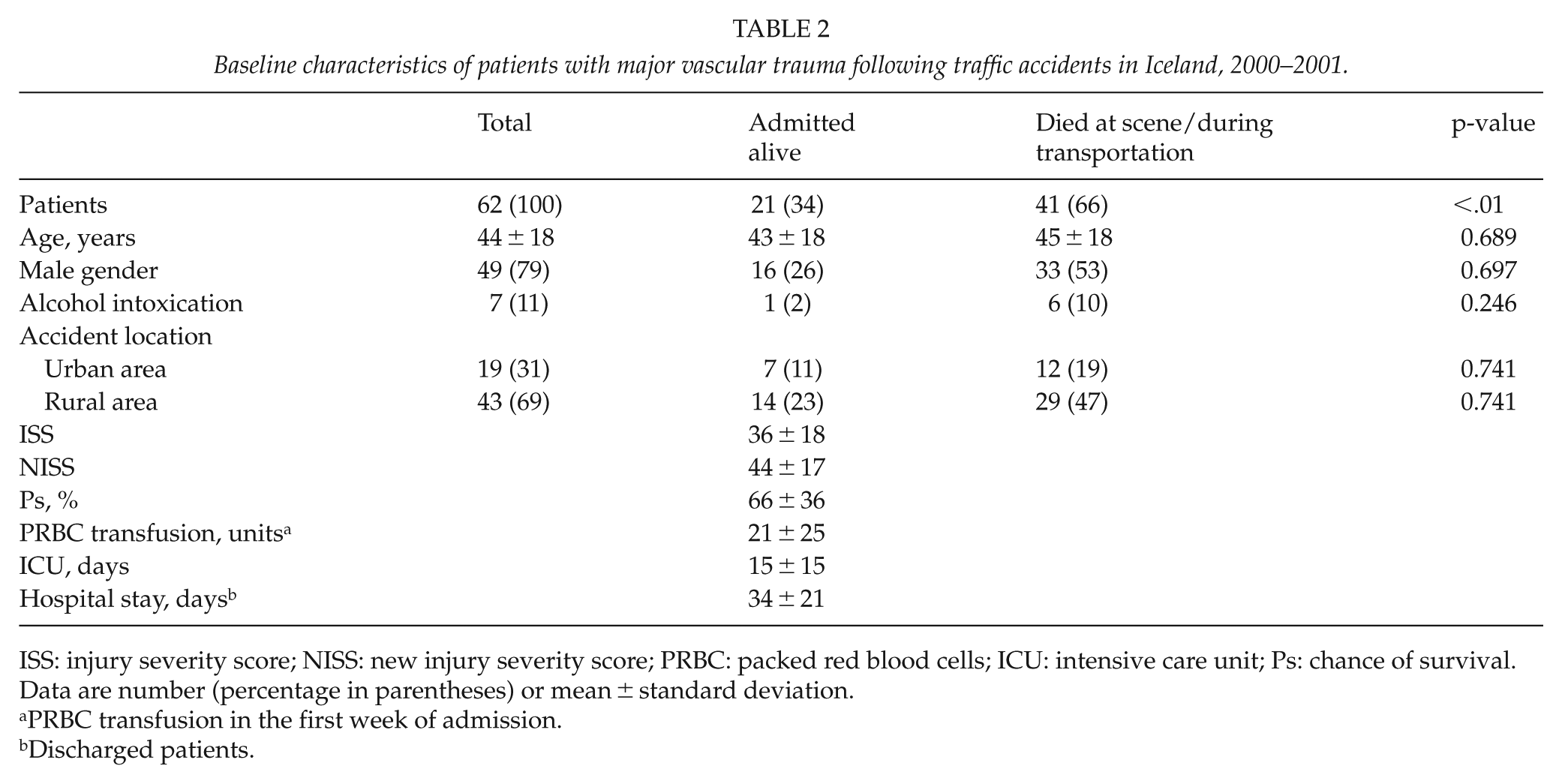
ISS: injury severity score; NISS: new injury severity score; PRBC: packed red blood cells; ICU: intensive care unit; Ps: chance of survival.
Data are number (percentage in parentheses) or mean ± standard deviation.
PRBC transfusion in the first week of admission.
