
Abstract
Background and Aims:
Emergency Response Teams have been employed by hospitals to evaluate and manage patients whose condition is rapidly deteriorating. In this study, we aimed to assess the outcomes of triggering the Emergency Response Teams at a high-volume arthroplasty center, determine which factors trigger the Emergency Response Teams, and investigate the main reasons for an unplanned intensive care unit admission following Emergency Response Team intervention.
Material and Methods:
We gathered data by evaluating all Emergency Response Team forms filled out during a 4-year period (2014–2017), and by assessing the medical records. The collected data included age, gender, time of and reason for the Emergency Response Teams call, and interventions performed during the Emergency Response Teams intervention. The results are reported as percentages, mean ± standard deviation, or median (interquartile range), where appropriate. All patients were monitored for 30 days to identify possible intensive care unit admissions, surgeries, and death.
Results:
The mean patient age was 72 (46–92) years and 40 patients (62%) were female. The Emergency Response Teams was triggered a total of 65 times (61 patients). The most common Emergency Response Team call criteria were low oxygen saturation, loss or reduction of consciousness, and hypotension. Following the Emergency Response Team call, 36 patients (55%) could be treated in the ward, and 29 patients (45%) were transferred to the intensive care unit. The emergency that triggered the Emergency Response Teams was most commonly caused by drug-related side effects (12%), pneumonia (8%), pulmonary embolism (8%), and sepsis (6%). Seven patients (11%) died during the first 30 days after the Emergency Response Teams call.
Conclusion:
Although all 65 patients met the Emergency Response Teams call criteria, potentially having severe emergencies, half of the patients could be treated in the arthroplasty ward. Emergency Response Team intervention appears useful in addressing concerns that can potentially lead to unplanned intensive care unit admission, and the Emergency Response Teams trigger threshold seems appropriate as only 3% of the Emergency Response Teams calls required no intervention.
Keywords
Introduction
Although the outcomes of total joint arthroplasty (TJA) have improved substantially in recent decades, arthroplasty procedures entail inherent risks of severe complications. The reported incidence of major adverse events after arthroplasty is between 1.7% and 4.6%, and the rate of life-threatening complications is as high as 4.4% (1, 2). It has been estimated that up to 1 in 30 patients will require critical care services after arthroplasty (3). Most major complications after TJA occur during hospitalization, usually within the first four postoperative days (1). Common medical emergencies include pulmonary embolism, tachyarrhythmia, and acute myocardial infarction (1).
As hospitals face issues of cost containment, planned and unplanned intensive care unit (ICU) admissions add significant costs to inpatient care.
Emergency Response Teams (ERTs) have been employed by hospitals to evaluate and manage hospitalized patients whose condition is rapidly deteriorating, and have been shown to reduce postoperative morbidity and mortality, and prevent unplanned ICU admissions (4–6). An ERT usually consists of physicians with experience in critical care and anesthesiology, and nurses who have received special training.
Several different terms are commonly used for the same type of service, providing immediate intervention by experienced healthcare professionals for patients whose condition is rapidly deteriorating. The most common terms used in the literature are ERT, rapid response team (RRT), and medical emergency team (MET). In our study, we chose to use the ERT term, which to our knowledge is synonymous with the other terms.
ERT studies have mostly been performed in whole-hospital settings with highly mixed patient populations (4–7), and the use of ERTs in specialized arthroplasty units has not been thoroughly described. Early ERT intervention might provide benefits regarding both patient safety and financial aspects by identifying and treating deteriorating ward patients early enough to prevent postoperative complications and unplanned ICU admissions. Evaluating ERT interventions may shed light on serious postoperative complications or close-call situations that might be preventable.
The aim of this study was to determine which factors trigger the ERT at a high-volume tertiary arthroplasty center, and subsequently to assess the outcomes of ERT intervention. We also aimed to assess the most common ERT interventions, and the main reasons for ICU admission following ERT intervention.
