
Abstract
Background and Aims:
Circulatory arrest carries a high risk of neurological damage, but modern monitoring methods lack reliability, and is susceptible to the generalized effects of both anesthesia and hypothermia. The objective of this prospective, explorative study was to research promising, reliable, and noninvasive methods of neuromonitoring, capable of predicting neurological outcome after hypothermic circulatory arrest.
Materials and Methods:
Thirty patients undergoing hypothermic circulatory arrest during surgery of the thoracic aorta were recruited in a single center and over the course of 4 years. Neuromonitoring was performed with a four-channel electroencephalogram montage and a near-infrared spectroscopy monitor. All data were tested off-line against primary neurological outcome, which was poor if the patient suffered a significant neurological complication (stroke, operative death).
Results:
A poor primary neurological outcome seen in 10 (33%) patients. A majority (63%) of the cases were emergency surgery, and thus, no neurological baseline evaluation was possible. The frontal hemispheric asymmetry of electroencephalogram, as measured by the brain symmetry index, predicted primary neurological outcome with a sensitivity of 79 (interquartile range; 62%–88%) and specificity of 71 (interquartile range; 61%–84%) during the first 6 h after end of circulatory arrest.
Conclusion:
The hemispheric asymmetry of frontal electroencephalogram is inherently resistant to generalized dampening effects and is predictive of primary neurological outcome. The brain symmetry index provides an easy-to-use, noninvasive neuromonitoring method for surgery of the thoracic aorta and postoperative intensive care.
Keywords
Introduction
Circulatory arrest is used during operations of the thoracic aorta (1), during which organs suffer transient ischemia, with the neurons of the central nervous system (CNS) being the most sensitive to prolonged ischemia (2). Injury is a result of parenchymal hypoperfusion, embolization, or reperfusion injury from both hyperperfusion and systemic inflammation reaction (2). Neuroprotective strategies, such as hypothermia and selective cerebral perfusion (SCP), have decreased the incidence of postoperative neurological complications (1, 3, 4).
Timely detection of these CNS injuries is a major challenge, due to the confounding effects of anesthesia and hypothermia, and the lack of reliable monitoring methods. With reliable detection of CNS ischemia, intraoperative protective strategies and neuroprotective critical care protocols could be better focused to high risk patients. Frontal tissue oxygenation monitoring with near-infrared spectroscopy (NIRS) is widely used to guide the initiation of intraoperative neuroprotective strategies in cardiac surgery (2, 3, 5–7). The NIRS monitoring is used to detect trend changes in regional hemoglobin oxygen saturation (rSO2), as specific saturation levels have not been directly linked to neuronal damage or outcome (2, 3, 5–7).
Previous studies have shown that certain electroencephalogram (EEG) variables are useful in neuromonitoring (2) and in neurological outcome prediction after hypothermia-treated cardiac arrest (8). However, the use of traditional full EEG montages is limited by monitoring setup and result interpretation (2, 9). A study by Leira et al. (10) showed that after a brief training, critical care nurses recognized correctly only 46% of epileptiform EEG patterns. In addition, traditional EEG evaluation suffers from the generalized dampening effects of both deep hypothermia and anesthesia.
Abbreviated EEG montages covering the frontal or temporal cortices can be used to detect generalized EEG changes, such as burst suppression, which may predict neurological damage (11). Spectral symmetry of the left and right cortical EEG activity, which is quantifiable by the brain symmetry index (BSI; hemispheric EEG power spectra differences normalized to a range of {0–1}, representing perfect symmetry to total asymmetry, respectively), has shown promising results in neuromonitoring during carotid surgery and stroke management (12–14). During carotid endarterectomy, BSI has been used successfully to detect patients at risk of cerebral ischemia (12, 14). In acute hemispheric stroke, BSI has shown a good correlation with the National Institute of Health Stroke Scale during resolution of symptoms (13) and with clinical improvement during thrombolytic treatment (15). Hemispheric asymmetry is inherently resistant to generalized effects, such as the dampening effect of anesthesia and hypothermia, and even global ischemia typically presents with local or hemispheric differences, which are reflected as changes in the symmetry of EEG spectral power of both hemispheres (16).
The aims of this prospective, explorative study were to search for potential, reliable, easy-to-use, and noninvasive neuromonitoring methods, which are predictive of neurological outcome in patients undergoing hypothermic circulatory arrest.
Material and Methods
In this prospective, single-center cohort study, we recruited 30 adult patients who underwent elective or emergency aortic surgery via a median sternotomy (n = 29; 97%) or left thoracotomy (n = 1; 3%), during cardiopulmonary bypass. All patients were operated under deep (⩽20.0 °C) or moderate (20.1 °C–28.0 °C) hypothermia (17) and circulatory arrest, with optional SCP during circulatory arrest. Anesthesia and ICU sedation were not standardized, representing actual clinical practices. The recruitment period was from November 2007 to May 2011. The sample size was based on a reasonable recruit time. Patients with a neurological disease, symptomatic carotid stenosis, or preoperative neurological symptoms were excluded.
