
Abstract
Background and Aims:
Colorectal cancer is the third most common cancer among both men and women in the United States. We aimed to determine racial and socioeconomic disparities in emergent colectomy rates for colorectal cancer in the US Health Care system.
Material and Methods:
We performed a retrospective analysis of the National Inpatient Sample including adult patients (⩾18 years) diagnosed with colorectal cancer, and who underwent colorectal resection while admitted between 2008 and 2015. Multivariable logistic and linear regression were used to assess the association between emergent admissions, compared to elective admissions, and postoperative outcomes.
Results:
A total of 141,641 hospitalizations were included: 93,775 (66%) were elective admissions and 47,866 (34%) were emergent admissions. Black patients were more likely to undergo emergent colectomy, compared to white patients (42% vs 32%, p < 0.0001). Medicaid and Medicare patients were also more likely to have an emergent colectomy, compared to private insurance (47% and 36% vs 25%, respectively, p < 0.0001), as were patients with low household income, compared to highest (38% vs 31%, p < 0.0001). Emergent procedures were less likely to be laparoscopic (19% vs 38%, p < 0.0001). Patients undergoing emergent colectomy were significantly more likely to have postoperative venous thromboembolism, wound complications, infection, bleeding, cardiac failure, renal failure, respiratory failure, shock, and inpatient mortality.
Conclusion:
There are significant racial and socioeconomic disparities in emergent colectomy rates for colorectal cancer. Efforts to reduce this disparity in colorectal cancer surgery patients should be prioritized to improve outcomes.
Introduction
Cancer is a major public health problem and is the second leading cause of death in the United States (1). Previous studies have shown that cancer patients are facing racial, socioeconomic, and geographic inequalities in terms of oncologic outcomes (2, 3).
Colorectal cancer (CRC) is the third most common cancer among both men and women in the United States, with approximately 135,430 individuals newly diagnosed and 50,260 deaths from the disease in 2017 (4). Screening by colonoscopy has proven to decrease CRC incidence and mortality, and prevent advanced-stage diagnosis of the disease (5). Late-stage CRC is often associated with complications requiring emergent surgery such as obstruction, perforation, and hemorrhage.
The US Health Care system is not universally accessible as in many countries of Europe, but rather a publicly and privately funded, complex, and fragmented system. Medicare and Medicaid, implemented by President Johnson in 1965, are government-funded programs intended to provide care to vulnerable populations. Despite continuous efforts to enhance medical care, many Americans still fail to obtain appropriate health care (6–8).
We hypothesized that there are still significant racial and socioeconomic disparities in emergent admissions for CRC. Therefore, we aimed to determine disparities in emergent colectomy rates for CRC in the US Health Care system.
Material and Methods
A retrospective analysis of the National Inpatient Sample (NIS) database was used to assess potential disparities in the surgical treatment of CRC. The NIS is part of a family of healthcare databases developed through a federal-state-industry partnership sponsored by the Agency for Healthcare Research and Quality (AHRQ) in the United States. The NIS is considered the largest publicly available all-payer health care database in the United States, representing a 20% stratified sample of all hospital discharges (roughly 7 million hospital stays each year), and includes patient demographics, diagnosis and procedure codes, hospital characteristics, discharge status, and length of stay. Eligible patients, their comorbidities, and inpatient complications were identified using International Classification of Disease, 9th revision, Clinical Modification (ICD-9-CM) diagnostic and procedural codes included in the discharge records.
Hospitalizations of adult patients (⩾18 years), diagnosed with CRC (ICD-9-CM 153-154.8), and who underwent either laparoscopic (17.3–17.39, 45.81, 48.42, and 48.51) or open (45.7–45.79, 45.82, 45.83, 48.40, 48.43, 48.49, 48.50, 48.52, 48.59, 48.64, and 48.69) colorectal resection while admitted between 1 January 2008 and 30 September 2015 (before ICD-10 codes were implemented) were included. Patients missing admission type (elective vs emergent) were excluded (n = 355). Patients with procedure codes for both laparoscopic and open resections (n = 695) were classified as open.
