
Abstract
Background and Aims:
The purpose of this study was to describe the frequency and types of complications after tube thoracostomy among all patients treated with tube thoracostomy for both traumatic and non-traumatic indications.
Material and Methods:
Retrospective register-based study of patients treated with tube thoracostomy between the years 2004 and 2014 in a university hospital.
Results:
In total, 1808 patients who had undergone tube thoracostomy were identified, complete data on tube thoracostomy treatment was available for 1169 patients. A total of 233 (19.9%) patients had 289 complications, 284 (98.3%) were positional resulting in tube malfunction. In 84 (7.2%) patients, malposition of the tube resulted in need for non-urgent operative treatment. There were 103 in-hospital deaths, but none due to tube thoracostomy complications. Empyema as a treatment indication was more frequent in patients with complications (15.9% vs 6.8%, p < 0.001) as was diabetes (21.9% vs 13.2%, p = 0.001). The likelihood of complications was lower with CH16 tubes (odds ratio 0.22, p < 0.001) and higher in diabetics (odds ratio 1.86, p = 0.001).
Conclusion:
Tube thoracostomy is a common procedure and complications occur in 19.9% of patients. Serious complications caused by the chest tube placement, however, are extremely rare. Complications were most common in patients treated for empyema and diabetics. Small CH16 tubes were associated with a lower incidence of complications.
Introduction
Tube thoracostomy (TT) as a treatment to remove excessive material from the pleural cavity has been known already for thousands of years. The oldest known documents of TT are from the 5th century before common era (BCE). Hippocrates is attributed as the first person to treat a patient with TT and successfully managed to treat inflammation with this procedure (1). TT is at present a ubiquitous treatment, for example, for pneumothorax, hemothorax, hemopneumothorax, pleural empyema, and pleural effusions. Although thoracostomy has been known for a long time, it was generally accepted as a treatment for the above-mentioned conditions as late as in the late 1950s (1). Currently, TT is one of the most commonly performed invasive therapeutic procedures (2).
Despite its relative safety and ease as a procedure, it can lead to potentially severe complications. In previous studies, the complication rates have been reported as high as 40%, ranging from 1% to 40% (3–6). Most of the existing literature focuses on outcomes in trauma patients (4, 6). The purpose of this study was to describe the frequency and types of complications of TT among all patients treated with TT for both traumatic and non-traumatic indications.
Material and Methods
The study was a retrospective register-based study. Consecutive patients treated with TT between the years 2004 and 2014 in a hospital Southwestern Finland Hospital District were identified from patient records and operative logs. Patients receiving TT were identified by the procedural codes (NOMESCO code GAA10). Patients receiving a postoperative chest tube after a thoracic or cardiac operation were excluded and data on thoracostomy patients dying outside the hospital (e.g. emergency treatment in the field or patients treated at primary health care facilities) could not be retrieved for this study. Also excluded were bedside TTs in the ICU and other intensive care units which are not necessarily assigned procedure codes in the patient records and could thus not be identified. Based on the criteria, 1808 patients were identified. The study flow chart is presented in Fig. 1. Of the 1808 patients, 497 were excluded due to incomplete or unclear patient records or incorrect coding of the procedure or diagnosis. A total of 230 of these 497 patients had received a tube and the total number of 1419 tubes was used to estimate the yearly incidence of TTs; 142 of the selected subjects had a postoperative tube after a thoracic or cardiac operation due to inaccurate coding. The final patient population used for outcome analyses was 1169 patients.