The postoperative primary neurological outcome of a patient was determined good if the patient survived the monitoring period with no significant neurological complications, or poor if the patient suffered a significant neurological complication (new neurological symptoms and lesions on a brain CT scan), or operative death. Mild neurological complications, such as transient delirium, were not classified as a poor outcome.
The monitoring period lasted from the preoperative stage (moments before anesthesia and intubation) until extubation in the ICU, or up to 48 h after surgery. Monitoring included EEG monitoring for the whole period, and NIRS until the patient was out of surgery. Transcranial Doppler (TCD) measurements were performed immediately after surgery, and 24 h after weaning from extracorporeal circulation. Temperature was monitored via a nasal and central venous line catheter. Data collection and assessments were computerized, with all data input and monitoring setup performed by a dedicated study nurse.
All available patients underwent a neuropsychological examination approximately 6 months after surgery, covering cognitive domains of memory, executive functions, processing and motor speed, language skills and visuospatial skills. The neuropsychological performance was considered good if only minor or no cognitive deficits were present, and poor when clinically significant cognitive deficits were present, or if the patient was unable to undergo neuropsychological examination due to a stroke (n = 2). As most cases call for emergency surgery, no baseline neurological evaluation is possible.
Ethics
All participants, or next of kin, gave their written informed consent. Ethical approval (HUS 133/E6/07) was provided by the Helsinki University Hospital Surgical Ethics Committee, Helsinki, Finland.
Neuromonitoring Methods
A continuous EEG recording with a sampling frequency of 500 Hz was gathered with a dedicated measurement module of the compact anesthesia monitor system (Datex-Ohmeda S/5, GE Healthcare). Seven self-adhesive EEG electrodes (Zipprep™, Medtronic) were positioned symmetrically on the frontal area above the eyes (a), on the anterior temporal area (b), and on the mastoid processes (c), with a ground electrode located on the frontal midline (11). All EEG data were recorded with the S/5 Collect Program (GE Healthcare). Four bipolar EEG derivations were used in the analysis: left and right frontal (a to b) and temporal (b to c). The EEG data were reviewed by a clinical neurophysiologist (T.S.) and classified into three categories (non-malignant, malignant, and highly malignant) (18), at three set time points (after anesthesia induction, rewarmed to 30 °C, and sedation break). The second and third analysis points were chosen to minimize the effects of hypothermia and sedation on EEG, respectively (19). Significant artifact corruption was visually identified and removed.
The continuous EEG data were subjected to power spectral analysis, as described in an earlier study (20). For EEG asymmetry quantification, the revised BSI (16) was used with a frequency band of 0.5–25 Hz to derive two separate BSI indices for symmetrical pairs of the frontal and temporal channels between the hemispheres. The BSI values were derived for each 5-s epoch with sliding 1-s intervals and were subjected to a 21-tap median filtering to obtain a more stable BSI trend.
A continuous venous-weighted rSO2 measurement of the frontal cerebral region was performed by a dedicated two-channel INVOS™ 5100C Cerebral/Somatic Oximeter (Medtronic) using NIRS, with sensors placed on the skin symmetrically frontally, just below the hairline. The initiation of circulatory arrest was chosen as a baseline for NIRS outcome analyses. The continuous bilateral rSO2 data were used for two separate analyses. For the first analysis, the surface integral of left and right rSO2 values against time was calculated during circulatory arrest (21). For the second analysis, both NIRS channels were calibrated to zero at the beginning of circulatory arrest, and the evolution of hemispheric NIRS changes with time was derived as an absolute difference between the calibrated NIRS values.
Statistical Methods
Demographic data were analyzed for inherent differences between the outcome groups by the Pearson χ2 test. The relationship of EEG and NIRS asymmetries to primary neurological outcome were assessed, using the EEG data within the 6-h time interval after end of circulatory arrest, and the NIRS data from the onset of circulatory arrest until the end of the NIRS monitoring period.
The median values of BSI for EEG and hemispheric asymmetry for NIRS were derived for each patient. These values were fed to a receiver operating characteristic (ROC) analysis. For BSI and NIRS asymmetry data, the area under curve (AUC) and its standard error (SE) were derived with the jack-knife analysis (22). The reported AUC and threshold values are the means of jack-knife estimates. The applicability of the BSI trend was further evaluated by comparing each BSI sample against the threshold value. Using the threshold value, the percentages of correctly classified samples within the 6-h time period were derived for each patient. The percentage of correct classification represents specificity in the good primary outcome group, and sensitivity in the poor primary outcome group.
Additional outcome analyses at set time points for hemispheric asymmetry and qualitative EEG findings, NIRS variables, TCD measurements, and biochemical data were performed with the Mann–Whitney U test, without multiple comparison correction, or the Pearson χ2 test. The neuropsychological data analysis was performed with the Fisher exact test. The type I error was set at 5% (two-sided) for all statistical tests.