Discharged patients.
type of Trauma, Location of Injury, and Early Mortality
The cause of injury for the 62 individuals included 52 motor vehicle accidents, six motorcycle accidents, one bicycle accident, and three pedestrian accidents. Fig. 3 shows the cause of the MVT following traffic accidents. A total of 47 patients (76%) had thoracic MVT and 19 (31%) had MVT to the abdominal region. Of the nine patients who had combined thoracic and abdominal MVT (15% of the group), all died before being admitted to hospital. Thoracic MVT was involved in 88% of the injuries (36/41) in patients who died before admission and in 52% of the injuries (11/21) in those who were admitted to hospital (p < 0.002) (Table 1). Most commonly, these injuries involved the thoracic aorta (n = 42) where 30-day mortality was 72% (34/47). Of the 41 patients who did not reach hospital alive, 78% (32/41) had thoracic aortic injury, as compared with 48% (10/21) of those who reached hospital alive (p = 0.015). In 77% of the fatal thoracic aortic trauma cases (26/34), there had been a frontal collisions and 74% of the cases happened in rural settings.
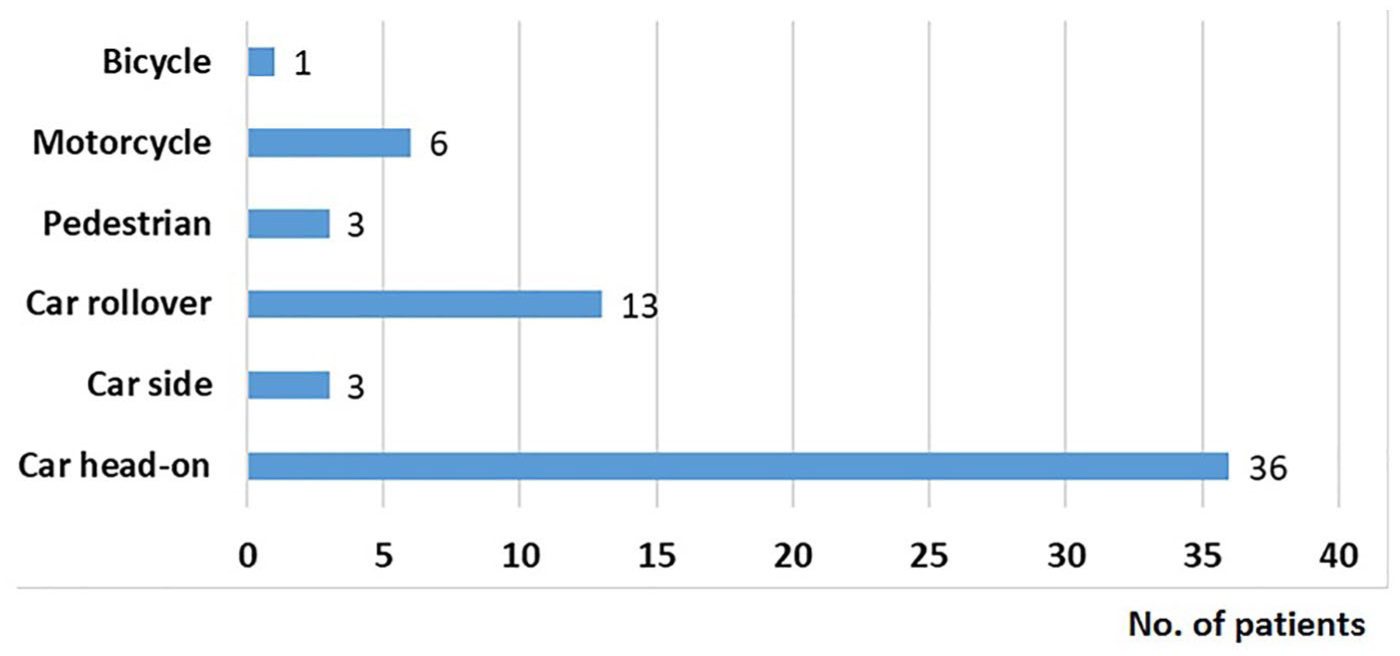
Reasons for accident-related injury in patients with major vascular trauma following traffic accidents in Iceland, 2000–2011.
MVTs in the abdominal area accounted for 32% (13/41) of all injuries in patients who died before admission and for 29% (6/21) of all injuries in those who were admitted to hospital (p = 0.803). Only one of the patients who was admitted with MVT in the abdominal area died within 30 days.
Rural Versus Urban Injury
A significantly higher proportion of individuals (69%) sustained their injuries in the rural (as opposed to urban) areas (69% vs 31%, p < 0.01) (Reykjavik area, n = 18; Akureyri area, n = 1). The mortality before admission to hospital was 67% (29/43) and 63% (12/19), respectively, for these two areas. Of the 14 individuals in the rural group who were admitted alive, 13 survived for more than 30 days and 11 were discharged. In the urban group, four of the seven patients who were admitted survived for more than 30 days, and all four were discharged.