Comorbidities of interest included hypertension (401–401.9 and 402–402.91), primary and secondary diabetes (249–249.91 and 250–250.93), obesity (278–278.8), renal insufficiency (585–585.9), coronary artery disease (414–414.9), peripheral vascular disease (443–443.9), chronic obstructive pulmonary disease (491–492.8), sleep apnea (327.23), tobacco abuse (305.1), chronic liver disease or cirrhosis (571–571.9), and anticoagulation use (V58.61).
The primary postoperative outcomes of interest included venous thromboembolism (415.11, 453.40–453.42, and V12.51), wound complications (998.13, 998.30–998.32, and 998.83), infection (54.91, 86.04, 567.22, 569.5, 995.9–995.99, 996.64, 998.5–998.59, and 999.3–999.39), bleeding (99.0–99.09, 998.11, and 998.12), shock (998.0–998.09), cardiac failure (410–410.9, 428–428.9), renal failure (38.95, 39.95, 584–584.9, 586, and V45.11), and respiratory failure (31.1–31.29, 96.04, 96.05, 96.7–96.72, and 799.1)
Statistical Analyses
Patient demographics, hospital characteristics, and procedure type were compared across procedure and admission type using Chi square and Student’s t tests, where appropriate. Quarterly rates of elective and urgent/emergent colorectal resections were estimated using Poisson regression.