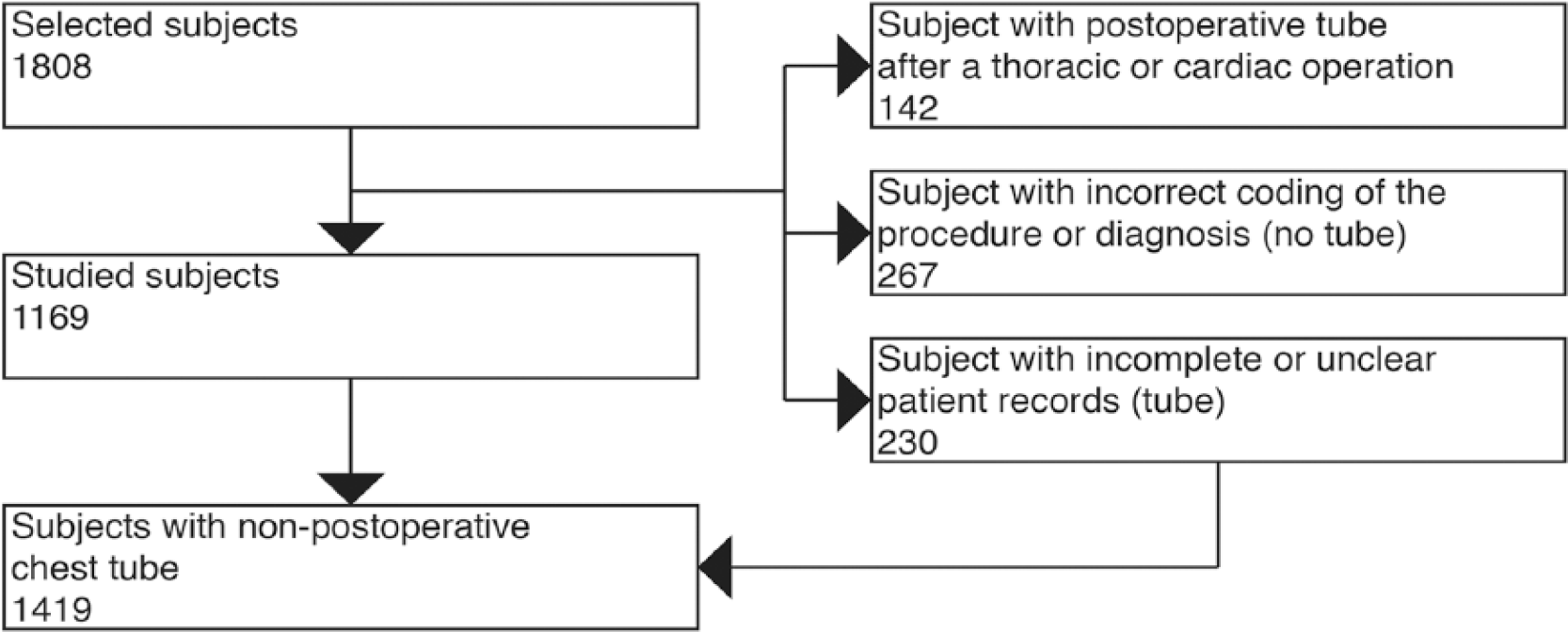
The study flow chart.
Patient records were reviewed for baseline characteristics and perioperative data (Tables 1 and 2).
Baseline characteristics.
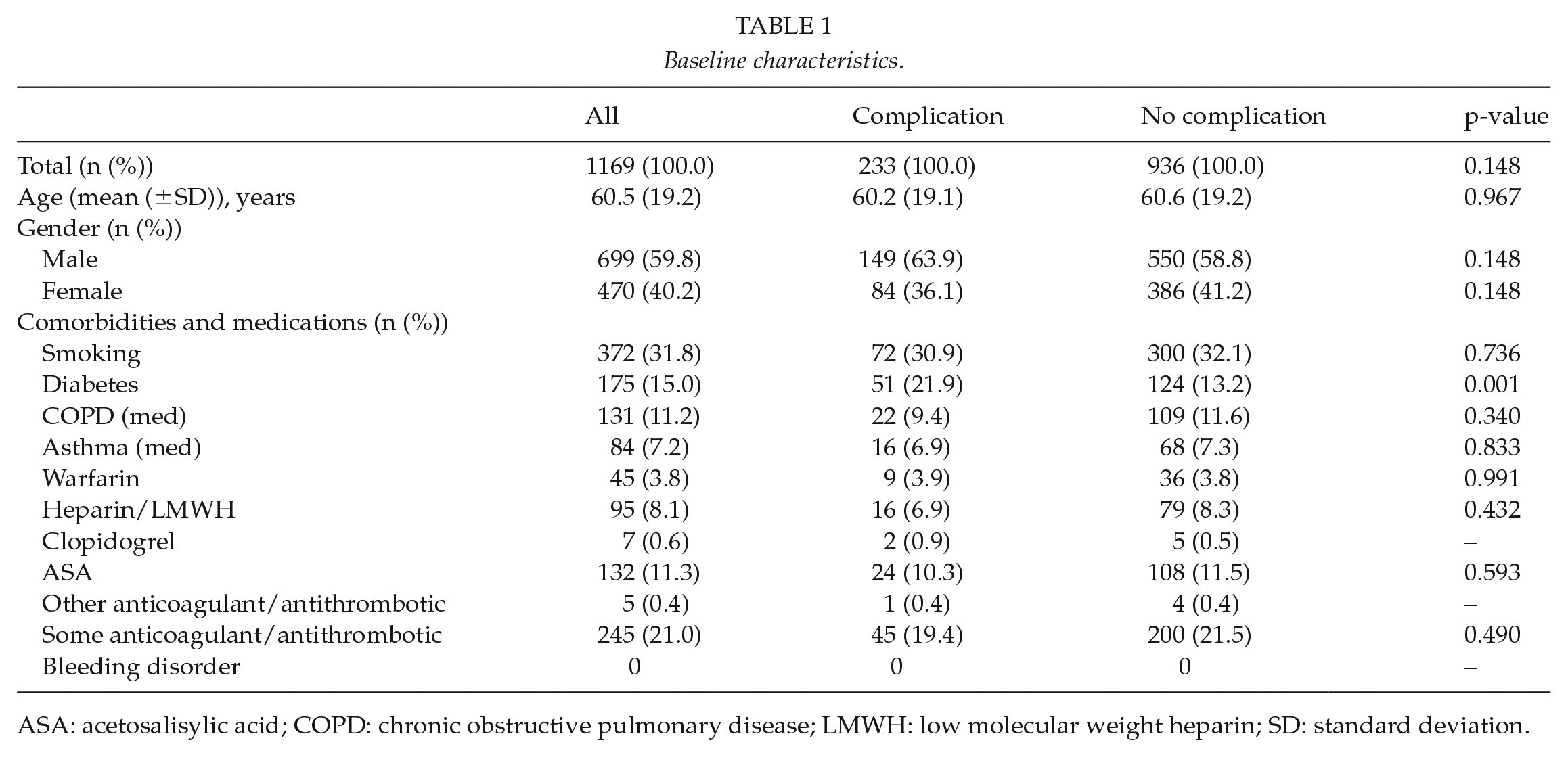
ASA: acetosalisylic acid; COPD: chronic obstructive pulmonary disease; LMWH: low molecular weight heparin; SD: standard deviation.
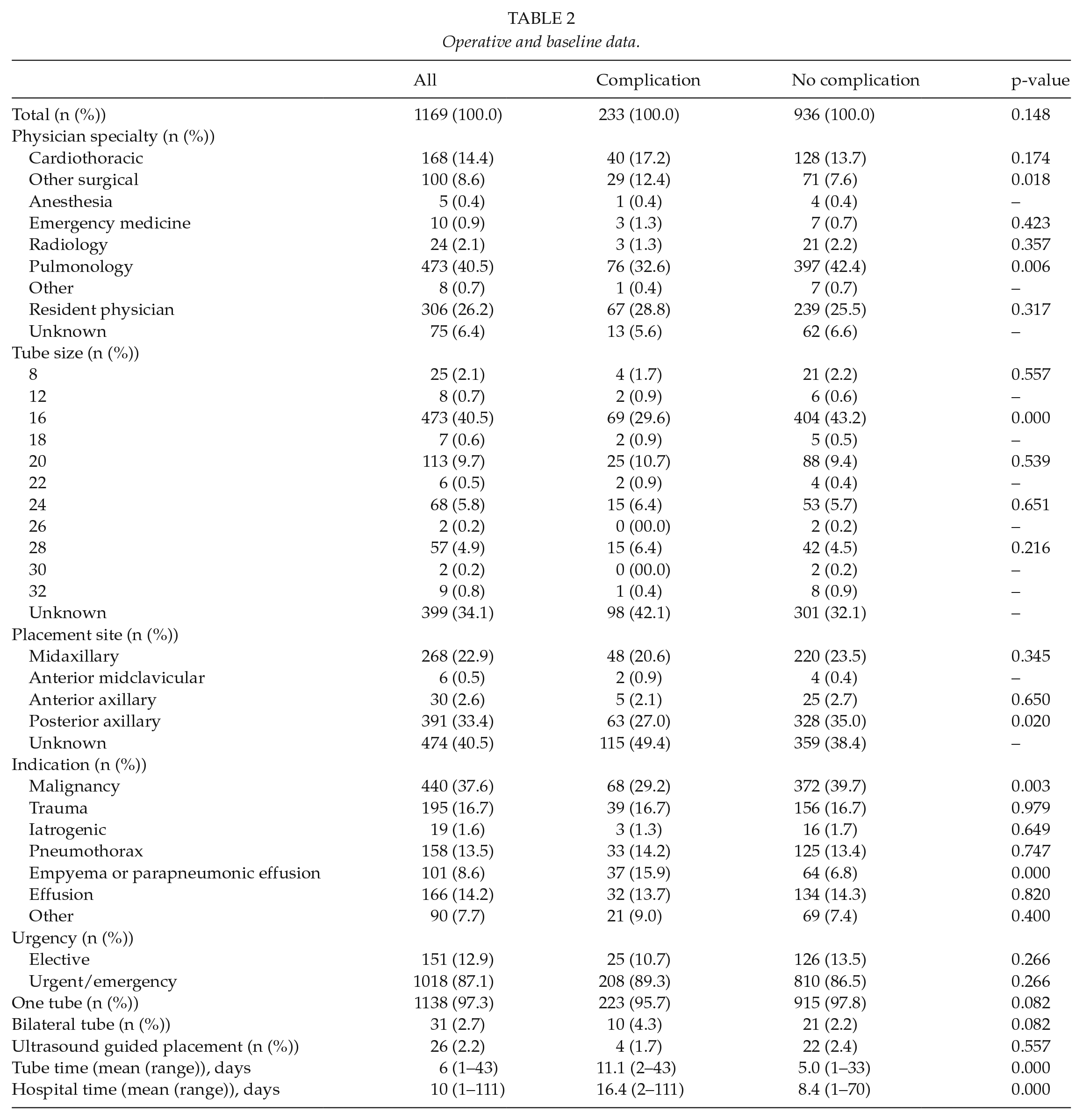
Operative and baseline data.
Indications for placement were grouped into malignancies, traumas, iatrogenic complications (e.g. central venous line placement complication), spontaneous pneumothoraxes, empyema or parapneumonic effusions, pleural effusions, and other. Urgency was classified as elective or urgent. Cases where the procedure was planned and postponed for the following or any later date were classified as elective and all other cases as urgent. Physician specialties were cardiothoracic, other