Results
Table 1 presents relevant demographic and clinical data, with no inherent differences detected. Of all the patients, 20 (67%) had a good and 10 (33%) a poor primary neurological outcome. Of all cases, 19 (63%) were emergency operations, 12 (60%) in the good outcome group, and 7 (70%) in the poor outcome group.
Demographic and clinical data.
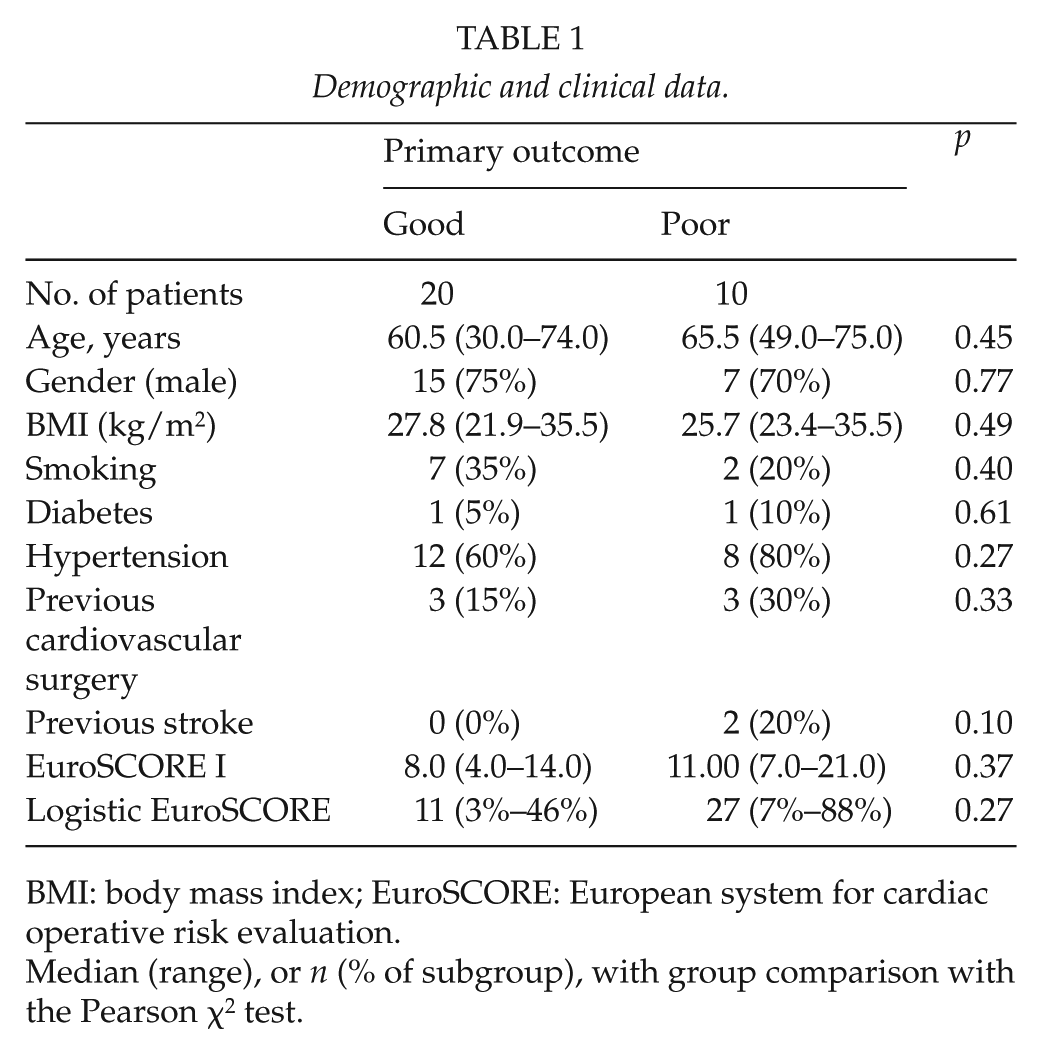
BMI: body mass index; EuroSCORE: European system for cardiac operative risk evaluation.
Median (range), or n (% of subgroup), with group comparison with the Pearson χ2 test.
Table 2 presents relevant surgical, postoperative, and complication data. Three (10%) patients needed short-term postoperative dialysis (14–35 days). Of the three (10%) in-hospital deaths, two were intraoperative due to refractory hypotension and generalized ischemia (including severe neuronal ischemia). One patient died on the 35th postoperative day (POD) without recovering consciousness, with large bilateral ischemic lesions on a postoperative brain CT scan. Patients with a poor primary outcome had higher sequential organ failure assessment (SOFA) scores at admission and on the first POD.
Peri- and postoperative data.