Multivariable logistic and linear regression was used to assess the association between emergent admissions, compared to elective admissions, and inpatient complications, length of stay (LOS), and inflation-adjusted hospital charges, after adjusting for patient and hospital characteristics. Models were adjusted for admission year, elective admission, laparoscopic procedure, age, sex, comorbidities, hospital region, teaching status, and hospital size. Age was modeled as a restricted cubic spline.
All analyses were performed using SAS software version 9.4 (SAS Inc., Cary, NC). A p-value < 0.05 was considered significant for all the statistical methods.
Results
A total of 141,641 hospitalizations were included: 93,775 (66%) were elective admissions and 47,866 (34%) were emergent admissions. Elective and emergent admissions have remained relatively consistent between 2008 and 2015 (Fig. 1).
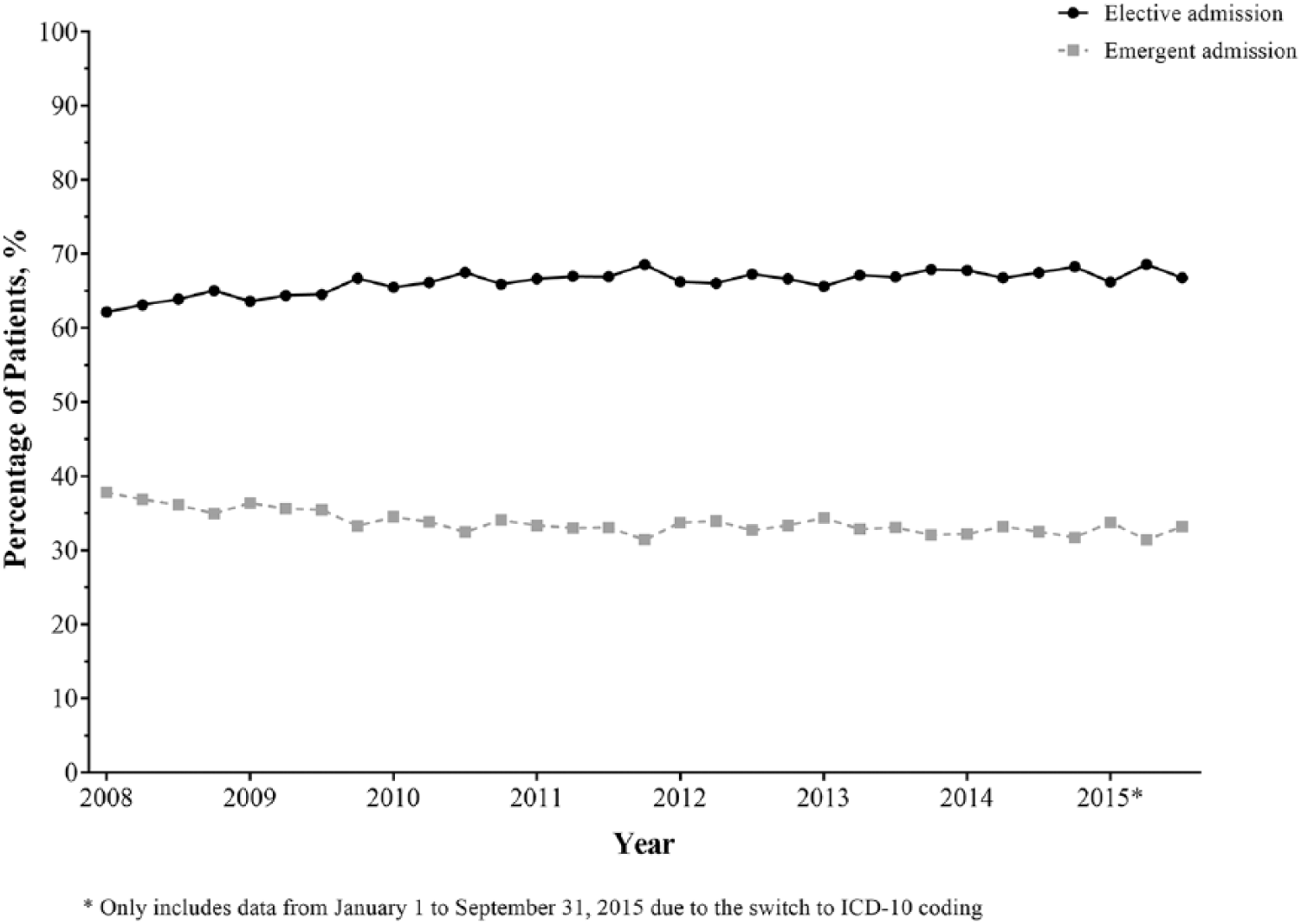
Quarterly rate of elective and emergent admissions for colectomy, among adult patients with colorectal cancer.
Black patients were more likely to undergo emergent colectomy, compared to white patients (42% vs 32%, p < 0.0001). Medicaid and Medicare patients were also more likely to have an emergent colectomy, compared to private insurance (47% and 36% vs 25%, respectively, p < 0.0001), as were patients with low household income, compared to highest (38% vs 31%, p < 0.0001). Emergent procedures were less likely to be laparoscopic (19% vs 38%, p < 0.0001). No meaningful regional differences in elective versus emergent admissions were seen (Table 1).