surgical, anesthesia, emergency medicine, radiology, pulmonology, other, resident physician, and unknown. The category “other” included other specialties, physicians with no specialty, and medical students. Chest tube size was registered as French (Fr). Placement site was classified as anterior axillary, midaxillary, posterior axillary, anterior midclavicular, and unknown.
Bleeding disorder, smoking, diabetes, COPD, asthma, and antithrombotic medication were registered as pertinent history relating to TT complications. Recorded antithrombotic/anticoagulant drugs were warfarin, heparin or low molecular weight heparin (LMWH), clopidogrel, acetosalisylic acid (ASA), and other antithrombotics. If there was no clear mention of smoking cessation, the patient was defined as a smoker. Chronic obstructive pulmonary disease (COPD) was defined as a diagnosis of chronic lung disease in the patient records. Diabetes (type 1 and type 2) were based on a diagnosis in patient records.
Aho et al. generated a standardized format for reporting TT complications. They grouped complications into five clearly defined categories: insertional, positional, infective/immunologic, removal, and instructional/educational/equipment related (7). The same grouping was used in this study. Insertional complications were complications occurring within 24 h and were further divided into malposition, perforation of organ, bleeding requiring transfusion, intractable pain, and need for operative intervention. Positional complications were complications occurring after 24 h and were classified as need for operative intervention, need for new tube (obstruction, inadequate drainage of liquid or blood), and prolonged air leak. Prolonged air leak was defined as air leak >7 days post-insertion. Operative intervention included any procedure performed under general anesthesia.