Materials and Methods
We retrospectively reviewed all prospectively collected ERT forms that were filled out between 2014 and 2017 at a single high-volume academic arthroplasty center. The ERT form is a standardized paper form that is filled out by the nurse who makes the ERT call (8). The ICU at our institution is level II according to the American College of Critical Care Medicine guidelines (9). It provides invasive monitoring, invasive mechanical ventilation, but not dialysis.
Fast-Track Protocol and Pain Management
A fast-track protocol for joint replacements (10, 11) has been in use at our institution since 2009, and the hospital length of stay (LOS) after elective primary TJA is usually 2 or 3 days. The average yearly number of TJAs during the study period was 1053 total knee arthroplasties (TKA), 144 revision TKA, 897 total hip arthroplasties (THA), and 222 revision THA. In total, 9265 TJAs were performed during the study period. Prior to surgery, patients receive both spoken and written information about rehabilitation. Patients are typically mobilized on the day of surgery, and receive physiotherapy daily until the mobilization-related discharge criteria are met. The discharge criteria are strictly functional; in other words, the patient is discharged when able to walk a short distance, dress and visit the bathroom independently, the pain is under control without strong opioids, and the wound is dry.
The standard postoperative pain medication consists of 600 mg ibuprofen three times daily and 1000 mg acetaminophen three times daily. Strong opioids (e.g. oxycodone) are usually given only on the first postoperative day, and weaker opioids (e.g. codeine or tramadol) are given starting on the second day postoperatively, if required. Patients are not discharged with strong opioids.
ERT Service
The ERT service was started in our arthroplasty unit in 2013. The ERT team consists of one anesthesiologist and one nurse from the ICU. The ERT call is answered by the anesthesiologist, but differs from a normal anesthesiologist consultation in several ways. The ERT service includes training for both the ERT and the nurses on the ward. The nurses on the ward receive training in what the ERT call criteria entail, which vital parameters to monitor, and how and when to make an ERT call. When an ERT call is made, the ERT nurse brings emergency equipment that is not always available on the ward—namely drugs commonly needed in acute situations and equipment for advanced airway control.
The ICU is located in the same building as the arthroplasty unit and has six beds. The number of beds and nurses is constant regardless of the number of patients. The ICU is staffed by nurses working in 3 shifts 7 days a week, and an anesthesiologist is on duty 24/7.
ERT Call Criteria
At our institution, basic details about every ERT call are collected on a standardized paper ERT form that is similar to recommendations in the literature (8). The form includes data on the time and date of the call, the specific ERT criteria that triggered the activation, the main interventions performed, and preliminary plans for further care. The criteria for an ERT call at our institution are presented in Table 1. All criteria were collected as filled out on the original ERT form, except for the subjective criterion “worried,” which was omitted if it was used together with any objective criterion. The “worried” criterion is intended to be used if the caregiver is concerned about the patient, but none of the objective criteria are met. Therefore, it does not provide any further benefit if used together with another criterion. Regarding all objective criteria, several could be met at the same time.
ERT call criteria leading to ERT call, all patients.