Patient demographics, comorbidities, and hospital characteristics, of adult patients with CRC and admitted for colectomy, stratified by admission type.
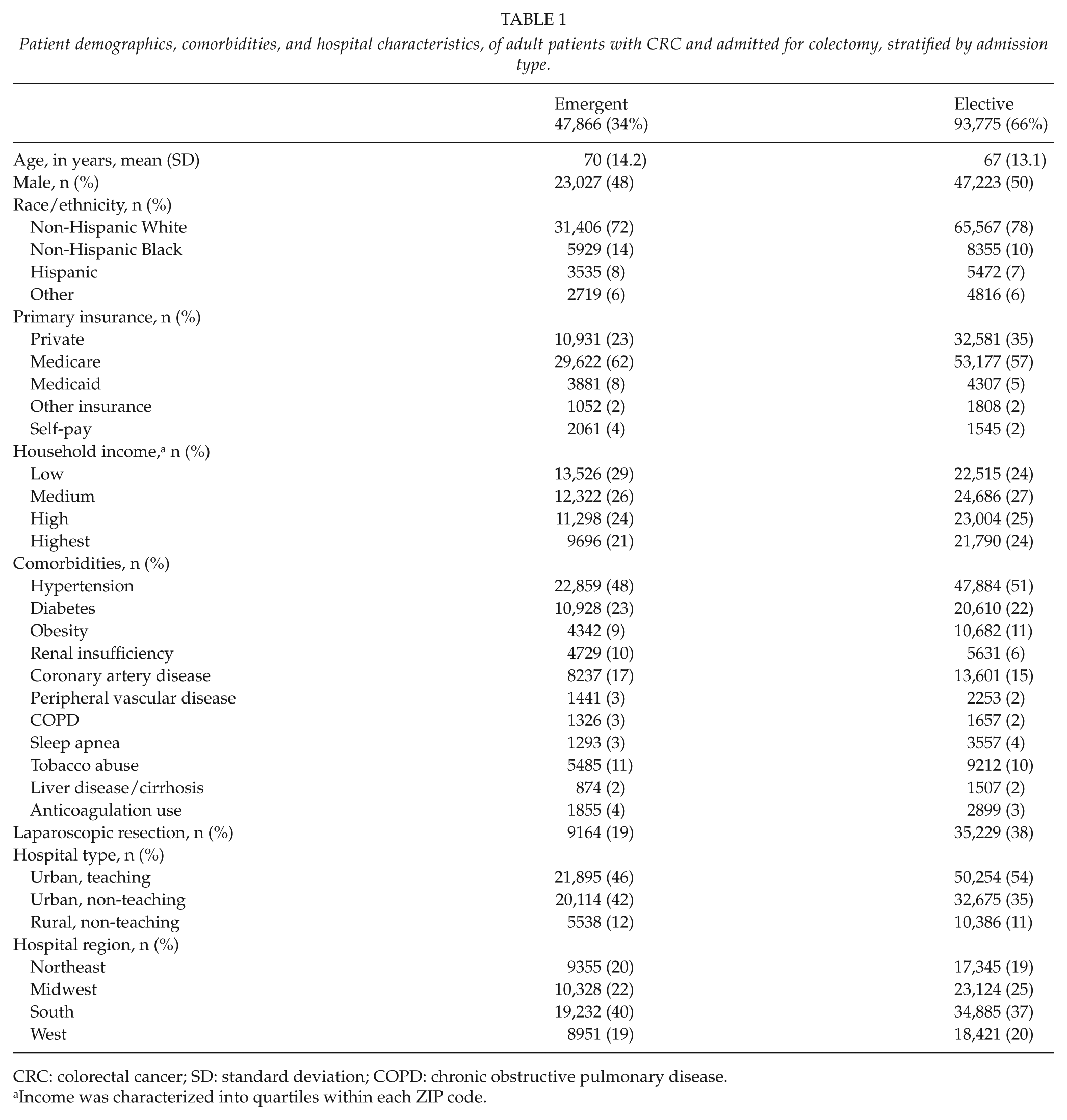
CRC: colorectal cancer; SD: standard deviation; COPD: chronic obstructive pulmonary disease.
Income was characterized into quartiles within each ZIP code.
After adjusting for patient demographics, comorbidities, and hospital characteristics, patients undergoing emergent colectomy, compared to elective colectomy, were significantly more likely to have postoperative venous thromboembolism (odds ratio (OR) 1.59, 95% confidence interval (CI) 1.50, 1.69), wound complications (OR 1.55, 95% CI 1.40, 1.72), infection (OR 2.96, 95% CI 2.84, 3.08), bleeding (OR 2.63, 95% CI 2.55, 2.70), cardiac failure (OR 1.97, 95% CI 1.88, 2.06), renal failure (OR 3.04, 95% CI 2.91, 3.18), respiratory failure (OR 2.99, 95% CI 2.84, 3.16), shock (OR 1.93, 95% CI 1.64, 2.26), and inpatient mortality (OR 3.23, 95% CI 2.98, 3.49). Emergent colectomy was also associated with significantly longer average LOS (CIE 4.8, 95% CI 4.7, 4.9) and significantly higher hospital charges (CIE 43.3, 95% CI 42.2, 44.4) (Table 2).
Adjusted associations between emergent colectomy, compared to elective, and inpatient outcomes, length of stay, and hospital charges, among adult patients with colorectal cancer.