Categorical variables were presented as numbers and proportions and continuous variables as mean and standard deviation. Between-group differences were evaluated with Chi-square-test for categorical variables and independent samples T-test for continuous variables. Independent predictors of complications were evaluated with binary multivariable logistic regression analysis. Variables with a p-value <0.10 on univariable analysis were entered in the multivariable model. P-values under 0.05 were considered statistically significant. SPSS for Mac version 24 (IBM, Armonk, NY, USA) was used for analyses.
Results
Baseline Characteristics
Baseline characteristics are shown in Table 1. The patient population used for analyses was 1169. Mean age of the population was 60.5 years and the age distribution was 1–98 years; 31.8% of the subjects were smokers. Diabetes was present in 15.0%, COPD 11.2%, and asthma in 7.2%. There were no patients with known bleeding disorders; 21.0% patients had one or more ongoing anticoagulant or antithrombotic medication. Diabetes was more prevalent in patients with complications compared to patients without complications (21.9% vs 13.2%, p < 0.001).
Operative and Baseline Data
Operative and baseline data are shown in Table 2. Most of the TT were performed by pulmonologists in 40.5% of subjects. Resident physicians performed 26.2% and cardiothoracic surgeons 14.4% of procedures. Anesthesiologists, emergency physicians, radiologists, and other physicians were a minority of performing physicians. Specialty of the treating physician was unknown in 6.4% of patients.
Tube size varied between 8 and 32 Fr. 16 Fr tubes were the most common size (40.5% of subjects). In 34.1% of the cases, tube size was not recorded.
33.4% of the tubes were placed in the posterior axillary and 22.9% in the midaxillary position. Anterior axillary placements were done in 2.6% cases and anterior midclavicular only in 0.5% patients; 40.5% of the placements were not clearly specified in the records.
Malignant effusions were the most common indication for TT with 37.6% subjects. Other indications in descending order of frequency were trauma, benign effusion, pneumothorax, empyema, pneumonia, iatrogenic, and infection. There was a statistically significant difference in indications for tube placement between groups. Patients who experienced a complications were more likely to have empyema or parapneumonic effusion as an indication for the procedure (p = 0). Most of the TT placements (87.1%) were urgent. 2.7% subjects received bilateral tubes and 2.2% of the tubes were inserted under ultrasound guidance.
Data on treatment duration were retrieved for 67.3% and data on length of stay for 89.6% patients. The mean tube treatment duration was 6 days and hospital stay was 10 days. The longest treatment duration was 43 days.
Complications
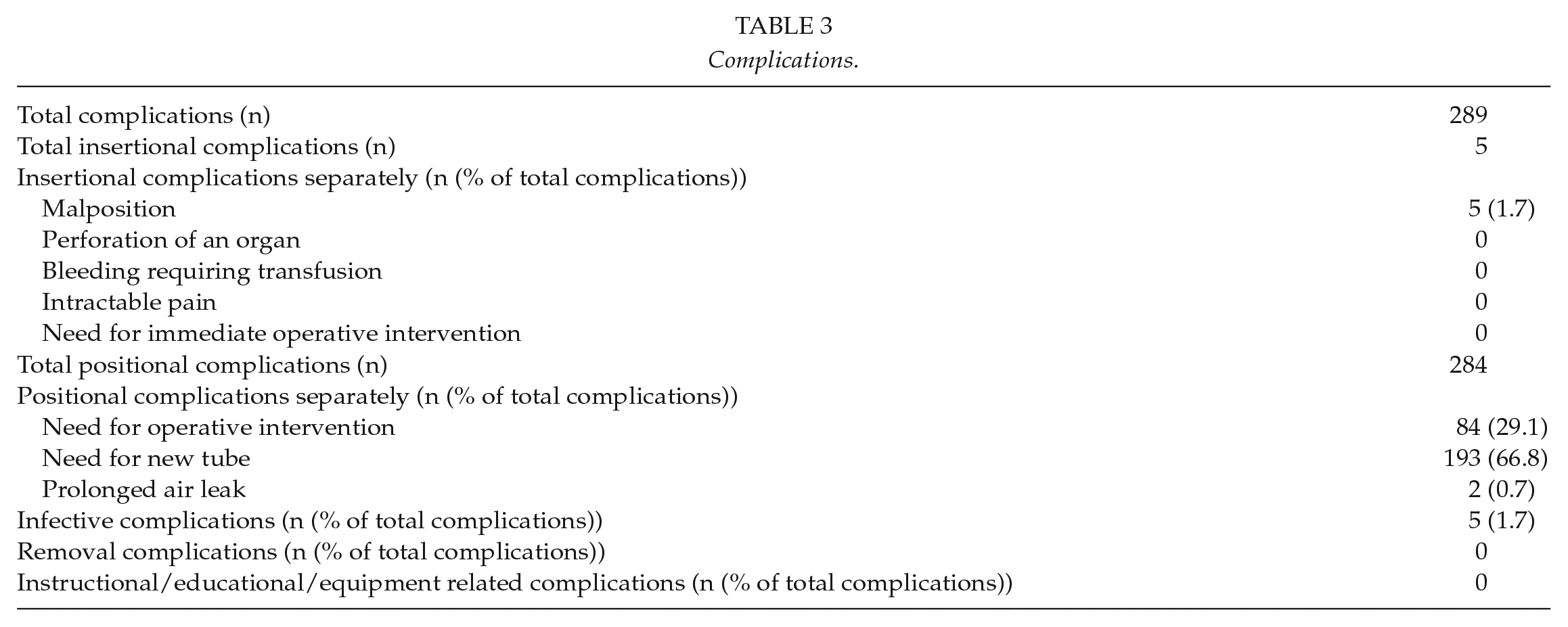