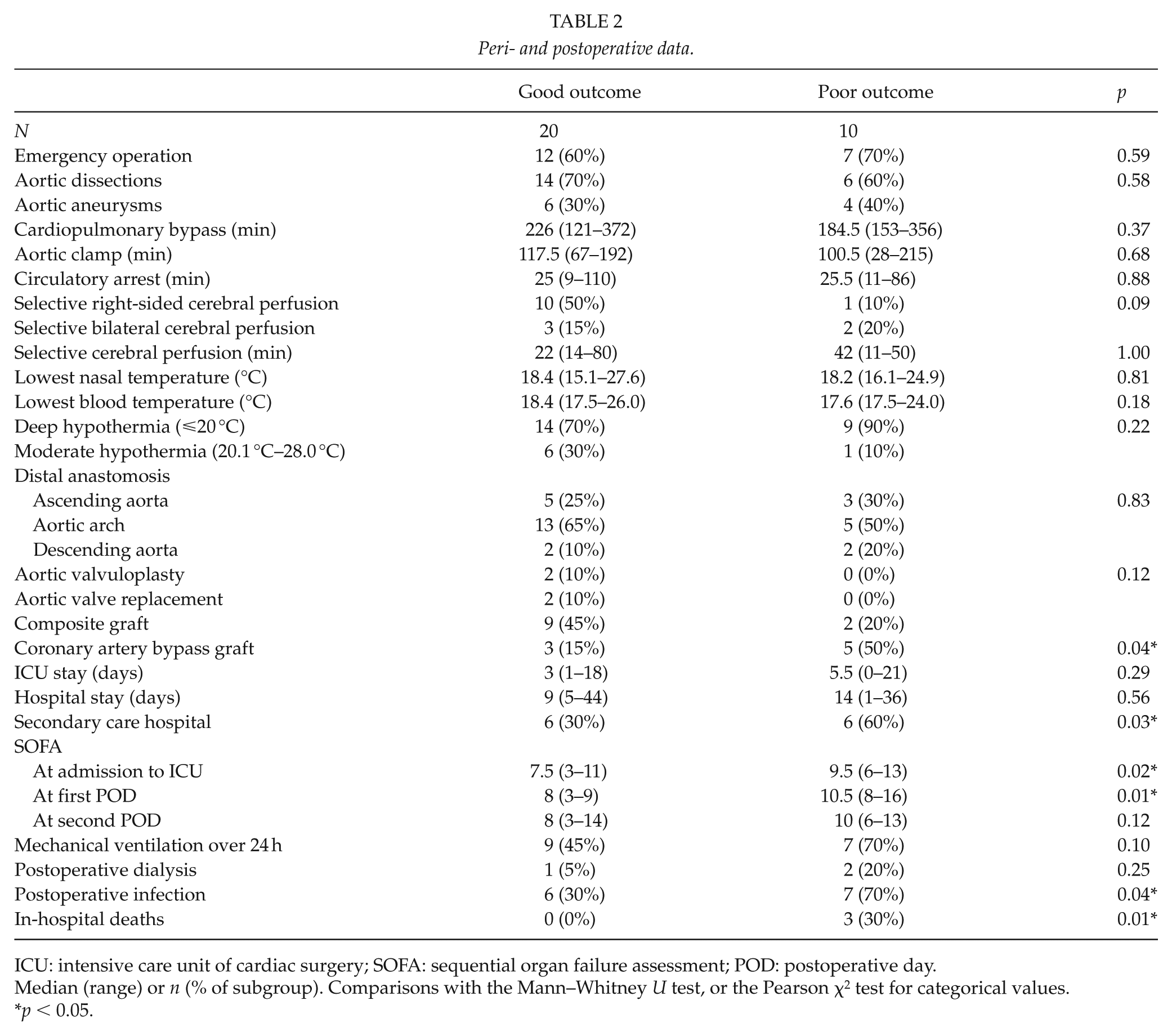
ICU: intensive care unit of cardiac surgery; SOFA: sequential organ failure assessment; POD: postoperative day.
Median (range) or n (% of subgroup). Comparisons with the Mann–Whitney U test, or the Pearson χ2 test for categorical values.
p < 0.05.
All poor primary outcome group survivors had hypoxic–ischemic lesions on a postoperative CT scan. Of the 7 (70%) surviving patients in the poor primary outcome group, one (10%) patient with hypoxic–ischemic encephalopathy remains in permanent tertiary care, and three (30%) patients suffered long-term neurological symptoms (left hemiparesis, two with cortical blindness from an occipital stroke). Three (30%) poor outcome patients made a full recovery.
After artifact removal, 23 (77%) patients’ EEG recordings were analyzed (six had less than 10 min of valid data, one had an erroneous electrode placement). Using the median BSI values of each patient, we obtained AUCs of 0.83 (SE 0.11) between the left and right frontal derivation, and 0.59 (SE 0.15) between the left and right temporal derivations. For the NIRS asymmetry analysis, the AUC value was 0.56 (SE 0.13).