Severity of Injury
The mean ISS and NISS values for patients who were admitted were 36 ± 18 and 44 ± 17, respectively, and with one exception all the patients had ISS and NISS scores above 15, indicating severe injury. The mean estimated chance of survival (Ps) was 66% (Table 2).
Hospital Stay and Number of Transfusions
The mean hospital stay was 34 ± 21 days (median 35 days) for the 15 patients who were discharged (range: 6–62 days). The average number of transfusions of packed red blood cells (PRBCs) administered within the first week of admission for these patients was 21 ± 25 units. This included nine patients who received 10 or more units of PRBCs in the first 24 h after hospital admission (Table 2).
Early Outcome and Treatment
Of the 62 patients in the study, 41 (66%) died before admission, including 33 who died at the scene of the accident and 8 (13%) who died during transportation to hospital; the other 21 patients (34%) reached hospital alive. Of the 21 who survived until admission, 18 were operated on– 16 of them with open vascular repair. A total of 16 patients of the 18 were operated on within the first 24 h of admission, three of them with acute endovascular stent graft insertion. One patient Underwent an emergency thoracotomy during ambulance transportation, but he died before reaching hospital (Fig. 4).
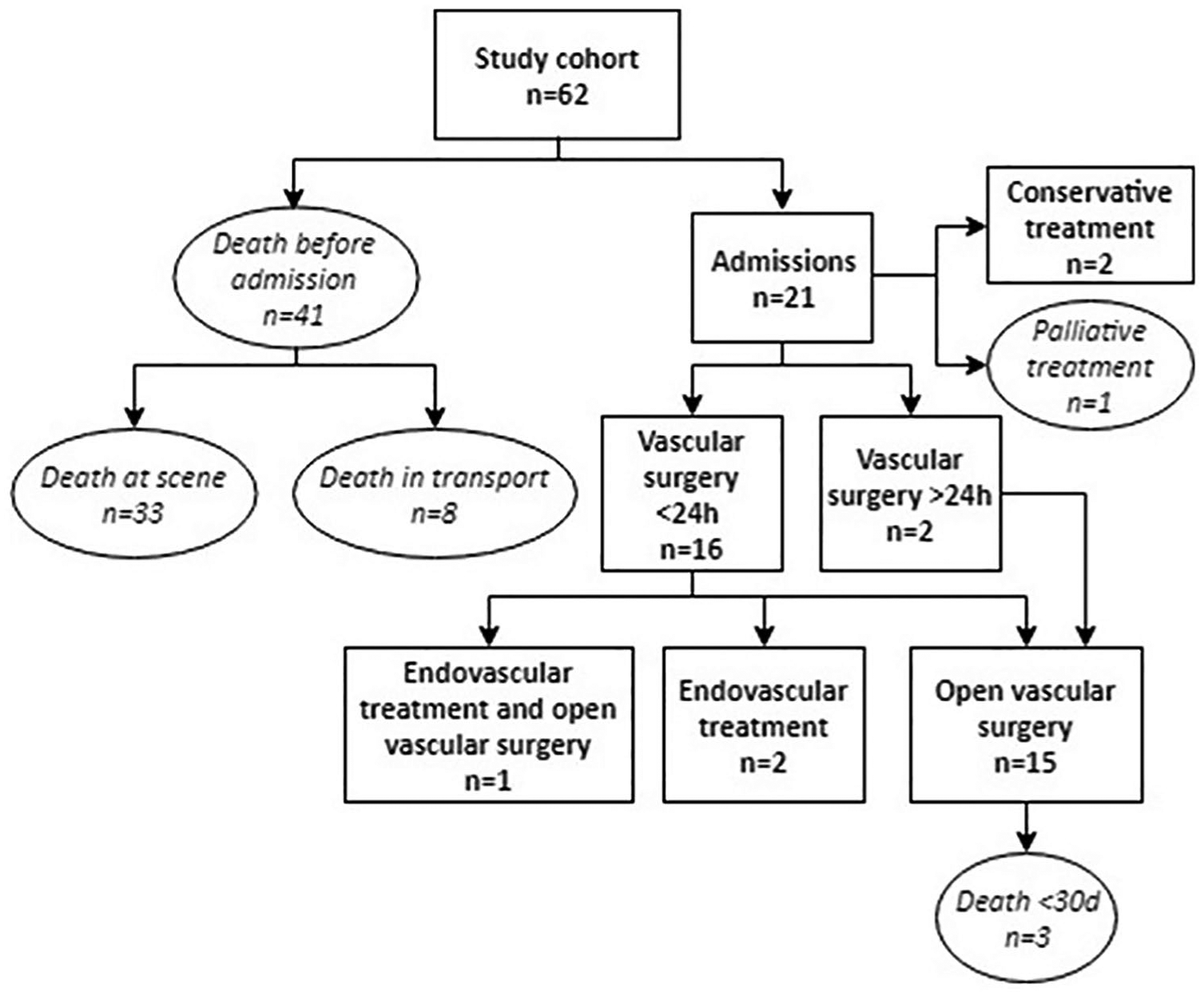
Flow chart showing the management of, and outcome in 62 patients with major vascular trauma following traffic accidents in Iceland, 2000–2011.