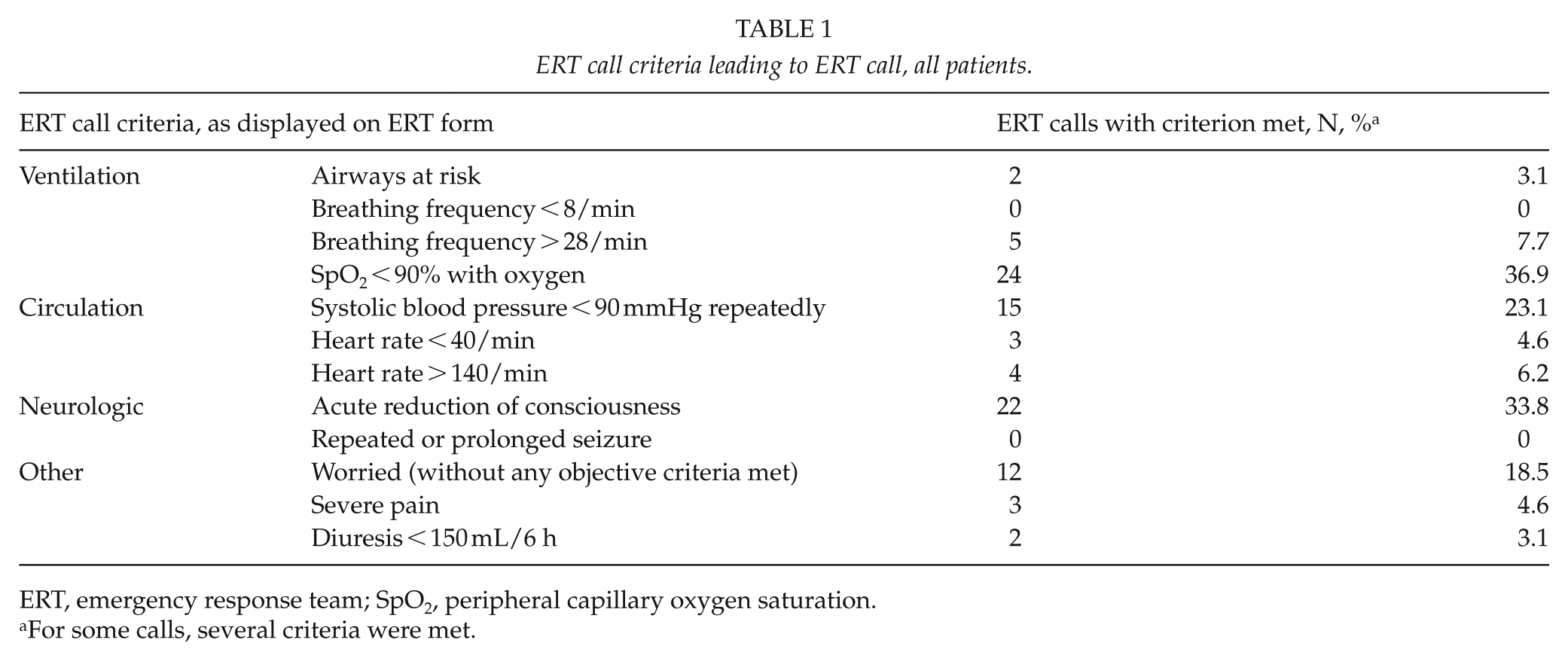
ERT, emergency response team; SpO2, peripheral capillary oxygen saturation.
For some calls, several criteria were met.
Data Collection
The ERT forms were reviewed and cross-checked with the electronic medical records. Further information on ERT interventions was obtained by thoroughly reviewing the medical records, and each patient was monitored for 30 days after the ERT call to track the clinical outcomes following the ERT intervention, recording possible ICU admissions, surgeries, and death. The 30 day survival was cross-checked with the national population register when the medical records failed to provide sufficient data to determine whether or not the patient was alive at 30 days. Patients that had several ERT calls at different time points were regarded as separate patients in all analyses, except for the 30 day survival count.
We reviewed the electronic medical records to collect data on age, sex, reason for hospitalization, American Society of Anesthesiologists (ASA) score, interventions during the ERT visit, discharge destination, and details of possible surgery preceding the ERT call. Furthermore, we reviewed all available data to find an explanation for what caused the patient’s emergency. The results are presented as number (percentage), mean (range), or median (interquartile range), where appropriate.
Results
The ERT was triggered a total of 65 times (61 patients) during the study period. The incidence of ERT calls was approximately 7 of 1000 patients. The mean patient age was 72 (range = 46–92) years and 40 patients (62%) were female. The median ASA score was 3 (range = 1–4). The mean LOS was 7.3 days (range = 1–50) and the median LOS was 4 days (interquartile range = 5). In total, 33 (54%) of the study patients were discharged home, 23 (38%) were discharged to further care, and 5 patients (8%) died before being discharged.