Only the frontal BSI derivation was selected for further analysis, for which the threshold value maximizing the sum of sensitivity and specificity of the median BSI values was 0.51. Using this threshold value, the percentage of correct classification for each patient was calculated. The median (interquartile range (IQR)) of valid monitored data without artifacts was 57 (27%–80%) for each patient (n = 23). From the valid data, the median (IQR) percentages of correctly classified samples was 75 (62%–87%) and 25 (13%–38%) for incorrectly classified samples. Based on these analyses, the threshold value of 0.51 for BSI has a sensitivity (correct classification in patients with a poor outcome, n = 6) of 79 (IQR; 62%–88%) and a specificity (correct classification in patients with a good outcome, n = 17) of 71 (IQR; 61%–84%). These results are illustrated in Fig. 1, and EEG spectra examples in Fig. 2.
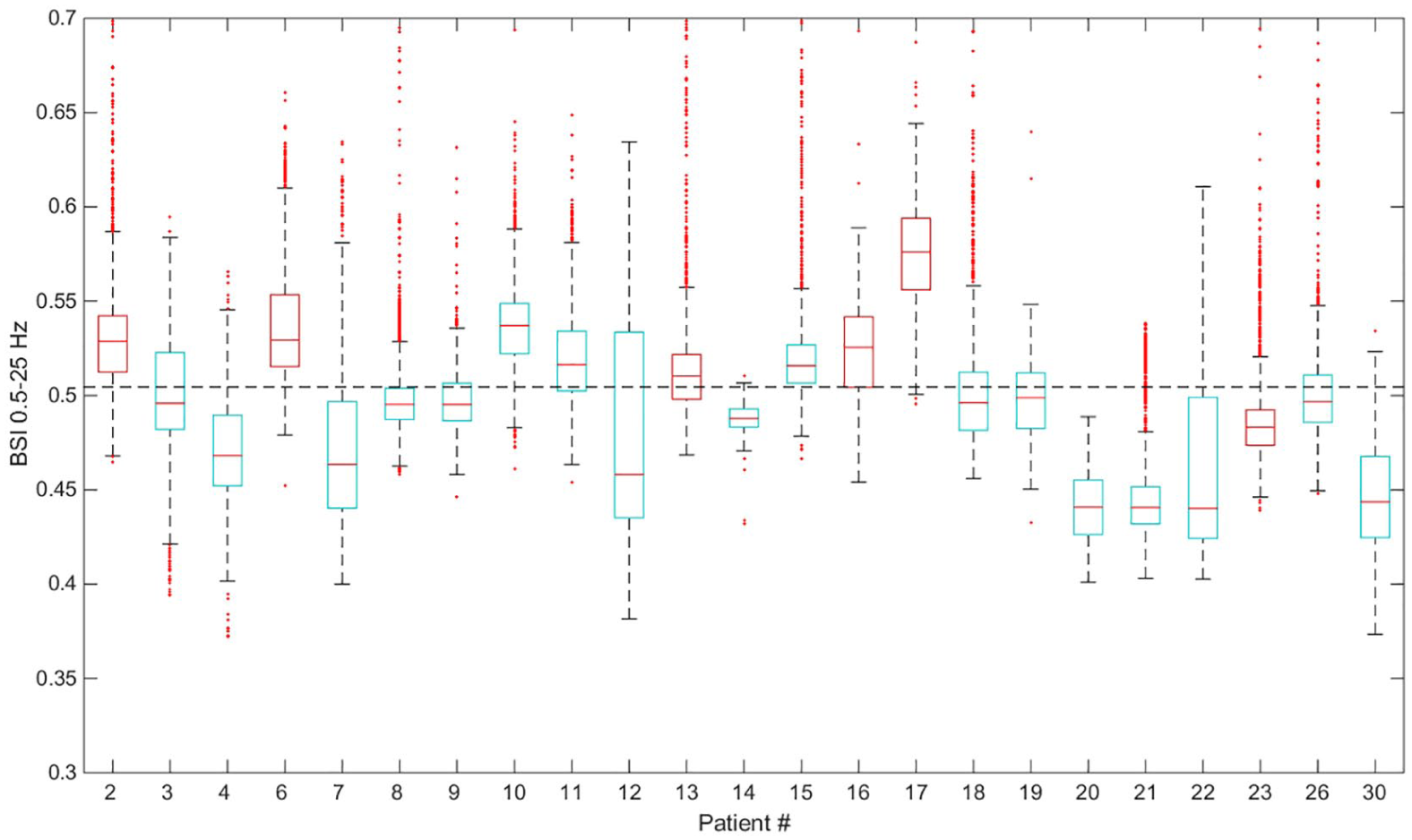
Distribution of the brain symmetry index (BSI) values after end of circulatory arrest. Outcomes are color-coded as blue (good) and red (poor). The box-and-whisker plots show median values as a line, box edges represent the 25%/75% quartiles, the whiskers represent non-outliers, and outliers are plotted individually. The optimum BSI threshold for outcome prediction is shown as a dotted line.