Of the 21 patients who were admitted, four (19%) died within 30 days. Each of these four patients had a GCS of less than 8 and severe shock, and all of them succumbed within 24 h (Fig. 4). Two patients died after 30 days of treatment and were never discharged. Altogether, 47 of the 62 patients (76%) died within 30 days of their injury.
Late Survival
The long-term survival of the 21 individuals who were admitted to hospital with MVT was 86% at both 1 year and 5 years, and this was not significantly different for men and women (log-rank test, p = 0.31).
The neurological outcome in the 15 patients who survived the injury and were discharged from hospital included one case of mild brain damage (GOS 5), two cases of spinal cord injury (both ASIA A), two patients who had had their limb amputated, and one patient with both spinal cord injury (ASIA E) and amputation.
Discussion
In this study, the epidemiology of MVT from traffic accidents was investigated in an entire population, and in contrast to most previous studies on MVTs we not only focused on those individuals who died before admission, but also on those who reached hospital alive. This was made possible by checking all forensic autopsies in the centralized database of the Medical Examiner Office of Iceland, as all patients who die from accidents outside hospital in Iceland must undergo forensic autopsy, by law.
In this study, the annual incidence of MVT following traffic accidents was 1.69 per 100,000 inhabitants. According to the Icelandic Transport Authority, 16,204 individuals were injured in traffic accidents over the 12-year period of this study, with 12% of them being considered to be seriously injured and 2% dying within 30 days (20). As shown in Fig. 5, the rate of road fatalities is relatively low in Iceland, or 4.6 per 100,000 inhabitants per year, as compared with 17.4 per 100,000 inhabitants in the rest of the world (1). Even so, according to WHO, Iceland has the second highest fatality rate in road accidents in the Nordic countries, after Finland (1).
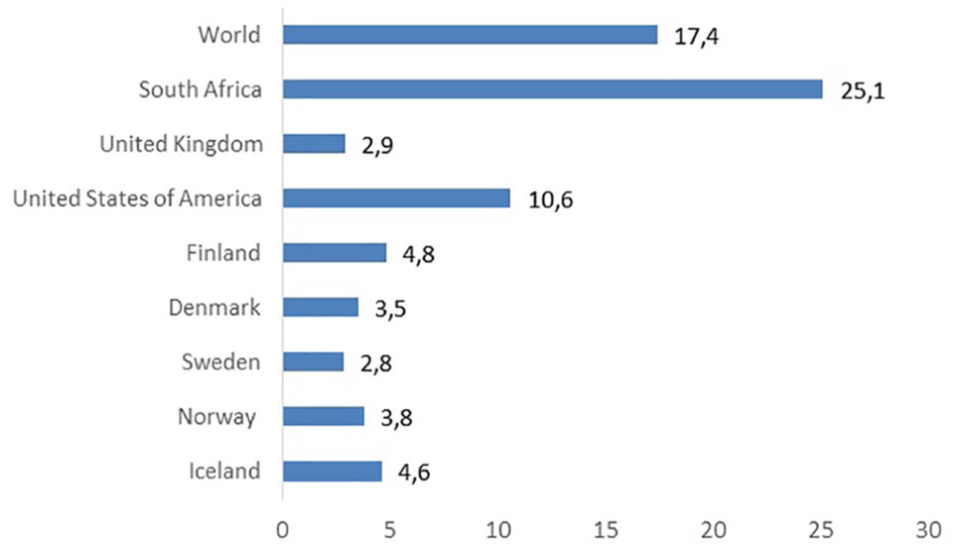
Estimated road traffic death rates in different countries per 100,000 population.