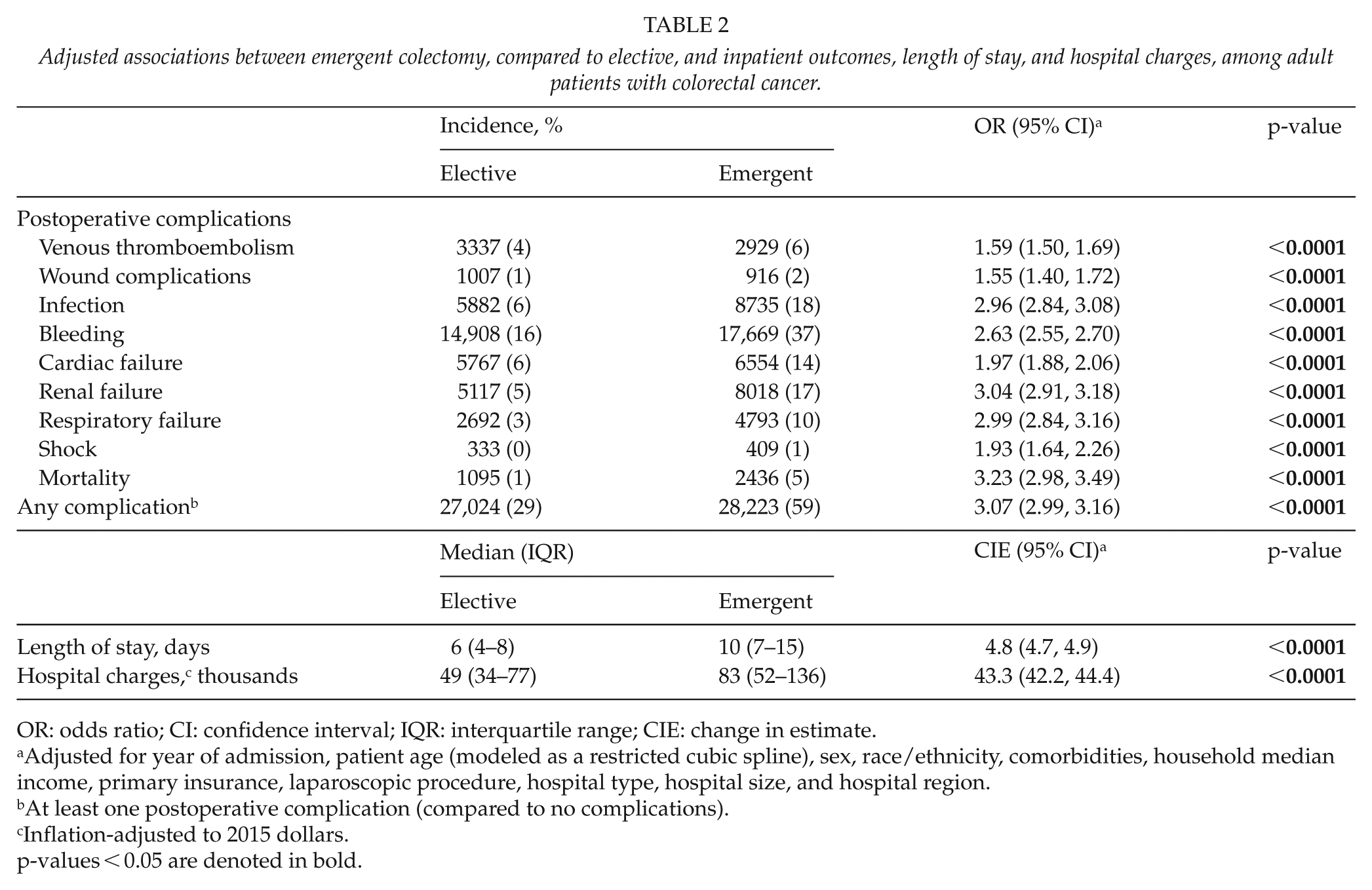
OR: odds ratio; CI: confidence interval; IQR: interquartile range; CIE: change in estimate.
Adjusted for year of admission, patient age (modeled as a restricted cubic spline), sex, race/ethnicity, comorbidities, household median income, primary insurance, laparoscopic procedure, hospital type, hospital size, and hospital region.
At least one postoperative complication (compared to no complications).
Inflation-adjusted to 2015 dollars.
p-values < 0.05 are denoted in bold.