In this study, there were 289 complications in 233 patients (19.9%) after chest tube placement. The most common type of complication was positional in 96.5% of patients, meaning that the tube did not perform adequately during the treatment period. Only 1.7% of the complications were insertional complications and 1.7% of the complications were infective. Removal and instructional/educational/equipment-related complications did not occur. In the present study, there was no perforation of an organ, bleeding requiring transfusion or intractable pain.
In 66.8% of cases, the positional complications were a need for a new tube and in 29.1% of cases, operative intervention was needed to treat the underlying cause for which the tube was placed. A combination of need for operative treatment and a new tube occurred in 49 cases. There were altogether 103 deaths, none of which were attributable to the chest tube placement itself, and all of them occurred later than 24 h after tube insertion.
Among the diabetic patients, complication types were distributed similarly to the whole population; 51 diabetics had altogether 60 complications; 1 (1.7%) malposition, 17 (28.3%) need for operative intervention, and 42 (70.0%) need for a new tube (Table 3).
Complications.
On multivariable binary logistic regression, chest tube size CH16 was associated with a lower risk of complications (odds ratio (OR) 0.22, 95% confidence interval (CI) 0.10–0.52, p < 0.001) and diabetes was associated with an elevated risk of complications (OR 1.86, 95% CI 1.28–2.70, p = 0.001).
Discussion
The main finding of this study is that although complications occur in one out of five patients receiving a TT, severe complications are infrequent. TT is a frequent procedure; based on the present study, the yearly incidence in Southwestern Finland is at least 28/100,000 inhabitants not including postoperative chest tubes and bedside tubes at intensive units (population of the catchment area approx. 460,000 inhabitants) (8). In spite of it being a staple procedure of acute medicine, its complications have not been extensively studied. Most of the previous studies on the epidemiology of chest tube complications have described outcomes in trauma patients only (4, 6). There exists few studies including patients treated with TT for non-traumatic indications (9). The complication rates have been reported between 1% and 40% in previous studies depending on the definition of complications. Hernandez et al. (6) found in their systematic review and meta-analysis that the TT complication rate for traumatic indications has been approximately 19% during the past three decades identical to our study. In another study including patients treated with TT for any indication, the complication rate has also been approximately 19% (9). Based on the current study and existing literature, the frequency of complications related to TT is quite high. The complication rate is similar to that seen in trauma patients, although the patient population is quite different. The most common indication for the procedure was a primary or metastatic thoracic malignancy in 37.6% of patients and most of these were treated by a pulmonologist, with pulmonologist consequently being responsible for 40.5% of the chest tube placements. Malignancies as an indication have not been as frequent in other studies or it has not been defined as an indication itself (9).