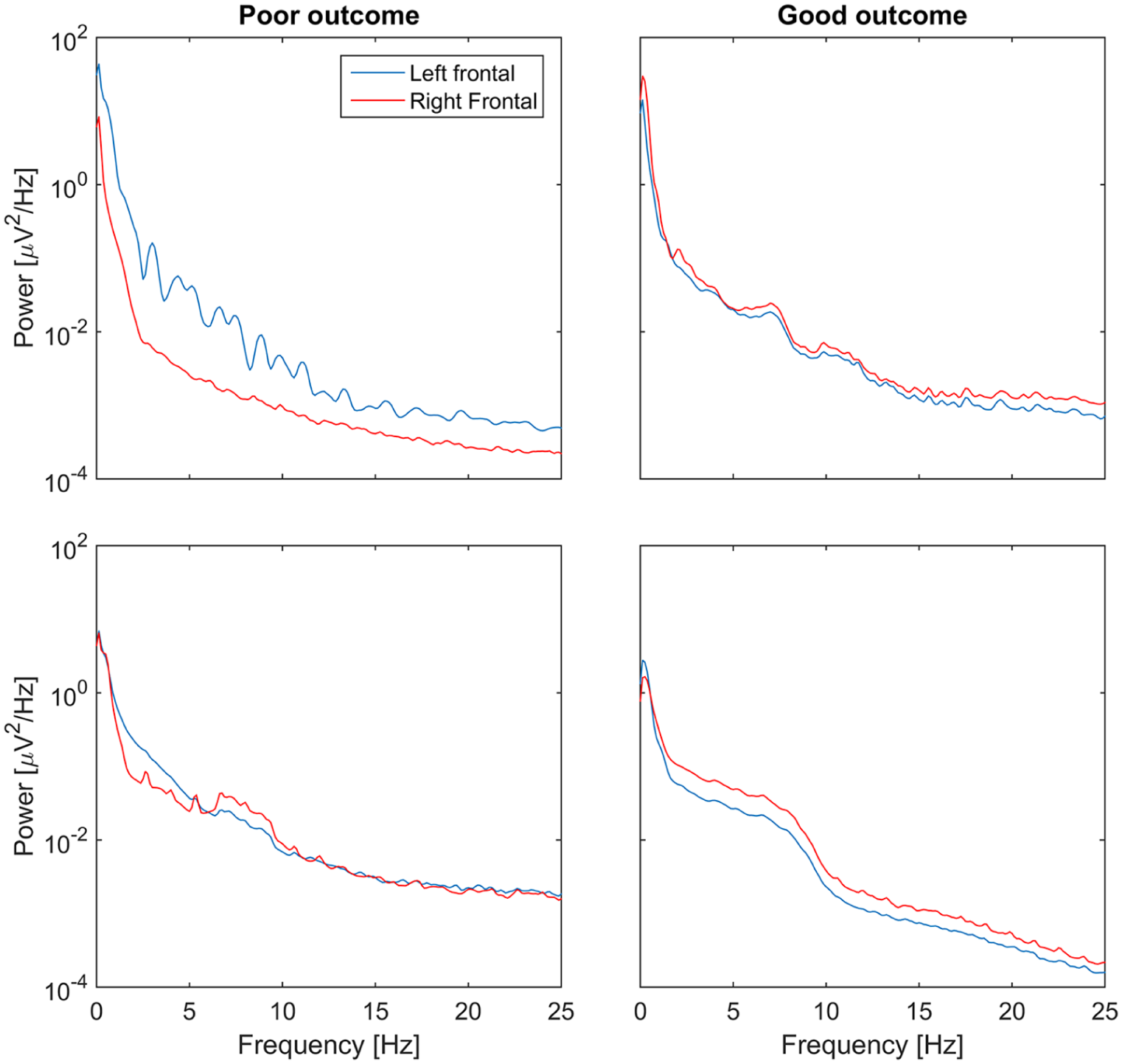
Illustrative examples of the electroencephalogram (EEG) mean spectra obtained from the left (blue) and right (red) frontal EEG derivations. On the left are examples with a poor primary outcome, showing notable hemispheric asymmetry, and on the right with a good primary outcome.
All other neuromonitoring data are presented in Table 3, with only S100β at the second POD having significantly higher values in the poor outcome group (p = 0.02).
Neuromonitoring data for at set time points.