Discussion
The objective of this analysis was to assess current disparities in emergency colectomy rates for CRC in the US Health Care system. We found that black patients, patients with Medicare/Medicaid, and patients with low household income were significantly more likely to undergo emergent colectomy for CRC. In addition, emergent colectomy was associated with significantly higher incidences of postoperative morbidity and mortality, longer LOS, and higher hospital charges compared to elective colectomy.
Previous studies have shown racial and socioeconomic disparities in CRC incidence, stage at diagnosis, and cancer related mortality (9–11). Since 1960, CRC mortality has declined by 39% among whites, but increased by 28% among blacks (12). The incidence and mortality from CRC is higher among blacks when compared with other race-ethnicities (13). A study calculated the age-standardized CRC death rates for three broad educational categories as a marker of socioeconomic status by race/ethnicity and state. Patients with the lowest level of education had significantly higher CRC death rates in virtually all states for each racial/ethnic group, suggesting that half the premature deaths resulting from CRC that occurred nationwide from 2008 through 2010 (7690 deaths annually) could have been avoided (14).
Screening rates are low among racial and ethnic minorities and socioeconomically disadvantaged patient populations. Shapiro et al. (15) reported than in 2005, about half of Americans ages ⩾50 years did not have appropriate CRC screening, and testing rates were particularly low among people without health-care coverage. Patients in lower socioeconomic neighborhoods are less likely to undergo a screening colonoscopy, even among insured subjects receiving care in integrated healthcare systems (16). Fear and past experiences with healthcare seems to influence preventive screening behaviors (17). Pruitt et al. (18), using 1992–2005 SEER-Medicare data, found that black individuals in low-income neighborhoods had increased odds of CRC emergency diagnosis and surgery. Similarly, we also found that traditionally underserved patients had higher rates of emergent colectomies for CRC. While these disparities may be due to lower rates of CRC screening among these patients, it is likely that reduced overall access to care, patient–physician miscommunication, and mistrust in the healthcare system may also play an important role.
An emergent colectomy for CRC is often performed in the setting of obstruction, bleeding, and/or perforation often in a septic critically ill patient. Hence, the procedure is associated with high morbidity and mortality rates (19, 20). In fact, our analysis demonstrated that CRC patients undergoing emergent colectomy had significantly higher incidence of life-threatening complications and inpatient mortality, as compared to those undergoing elective colectomy. In addition, we found significant lower rates of laparoscopic surgery in emergent procedures (19% vs 38%). This is particularly alarming considering the proven benefits of laparoscopic colectomy for CRC, offering faster recovery, less use of analgesia, and comparable oncological outcomes (21–23).
The US spends more on health care than other high-income countries in the world, and those spending have been increasing continuously over the last three decades reaching almost 20% of the gross domestic product (24). The uninsured rate dropped from 16.0% in 2010% to 9.1% in 2015, being the largest decline since the implementation of Medicare and Medicaid in 1965 (8). The largest gain in coverage was among the low-income adults due to Medicaid expansion fostered by the Affordable Care Act (ACA). However, people who make above 200% of the federal poverty level (about US$24.000 per year) are still responsible for considerable premium payments, preventing many Americans to their enrollment into ACA plans. In addition, even if patients are able to obtain government insurance, our study demonstrates that health outcomes are worse, as compared to those with private insurance.
This study has several limitations. First, the NIS does not link hospital records, and therefore all postoperative complications and mortality are limited to the initial admission. Second, there is potential for coding errors and differences in coding practices across hospitals in a national administrative database. Third, information about the complexity of the operation and stage of disease is not available, and we were not able to adjust for it. Finally, the use of diagnostic and procedure codes to identify inpatient complications is likely to underestimate the true incidence.
In conclusion, our data suggest that there are significant racial and socioeconomic disparities in emergent admission and colectomy rates for CRC. Considering the high prevalence of CRC and the existence of effective screening tools, efforts to eliminate these differences in CRC surgery patients should be prioritized to improve outcomes.
Footnotes
Acknowledgements
Francisco Schlottmann, Paula Strassle, Ashley Cairns, Fernando Herbella, Alessandro Fichera, and Marco Patti conceived the study and helped with literature search and writing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.