Serious complications in the present study were, however, infrequent and no death was attributable to the chest tube placement. Nevertheless, 29.1% needed operative intervention, but operations were performed to treat the pre-existing condition for which the chest tube was placed, and no patient required surgery because of a complication related to the chest tube per se. There were 103 deaths after tube placement, which were almost exclusively due to malignancy in the nearly half of patients who received a TT for malignant pleural effusion.
In total, 98.3% of the complications occurred after 24 h and only five patients had early complications, all of which were malpositions. In earlier studies, the early complication rates have been higher. This is unlikely due to major differences in definitions as the classification of complications used in this study is quite similar to other studies (2, 7).
The most frequent complication was need for a new tube due to malfunction (e.g. occlusion) and the second most frequent complication was need for operative treatment. These two complications represented 95.9% of all complications and occurred in 19.5% of TT-treated patients. This is clinically relevant and implies that some form of reintervention is to be anticipated during the hospitalization. Whether some tube malfunctions could be avoided by primary placement of large bore tubes is possible, but previous literature on the importance of tube diameter is conflicting; many studies show similar treatment failure rates for both small and large tubes and based on the existing literature and for example, the British Thoracic society advocates small size chest tubes as first-line treatment for noninfectious indications. Most of the studies on size, however, are also retrospective and do furthermore do not fully adjust for the viscosity of the treated effusion and other patient-specific factors (10–12). The prospective randomized TIME study showed no difference in efficacy or complications between small and large tubes, although notably the study was no designed to assess complication rates (13). Several studies, including one prospective randomized, specifically on malignant effusion have demonstrated similar results and complication rates irrespective of tube diameter (14–16). In this study, small CH16 tubes were independently associated with fewer complications. These tubes were mostly inserted by pulmonologists (95.8%) and almost exclusively for malignant effusion. Consequently, extrapolating the results to other indications should be made with caution.
Diabetics were also more likely to experience a complication. The reason for this is unclear as the higher incidence of complications was not explained by a higher infection rate. Also, the indications were similar to the whole population in diabetics and the frequency of infective indications was even slightly lower (13.7% vs 15.9%). The most likely explanation is a type I error, but it could also be explained by a higher comorbidity burden in diabetics. This is possible especially as most of the diabetics had type II diabetes, alluding to obesity and other lifestyle-related factors that typically increase the frequency of postprocedural complications. Aside from diabetes, empyema or parapneumonic effusion as an indication for treatment was associated with complications. This is intuitive, as infective collections of the pleura are often viscous and adhesions are frequent, which entail a propensity for tube occlusion. Notably, most studies advocating preference of small tube sizes for other indications still recommend large sizes for empyema and hemothorax.
Infection was the only potentially serious complication directly caused by the tube in this study. Infections accounted for only 1.7% (five cases) of the complications. Other serious complications primarily caused by the drain were nonexistent in the present study while the literature describes a large spectrum of possible complications (9, 17).
Limitations
The study has all the limitations inherent in a retrospective registry-based study; incompleteness of data and lack of prospective data collection leading to possible missing data on preprocedural characteristics. Some minor complications might be missing, but complications requiring in-hospital treatment are identifiable from procedural codes, medication charts, and blood product reporting. Also, the information gained from this study cannot be directly applied to describe complication frequencies in patients receiving bedside or imaging guided chest tubes, which were not included in the present patient population.
Conclusion
TT is a common procedure and complications occur in 19.9% of patients. Serious complications caused by the chest tube placement, however, are extremely rare. Complications were more common in diabetics and patients receiving a chest tube for empyema or parapneumonic effusion. Small CH16 tubes were associated with a lower incidence of complications but were also most frequently used for palliative care in cancer patients. Cases where TT is insufficient or malfunctioning the need for a new tube (16.5%) or operative intervention (7.2%) are, however, quite common and should be anticipated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the institutional review board of Southwestern Finland Hospital District.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.