Most ERT calls occurred during the daytime and only 13 (20%) occurred between 11:00 p.m. and 8:00 a.m. In total, 58 patients (89%) had arthroplasty surgery performed during the same hospitalization prior to the ERT call (19 primary THA, 12 revision THA, 17 primary TKA, 8 revision TKA, and 2 femoral amputations due to prior failed treatment of a periprosthetic infection). The ERT call occurred on average 2.3 days after surgery and one-third of the calls occurred during the first postoperative day. Thirty days after the ERT call, 54 of the 61 patients (89%) were alive. Descriptive statistics for the different subgroups is presented in Table 2.
Descriptive statistics.
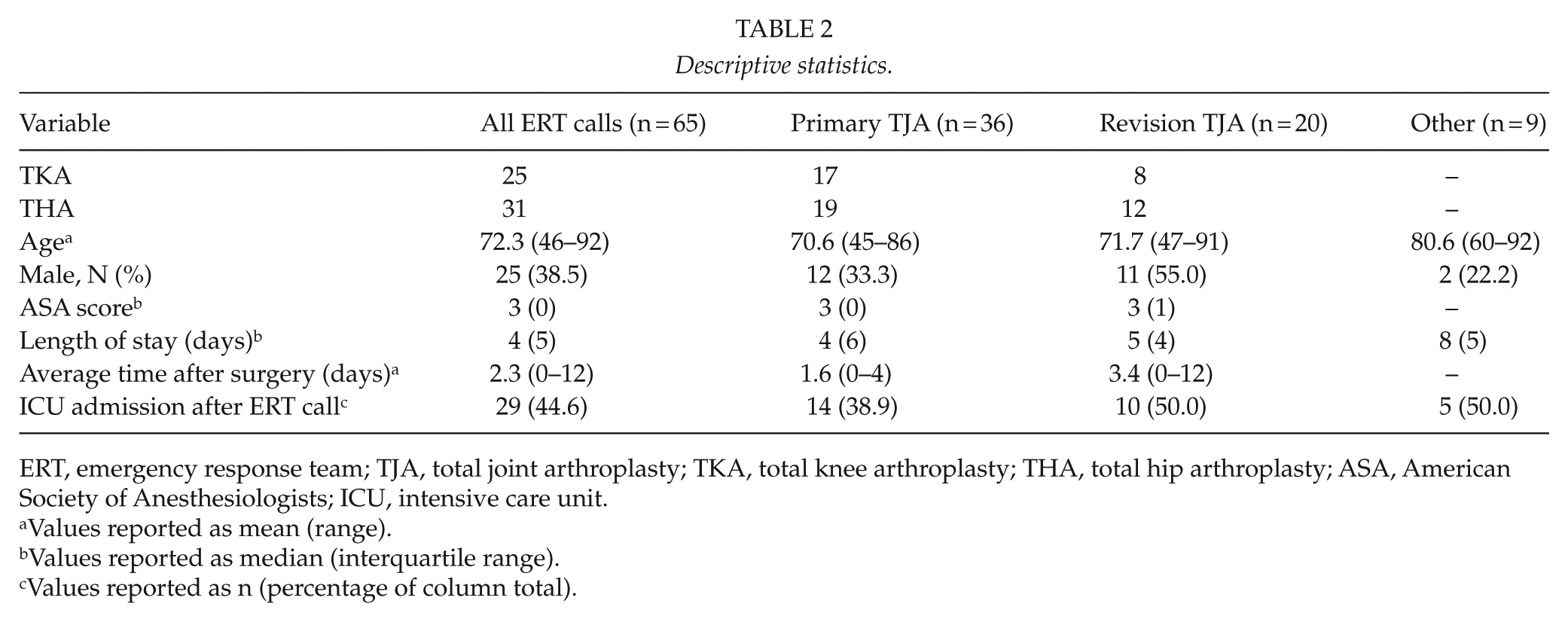
ERT, emergency response team; TJA, total joint arthroplasty; TKA, total knee arthroplasty; THA, total hip arthroplasty; ASA, American Society of Anesthesiologists; ICU, intensive care unit.