Two-thirds of the patients in this study either died at the scene of the accident or during transportation to hospital. Furthermore, of the one-third patients who reached hospital alive, 29% did not survive long enough to be discharged. Studies on patients with MVT who survive until hospital admission have found mortality rates in the 18–24% range (6–8).
Clinical signs following aortic injury can be unreliable, and delays in recognition and management is associated with greater mortality and a longer hospital stay (21, 22). Thus, individuals with MVT who are injured in rural areas often have a less favorable outcome than urban residents (3, 23, 24). In this study, a significantly higher proportion of individuals (69%) sustained their injuries in the rural parts of Iceland (p < 0.01). For comparison, in other studies including all trauma patients admitted from rural areas, survival rates have varied from 70% to 80%, compared with 93% in this study for patients with MVT following traffic accidents (25, 26).
Although safety measures designed to minimize the occurrence of aortic injuries have improved, the incidence of blunt aortic injury in fatal motor vehicle accidents has not decreased during the past decade (27). Studies on MVT patients have shown that transections of the thoracic aorta and major injuries to the abdominal veins have the highest mortality (28), with up to 80% of injuries resulting from motor vehicle accidents at high speed, after rapid deceleration following head-on or side-impact collisions (29). When traffic streams are not separated using barriers, as is often the case in rural areas of Iceland, head-on collisions are frequent and they are the most likely type of collision to cause fatality and severe injury (6).
A study by Williams et al. (29) showed that the incidence of trauma to the aorta in fatal motor vehicle accidents was very high, or about 17%, and death occurred before admission (at the scene of the accident) in 44% of cases–with 94% of the victims dying within 1 h of injury. This is in line with the results of this study were the majority of patients who died had fatal aortic injury, with 74% of them dying in rural settings. Our findings, therefore, highlight the high mortality of patients at the scene of the accident, especially in rural areas, with trauma to the thoracic aorta being the major cause of death.
For the 21 patients who were admitted alive, 14 underwent open surgery within 24 h of admission–most often laparotomy or thoracotomy. The golden standard for management of all vascular injury over the past 50 years has been open surgery with primary repair, vein patch, and interposition or bypass grafting (21). This strategy has been challenged by rapid developments in the fields of imaging technology and endovascular treatment. Three patients in our study had endovascular stent graft insertion within the first 24 h after admission. However, patients with haemorrhagic shock and classical signs of arterial injury should still be taken immediately to open surgery (21, 30). In a modern setting, MVT can be treated with open and endovascular technology in a hybrid OR.
The main strength of this study was the well-defined study population representing a whole nation with a modern single-payer, nationalized healthcare system. A further strength was the fact that we had access to centralized nationwide hospital and autopsy databases, together with detailed patient records and survival follow-up that was 100% complete. The main limitation of the study was the small number of cases of MVT in a population that is relatively small. Another limitation was the retrospective design, with potential bias.
Conclusion
In summary, MVT from traffic accidents is an uncommon injury in Iceland with an incidence of 1.69 per 100,000 inhabitants (95% CI: 1.27–2.21). Men were injured almost four times more often than women, and two of every three individuals who sustained MVT died before reaching hospital, with significantly more individuals being injured in the rural parts of Iceland. The most serious vascular injuries were to the thoracic aorta, usually because of a frontal car collision. Patients who were admitted alive were often severely injured and in need of emergency surgery, with high demands on hospital resources. However, most patients who were admitted survived to discharge and there was a good 5-year survival rate (86%).
Footnotes
Acknowledgements
Special thanks to Gunnhildur Johannesdottir for collection of data and medical chart collection, Ingibjorg Richter for searching the Landspitali databases, Dr Karl Logason MD (Landspitali, Reykjavik, Iceland) in planning the study, and Professor Bjarni A Agnarson MD (Landspitali, Reykjavik, Iceland) for help in acquiring autopsy data. We also thank Dr Gustav Pedersen (Haukeland University Hospital, Bergen, Norway) and Professor Einar Stefansson (Landspitali, Reykjavik, Iceland) for giving valuable comments.
Author Contributions
All the authors of this research paper directly participated in the study. B.K.J., B.M., and T.G. participated in planning the study. B.K.J. did the data collection. B.K.J., T.J., T.G., B.M., and S.H.L. interpreted the data and S.H.L. performed part of the statistical analyses. B.K.J., U.J., B.M., and T.G. wrote the manuscript, with B.K.J. being the major contributor. All of the authors read, commented on, and approved the final version submitted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Landspitali University Hospital Scientific Fund and the University of Iceland Research Fund.