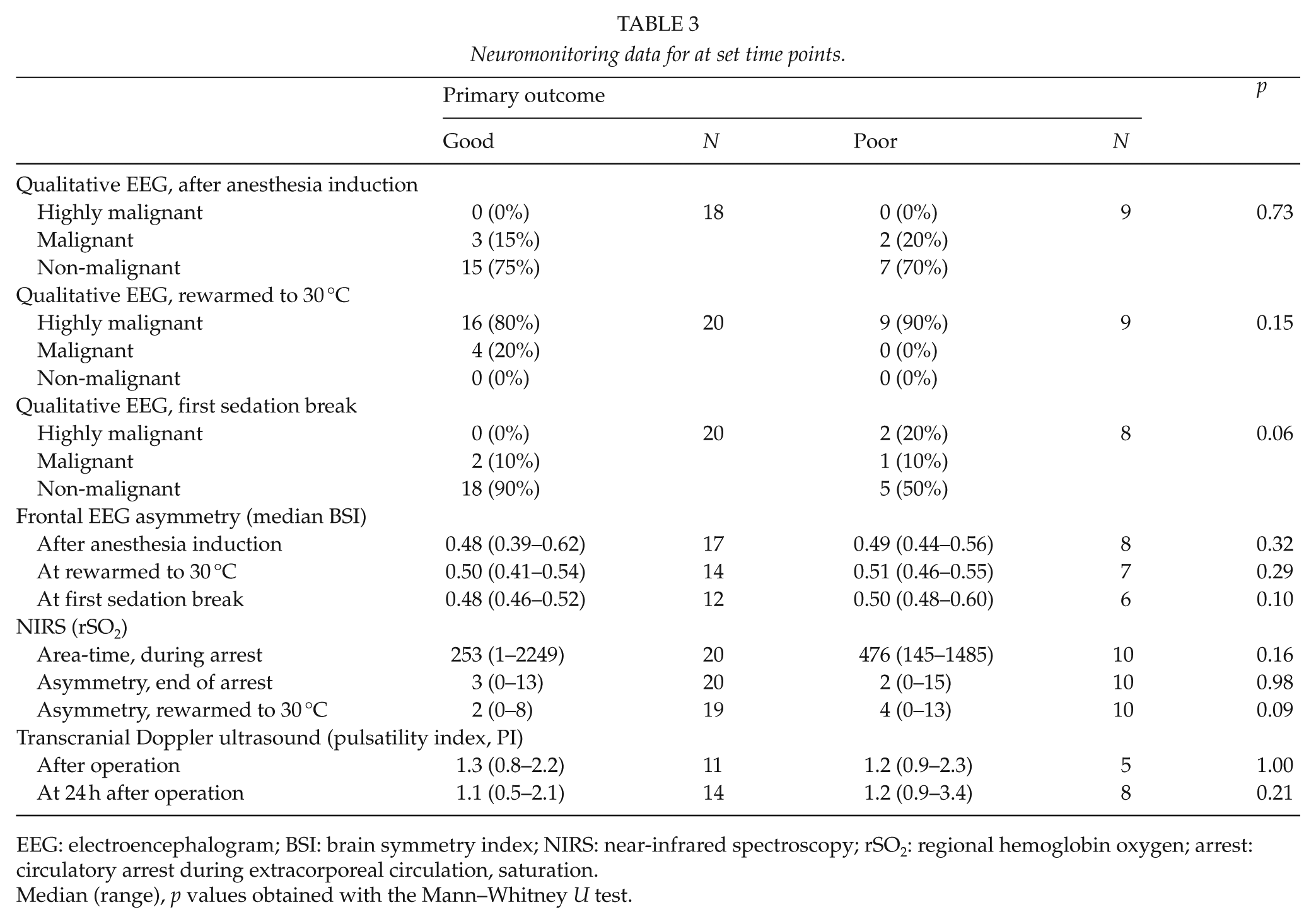
EEG: electroencephalogram; BSI: brain symmetry index; NIRS: near-infrared spectroscopy; rSO2: regional hemoglobin oxygen; arrest: circulatory arrest during extracorporeal circulation, saturation.
Median (range), p values obtained with the Mann–Whitney U test.
A neuropsychological evaluation was carried out for 21 (78%) of the 27 patients alive at the time of the interview, with a median (range) of 6 (3–14) months after surgery. Only three (14%) patients presented with major neuropsychological complications at evaluation (major challenges in memory functions and concentration). All these patients were from the poor outcome group, with one poor outcome patient presenting with only mild neuropsychological symptoms (p = 0.003).
Discussion
Hemispheric asymmetry of frontal EEG shows potential as a noninvasive neuromonitoring method during surgery and ICU stay, with frontal BSI predicting primary neurological outcome after hypothermic circulatory arrest for surgery of the thoracic aorta. In this study, we show that BSI predicts neurological outcome with a sensitivity of 79 (IQR; 62%–88%) and a specificity of 71 (IQR; 61%–84%), using a threshold value of 0.51 and during the first 6 h after end of arrest. This is a potentially important finding, as typically the confounding effects of hypothermia and deep anesthesia blunt EEG variables, and this is also the time when neurological complications typically develop. A brain CT was performed for six patients, of which 5 (83%) had a BSI score over the threshold value of 0.51. All these patients had acute lesions presenting more distinctly in one hemisphere, although the patient with a BSI below the set threshold value had almost symmetrical lesions in the cerebellum. Such deep lesions would probably have very little effect on fronto-temporal EEG.