Values reported as mean (range).
Values reported as median (interquartile range).
Values reported as n (percentage of column total).
ERT Call Criteria and Initial Assessment
The most common criteria that triggered the ERT call were low oxygen saturation, loss or reduction of consciousness, hypotension, and worry about the patient (Table 1). Two or more criteria were met in 24 cases (36.9%). The ERT call criteria for the different subgroups are presented in Table 3. Immediately following the ERT visit, 29 patients (45%) were transferred to the ICU, and one patient died. The remaining 35 patients (54%) were initially treated in the arthroplasty ward. Three out of all patients (4.9%) required further surgery during the same hospitalization (two irrigation and debridement and one removal of implant, all three due to infection). For a flowchart of the ERT call outcomes, see Fig. 1.
ERT call criteria leading to ERT call, by patient subgroups.
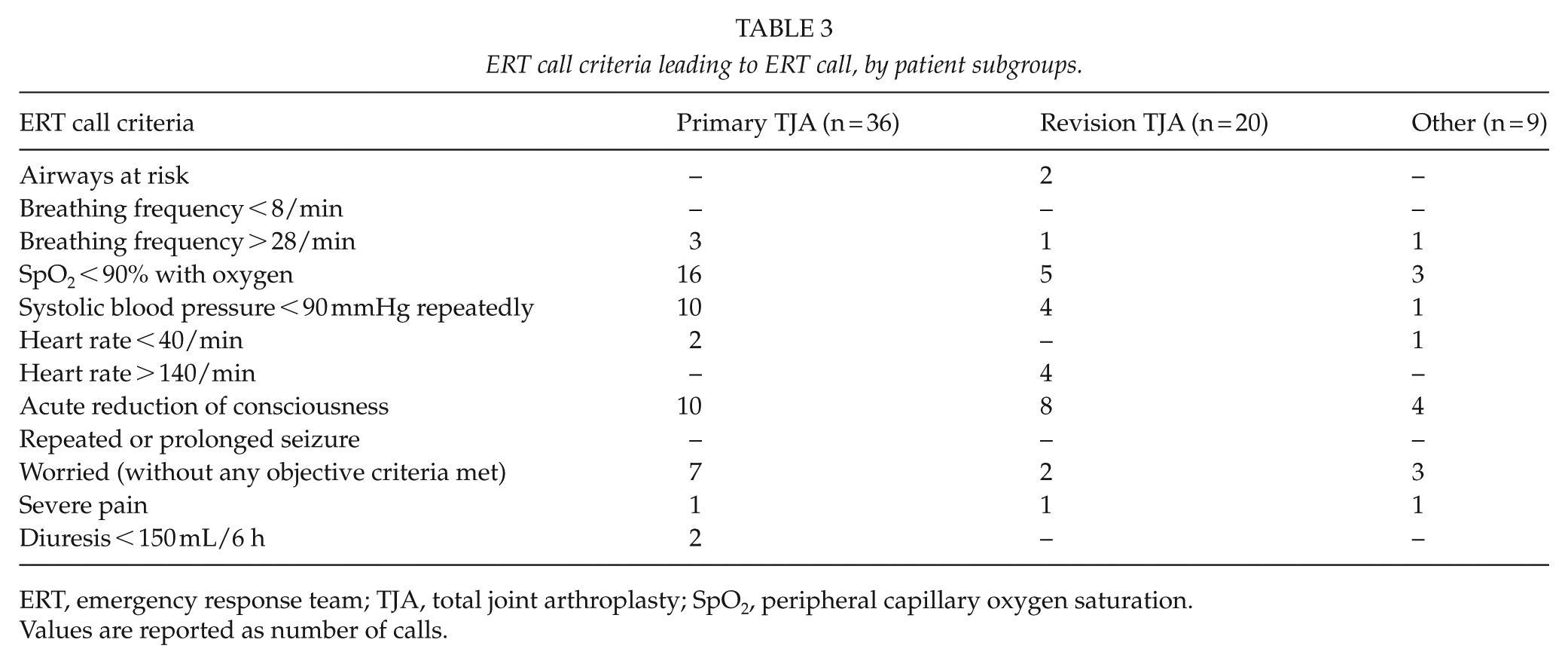
ERT, emergency response team; TJA, total joint arthroplasty; SpO2, peripheral capillary oxygen saturation.
Values are reported as number of calls.
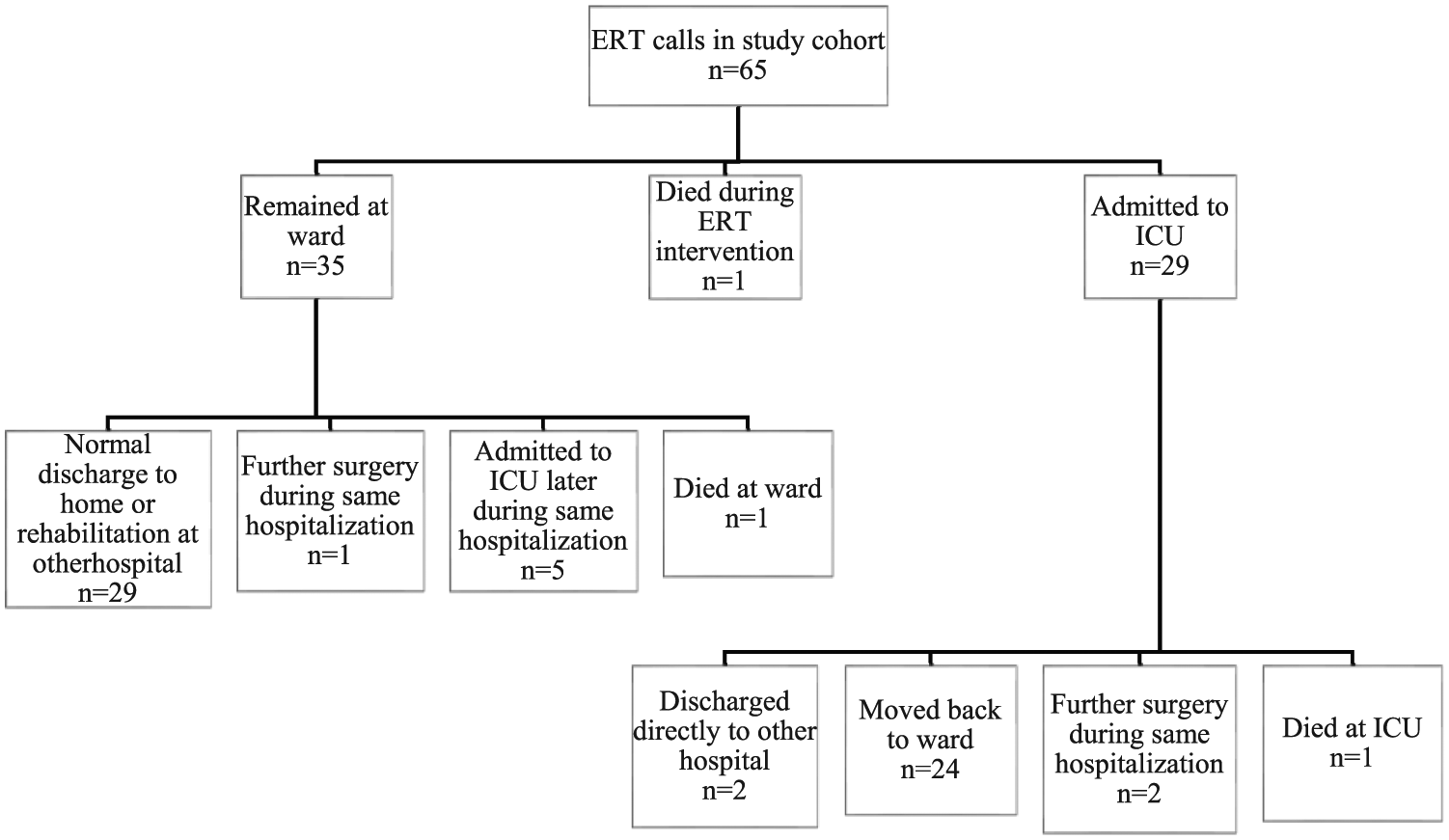
Flow chart of ERT call outcomes.