Contrary to the frontal BSI, visual EEG classification by a clinical neurophysiologist (non-malignant, malignant, and highly malignant) was not predictive of outcome (Table 3). The classification system used was developed for cardiac arrest patients, and it lacks the assessment of hemispheric asymmetry (23). In comatose patients, certain EEG findings, such as isoelectric or low-voltage EEG or burst suppression at 24 h after cardiac arrest, predict unequivocally a poor outcome (23). In accordance, similar EEG patterns were seen at the first sedation break in two patients from the poor primary outcome group. Visual EEG analysis is best suited to detect rapid changes (seconds to minutes) and notable patterns, such as epileptiform discharges and periodic patterns (such as burst suppression) (9). However, visual analysis is not as sensitive in detecting gradual changes and changes in trends, nor in comparing such changes (9). The detection of gradual changes in hemispheric asymmetry is therefore more suited for computerized analysis (9).
Unlike NIRS, which measures the tissue and blood oxygenation of the frontal cortices, frontal EEG measures change in cortical neuronal activity. These changes are associated with neuron ischemia and damage during and after surgery and correlate with neurological outcome (11, 13, 15). Typical confounding factors, such as sedation and hypothermia, exert a generalized effect on EEG, which are not reflected in hemispheric asymmetry. On the other hand, tracking the evolution of hemispheric asymmetry is crucial, as even generalized changes typically present initially as asymmetric changes in the EEG power spectrum. The results of neuromonitoring with BSI are promising, especially as other noninvasive methods have shown contradictory results. Hemispheric EEG asymmetry could form the basis of a reliable, predictive, and easily applicable method of neuromonitoring, usable, and desperately needed in both the OR and ICU. The timely detection of perioperative neurological injury is important in guiding the use of neuroprotective methods, but also in future study. To test whether a neuroprotective intervention is useful, we must first be able to detect the neurological insult in real-time.
Typically, the inherent variance in EEG spectrum estimation is reduced by successive averaging of the spectra to form a final estimate. In this explorative study, the objective was to evaluate predictive variables which could be used in real-time EEG monitoring. Thus, the BSI values were derived from non-averaged estimates, resulting in higher BSI baseline levels than in previous studies (12–14). With averaged spectra, the BSI dynamic range was increased, but the predictive performance was not affected (data not shown). Contrary to earlier works, where one aggregate BSI value was derived over all derivations, we derived two separate BSI values, each between only two symmetric EEG derivations. The results from the temporal channels did not perform as well, probably due to anatomical and circulatory differences. The main challenge with EEG is the susceptibility to artifacts, which corrupted a lot of data in this study. Good electrode contact is crucial in eliminating artifacts; therefore, a simpler two-channel frontal montage would be easier to place and check for loss of contact.
The analysis of spatial NIRS values has been actively used in neuropsychological research of functional brain asymmetry (24), but only few studies have explored spatial NIRS in cardiac surgery (25–27). It is estimated that up to 85% of the changes of NIRS values during cardiopulmonary bypass are the result of notable changes in vascular tone, fraction of inspired oxygen, body temperature, and hematocrit (5, 28). To minimize the confounding effect of these variables, the beginning of circulatory arrest was chosen as a baseline for neurological outcome analyses. However, neither the magnitude of decrease of NIRS during circulatory arrest, nor the asymmetry between left and right NIRS channels during and after circulatory arrest, predicted neurological outcome. Biomarkers (except S100β on the second POD) and TCD measurements were not predictive. The methods and results are presented in the Supplemental Appendix, along with sedation data and statistical methods.
There are potential limitations to this study. Signal quality would be better with an automatic sensor impedance check function, and a baseline neurological evaluation was not available, as over half of the patients were emergency cases. For the purposes of this explorative study, EEG data were processed and analyzed post hoc, but the processes could be automated and used in real-time monitoring.
Supplemental Material
Total_arrest_Scan_J_Surg_Suppl – Supplemental material for Noninvasive Neuromonitoring of Hypothermic Circulatory Arrest in Aortic Surgery
Supplemental material, Total_arrest_Scan_J_Surg_Suppl for Noninvasive Neuromonitoring of Hypothermic Circulatory Arrest in Aortic Surgery by J. A. Stewart, M. O. K. Särkelä, T. Salmi, J. Wennervirta, A. P. Vakkuri, T. L. S. Vainikka, R. Suojaranta, K. Mäki, V. H. Ilkka, H. Viertiö-Oja and U.-S. Salminen in Scandinavian Journal of Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The main author was supported by the HUS Special Funds. M.O.K.S. and H.V.-O. are GE Healthcare employees.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.