ERT Interventions in the Ward
For the patients that remained in the arthroplasty ward, the most common ERT interventions were further diagnostics by ordering laboratory tests (25, 71%), changes to medication (19, 54%), fluid resuscitation (19, 54%), and oxygen therapy (8, 23%). The most common drugs administered were naloxone, furosemide, and oxycodone. In two cases (3% of study patients), no interventions were needed at all because the emergency had already been resolved (one patient choked on a piece of bread and one patient had benign fainting). Five patients (14%) initially treated in the ward were admitted to the ICU later during the same hospitalization.
Patients Admitted to ICU
The most common reasons for ICU admission following an ERT call were respiratory related (18 patients, 62%), decreased level of consciousness (11 patients, 38%), and hemodynamic instability (10 patients, 34%). Seventeen patients had more than one reason for being admitted to the ICU. The most common interventions in the ICU were norepinephrine infusion (10 patients, 34%), ventilatory support (6 patients, 21%), and invasive arterial pressure monitoring (11 patients, 38%). The median ICU stay before being moved back to the arthroplasty ward or to another hospital was 2 days. No patients required transfer to a level I ICU.
Reasons for the Emergency
When evaluating retrospectively, a medical cause explaining the rapid deterioration in the patient’s condition was established in 54% of the cases. The most common causes were drug-related side effects (12%), pneumonia (8%), pulmonary embolism (8%), and sepsis (6%). The drug-related side effects were mostly hypotension (side effects of spinal infusion, antihypertensive medication, and nitroglycerin) and decreased level of consciousness due to psychiatric or pain medication.
Discussion
In this study, we determined what triggers the ERT at a high-volume arthroplasty center, why patients are admitted to ICU following the ERT call, and what interventions are most commonly carried out by the ERT and in the ICU. To our knowledge, this is the first study describing the outcomes of triggering the ERT in an arthroplasty unit. While previous studies have mostly looked at risk factors for adverse events and/or ICU admission after arthroplasty surgery, we were able to provide firsthand data on both reasons and interventions, for both ERT visits and subsequent ICU admissions.
ERT Call Criteria and Initial Assessment
There were approximately seven ERT calls per 1000 patients, which is somewhat higher than previously reported for surgical patients (7). The most common criteria triggering the ERT call in the arthroplasty ward are mostly in line with previous reports of ERTs in whole-hospital settings. One study reported “airway threatened” as the most common criterion, followed by “staff worried,” “decrease in Glasgow Coma Scale (GCS) score > 2,” and “systolic blood pressure below 90 or over 200” (12). In another study (13), also performed in a whole-hospital setting, the most common ERT criteria were “systolic blood pressure < 90,” “worried,” and “decrease in GCS score > 2.”
The fourth most common ERT call criterion in our study was “worried.” As ERT calls are mostly made by nurses, objective changes in vital signs are used as ERT call criteria, as such changes may reflect an underlying medical emergency. Although most criteria are objective, a nurse can still make an ERT call due to any kind of concern about the patient’s condition using the “worried” criterion. This ensures that any kind of subjective concern, possibly giving clues about an ensuing medical emergency, will be addressed correctly and not overlooked. However, this could theoretically lead to a large number of false alarms, especially if the nurse is inexperienced. In this study, however, this did not seem to be a concern. Every fifth call was triggered by the “worried” criterion, and only 3% of all ERT calls required no intervention.
ERT Interventions in the Ward
About half of the patients (45%) with a medical emergency could be treated in the ward. It is likely that without the ERT service, many of these patients would have been admitted to the ICU.
As the most common interventions for the patients treated in the ward were further diagnostics byordering laboratory tests, changing medication and administering intravenous fluid, some of the interventions might have been performed by an attending physician alone, without making an ERT call. However, the ERT call threshold should be low enough to allow for some “easy calls,” since the consequences of not noticing a real emergency in time may be catastrophic.
Patients Admitted to ICU
Memtsoudis et al. (3) found that cardiac and pulmonary complications were the most common reasons for patients to require critical care services after TJA. Another recent study (14) reported that oxygen requirement >6 liters, or positive pressure ventilation, and hypotension requiring vasopressors were the most common ICU interventions after TJA. Our results are consistent with these previous results, as respiratory insufficiency and hemodynamic instability were among the most common reasons for ICU admission in our study.
Reasons for the Emergency
The retrospectively determined medical reasons for the emergency leading to ERT activation are partially in line with previous knowledge about common medical emergencies after arthroplasty surgery. One study reported pulmonary embolism, tachyarrhythmia, and acute myocardial infarction as the most common major systemic complications after TJA (1). In the latter study, as opposed to ours, pneumonia and sepsis were rarer complications.
In our study, every 10th medical emergency was caused by a drug-related side effect. Patients undergoing TJA require strong pain medication during the first few days after surgery, and the surgery may affect the physiology enough to interfere with the patient’s regular medication. About half of the drug-related side effects were excessive sedation due to opioids or psychiatric drugs, or due to other drugs interacting with the pain medication. Although these patients comprise a small fraction of all patients treated during the study period, drug interactions might still be more easily preventable than pneumonia and sepsis, for example, and this issue should therefore be highlighted.
Limitations
Our study has its limitations. First, there were sometimes several criteria triggering the ERT call, and occasionally several reasons for being admitted to the ICU. These results might therefore be difficult to interpret when the single most important reason is not evident. Also, upon retrospective review, it was sometimes difficult to conclusively identify a medical reason for the emergency leading to the ERT call, and only clear cases were therefore taken into account. However, due to the retrospective assessment, the causes should be interpreted with caution. Finally, it is difficult to establish whether the utilization of an ERT service lowers the rate of unplanned ICU admissions, since undertaking a controlled study would not be feasible. It seems plausible, however, that the implementation of an ERT service has some effect on lowering the number of unplanned ICU admissions, as supported by previous studies (4, 6).
Conclusion
The most common triggers for ERT activation were low oxygen saturation, loss or reduction of consciousness, and hypotension. Although all of the study patients met the ERT call criteria, potentially having severe emergencies, half of the emergencies could be resolved in the arthroplasty ward, with only five patients subsequently being moved to the ICU. The ERT trigger threshold seems appropriate, as only 3% of the ERT calls required no intervention. ERT intervention duly appears useful in addressing concerns that can potentially lead to unplanned ICU admission.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by grants from Finska Läkaresällskapet, Ålands Kulturstiftelse, Ålands Landskapsregering, Vappu Uuspään Säätiö, Medicinska understödsföreningen liv och hälsa, Svenska Kulturfonden, Suomen Artroplastiayhdistys, and Suomen Lääketieteen Säätiö.